

Abstract
Bioelectrical impedance analysis (BIA) is the most widely used technique in body composition analysis. When we focus the use of phase sensitive BIA on its raw parameters Resistance (R), Reactance (Xc) and Phase Angle (PhA), we eliminate the bias of using predictive equations based on reference models. In particular PhA, have demonstrated their prognostic utility in multiple aspects of health and disease. In recent years, as a strong association between prognostic and diagnostic factors has been observed, scientific interest in the utility of PhA has increased. In the different fields of knowledge in biomedical research, there are different ways of assessing the impact of a scientific-technical aspect such as PhA. Single frequency with phase detection bioimpedance analysis (SF-BIA) using a 50 kHz single frequency device and tetrapolar wrist-ankle electrode placement is the most widely used bioimpedance approach for characterization of whole-body composition. However, the incorporation of vector representation of raw bioelectrical parameters and direct mathematical calculations without the need for regression equations for the analysis of body compartments has been one of the most important aspects for the development of research in this area. These results provide new evidence for the validity of phase-sensitive bioelectrical measurements as biomarkers of fluid and nutritional status. To enable the development of clinical research that provides consistent results, it is essential to establish appropriate standardization of PhA measurement techniques. Standardization of test protocols will facilitate the diagnosis and assessment of the risk associated with reduced PhA and the evaluation of changes in response to therapeutic interventions. In this paper, we describe and overview the value of PhA in biomedical research, technical and instrumental aspects of PhA research, analysis of Areas of clinical research (cancer patients, digestive and liver diseases, critical and surgical patients, Respiratory, infectious, and COVID-19, obesity and metabolic diseases, Heart and kidney failure, Malnutrition and sarcopenia), characterisation of the different research outcomes, Morphofunctional assessment in disease-related malnutrition and other metabolic disorders: validation of PhA with reference clinical practice techniques, strengths and limitations. Based on the detailed study of the measurement technique, some of the key issues to be considered in future PhA research. On the other hand, it is important to assess the clinical conditions and the phenotype of the patients, as well as to establish a disease-specific clinical profile. The appropriate selection of the most critical outcomes is another fundamental aspect of research.
Supplementary Information
The online version contains supplementary material available at 10.1007/s11154-023-09803-7.
Keywords: Phase sensitive bioelectrical impedance analysis, Phase angle, Body composition, Morphofunctional assessment, Bioelectrical impedance vector analysis, Outcome research
Introduction
Bioelectrical impedance analysis (BIA) is a technique often incorporated in daily clinical practice to assess body composition, mainly to assess muscle mass and hydration. The classical approach to BIA is based on regression models, derived from human subject studies of certain profiles, which restricts the usefulness of the derived model in other patients. Measurements are compared with reference techniques, such as dual energy Dual Energy X-Ray Absorptiometry (DXA) and computed tomography (CT), to create regression equations [1, 2]. These results are usually expressed in IU metric system (kilograms or liters), are used to set cut-off points that relate to clinical outcomes and help us make decisions in clinical practice. However, raw bioelectrical parameters, such as phase angle (PhA), are emerging in clinical practice.
More recently, the technique of bioelectrical impedance vector analysis (BIVA) with raw bioelectrical data has started to be applied with vigor. Bioelectrical data has made it possible to compare parameters [resistance (Rz), reactance (Xc), impedance (Z), PhA, and body cell mass (BCM) derives from equations of total body Capacitance] that do not depend on regression formulas. This technique can be understood in a similar way to other “electrogram techniques” that record the electrical activity of organs such as the brain and heart, measured by monitoring the change in electrical properties. This is a new concept called "the electrogram of the cell" or “electrocellgram®” [3].
It is essential to establish future lines of research on PhA based on an exhaustive knowledge of the measurement mechanism. It is necessary to know the bioelectrical bases that establish the passage of the current through the organism, evaluating the voltage drop as a function of body R, and therefore of the volume of water and hydration, up to the measurement of the circuit capacitance evaluated through the Total body Parallel Xc evaluates the cell and the integrity of cell membranes. This global model makes it possible, expressed jointly through the PhA, to evaluate changes in cell membranes and the hydration status of the organism [4].
Raw bioelectrical parameters, in particular PhA, have demonstrated their prognostic utility in multiple aspects of health and disease [5]. Future research on the clinical characteristics of different diseases is needed to determine how to translate scientific knowledge on PhA into clinical practice.
Some of the key issues to be considered in future PhA research are based on the accurate study of the measurement technique. Secondly, it is important to assess the clinical conditions and phenotype of the patients, as well as to establish a specific clinical profile for each disease. Another fundamental aspect of research is the appropriate selection of the most critical outcomes. The prognostic value of PhA can be assessed in terms of overall mortality, cause-specific mortality, medical and surgical complications, length of hospital stay and use of healthcare resources. There is limited work evaluating the prognostic changes produced by PhA modification with different interventions and treatments. Future research should be directed at assessing how different treatments modify the PhA and this in turn leads to a prognostic change in morbidity and mortality.
Due to the inherent limitations in the performance of the technique and the analysis of bioelectrical data, external validation of PhA with other techniques in routine clinical practice as nutritional ultrasound or handgrip strength is very important. Morphofunctional assessment consists of a set of methods for the clinical evaluation of changes in body composition from a morphological and functional approach [6].
Overview of the value of PhA in biomedical research
Scientific interest in the usefulness of PhA has been increasing in recent years, as a strong association between prognostic and diagnostic factors has been observed. There are different ways to evaluate the impact of a scientific-technical aspect, such as PhA, in the different areas of knowledge in biomedical research. One of the aspects to highlight would be to evaluate the number of publications and the number of publications in different scientific journals and other bibliometric sources indexed in biomedical and research databases.
In an analysis of the impact that the PhA has on research, we have carried out a search in “Scopus” from Jan 2004 applying the terms "phase angle" AND "PhA". The result has been more than 350 publications since 2004, with a progressive increase in recent years. The trend is increasing and in 2022 alone 20% of the articles were published. Most of them were original articles, although the number of reviews increased, given the interest in the joint evaluation of publications from different areas (Fig. 1A). Systematic reviews have been published on cancer [5, 7–10], sarcopenia [11], surgery [12], critical illness [13], heart failure and chronic kidney disease [14], obesity [15], metabolic diseases [16], coronavirus disease-2019 (COVID-19) [17] and in different diseases states [18]. Systematic reviews and meta-analysis to estimate mean PhA values in healthy individuals [19], critical illness [20], and cardiovascular diseases [21].
Fig. 1.

Overview of the diversity in distribution of peer-reviewed publications in Scopus including phase angle in biomedical research. a Number of publications. b Publication areas. c Geographical distribution of publications. d Type of medical journal. Abbreviations: PhA: phase angle
Although initially it could be for global interest from the point of view of social sciences, environmental sciences, engineering, agriculture, etc., the largest number of PhA publications is focused on the field of health. Almost half of the publication areas are in medicine, with a high percentage in nursing and health professionals (Fig. 1B). This is important as it seems that in the future, research proposals aimed at different diseases will be launched to ascertain the prognostic factors and the impact of PhA in their evaluation. The PhA can be useful for assessing mortality risk, staging, severity and severity of emerging diseases such as COVID-19 [22].
In the world-wide geographical distribution of publications, Europe stands out with more than 50% of the publications, mainly in Italy, Portugal and Germany. United States, Brazil and the United States also stand out with Asia (Japan and China) to a lesser degree. These geographical areas are prominent as a result of the availability of different phase sensitive bioimpedance measurement devices (Akern, Data Input, InBody, Maltron, RJL, Tanita, Xitron, etc.) (Fig. 1C).
It is also interesting to note how most of the publications are concentrated in emerging open access indexed journals with a focus on nutrients (Fig. 1D). It is important to highlight or reflect on how such a specific aspect as PhA needs reviewers specialized in the evaluation of manuscripts submitted to journals. It is probably necessary to extend knowledge of PhA to journals with a more global scope.
The analysis of the “Web of Science” database yielded 361 publications classified in research areas with more than 10% of bibliometric impact: physiology, nutrition and dietetics, endocrinology metabolism, geriatrics gerontology, pathology, demography, health sciences services, science technology, other subjects, biochemistry molecular biology, general internal medicine, food science technology, anatomy morphology, sports science, mathematics, neurosciences neurology, gastroenterology hepatology, oncology, and paediatrics (Fig. 2).
Fig. 2.

Phase angle research areas. Web of Science
The “Knowledge Map” from PubMed presents a topical summary of PhA research based on the 100 most relevant articles that match the search query. The algorithm groups documents that have many words in common. Area titles are created from the subject keywords of the documents that have been assigned to the same area. In this search 13 areas are listed (Material Supplementary). They select those keywords and phrases that appear frequently in one area and rarely in others (Fig. 3).
Fig. 3.

Knowledge Map of "phase angle" of the main areas and the documents (https://openknowledgemaps.org/)
Scientific visualization is necessary to graphically illustrate a large amount of scientific information currently available. VOSviewer is a powerful tool for analyzing bibliomeric data and can be used in various fields, including science, social sciences, and humanities. Through the VOSviewer software, the bibliographic review can be complemented with this scientometric analysis. A bibliographic search was performed using equations that included units of analysis (authors, MeSH and keywords) and measurements units (co-authorship, co-occurrence and citation) related to PhA in the articles found in PUBMED. The result is a map with the most common topics (Fig. 4). In this way, it is possible to determine what research has been done on the subject.
Fig. 4.

Bibliometric map of keywords related to phase angle (VOSviewer software). The search was carried out on February 2, 2023
The circles or "nodes" on the map describe the presence of the relevant keywords. We can see that "body composition", "bioelectrical impedance", "malnutrition", "sarcopenia" are the most relevant nodes by size and proximity to "phase angle". In other words, they are the most researched topics. More distant and less focused nodes such as "cachexia", "intensive care unit", "heart failure" indicate that they are less related to the other nodes and may be isolated or emerging research trends. This tool is very useful to see trends in research, authors and relevant institutions. It is even possible to perform a temporal analysis that locates by years the evolution of research in a thematic area [23].
The global vision of the different areas of research highlights the need to deepen in different aspects related to new areas where evidence is important to advance the application of PhA in clinical practice.
Technical and instrumental aspects of phase angle research
Research is increasing on the use of bioimpedance variables including PhA as potential markers of nutrition status and/or clinical outcomes. Regardless of the device, bioimpedance involves the administration of a weak, alternating electrical current at one or more radiofrequencies through leads attached to surface electrodes in order to characterize the conductive and nonconductive tissue and fluid components of the body composition [4].
Therefore, the potential applications available depend on the nature of the device at hand, including the number and range of frequencies, software capacity, quality of circuit board, and other factors.
Mixed reports in the validation literature for all bioimpedance approaches have raised questions about absolute accuracy to estimate whole body composition in clinical populations, particularly those with abnormal fluid status and/or heterogenous body geometry in whom underlying method assumptions may be violated.
Although refinements in bioimpedance techniques have led to important advancements in the management of individuals, the clinical applications for whole body lean tissue assessment require additional development.
Validation studies in clinical populations have typically reported good group-level agreement between bioimpedance and reference methods based on correlation and paired t-test statistics, but poor accuracy at the individual level (ie: wide limits of agreement by Bland–Altman analysis) raises doubts about the capacity of bioimpedance techniques to accurately quantify whole body compartments. The estimation of kilograms or litres in absolute terms should not be the primary objective of BIA techniques.
Single-frequency bioelectrical impedance analysis (SF-BIA) using a 50-kHz single-frequency phase or non-phase detecting devices and wrist-ankle tetrapolar electrode placement is the most widely used bioimpedance approach to characterize whole body composition. However, the incorporation of vector representation of raw bioelectrical parameters and direct mathematical calculations without the need for regression equations for the analysis of body compartments has been one of the most important aspects for the development of research in this area [24].
Segmental bioelectrical impedance, may be used to discriminate fluid distribution in some disease (ascites, renal failure, surgery, etc.), skeletal muscle assessment in healthy subjects and individuals with altered muscle mass such as sarcopenia or cancer [25, 26]. To homogenise results in research, these techniques need to complement the global view of the organism with a segmental analysis that provides information on the pathology. The main scientific limitation of segmental devices is that they provide Rz and Xc values of each body segment (e.g., arm, leg, trunk) that are highly influenced by geometry (length and girth) and differ from whole-body measurements [27]. It is also important to standardise the position in which the measurement is taken, as this determines different values of Rz and Xc in the supine, sitting and standing positions and are dependent on gravitational effects on fluid distribution. Standardisation of the measurement technique, the frequency of measurement and the patient's position are all important in order to obtain homogeneous results that can be used to compare different studies.
Future research applications of BIA require a global measurement protocol that BI devices to give an overview of the bioelectric model of PhA and subsequently complement it with different approaches: segmental, multifrequency, different postures, etc.
Multifrequency BI devices introduce alternating current over frequencies ranging from 1 to 1000 kHz. This allows the PhA to be estimated at each frequency. Evaluation of PhA at other frequencies has not shown any clinical utility in the global model, probably because the peak current to voltage delay is recorded between 49 to 51 kHz. More clinical research is needed to clarify the usefulness and validate its appropriate application. [28, 29].
Bioimpedance measurements from current single- and multifrequency devices should not be used interchangeably because there is no agreement between devices to determine individual R, Xc, Z and PhA values of highly active populations, possibly due to methodological and biological factors [30].
Biophysical modelling of the spectral (Rz and Xc) data with nonlinear, least-squares curve fitting yields an interrupted semicircle or impedance locus that allows calculation of Cole model variables, principally R0 (resistance associated with extracellular conduction), R∞ (resistance associated with extra- and intracellular conduction), critical frequency indicated at the largest Xc value and membrane capacitance [31]. This technique can be used to estimate the frequency at which the PhA or Xc are highest. The clinical application of accurately measuring these parameters is currently unknown.
There are several PhA determinants. The PhA decreases with age due to a decrease in muscle mass which reduces Xc, and a decrease in water which increases R. Women have lower PhA values due to lower body muscle mass. The PhA increases proportionally with body mass index (BMI) due to the greater number of muscle and adipose cells at BMI values < 30 kg/m2 [32]. All these aspects are fundamental when carrying out research projects that consider physiological and pathological factors that may influence PhA values.
Normalization of BIA measurements is very important in epidemiological studies and in clinical practice, as bioelectrical impedance increases throughout the day in subjects in the supine position due to the displacement of body fluids from the extremities to the thorax [33]. Ellis et al. suggest that the BIA measurement be performed after 10 min of fasting in the supine position [34].
One of the main challenges for future research is to overcome the difficulties in analysing raw bioelectrical data, such as Rz and Xc, for which it is necessary to establish reference population parameters and normal distribution data of bioelectrical measurements [35]. It is essential to have an adequate standardisation of PhA results at the population level perhaps derived from meta-analysis of reference population data [19] to establish consensus on reference cut-off points for the interpretation of these markers. Additional research on the applications of standardized PhA data for clinical assessment is vitally needed. It is unclear whether adjustments can be made to align reference data generated from different populations using different devices [36]. Furthermore, additional research is needed to determine the appropriate use of standardized PhA (SPhA).
It is essential to establish adequate standardization of the PhA measurement technique to allow the development of clinical research that provide consistent results. Standardization of test protocols will facilitate the diagnosis and assessment of the risk associated with reduced PhA and for the evaluation of changes in response to therapeutic interventions.
Clinical application of PhA to assess nutritional status via body cell mass requires simultaneous evaluation in the context of hydration status by examining vector length on the R/Xc plot (a scatterplot that represents resistance in X-axis and reactance in Y-axis divided by height in meters) using BIVA. These results provide new evidence for the validity of phase-sensitive bioelectrical measurements as biomarkers of fluid and nutritional status [4] (Fig. 5).
Fig. 5.
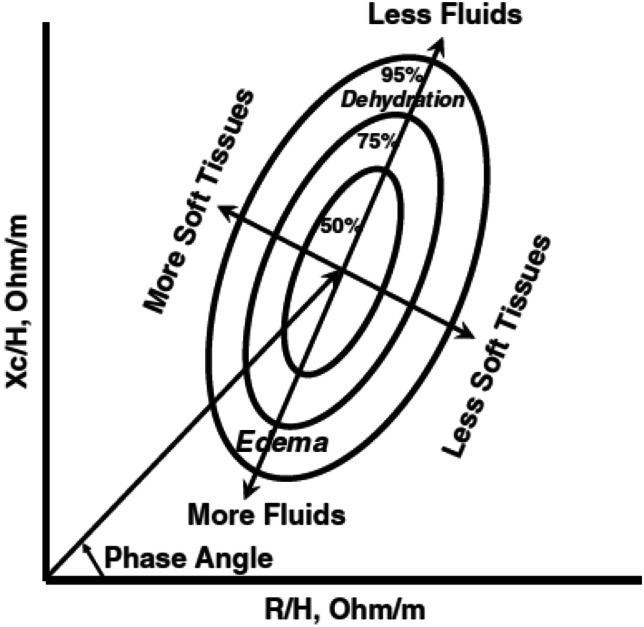
Generic RXc plot that illustrates the vector distributions with interpretations for fluid status and cell mass. Xc: reactance. Rz: resistance. H: height. Ohm: Ohms. M: meters
In the healthy situation there is a balance between the BCM and the hydration status of the FFM (Fig. 6A). In disease, different mechanisms can be established that affect both cellular health and hydration of the organism. In terms of a etiological mechanisms that can lead to a decrease in BCM, we can establish quantitative changes, e.g. malnutrition, sarcopenia and cachexia, which lead to a net loss of BCM and cell membrane surface area. This is related to the decrease in reactance and BCM (Fig. 6B). Cell damage is represented by the shift of the vector on the X-axis in the direction of cell mass loss (Fig. 6C) and leads to a decrease in PhA. Similarly, in the absence of a clear reduction in cell number, tissue or cell damage may be caused by inflammatory processes or oxidative stress, which alter and damage the cell membrane and lead to a functional loss of cell number. This is common in critically ill patients, situations of toxicity, hypoperfusion, oxygenation damage such as chronic cellular hypoxia, etc. (Fig. 6D).
Fig. 6.

Graphical representation of cell damage and hydration changes in the BIVA model. A Healthy person. Normal values of PhA, BCM and hydration. B Mecanism. Malnutrition, sarcopenia, caquexia. Values: low PhA, low BCM and normal hydration. C Cell damage is represented by the shift of the vector on the X-axis in the direction of cell mass loss and leads to a decrease in PhA. D Mecanism. Inflammatory damage, oxidative stress. E Mecanism. Congestion: heart failure (PRO BNP and CA125) and chronic kidney disease (glomerular filtration rate). F In the hydration mechanism, with no change in cell mass, there is a shift of the vector along the Y-axis, resulting in a decrease in PhA. G Mecanism. Inflammation (CRP and CRP/Prealbumin ratio). Low PhA, normal BCM, hight hydration. H: Disease. Patients. Low PhA, low BCM, high hydration. Legend:
 Heart failure.
Heart failure.
 Inflammation. Abbreviations: BCM: body cell mass. ECW: extra cellular water. NT-proBNP = N-terminal b-type natriuretic peptide pro. PhA: phase angle. Rz: resistance. TBW: total body water. Xc: reactance
Inflammation. Abbreviations: BCM: body cell mass. ECW: extra cellular water. NT-proBNP = N-terminal b-type natriuretic peptide pro. PhA: phase angle. Rz: resistance. TBW: total body water. Xc: reactance
Regarding the mechanisms of cellular hydration changes, we can see that there is a situation of increased hydration of the FFM in relation to vascular congestion, as occurs in situations of heart failure or chronic renal failure, where extracellular water increases due to hemodynamic failure (Fig. 6E). In the hydration mechanism, with no change in cell mass, there is a shift of the vector along the Y-axis, resulting in a decrease in PhA (Fig. 6F). A second mechanism is related to the inflammatory process that causes an increase in intracellular fluid due to the inflammatory situation by acute phase reactants that can occur in sepsis, intensive care, post-surgery, polytrauma, etc. (Fig. 6G).
In disease, there is usually a heterogeneous mixture of different etiological factors and adaptive mechanisms that can cause a quantitative and qualitative change in the BCM due to damage to cell membranes, while at the same time activating mechanisms that increase extracellular water in the context of congestion or inflammation (Fig. 6H).
Areas of clinical research
The usefulness of PhA assessment includes many different pathophysiological conditions. In both medical and surgical pathologies, there is a strong scientific interest in the study of oncology, critically ill patients, cardiology, nephrology, infectious and metabolic diseases.
Cancer patients
There is an important area of interest in the study of PhA in cancer patients in relation to nutritional status, body composition, physical function, complications of cancer treatments, overall survival, symptoms and quality of life (QoL). The literature suggests that PhA is correlated with body composition and physical function but only weakly correlated with nutritional status, complications, survival, symptoms, and QoL [7]. Furthermore, the PhA cutoff values vary significantly according to study and patient population. Thus, PhA has yet to be routinely incorporated into clinical practice for patients with cancer. Future research is needed to determine how to translate scientific understanding of PhA to clinical practice [37].
The association among PhA, symptoms, complications and QoL in patients with cancer is still unclear. Further research is needed in this area. In particular, the association of PhA with risk for complications of cancer surgery, severe adverse events like treatment interruption on radiotherapy treatment and overall mortality in patients with cancer should be investigated in the near future. We need to found clear PhA cutoffs demonstrating how PhA can enhance stratification of cancer patients and clinical decision-making prevents it from being adopted in routine practice. Future studies are necessary to examine the use of PhA in making therapeutic decisions. In addition, more research is needed to identify the critical PhA thresholds for predicting clinical outcomes, such as deteriorated functional status and increased mortality risk in cancer patients [38].
Critical and surgical patients
The assessment of raw parameters derived from bioelectrical impedance analysis (BIA) has gained importance in critically ill patients. PhA reflects cell membrane integrity that can inform us about malnutrition and cellular oxidative damage, and bioelectrical impedance vector analysis (BIVA) is indicative of patients' hydration status that can inform us about inflammation or congestion status. Despite the limited evidence, low PhA is associated in different studies with increased mortality and length of intensive care unit stay. BIVA-classified hydration is an additional tool for fluid status assessment in critically ill patients and is feasible to use in such patients. Directional changes in BIVA were consistent with directional changes in fluid balance. BIVA measurements of hydration status correlated with cumulative fluid balance during the time in the intensive care unit. High extracellular water/total body water (ECW/TBW) showed significant correlations with biochemical data like albumin, which are conventional nutritional assessment indicators. High ECW/ TBW was correlated with long duration of mechanical ventilation. PhA was also lower and ECW/TBW higher among no survivors than survivors, which implies utility of BIA for predicting survival rate. The fundamental limitation is that in the literature review, more than 40% of the primary studies were classified with a high risk of bias, and the quality of evidence ranged from low to very low [20]. We need further studies to assess the utility of BIVA in critically ill patients.
Future research should be directed towards the study of inflammatory changes and vascular congestion correlated with biochemical (N-terminal pro b-type natriuretic peptide (NT-proBNP), cancer antigen 125), clinical and imaging (point-of-care ultrasound) markers. It may also be useful to assess measures of Xc and body cell mass in studies of cell membrane damage in critically ill patients associated with hypoxia and other problems such as malnutrition and sarcopenia.
Preoperative assessment of PhA and SPhA, as an indirect estimator of host susceptibility, could predict the occurrence of infections, fistulas and other complications after major surgery. These BIVA parameters play an important and independent role in the outcome of surgical patients. In particular, preoperative assessment of PhA can predict the likelihood of infections after surgery and could therefore be used to identify tailored interventions, such as personalised antibiotic prophylaxis, to mitigate life-threatening sequelae [39]. Nutritional rehabilitation positively modulates cell mass parameters on patients scheduled for elective surgery and could therefore represent a beneficial strategy to attenuate the impact of the surgical stress response on lean tissue in an Enhanced Recovery After Surgery® setting. This effect may be even more evident in patients at high nutritional risk. It is necessary to design studies aimed at different surgical areas (abdominal, urological, gynaecological, thoracic, cardiac, head and neck surgery, etc.), different techniques (laparoscopic, robot-assisted, etc.), assessing risk detection and prevention strategies [40].
Digestive and liver diseases
In digestive pathology, malnutrition associated with inflammatory alterations and oxidative stress is common. the usefulness of PhA in patients with inflammatory bowel disease and liver disease has been validated in different studies, but there is significant heterogeneity between studies, mainly associated with differences in age, sample size and racial differences. In many series there are no data adjusted for age, sex, BMI or disease stage (severity and duration), which are factors influencing the PhA. This clearly affects the interpretation of PhA in the different pathologies of the gastrointestinal tract: upper and lower digestive tract, hepatobiliary, pancreas, inflammatory bowel disease, short bowel, ostomies, etc. Therefore, new studies should be designed to better characterize these diseases and address potential sources of bias. Nevertheless, PhA has been consistently found to be associated with prognosis, stage and severity of disease and has been found to be useful for monitoring fluid changes and response to interventions. Application in clinical practice on a prospective basis with serial measurements would allow monitoring of interventions and response to more individualized treatments and improve outcomes. In future research, efforts to harmonize measurements between different devices should be considered in order to obtain a more objective interpretation of the output data, with standardized phase angle values (SPhA) [41].
Respiratory, infectious, and COVID-19 disease
Malnutrition is a problem that cannot be ignored in patients with chronic lung diseases, in particular chronic obstructive pulmonary disease (COPD) and idiopathic pulmonary fibrosis (IPF), in their different stages of evolution and in relation to treatments as well as their follow-up, with special reference to the prognostic factors that may influence the therapeutic attitude. Among the BIA parameters, PhA allows clinical assessment of lean soft tissue mass in patients with COPD and IPF (malnourished, normal weight or overweight), independent of individual BMI. Future lines of research are required to establish further clinical evidence of the relationship between PhA at different stages of the disease, impaired muscle strength, reduced exercise capacity, higher mortality and increased risk of all-cause mortality [42].
The emergence of a new infectious disease, SARS-CoV2, has raised the scientific question of whether PhA by BIA could be a predictor of mortality and complications in patients admitted to hospital with COVID-19. With the scientific data currently available, we can conclude that PhA is a good prognostic marker of mortality and complications in this population. Although the results are promising, a universal cut-off point for PhA in this pathology has not yet been established. Future studies are needed to identify the PhA cut-off to guide therapeutic decisions more accurately. Low levels of PhA may indicate a worse prognosis and allow more appropriate supportive care for these patients. What we have learned in this infectious pathology opens the door for future studies in emerging pathologies for which we do not have reliable prognostic data [22, 43].
Obesity and metabolic diseases
PhA could be used as a prognostic marker of clinical conditions associated with obesity (such as fluid overload in heart failure, worsening of diabetes and its complications, inflammatory state, etc.) and to monitor some inflammatory, metabolic or endocrine diagnoses. PhA values, influenced by BMI, regional fat distribution and obesity-related comorbidities, can be used as new markers of cellular health during weight loss. PhA research is essential for the development of new therapeutic approaches to obesity and its consequences. Studies are required to assess new pharmacological treatments (such as glucagon-like peptide 1 agonists), lifestyle and physical activity programs (aerobic exercise and resistance training), and bariatric surgery procedures, to study the PhA and changes in the body composition. This is also relevant for establishing long-term weight maintenance protocols after weight loss [44]. It is essential to measure electrical values of resistance, Xc and PhA to assess changes in body composition in obese patients with a BMI above 35 [45].
Most chronic diseases, such as diabetes, atherosclerosis, cardiovascular disease, etc., share a common pathogenesis based on low-grade chronic inflammation associated with increased oxidative stress at the cellular level. Although fewer studies have evaluated the relationship between PhA and markers of oxidative stress, available data also suggest that PhA may be a potential indicator of oxidative damage. Future studies, including diverse pathologies, are required to confirm the validity and accuracy of PhA as a marker of inflammation and oxidative stress for clinical use [46, 47].
Heart failure
The application of PhA in clinical evaluation of patients with acute heart failure and chronic heart failure might be a good option in the future flow-chart evaluation of patients with heart failure [48]. Research should be based on large population studies to evaluate the impact of BIVA variables, PhA in particular associated with other parameter of water distribution ((total body water/fat free mass) (TBW/FFM), ECW/TBW, ECW %, etc.)) on the daily clinical management and prognostic stratification of HF patients. PhA per se cannot be considered as a “pure” biomarker in heart failure. The simple BIVA mode allows vector displacement as therapeutic feedback to detect, monitor, and even control congestion status. [49]. Multiparametric model for clinical and prognostic evaluation of heart failure should be preferred. Further studies are necessary for definite the clinical correlation to analytical (NT-proBNP, cancer antigen 125) and complementary test to quantifying systemic congestion with Point-Of-Care ultrasound: venous excess ultrasound grading system (Vex US) [50, 51].
Fluid overload is traditionally assessed non-quantitatively by clinical examination. Bedside medical devices using ultrasound and bioimpedance technology have been developed to standardise and more accurately quantify fluid status in heart. Fluid overload is a common manifestation in both conditions and has clinical and prognostic implications [52].
Associations between fluid overload and specific causes of death have not been widely reported in heart failure cohorts, so the review was limited to all-cause mortality. Therefore, future research is needed to analyse the different causes of mortality, progression of cardiovascular complications.
Its future scientific development for cardiac populations would benefit from consensus on the optimal device and standardization of methods for such patients. Large studies recording serial measurements and more detailed baseline and follow-up characterization of cardiac phenotypes are needed to more accurately and definitively quantify any threshold above which fluid overload is associated with risk and complications.
Chronic kidney disease (CKD)
This special issue on PhA did not provide a comprehensive review of the contributions of BIA methods to estimate fluid overload and predict volume of fluid to be removed during a dialytic session in patients with impaired kidney function. This omission was predicated on the limitations of the diverse applications of BIA and the inconsistent and contradictory findings. We provide a succinct description of viable BIA approaches that address clinically relevant issues related to patient care addressing the adverse physiological effects of severely diminished kidney function.
Chronic kidney disease is defined as a permanent impairment in renal function or damage to kidney structure. Advanced CKD, which can develop into end stage renal disease (ESRD), is a chronic inflammatory state that manifests clinically as excess fluid retention with hypertension and malnutrition due to prolonged inadequate protein intake. BIA can provide novel information to identify and monitor altered fluid status and loss of BCM.
Treatment of ESRD utilizes renal replacement therapy, notably HD to purify the blood. It is an extracorporeal technique that includes ultrafiltration to purify blood by removing water, electrolytes and urea using a semi-permeable membrane. The goal of UF is to achieve fluid balance (eliminate excess fluid) without undesirable side effects, such as cardiovascular events, nausea, and post-dialytic fluid retention, for the patient. Traditional approaches to assess hydration in patients with ESRD are unreliable because they rely on body weight to identify excess fluid and are insensitive to fluid overload in the presence of oedema [53].
Estimation of the volume of fluid for removal during HD is subjective and generally related to previous post-dialytic body weight, which can be unreliable [53]. Dry weight is the general term associated with the post-dialytic body weight at which most of the excess fluid has been removed. The “optimal” dry weight is estimated clinically and operationally as the weight at which a patient can tolerate HD without adverse intra-dialytic symptoms, notably hypotension. Unfortunately, post-HD dry weight can be mistakenly considered as a surrogate for adequate hydration and be undependable for an individual patient [54].
Initial BIA approaches have not successfully enabled reliable and appropriate fluid removal without complications during HD. Use of 50 kHz and multiple frequency BIA measurements in population-based multiple regression equations, which include body weight and derived in healthy individuals to predict pre-HD fluid volumes, as well as BIS with questionable assumptions on intracellular and extracellular resistivity and also include body weight to estimate fluid overload, have not been adequate for patient care [28, 55–57]. Multiple frequency and 50 kHz BIA measurements similarly track fluid removal during HD, which indicates the equivalence of the measurements per se, highlights the limitations of using dubious prediction models to estimate fluid volumes in CKD [58].
Successive Rz and Xc measurements standardized for height provide individual vectors using BIVA before and after HD reveal a classic pattern of fluid removal and repletion during a standard 3-d HD cycle. Fluid removal using UF accompanies vector lengthening and PhA increase parallel to the mean vector of healthy adults. Within the first 2 h post HD, vectors are relatively stable near the post HD vector. During the next 24, 48, and 72 h however, vectors progressively shorten and reflect fluid repletion of 1.4, 2.6, and 3.4 L [53, 59]. Thus, vector displacement is sensitive and specific to identify and monitor fluid shifts in the wet and dry cycle of HD. Additionally, patients with low PhA values (< 4.5°) and normal Rz values have an increased risk of mortality [60], which is consistent with results of prospective studies in which low PhA and shortened vector length were associated with increased risk of death and incident heart failure [61].
Patients with CKD are progressively at risk for malnutrition, worsening of renal function and protein energy wasting that can lead to increased mortality risk and ESRD [62]. Patients with CKD have shorter vectors and decreased PhA values compared to age and sex-matched healthy controls [63]. Reduced PhA values generally indicate loss of BCM, provided that hydration status is considered [64], and an increase in extracellular water/intracellular water (ECW/ICW) due to disproportionate loss of muscle and expansion of ECW indicating fluid overload. Low pre-HD PhA values are prognostic for increased risk of morbidity and mortality.
Reduced nutritional status classified using the subjective global assessment screening tool impacted BIA measurements before and after an HD session [65]. Before dialysis, patients with adequate nutritional status had vectors indicating normal hydration whereas patients with poor or at increased risk of malnutrition had vectors indicating progressive fluid overload. Importantly, Xc decreased with increasing exacerbation of nutritional risk. The vectors of all patients lengthened proportional to amount of fluid removed. However, an increase in Xc/H occurred only in patients with normal or moderate malnutrition risk suggesting loss of BCM in patients at high risk of malnutrition. The inference is that post-HD PhA indicates poor nutritional status. Importantly, patients with low PhA values (< 4.5°) and normal Rz values had increased risk of mortality [60].
A compilation of the variations in altered fluid status (overload and dehydration) and malnutrition on BI measurements emphasizes the importance of the simultaneous evaluation of PhA and vector position on the R/Xc graph (Fig. 7). Compared to healthy adults, patients with CKD, who are fluid overloaded, have an expanded ECW and can have normal ICW with a decreased PhA and a shortened impedance vector located in the lower left quadrant of the R/Xc graph whereas malnourished patients with CKD can have expanded ECW with loss of body fat and diminished ICW shown with a reduced PhA and vector length that is positioned in the lower right quadrant. The combination of fluid overload and malnutrition is expressed with loss of body fat, abnormal increase in ECW with diminution of ICW that is shown with a low PhA and a short vector in the right lower quadrant. The dehydrated patient with CKD can have a reduced ECW with a normal ICW and an increased PhA with a vector in the upper left quadrant. The dehydrated-malnourished patient with CKD has depleted body fat with decreased ECW and ICW; PhA is near normal and vector length is elongated. It also is important to recognize that individuals with the same PhA can have different hydration status based on vector position on the R/Xc graph [41, 66].
Fig. 7.

Illustration of the effects of hydration status and malnutrition on bioimpedance measurements and vector positions on the resistance-reactance graph using bioimpedance vector analysis. Abbreviations: ECW: extracellular water. ICW: intracellular water. abn: abnormal. nl: norma.l PhA: phase angle. R/H: resistance normalized for height. Xc/H: reactance normalized for height
Rigorous evaluation of PhA in relation of BIVA should be assessed as a clinical tool to evaluate fluid status in patients with CKD to ascertain the sensitivity and specificity to monitor the safety of the rate of fluid volume removal to mitigate adverse intradialytic responses to HD [67]. Additional research is needed to evaluate PhA, in consideration to hydration status, as a clinically useful indicator of risk of malnutrition and depletion of BCM. Key issues include determination of predictive value of vector length and displacement, assessed with PhA, in relation to intermediate cardiovascular variables (blood pressure, cardiac dynamics, morphology) to preserve residual kidney function.
Malnutrition and sarcopenia
BIVA offers a practical approach to identify malnutrition and prognosis by assessing whole-body cell membrane quality and depicting fluid distribution for an individual [37, 66]. PhA and FFM measures were most commonly evaluated and correlated with nutritional status and survival rate. One limitation of FFM measures with quantitative values is the high interpatient variability which requires careful interpretation of results in the context of the individual patient rather than comparison with population data [37]. The use of measured raw variables from BIA rather than estimation of body compartments has gained popularity in the clinical setting. BIVA has been developed to partially eliminate multiple sources of error [68].
However, PhA is strongly influenced by age, gender and body mass index. This observation has stimulated its implementation and the development of z-scores (SPhA) normalized to age, sex and BMI strata reference values from the general healthy population [69]. Nevertheless, the impedance vector, which mainly reflects soft tissue mass, still has value in clinical assessment. It is noteworthy that lean body mass is closely associated with malnutrition and inflammation, both of which are predictors of SPhA. Multiples studies that addressed the relationship of SPhA use to nutritional status, complications, and survival in patients have been evaluated. The standard cut-off value for SPhA has not yet been determined. Data from the selected studies suggest that SPhA might be a predictor of nutritional status. Further studies are needed to determine the value of SPhA in predicting nutritional status and clinical outcomes in different patients [36].
BCM, the metabolically active component of lean body mass, is the best predictor of a patient's nutritional status. The normal range of BCM changes with differences in body weight. Body cell mass index (BCMI), calculated as BCM divided by height squared (kg/m2) [5], has been shown to be more sensitive than BMI to changes in protein status and lean tissue. The loss of muscle mass in pathological conditions such as malnutrition is best described by the loss of BCM [70]. In overweight and moderately obese patients, BCM is more closely related to lean body mass than BMI. In addition, the BCM, extracellular water and fat mass (FM) values obtained with BIVA allow the assessment of nutritional status and body fluid balance, which are often affected in malnourished patients. Different BIA devices may under- or overestimate BCM when using the manufacturer's equations. Therefore, it may be useful to apply the device-specific equations, which reduce bias and limits of agreement with the reference method. However, external validation of the algorithms will be required before these equations can be adopted for other groups. A major goal for future body composition research must be to standardize the different bioimpedance analyzers in terms of their comparability and validity. This will require multicenter studies in defined populations and different clinical conditions [71].
Some studies have proposed other parameters that aim to integrate the information provided by impedance vector and PhA into a single numerical variable with a focus on specific resistance changes (Rz/H). The Nutrigram® parameter was developed to provide a numerical index of nutritional status that adequately reflects Body cell mass index (BCMI). The index is consistent with the creatinine height index (an index based on the ratio of actual to ideal urinary creatinine excretion) and the normalization of ideal urinary creatinine values for height. The evaluation of 24-h urinary creatinine as a surrogate for muscle mass, the main component of BCM, in humans has been the subject of several studies. Normalization of the resulting values for height allows patients to be categorized into four intervals with easy and immediate identification of malnutrition. Sex-specific reference values are provided. Its prognostic value and association with nutritional and functional status has been compared with fat free mass index (FFMI) and SPhA, two recognized relevant prognostic body composition parameters, in different cohorts of patients [72].
In malnutrition, the use of BIVA, where hydration is a function of the distribution of fluids in the extracellular and intracellular spaces, particularly BCM, is important. The use of BIVA in the assessment of malnutrition is increasing, especially in diseases with muscle wasting when hydration is impaired. In overhydrated patients, the fluid shift resulted in an increase in mean vectors due to large changes in Rz/H for normal and moderately malnourished patients. In contrast, the mean vector of severely malnourished patients flattened, with a smaller R/H change associated with fewer fluid shifts. Thus, BIVA discriminates excess fluid from nutritional status and identifies muscle mass deficiencies in malnourished patients with different hydration [56].
The tools currently available to assess hydration status are limited, not well standardized and validated for all clinical situations, and in many cases, it is difficult to distinguish between changes in nutritional status and hydration homeostasis. However, there is increasing interest in establishing reference values and the prognostic value of hydration measures. It is therefore important to make progress in the systematization of hydration measurements, to work on the development of predictive models based on pure bioelectrical measurements, which are known to be unaffected by confounding factors such as weight, and which allow us to obtain information on the distribution of body water and the cellular matrix. Currently, the analysis of phase-sensitive impedance variations is a non-invasive technique capable of specifically assessing hydration changes in different clinical conditions, independent of weight. The vector model allows the loss of BCM or increased ECW to be seen in inflammatory conditions related to malnutrition, which has been linked to poor prognosis [64].
Future research will evaluate the use of BIVA and PhA measurement in the clinical management of patients in a variety of ways: prevention, diagnosis, prognosis, and outcomes related to treatments that affect nutritional and overall health status.
Another interesting aspect related to malnutrition is sarcopenia. Sarcopenia and frailty are associated with changes in body composition. BIA is used with DEXA to determine lean body mass according to The European Working Group on Sarcopenia in Older People sarcopenia diagnostic protocol. PhA has been associated with sarcopenia by measuring muscle mass. Low PhA is associated with progression of frailty and sarcopenia, disability and poor outcomes in geriatric patients [35, 36].
Modern studies point out the positive aspects of BIA compared to DEXA, such as speed of diagnosis, no exposure of the patient's body to ionizing radiation, lower cost of the examination with high information content. The PhA indicates the quality of cell membranes and metabolic activity. The linear relationship between muscle mass and strength and clinical and biochemical parameters, including PhA at multivariate analysis were performed. PhA is inversely related to muscle mass and strength in elderly subjects and may be considered a good bioelectrical marker to identify elderly patients at risk of sarcopenia [73].
In future research, we need to investigate whether PhA has a good predictive capacity in relation to the diagnostic components of sarcopenia (physical performance, muscle mass and strength) and the capacity to assess change with intervention in clinical practice with a nutrition and exercise programmed [74].
Resistance training promoted an increase in PhA, resulting from an increase in Xc accompanied by a decrease in Rz. According to bioimpedance vector analysis, resistance trained individuals experienced a beneficial leftward vector displacement, whereas inactivity induced a rightward vector displacement within the R/Xc graph. More sophisticated and rigorous studies using specific criteria, methods and targeted designs are needed to determine which equipment and protocols allow for the optimization of resistance training effects [75].
Characterization of the different outcomes research
One of the greatest challenges in medicine today is to predict or estimate the risk of a pathological event occurring in a healthy individual or in a specific patient. Hence the growing interest in the role of diagnostic and prognostic biomarkers that can be identified in the subject. The National Institutes of Health (NIH) has defined a biomarker as an objectively measurable biological, biochemical, anthropometric, physiological, etc. characteristic that can be used to identify physiological or pathological processes or a pharmacological response to a therapeutic intervention. There are different types of biomarkers: diagnostic, prognostic or therapeutic. The ideal biomarker should be specific, sensitive, predictive, rapid and inexpensive, stable, non-invasive, and have sufficient preclinical and clinical relevance to change decisions about the pathological process to which it is applied. The PhA is a bioelectrical characteristic of the organism that can meet all these requirements [76].
The limitation of nutritional assessment to estimate BC status determines the need for biological determinants that can objectively and accurately quantify nutritional status. Biomarkers provide a more proximal measure of nutritional status [77].
The correct interpretation of a biomarker as PhA requires clearly defined reference values. Reference values are the values of PhA in a reference population, usually a group of healthy individuals. If the values follow a normal distribution, the reference range is the population mean ± 2 times the standard deviation, i.e. the central interval of 95% of the distribution. The interpretation of results obtained in BIVA is based on comparison with the reference values. A value that deviates from the reference range does not necessarily mean that it is abnormal, but it does mean that it is more likely to be associated with a deficit or excess and therefore relatively closer to pathological values. Reference ranges may depend on the characteristics of the population, age and sex; they may also differ for the different instruments, etc. The normal range of PhA in healthy individuals has been clearly defined [78].
One of the fundamental issues in future research on PhA is the definition of outcome research through global measures of health, health-related quality of life, health service utilization and its determinants, patient satisfaction and preferences for specific services, costs, etc. Outcome research uses almost all epidemiological designs, mainly observational. These include descriptive studies, prospective or retrospective cohort studies, case–control studies, and analyses of variations in clinical practice. The main limitation of observational studies is the presence of confounding factors, particularly disease severity and comorbidity. To control for these factors, specific measures of severity and comorbidity and adjustment techniques are available: regression models for risk adjustment (logistic regression, Cox, etc.).
The three main outcomes measured by outcome research are as follows: clinical, economic, and humanistic. Clinical outcomes are medical events (e.g., mortality or the rate of infection and hospitalization due to malnutrition) or physiologic measures (e.g., albumin, weight), whereas economic outcomes are disease- or treatment-related resource use and costs. Humanistic outcomes capture the impact of a treatment on patient well-being or health-related quality of life (HRQoL).
There is a need to include specific outcome research publications related to sarcopenia and malnutrition and frailty, which requires a standardized and agreed definition. It is also essential to include in PhA analysis global prognostic factors such as mortality or complications or length of stay and readmissions, and also some specific to certain processes such as surgery (dehiscence, re-invention), critical (need for mechanical ventilation) or other specific pathologies. It is also essential to incorporate the prognostic determination of the PhA in therapeutic intervention programs. This will allow the evaluation of changes with the implementation of different therapeutic strategies, nutritional support, pathology specific treatments and the impact of these measures on global and specific health.
The importance of the parameters for analysis of the results of the PhA as a diagnostic test is its ability to discriminate with certainty between a diseased subject and a healthy subject. Therefore, an ideal diagnostic test would be one that is able to detect the greatest number of patients with the clinical condition under investigation, while excluding the greatest number of patients without the condition. The most important parameters are sensitivity, specificity, positive and negative predictive values, likelihood ratios, and pre- and post-test probabilities. Procedures for their calculation and interpretation of results would be also provided. For any test related to the diagnosis of a defined disease (malnutrition, sarcopenia, etc.), reliability, reproducibility, internal validity (intra-test variability) and external validity (inter-test variability) must be considered, in addition to the quality control required to estimate the results. The PhA results help us to know the probability that a given patient does or does not have a particular condition, hence the importance of analysing these results in terms of sensitivity, specificity and positive and negative predictive values. In addition, the use of the likelihood ratio provides further support to the clinician in the diagnostic process by making explicit the change between pre-test and post-test probability. In this sense, the sensitivity and specificity of diagnostic tests can also vary considerably. Because the results of a diagnostic test may depend on the individual characteristics of many patients, studies reporting diagnostic correlations should also provide a detailed description of the different patient subgroups. Similarly, the potential effects of medical history, comorbidities, test protocol, and extent or severity of disease need to be considered so that the clinician can interpret PhA results as a diagnostic test with greater confidence [79].
It is important to make a critical reading of the validation studies of PhA as a diagnostic test, focusing on those publications that provide more information to the clinician with cross-sectional studies, which include a representative sample of the population of interest and where the results of PhA and the results obtained with a reference test (Gold Standard) that has previously proven to be useful, are analysed simultaneously [80, 81].
The research process would start with a clinical question. This would explicitly include all important and critical outcomes. Risk of bias, inconsistency, indirectness of evidence, imprecision and publication bias are the main areas used to assess the certainty of the evidence. Dose–response gradients, large effect sizes, and the effect of plausible residual confounding are factors that may increase the certainty of the evidence. For each outcome of interest, the quality of the evidence reflects how confident we are that the estimate of an effect is sufficient to support a recommendation. The GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach summarise the process in a simplified way [82].
Future studies need to be of the highest possible quality, internally valid, accurate, unbiased, and include clinical outcomes such as morbidity, mortality or serious complications. Knowing the variation in PhA that is clinically relevant in outcome research would allow health professionals to make decisions and incorporate it into clinical practice [83, 84].
Validation of PhA with reference Morphofunctional Assessment® techniques in clinical practice
Morphofunctional Assessment® focusing on the study of body composition and functionality provides a more sensitive and accurate understanding of nutritional status and body composition (BC), with consequent prognostic implications. Measurement of functional capacity with dynamometry and assessment of muscle and fat in specific regions with nutritional ultrasound® reflect the functional and morphological status of patients and their relationship to morbidity and mortality [85–88].
Morphofunctional Assessment® integrates various classical and advanced nutritional assessment techniques by evaluating changes in composition and function. This is done using parameters such as PhA, BCM and other electrical bioimpedance measurements, Nutritional Ultrasound®, Hand Grip Strength, functional tests, biochemical parameters such as C-reactive protein (C-reactive protein)/prealbumin, Health Related Quality of Life (HRQoL) and dietary compliance monitoring [6, 88, 89].
There are already studies showing correlations between PhA and other body composition parameters using nutritional ultrasound or functional parameters such as dynamometry in different pathologies (cancer patients, obesity, cystic fibrosis, hospital malnutrition or colon cancer) [85–87, 89–93].
There are other standardized techniques for measuring BC in research studies, such as DEXA, magnetic resonance image (MRI) and CT. The emerging techniques, such as ultrasound, are exploratory techniques that need to be validated against reference techniques as “gold standard” techniques whenever available [6].
The loss of lean mass affects the clinical outcome of both acute and chronic illnesses, and as such, its assessment is of particular interest in clinical nutrition. The application of emerging techniques such as the BIA and nutritional ultrasound are becoming increasingly important for nutritional status assessment.
An Expert Consensus on Morphofunctional Assessment in disease-related malnutrition has recently been published. This study develops evidence-based recommendations on the prognostic value of a range of morpho-functional tools and tests to assess malnutrition or risk of malnutrition. It also sought expert consensus on the usefulness and feasibility of these tools and tests in routine clinical practice. The implementation of these tools and tests is therefore recommended to improve diagnosis, treatment and patient outcomes [94]. It has become essential in clinical nutrition to establish lines of research that can provide results that help implement a clinically accurate approach based on the final health outcome.
It is important to have a global vision that brings together the different characteristics of the parameters analyzed in the clinical scenario in which they are to be performed, what variables we are going to measure and how we are going to correlate the variables derived from PhA and BIA together with the morpho-functional assessment. In this sense, as far as the main parameters are concerned, the PhA is obtained by a simple electrical determination in which the Xc and Rz of the hemisoma are measured at 50 KH conduction and a numerical data is obtained together with a vectorial representation in which it is compared with a reference population. Therefore, it is important that the data of the pure bioelectrical parameters and their comparison with the reference population are homogeneous and have a uniformity in order to be compared with different populations.
In the case of disease, we need to study in detail different clinical scenarios in different pathologies (cancer, surgery, critically ill patients, etc.). Each pathology involves a different mechanism of cell damage or hydration changes. For example, in patients with cardiac pathology, hydration changes predominate, but it is very important to estimate cell mass because malnutrition can be a very important determinant of health in patients with cardiorespiratory failure. Similarly, changes in oxidative stress and inflammation can be assessed by BIA and PhA. In terms of analyzing health outcomes, it is very important to establish that PhA as a biomarker correlate and establishes validated cut-off points in determining or predicting important health events such as mortality, morbidity, need for hospital admission, complications, as well as health care costs and quality of life.
The main point of interest of PhA in relation to prognosis is the ability to measure and predict, together with the ability to see the evolutionary changes of the therapeutic intervention. Therefore, we need to be able to assess the effectiveness of treatments for malnutrition, heart failure, inflammation, etc., measured by changes in PhA, vector distribution and derived bioelectrical parameters.
BIA is subject to limitations, to errors in the technique, therefore its validation with other techniques in clinical use through morphofunctional assessment is probably one of the most important aspects when it comes to the external validity of the results of PhA. In this sense, the support of other morphological techniques, such as Nutritional Ultrasound® or CT, is quite robust in the assessment of BC changes, while the assessment of functionality can integrate other important data that speak to the quality of the cell and the cell mass, such as Hand Grip Strength and functional tests (Fig. 8).
Fig. 8.

Graphical abstract: Parameters, Diseases, Cell mass and hydration changes, Outcomes and Morphofunctional assessment
Morphofunctional assessment is open to expansion into new areas outside malnutrition, such as metabolic disease, obesity, cardiology, critical patients, etc. It is also important to consider its usefulness in physiological changes such as ageing (frailty) and adaptations to changes in physical activity (training and exercise). In inflammatory processes involving oxidative stress and changes in cell membranes, PhA may be a critical factor in discriminating the degree of inflammation and cellular oxidation within a morpho-functional assessment protocol [47].
We must not forget that all this assessment must be immersed in structured, analytical, and biochemical tests, as well as measurements of adherence and quality of life, in order to be able to make a global and joint assessment of the patient. Therefore, morpho-functional assessment is a scheme that incorporates PhA and tries to provide a global vision of the diagnostic and prognostic values associated with different diseases [6, 94].
In the future, lines of research will be established that include PhA along with these morpho-functional variables in the design of projects on the diagnostic and prognostic value and evaluation of specific therapeutic intervention protocols.
Strength
PhA is a biological value that provides information on cellular health and has intrinsic prognostic value. The measurement technique is simple, inexpensive and can be systematically applied in different clinical settings, both inpatient and outpatient, for different pathologies.
The PhA is an objective parameter that can be used to establish cut-off points. It is sensitive and specific for diagnosis and determination of prognostic factors in health and disease. It is a parameter that is sensitive to changes over time and can therefore be useful in the evaluation of different treatments.
The vector representation adds value to the numerical value of the PhA in describing the degree of hydration and cell mass. It therefore better represents the pathophysiological mechanisms of cellular involvement and hydration. These have prognostic implications (Fig. 6).
In the future, the presentation of bioelectrical data in different forms could allow a simpler and more comprehensible analysis of Rz/Xc data in terms of comparing population levels, different pathologies, etc.
Limitations
The main limitation is related to measurement differences between BIA devices from different manufacturers. An international manufacturing standard is needed to facilitate direct comparison of results from different studies as well as the application of generally accepted reference values [32, 64]. Harmonization of technology, as well as cross-calibration of electrical resistors, should be a future goal. Harmonization of electrical resistors should be a mandatory future goal for impedance companies. In addition, only BIA devices that can detect phase-sensitive impedance variation should be used [32]. If there were a single approved device, for example, as there is for measuring glycosylated hemoglobin, we would be sure that, regardless of the brand of the device, it would accurately measure Rz, Xc and PhA, and we would have no problem obtaining universal results. It is necessary to consider the physiological and pathological conditions that influence the measurement (age, sex, BMI, race) [32]. Raw PhA is limited in that it does not take into account the determining factors. Although the raw value should always be assessed, the addition of the SPhA measure is an added value. The value of PhA increases with weight and BMI in both men and women, but not uniformly. This is because there is a direct relationship with FM rather than weight [95]. Adjustment of PhA should be made more to the increase in adipose tissue as FM than to the increase in weight or BMI.
There is a conceptual difficulty in understanding the concepts of reactance and resistance, particularly in their graphic representation, as the different scale on which Xo and Rz, are represented means that the hydration axis may appear to depend on reactance and nutrition or tissue status on resistance. Therefore, new models of graphical representation and vector analysis may be of interest in the future to facilitate understanding and to promote correlations with global prognostic factors.
The decrease due to the inflammatory component of hydration or hydration versus cell mass loss or cell damage cannot be distinguished from the numerical value of the PhA In this sense, morpho-functional assessment can provide correlating data with other morphological or functional techniques that focus the phase angle value in the appropriate direction.
In addition, there is a limitation on the use of the technique in pregnant women, children and subjects with pacemakers or patients in whom electrodes cannot be used such as skin lesions. Caution should be exercised in situations in which the water and electrolyte balance is altered. Intense physical activity, diet, alcohol and fluid intake prior to testing, dehydration or fluid retention, diuretic use and menstrual cycle may affect the results [96].
Conclusions
PhA is a raw parameter of cellular health, equivalent to “the electrocellgram®”. It has prognostic value in health and disease. As an isolated numerical value, provides global and non-specific information on cell mass and health, as well as congestion or inflammation.
The vectorial representation distributes the changes in cell mass and hydration in relation to reference population levels in ellipses of tolerance 50–75-95%. Its usefulness is demonstrated in the tetrapolar phase-sensitive single-frequency impedance in decubitus at 50 kHz. It is essential to know its determinants in order to make an objective assessment.
It is necessary to identify the characteristics of the different clinical scenarios, determining variables (age, race, sex, height, BMI) and physiological functions (ageing, physical activity) in order to make a phenotypic diagnosis at the individual level.
The use of the SPhA allows it to be adjusted for some of these determinants. It will probably be useful in the future to have standardised data on other factors such as type of pathology (cancer, critical, surgical).
Future lines of research on PhA should focus on diagnostic and prognostic values, sensitive and pathology-specific cut-off points, and quantification of clinically meaningful change in PhA with different health interventions. The main strength of PhA is its simplicity and ability to report on cellular health globally.
The main limitation is the complexity of the determinants that requires its adjustment to the individual phenotypic diagnosis of each patient, together with the need for a universally standardised measurement that reproduces global values comparable between different devices and measurement techniques.
PhA and vector impedance bioelectric measurements should be included in the morpho-functional assessment with other morphological techniques such as nutritional ultrasound and CT, and functional techniques such as dynamometry, test timed up and go, etc.
We would like to end this article with a sentence from the author H. S. Frazier, 1980: "Nature is probabilistic. Information is incomplete. Results are essential. Resources are limited. Decisions are inevitable".
Supplementary Information
Below is the link to the electronic supplementary material.
Acknowledgements
We would like to thank the Editors for inviting this review
Abbreviations
- BC
Body Composition
- BMI
Body Mass Index
- BCM
Body Cell Mass
- BIA
Bioelectrical Impedance Analysis
- BIVA
Bioelectrical Impedance Vector Analysis
- CKD
Chronic Kidney Disease
- COPD
Chronic obstructive pulmonary disease
- CT
Computed tomography
- DXA
Dual Energy X-Ray Absorptiometry
- ECW
Extracellular Water
- ESRD
End Stage Renal Disease
- FFM
Fat Free Mass
- FFMI
Fat Free Mass Index
- FM
Fat Mass
- GLIM
Criteria Global Leadership Initiative on Malnutrition Criteria
- HD
Hemodialysis
- HRQoL
Health Related Quality of Life
- IWC
Intracellular Water
- MRI
Magnetic Resonance Image
- NT-proBNP
N-terminal pro b-type natriuretic peptide
- PD
Peritoneal dialysis
- PhA
Phase Angle
- QoL
Quality of life
- SF-BIA
Single-Frequency Bioelectrical Impedance Analysis
- SPhA
Standardized phase angle
- TBW
Total Body Water
- Xc
Reactance
- Rz
Resistance
- Z
Impedance
Author contribution
All the Authors significantly contributed this manuscript and approved.its final version for submission.
Financial or non-financial interests
Nothing to declare.
Declarations
Ethical approval
Not required.
Informed consent
Not required.
Conflicts of Interest
The authors declare no conflicts of interest.
Footnotes
Diego Bellido and Cristina García-García contributed equally to this work and share the first authorship.
José Manuel García-Almeida is a senior author.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Diego Bellido, Email: diegobellido@gmail.com.
Cristina García-García, Email: cristina-garcia-garcia@hotmail.com.
Antonio Talluri, Email: tonytalluri@gmail.com.
Henry C. Lukaski, Email: henry.lukaski@und.edu
José Manuel García-Almeida, Email: jgarciaalmeida@gmail.com.
References
- 1.Lukaski HC. Requirements for clinical use of bioelectrical impedance analysis (BIA) Ann N Y Acad Sci. 1999;873:72–76. doi: 10.1111/j.1749-6632.1999.tb09451.x. [DOI] [PubMed] [Google Scholar]
- 2.Bellido D, Carreira J. Análisis por absorciometría de rayos X de doble energía y composición corporal. Nutr Clin Med. 2008;85–108.
- 3.García Almeida J, Bellido Guerrero D, Botella Romero F. Valoración Morfofuncional de la Desnutrición Relacionada con la Enfermedad. Madrid. España.: Editorial Médica Panamericana; 2022.
- 4.Lukaski HC, Talluri A. Phase angle as an index of physiological status: validating bioelectrical assessments of hydration and cell mass in health and disease. Rev Endocr Metab Disord. 2022. [DOI] [PubMed]
- 5.Garlini LM, Alves FD, Ceretta LB, et al. Phase angle and mortality: a systematic review. Eur J Clin Nutr. 2019;73:495–508. doi: 10.1038/s41430-018-0159-1. [DOI] [PubMed] [Google Scholar]
- 6.García Almeida JM, García García C, Vegas Aguilar IM, et al. Morphofunctional assessment of patient´s nutritional status: a global approach. Nutr Hosp. 2021;38:592–600. doi: 10.20960/nh.03378. [DOI] [PubMed] [Google Scholar]
- 7.Arab A, Karimi E, Vingrys K, et al. Is phase angle a valuable prognostic tool in cancer patients’ survival? A systematic review and meta-analysis of available literature. Clin Nutr. 2021;40:3182–3190. doi: 10.1016/j.clnu.2021.01.027. [DOI] [PubMed] [Google Scholar]
- 8.Pereira MME, Queiroz MDSC, de Albuquerque NMC, et al. The Prognostic Role of Phase Angle in Advanced Cancer Patients: A Systematic Review. Nutr Clin Pract. 2018;33:813–824. doi: 10.1002/ncp.10100. [DOI] [PubMed] [Google Scholar]
- 9.Morlino D, Cioffi I, Marra M, et al. Bioelectrical Phase Angle in Patients with Breast Cancer: A Systematic Review. Cancers (Basel) 2022;14:2002. doi: 10.3390/cancers14082002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Martins AD, Oliveira R, Brito JP, et al. Effect of exercise on phase angle in cancer patients: a systematic review. J Sports Med Phys Fitness. 2022;62:1255–1265. doi: 10.23736/S0022-4707.21.12727-6. [DOI] [PubMed] [Google Scholar]
- 11.Di Vincenzo O, Marra M, Di Gregorio A, et al. Bioelectrical impedance analysis (BIA) -derived phase angle in sarcopenia: A systematic review. Clin Nutr. 2021;40:3052–3061. doi: 10.1016/j.clnu.2020.10.048. [DOI] [PubMed] [Google Scholar]
- 12.Matthews L, Bates A, Wootton SA, et al. The use of bioelectrical impedance analysis to predict post-operative complications in adult patients having surgery for cancer: A systematic review. Clin Nutr. 2021;40:2914–2922. doi: 10.1016/j.clnu.2021.03.008. [DOI] [PubMed] [Google Scholar]
- 13.Madsen JM, Wichmann S, Bestle MH, et al. Bioimpedance as a measure of fluid status in critically ill patients: A systematic review. Acta Anaesthesiol Scand. 2021;65:1155–1167. doi: 10.1111/aas.13924. [DOI] [PubMed] [Google Scholar]
- 14.Mayne KJ, Shemilt R, Keane DF, et al. Bioimpedance Indices of Fluid Overload and Cardiorenal Outcomes in Heart Failure and Chronic Kidney Disease: a Systematic Review. J Card Fail. 2022;28:1628–1641. doi: 10.1016/j.cardfail.2022.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Di Vincenzo O, Marra M, Sacco AM, et al. Bioelectrical impedance (BIA)-derived phase angle in adults with obesity: A systematic review. Clin Nutr. 2021;40:5238–5248. doi: 10.1016/j.clnu.2021.07.035. [DOI] [PubMed] [Google Scholar]
- 16.Praget-Bracamontes S, González-Arellanes R, Aguilar-Salinas CA, et al. Phase Angle as a Potential Screening Tool in Adults with Metabolic Diseases in Clinical Practice: A Systematic Review. Int J Environ Res Public Health. 2023;20:1608. doi: 10.3390/ijerph20021608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Alves EAS, do Salazar Nascimento TC, Silvino VO, et al. Association between phase angle and adverse clinical outcomes in hospitalized patients with COVID-19: A systematic review. Nutr Clin Pract. 2022;37:1105–1116. doi: 10.1002/ncp.10901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rinaldi S, Gilliland J, O’Connor C, et al. Is phase angle an appropriate indicator of malnutrition in different disease states? A systematic review. Clin Nutr ESPEN. 2019;29:1–14. doi: 10.1016/j.clnesp.2018.10.010. [DOI] [PubMed] [Google Scholar]
- 19.Mattiello R, Amaral MA, Mundstock E, et al. Reference values for the phase angle of the electrical bioimpedance: Systematic review and meta-analysis involving more than 250,000 subjects. Clin Nutr. 2020;39:1411–1417. doi: 10.1016/j.clnu.2019.07.004. [DOI] [PubMed] [Google Scholar]
- 20.Lima J, Eckert I, Gonzalez MC, et al. Prognostic value of phase angle and bioelectrical impedance vector in critically ill patients: A systematic review and meta-analysis of observational studies. Clin Nutr. 2022;41:2801–2816. doi: 10.1016/j.clnu.2022.10.010. [DOI] [PubMed] [Google Scholar]
- 21.de Borba EL, Ceolin J, Ziegelmann PK, et al. Phase angle of bioimpedance at 50 kHz is associated with cardiovascular diseases: systematic review and meta-analysis. Eur J Clin Nutr. 2022;76:1366–1373. doi: 10.1038/s41430-022-01131-4. [DOI] [PubMed] [Google Scholar]
- 22.Cornejo-Pareja I, Vegas-Aguilar IM, García-Almeida JM, et al. Phase angle and standardized phase angle from bioelectrical impedance measurements as a prognostic factor for mortality at 90 days in patients with COVID-19: A longitudinal cohort study. Clin Nutr. 2021;S0261–5614(21):00091–101. doi: 10.1016/j.clnu.2021.02.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics [Internet]. 2010 [cited 2023 Feb 11];84:523–538. Available from: 10.1007/s11192-009-0146-3. [DOI] [PMC free article] [PubMed]
- 24.Piccoli A, Rossi B, Pillon L, et al. A new method for monitoring body fluid variation by bioimpedance analysis: the RXc graph. Kidney Int. 1994;46:534–539. doi: 10.1038/ki.1994.305. [DOI] [PubMed] [Google Scholar]
- 25.Lorenzo AD, Andreoli A. Segmental bioelectrical impedance analysis. Curr Opin Clin Nutr Metab Care. 2003;6:551–555. doi: 10.1097/00075197-200309000-00008. [DOI] [PubMed] [Google Scholar]
- 26.Jiménez A, Omaña W, Flores L, et al. Prediction of whole-body and segmental body composition by bioelectrical impedance in morbidly obese subjects. Obes Surg. 2012;22:587–593. doi: 10.1007/s11695-011-0570-3. [DOI] [PubMed] [Google Scholar]
- 27.Kim K, Jun M-H, Hong S, et al. Effect of body posture on segmental multifrequency bioimpedance variables. J Mech Med Biol [Internet]. 2022 [cited 2023 Feb 13];22:2240053. Available from: https://www.worldscientific.com/doi/full/10.1142/S021951942240053X.
- 28.Tabinor M, Elphick E, Dudson M, et al. Bioimpedance-defined overhydration predicts survival in end stage kidney failure (ESKF): systematic review and subgroup meta-analysis. Sci Rep. 2018;8:4441. doi: 10.1038/s41598-018-21226-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Mohamed M, Matthie J, Fan SL. Bioimpedance spectroscopy: Is a picture worth a thousand words? Semin Dial. 2022. 10.1111/sdi.13084. Epub ahead of print. [DOI] [PubMed]
- 30.Silva AM, Matias CN, Nunes CL, et al. Lack of agreement of in vivo raw bioimpedance measurements obtained from two single and multi-frequency bioelectrical impedance devices. Eur J Clin Nutr. 2019;73:1077–1083. doi: 10.1038/s41430-018-0355-z. [DOI] [PubMed] [Google Scholar]
- 31.Matthie JR. Bioimpedance measurements of human body composition: critical analysis and outlook. Expert Rev Med Devices. 2008;5:239–261. doi: 10.1586/17434440.5.2.239. [DOI] [PubMed] [Google Scholar]
- 32.Norman K, Stobäus N, Pirlich M, et al. Bioelectrical phase angle and impedance vector analysis–clinical relevance and applicability of impedance parameters. Clin Nutr. 2012;31:854–861. doi: 10.1016/j.clnu.2012.05.008. [DOI] [PubMed] [Google Scholar]
- 33.Slinde F, Bark A, Jansson J, et al. Bioelectrical impedance variation in healthy subjects during 12 h in the supine position. Clin Nutr. 2003;22:153–157. doi: 10.1054/clnu.2002.0616. [DOI] [PubMed] [Google Scholar]
- 34.Ellis KJ, Bell SJ, Chertow GM, et al. Bioelectrical impedance methods in clinical research: a follow-up to the NIH Technology Assessment Conference. Nutrition. 1999;15:874–880. doi: 10.1016/S0899-9007(99)00147-1. [DOI] [PubMed] [Google Scholar]
- 35.Gonzalez MC, Barbosa-Silva TG, Bielemann RM, et al. Phase angle and its determinants in healthy subjects: influence of body composition. Am J Clin Nutr. 2016;103:712–716. doi: 10.3945/ajcn.115.116772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Jiang N, Zhang J, Cheng S, et al. The Role of Standardized Phase Angle in the Assessment of Nutritional Status and Clinical Outcomes in Cancer Patients: A Systematic Review of the Literature. Nutrients. 2022;15:50. doi: 10.3390/nu15010050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Grundmann O, Yoon SL, Williams JJ. The value of bioelectrical impedance analysis and phase angle in the evaluation of malnutrition and quality of life in cancer patients–a comprehensive review. Eur J Clin Nutr. 2015;69:1290–1297. doi: 10.1038/ejcn.2015.126. [DOI] [PubMed] [Google Scholar]
- 38.Amano K, Bruera E, Hui D. Diagnostic and prognostic utility of phase angle in patients with cancer. Rev Endocr Metab Disord. 2022. 10.1007/s11154-022-09776-z. Epub ahead of print. [DOI] [PubMed]
- 39.Roccamatisi L, Gianotti L, Paiella S, et al. Preoperative standardized phase angle at bioimpedance vector analysis predicts the outbreak of antimicrobial-resistant infections after major abdominal oncologic surgery: A prospective trial. Nutrition [Internet]. 2021 [cited 2023 Feb 13];86:111184. Available from: https://www.sciencedirect.com/science/article/pii/S0899900721000460. [DOI] [PubMed]
- 40.Fiorindi C, Cuffaro F, Piemonte G, et al. Effect of long-lasting nutritional prehabilitation on postoperative outcome in elective surgery for IBD. Clinical Nutrition [Internet]. 2021 [cited 2023 Feb 13];40:928–935. Available from: https://www.clinicalnutritionjournal.com/article/S0261-5614(20)30331-9/fulltext. [DOI] [PubMed]
- 41.Casirati A, Crotti S, Raffaele A, et al. The use of phase angle in patients with digestive and liver diseases. Rev Endocr Metab Disord. 2023. 10.1007/s11154-023-09785-6. Epub ahead of print. [DOI] [PubMed]
- 42.De Benedetto F, Marinari S, De Blasio F. Phase angle in assessment and monitoring treatment of individuals with respiratory disease. Rev Endocr Metab Disord. 2023. 10.1007/s11154-023-09786-5. Epub ahead of print. [DOI] [PubMed]
- 43.Cornejo-Pareja I, Vegas-Aguilar IM, Lukaski H, et al. Overhydration Assessed Using Bioelectrical Impedance Vector Analysis Adversely Affects 90-Day Clinical Outcome among SARS-CoV2 Patients: A New Approach. Nutrients. 2022;14:2726. doi: 10.3390/nu14132726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Cancello R, Brunani A, Brenna E, et al. Phase angle (PhA) in overweight and obesity: evidence of applicability from diagnosis to weight changes in obesity treatment. Rev Endocr Metab Disord. 2022;1–14. 10.1007/s11154-022-09774-1. Epub ahead of print. [DOI] [PMC free article] [PubMed]
- 45.Kyle UG, Bosaeus I, De Lorenzo AD, et al. Bioelectrical impedance analysis–part I: review of principles and methods. Clin Nutr. 2004;23:1226–1243. doi: 10.1016/j.clnu.2004.06.004. [DOI] [PubMed] [Google Scholar]
- 46.da Silva BR, Orsso CE, Gonzalez MC, et al. Phase angle and cellular health: inflammation and oxidative damage. Rev Endocr Metab Disord. 2022;1–20. 10.1007/s11154-022-09775-0. Epub ahead of print. [DOI] [PMC free article] [PubMed]
- 47.Polak-Szczybyło E, Stępień AE, Zielińska M, et al. Hashimoto Thyroiditis, but Not Hypothyroidism Due to Other Causes, Is Associated with Lower Phase Angle Score in Adult Women: A Pilot Cross-Sectional Study. J Clin Med. 2022;12:56. doi: 10.3390/jcm12010056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Liang B, Li R, Bai J-Y, et al. Bioimpedance Vector Analysis for Heart Failure: Should We Put It on the Agenda? Frontiers in Cardiovascular Medicine [Internet]. 2021 [cited 2023 Feb 13];8. Available from: https://www.frontiersin.org/articles/10.3389/fcvm.2021.744243. [DOI] [PMC free article] [PubMed]
- 49.Piccoli A. Bioelectric impedance measurement for fluid status assessment. Contrib Nephrol. 2010;164:143–152. doi: 10.1159/000313727. [DOI] [PubMed] [Google Scholar]
- 50.Scicchitano P, Massari F. The role of bioelectrical phase angle in patients with heart failure. Rev Endocr Metab Disord. 2022;1–13. 10.1007/s11154-022-09757-2. Epub ahead of print. [DOI] [PMC free article] [PubMed]
- 51.Beaubien-Souligny W, Rola P, Haycock K, et al. Quantifying systemic congestion with Point-Of-Care ultrasound: development of the venous excess ultrasound grading system. Ultrasound J. 2020;12:16. doi: 10.1186/s13089-020-00163-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Wang Y, Gu Z. Effect of bioimpedance-defined overhydration parameters on mortality and cardiovascular events in patients undergoing dialysis: a systematic review and meta-analysis. J Int Med Res. 2021;49:3000605211031063. doi: 10.1177/03000605211031063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Pillon L, Piccoli A, Lowrie EG, et al. Vector length as a proxy for the adequacy of ultrafiltration in hemodialysis. Kidney Int. 2004;66:1266–1271. doi: 10.1111/j.1523-1755.2004.00881.x. [DOI] [PubMed] [Google Scholar]
- 54.Kushner RF, de Vries PM, Gudivaka R. Use of bioelectrical impedance analysis measurements in the clinical management of patients undergoing dialysis. Am J Clin Nutr. 1996;64:503S–509S. doi: 10.1093/ajcn/64.3.503S. [DOI] [PubMed] [Google Scholar]
- 55.Covic A, Ciumanghel A-I, Siriopol D, et al. Value of bioimpedance analysis estimated “dry weight” in maintenance dialysis patients: a systematic review and meta-analysis. Int Urol Nephrol. 2017;49:2231–2245. doi: 10.1007/s11255-017-1698-4. [DOI] [PubMed] [Google Scholar]
- 56.Lukaski HC, Vega Diaz N, Talluri A, et al. Classification of Hydration in Clinical Conditions: Indirect and Direct Approaches Using Bioimpedance. Nutrients. 2019;11:809. doi: 10.3390/nu11040809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.van der Sande FM, van de Wal-Visscher ER, Stuard S, et al. Using Bioimpedance Spectroscopy to Assess Volume Status in Dialysis Patients. Blood Purif. 2020;49:178–184. doi: 10.1159/000504079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Piccoli A, Pastori G, Guizzo M, et al. Equivalence of information from single versus multiple frequency bioimpedance vector analysis in hemodialysis. Kidney Int. 2005;67:301–313. doi: 10.1111/j.1523-1755.2005.00083.x. [DOI] [PubMed] [Google Scholar]
- 59.Di Iorio BR, Scalfi L, Terracciano V, et al. A systematic evaluation of bioelectrical impedance measurement after hemodialysis session. Kidney Int. 2004;65:2435–2440. doi: 10.1111/j.1523-1755.2004.00660.x. [DOI] [PubMed] [Google Scholar]
- 60.Piccoli A. Identification of operational clues to dry weight prescription in hemodialysis using bioimpedance vector analysis. The Italian Hemodialysis-Bioelectrical Impedance Analysis (HD-BIA) Study Group. Kidney Int. 1998;53:1036–1043. doi: 10.1111/j.1523-1755.1998.00843.x. [DOI] [PubMed] [Google Scholar]
- 61.Bansal N, Zelnick LR, Himmelfarb J, et al. Bioelectrical Impedance Analysis Measures and Clinical Outcomes in CKD. Am J Kidney Dis. 2018;72:662–672. doi: 10.1053/j.ajkd.2018.03.030. [DOI] [PubMed] [Google Scholar]
- 62.Maggiore Q, Nigrelli S, Ciccarelli C, et al. Nutritional and prognostic correlates of bioimpedance indexes in hemodialysis patients. Kidney Int. 1996;50:2103–2108. doi: 10.1038/ki.1996.535. [DOI] [PubMed] [Google Scholar]
- 63.Bellizzi V, Scalfi L, Terracciano V, et al. Early changes in bioelectrical estimates of body composition in chronic kidney disease. J Am Soc Nephrol. 2006;17:1481–1487. doi: 10.1681/ASN.2005070756. [DOI] [PubMed] [Google Scholar]
- 64.Lukaski HC, Kyle UG, Kondrup J. Assessment of adult malnutrition and prognosis with bioelectrical impedance analysis: phase angle and impedance ratio. Curr Opin Clin Nutr Metab Care [Internet]. 2017 [cited 2023 Feb 22];20:330–339. Available from: 10.1097/MCO.0000000000000387. [DOI] [PubMed]
- 65.Piccoli A, Codognotto M, Piasentin P, et al. Combined evaluation of nutrition and hydration in dialysis patients with bioelectrical impedance vector analysis (BIVA) Clin Nutr. 2014;33:673–677. doi: 10.1016/j.clnu.2013.08.007. [DOI] [PubMed] [Google Scholar]
- 66.Lukaski HC, Kyle UG, Kondrup J. Assessment of adult malnutrition and prognosis with bioelectrical impedance analysis: phase angle and impedance ratio. Curr Opin Clin Nutr Metab Care. 2017;20:330–339. doi: 10.1097/MCO.0000000000000387. [DOI] [PubMed] [Google Scholar]
- 67.Kotanko P. The promise of bioimpedance for volume management in American dialysis patients: An unfulfilled opportunity. Semin Dial. 2019;32:223–224. doi: 10.1111/sdi.12790. [DOI] [PubMed] [Google Scholar]
- 68.Lukaski HC. Evolution of bioimpedance: a circuitous journey from estimation of physiological function to assessment of body composition and a return to clinical research. Eur J Clin Nutr. 2013;67(Suppl 1):S2–9. doi: 10.1038/ejcn.2012.149. [DOI] [PubMed] [Google Scholar]
- 69.Bosy-Westphal A, Danielzik S, Dörhöfer R-P, et al. Phase angle from bioelectrical impedance analysis: population reference values by age, sex, and body mass index. JPEN J Parenter Enteral Nutr. 2006;30:309–316. doi: 10.1177/0148607106030004309. [DOI] [PubMed] [Google Scholar]
- 70.Talluri A, Liedtke R, Mohamed EI, et al. The application of body cell massindex for studying muscle mass changes in health and diseaseconditions. Acta Diabetol [Internet]. 2003 [cited 2023 Feb 22];40:s286–s289. Available from: 10.1007/s00592-003-0088-9. [DOI] [PubMed]
- 71.Dittmar M, Reber H. Validation of different bioimpedance analyzers for predicting cell mass against whole-body counting of potassium (40K) as a reference method. Am J Hum Biol. 2004;16:697–703. doi: 10.1002/ajhb.20078. [DOI] [PubMed] [Google Scholar]
- 72.Cereda E, Caraccia M, Klersy C, et al. Validation of a new prognostic body composition parameter in cancer patients. Clin Nutr. 2021;40:615–623. doi: 10.1016/j.clnu.2020.06.011. [DOI] [PubMed] [Google Scholar]
- 73.Basile C, Della-Morte D, Cacciatore F, et al. Phase angle as bioelectrical marker to identify elderly patients at risk of sarcopenia. Exp Gerontol. 2014;58:43–46. doi: 10.1016/j.exger.2014.07.009. [DOI] [PubMed] [Google Scholar]
- 74.de Moraes Santana N, Pinho CPS, da Silva CP, et al. Phase Angle as a Sarcopenia Marker in Hospitalized Elderly Patients. Nutr Clin Pract. 2018;33:232–237. doi: 10.1002/ncp.10016. [DOI] [PubMed] [Google Scholar]
- 75.Campa F, Colognesi LA, Moro T, et al. Effect of resistance training on bioelectrical phase angle in older adults: a systematic review with Meta-analysis of randomized controlled trials. Rev Endocr Metab Disord. 2022. 10.1007/s11154-022-09747-4. Epub ahead of print. [DOI] [PMC free article] [PubMed]
- 76.Richards AM. New biomarkers in heart failure: applications in diagnosis, prognosis and guidance of therapy. Rev Esp Cardiol. 2010;63:635–639. doi: 10.1016/s1885-5857(10)70137-7. [DOI] [PubMed] [Google Scholar]
- 77.Picó C, Serra F, Rodríguez AM, et al. Biomarkers of Nutrition and Health: New Tools for New Approaches. Nutrients. 2019;11:1092. doi: 10.3390/nu11051092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Marshall WJ, Bangert SK. Clinical Biochemistry: Metabolic and Clinical Aspects. London: Livingstone/Elsevier; 2008.
- 79.Eusebi P. Diagnostic accuracy measures. Cerebrovasc Dis. 2013;36:267–272. doi: 10.1159/000353863. [DOI] [PubMed] [Google Scholar]
- 80.Richardson WS, Wilson MC, Guyatt GH, et al. Users’ guides to the medical literature: XV. How to use an article about disease probability for differential diagnosis. Evidence-Based Medicine Working Group. JAMA. 1999;281:1214–1219. [DOI] [PubMed]
- 81.Lijmer JG, Mol BW, Heisterkamp S, et al. Empirical evidence of design-related bias in studies of diagnostic tests. JAMA. 1999;282:1061–1066. doi: 10.1001/jama.282.11.1061. [DOI] [PubMed] [Google Scholar]
- 82.Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64:383–394. doi: 10.1016/j.jclinepi.2010.04.026. [DOI] [PubMed] [Google Scholar]
- 83.Kirmayr M, Quilodrán C, Valente B, et al. The GRADE approach, Part 1: how to assess the certainty of the evidence. Medwave. 2021;21:e8109. doi: 10.5867/medwave.2021.02.8109. [DOI] [PubMed] [Google Scholar]
- 84.Sanabria AJ, Rigau D, Rotaeche R, et al. Sistema GRADE: metodología para la realización de recomendaciones para la práctica clínica. Aten Primaria [Internet]. 2015 [cited 2023 Mar 2];47:48–55. Available from: https://www.elsevier.es/es-revista-atencion-primaria-27-articulo-sistema-grade-metodologia-realizacion-recomendaciones-S0212656714000493. [DOI] [PMC free article] [PubMed]
- 85.Fernández-Medina B, Vegas-Aguilar I, García-Almeida JM, et al. Morfo-functional nutritional status in patients with gastroenteropancreatic neuroendocrine tumors (GEPNET) Endocrinol Diabetes Nutr (Engl Ed) 2022;69:466–475. doi: 10.1016/j.endien.2022.07.007. [DOI] [PubMed] [Google Scholar]
- 86.Fernández-Jiménez R, Dalla-Rovere L, García-Olivares M, et al. Phase Angle and Handgrip Strength as a Predictor of Disease-Related Malnutrition in Admitted Patients: 12-Month Mortality. Nutrients. 2022;14:1851. doi: 10.3390/nu14091851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Vegas-Aguilar IM, Guirado-Peláez P, Fernández-Jiménez R, et al. Exploratory Assessment of Nutritional Evaluation Tools as Predictors of Complications and Sarcopenia in Patients with Colorectal Cancer. Cancers [Internet]. 2023 [cited 2023 Feb 16];15:847. Available from: https://www.mdpi.com/2072-6694/15/3/847. [DOI] [PMC free article] [PubMed]
- 88.García-Almeida JM, García-García C, Vegas-Aguilar IM, et al. Nutritional ultrasound®: Conceptualisation, technical considerations and standardisation. Endocrinología, Diabetes y Nutrición [Internet]. 2022 [cited 2023 Feb 16]; Available from: https://www.sciencedirect.com/science/article/pii/S2530016422001471. [DOI] [PubMed]
- 89.García-García C, Vegas-Aguilar IM, Rioja-Vázquez R, et al. Rectus Femoris Muscle and Phase Angle as Prognostic Factor for 12-Month Mortality in a Longitudinal Cohort of Patients with Cancer (AnyVida Trial) Nutrients. 2023;15:522. doi: 10.3390/nu15030522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Primo D, Izaola O, Gómez JJL, et al. Correlation of the Phase Angle with Muscle Ultrasound and Quality of Life in Obese Females. Dis Markers. 2022;2022:7165126. doi: 10.1155/2022/7165126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Cornejo-Pareja I, Soler-Beunza AG, Vegas-Aguilar IM, et al. Predictors of Sarcopenia in Outpatients with Post-Critical SARS-CoV2 Disease. Nutritional Ultrasound of Rectus Femoris Muscle, a Potential Tool. Nutrients. 2022;14:4988. doi: 10.3390/nu14234988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Sánchez-Torralvo FJ, Porras N, Ruiz-García I, et al. Usefulness of Muscle Ultrasonography in the Nutritional Assessment of Adult Patients with Cystic Fibrosis. Nutrients [Internet]. 2022 [cited 2022 Aug 23];14:3377. Available from: https://www.mdpi.com/2072-6643/14/16/3377. [DOI] [PMC free article] [PubMed]
- 93.López-Gómez JJ, Benito-Sendín Plaar K, Izaola-Jauregui O, et al. Muscular Ultrasonography in Morphofunctional Assessment of Patients with Oncological Pathology at Risk of Malnutrition. Nutrients. 2022;14:1573. doi: 10.3390/nu14081573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.García-Almeida JM, García-García C, Ballesteros-Pomar MD, et al. Expert Consensus on Morphofunctional Assessment in Disease-Related Malnutrition. Grade Review and Delphi Study. Nutrients [Internet]. 2023;15:612. 10.3390/nu15030612. [DOI] [PMC free article] [PubMed]
- 95.Di Vincenzo O, Marra M, Antognozzi V, et al. Comparison of bioelectrical impedance analysis-derived phase angle in individuals with different weight status. Nutrition. 2022;108:111960. doi: 10.1016/j.nut.2022.111960. [DOI] [PubMed] [Google Scholar]
- 96.Mialich M, Sicchieri J, Júnior A a. J. Analysis of Body Composition: A Critical Review of the Use of Bioelectrical Impedance Analysis [Internet]. 2014 [cited 2023 Feb 3]. Available from: https://www.semanticscholar.org/paper/Analysis-of-Body-Composition%3A-A-Critical-Review-of-Mialich-Sicchieri/06ed3208eebcfa9848d979c4715a587ddaedc60a.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.