

Abstract
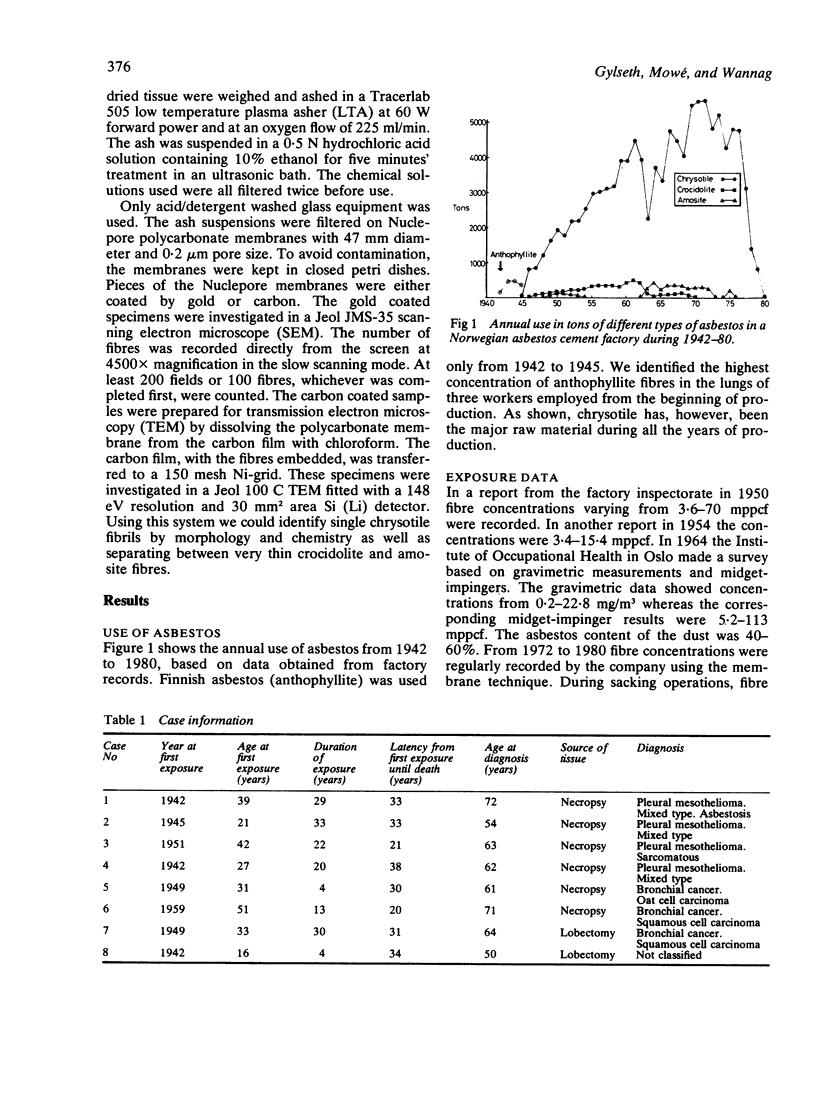
The predominant asbestos fibre type used in the production of asbestos cement is chrysotile. The use of asbestos in relation to fibre type in a Norwegian asbestos cement plant during 1942-80 was 91.7% chrysotile, 3.1% amosite, 4.1% crocidolite, and 1.1% anthophyllite respectively. Electron microscopy and x ray microanalysis of lung tissue samples of asbestos cement workers who had died of malignant pleural mesothelioma or bronchogenic carcinoma showed a completely inverse ratio with regard to fibre type. The percentage of chrysotile asbestos in lung tissue varied between 0% and 9% whereas the corresponding numbers for the amphiboles were 76% and 99%. These differences are discussed with respect to the behaviour of different fibre types in the human body and to the occurrence of malignant mesothelioma in this asbestos cement factory.
Full text
PDF

Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Clemmesen J., Hjalgrim-Jensen S. Cancer incidence among 5686 asbestos-cement workers followed from 1943 through 1976. Ecotoxicol Environ Saf. 1981 Mar;5(1):15–23. doi: 10.1016/0147-6513(81)90042-7. [DOI] [PubMed] [Google Scholar]
- Dement J. M., Harris R. L., Jr, Symons M. J., Shy C. Estimates of dose-response for respiratory cancer among chrysotile asbestos textile workers. Ann Occup Hyg. 1982;26(1-4):869–887. [PubMed] [Google Scholar]
- Finkelstein M. M. Asbestosis in long-term employees of an Ontario asbestos-cement factory. Am Rev Respir Dis. 1982 May;125(5):496–501. doi: 10.1164/arrd.1982.125.5.496. [DOI] [PubMed] [Google Scholar]
- Lacquet L. M., van der Linden L., Lepoutre J. Roentgenographic lung changes, asbestosis and mortality in a Belgian asbestos-cement factory. IARC Sci Publ. 1980;(30):783–793. [PubMed] [Google Scholar]
- McDonald A. D., McDonald J. C., Pooley F. D. Mineral fibre content of lung in mesothelial tumours in North America. Ann Occup Hyg. 1982;26(1-4):417–422. [PubMed] [Google Scholar]
- McDonald J. C., McDonald A. D. Epidemiology of mesothelioma from estimated incidence. Prev Med. 1977 Sep;6(3):426–442. doi: 10.1016/0091-7435(77)90025-1. [DOI] [PubMed] [Google Scholar]
- Newhouse M. L., Berry G., Skidmore J. W. A mortality study of workers manufacturing friction materials with chrysotile asbestos. Ann Occup Hyg. 1982;26(1-4):899–909. [PubMed] [Google Scholar]
- Thomas H. F., Benjamin I. T., Elwood P. C., Sweetnam P. M. Further follow-up study of workers from an asbestos cement factory. Br J Ind Med. 1982 Aug;39(3):273–276. doi: 10.1136/oem.39.3.273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weill H., Hughes J., Waggenspack C. Influence of dose and fiber type on respiratory malignancy risk in asbestos cement manufacturing. Am Rev Respir Dis. 1979 Aug;120(2):345–354. doi: 10.1164/arrd.1979.120.2.345. [DOI] [PubMed] [Google Scholar]
- Weiss W. Mortality of a cohort exposed to chrysotile asbestos. J Occup Med. 1977 Nov;19(11):737–740. [PubMed] [Google Scholar]