

Abstract
The high level of uncertainty brought about by the COVID‐19 pandemic has affected the general population's well‐being and capacity for adaptive responding. Studies indicate that flexibility, defined as the ability to choose and employ a variety of emotional, cognitive and behavioural strategies in accordance with changing contextual demands, may significantly contribute to adaptive responding to long‐term stressors such as COVID‐19. In the current study, we aimed to investigate which facets of flexibility predict different latent profiles of adaptive responding to the COVID‐19 pandemic in Israel and Germany. A total of 2330 Israelis and 743 Germans completed online questionnaires measuring cognitive and coping regulatory flexibility and cognitive, emotional and behavioural responding to the COVID‐19 pandemic. Analyses revealed three distinct response profiles in each country (high, medium and low). These profiles differed in both anxiety and depression symptoms with the non‐adaptive response group experiencing clinically relevant symptoms both in Israel and Germany. Additionally, cognitive flexibility and coping flexibility emerged as significant predictors of response profiles in both countries. Training cognitive and coping flexibility may thus help individuals respond more adaptively to psychosocial stressors such as COVID‐19. Such training could be selectively administered to less flexible subpopulations as well as adapted to the specific population characteristics.
Keywords: anxiety, depression, flexibility, response, stress exposure
What is known about this topic?
The worldwide spread of the Coronavirus disease affected the general population's well‐being and capacity for adaptive responding.
Subgroups of individuals tend to develop persistent mental health problems following stress exposure.
Recently, flexibility was suggested as a critical contributor to adaptive responding to stress.
What this paper adds?
Three distinct response profiles (low‐, medium‐ and highly adaptive responding) that differed in anxiety and depression symptoms were found both in Germany and in Israel.
Cognitive flexibility and coping regulatory flexibility emerged as significant predictors of adaptive responding in both countries.
Results highlight that training cognitive and coping regulatory flexibility may help individuals respond better to psychosocial stressors.
1. INTRODUCTION
The worldwide spread of the Coronavirus disease (COVID‐19) has drastically changed everyday lives across the globe (Goldfarb, 2020). These changes and the high level of uncertainty that came with them have affected the general population's well‐being and ability to cope with daily challenges (Paredes et al., 2021). As a result, a significant rate of the general population has been experiencing mental health problems (Pfefferbaum & North, 2020). Meta‐analyses indicate that 33% has experienced anxiety, whereas 30% has experienced depression (Salari et al., 2020; Wang et al., 2020). Since these estimates are based on self‐report data rather than confirmed diagnoses, they cannot be used as indicators of disease prevalence. Nevertheless, they illustrate a significant momentaneous impact of COVID‐19 on mental health, as also evident in high rates of sleep problems (34%) and general stress (36%) (Krishnamoorthy et al., 2020). Critically, these rates mostly come from cross‐sectional studies investigating acute responses in the early stages of the pandemic (Salari et al., 2020). This is important to consider since previous research examining longitudinal trajectories of mental health after stressful life events suggest that the majority of the population will adjust to the psychosocial stress arising from COVID‐19 over time (Chen & Bonanno, 2020). As such, a fairly stable trajectory of mental health will likely be the most common response seen in the general population (Bonanno, 2004). This assumption is broadly consistent with a meta‐analysis comparing mental health before and during the pandemic (Robinson et al., 2021). Notwithstanding, smaller subgroups will likely develop persistent mental health problems, making the identification of key predictors of early adaptive responding to COVID‐19 an important agenda for current research.
Studies examining successful adjustment to stressful or traumatic life events indicate that flexibility may be a critical contributor to adaptive responding to COVID‐19 (Chen & Bonanno, 2020). Broadly speaking, flexibility refers to the ability to employ a variety of emotional, cognitive, and behavioural strategies and to adapt them according to changing contextual demands (Cañas et al., 2006; Ionescu, 2012; Keith et al., 2015). It enables individuals to shift between discrepant tasks or demands and adapt to different challenges (Koesten et al., 2009; Leung & Zakzanis, 2014). By emphasising that successful responding can only be achieved if cognitive, behavioural and emotional strategies closely match situational demands, the flexibility concept opposes the notion that some strategies are more beneficial than others, rather suggesting that each strategy can have beneficial effects if used in the right situation (Burton & Bonanno, 2016). For example, positive reframing, which is commonly believed to be a beneficial emotion regulation strategy, can have adverse effects if applied in an inflexible manner since this can lead to avoidance. The concept of flexibility is thus particularly relevant for responding to multidimensional stressors, which bring about various challenging situations with very diverse characteristics. Such stressors naturally require a repertoire of different strategies that are rapidly deployed in accordance with situational characteristics as well as the ability to flexibly switch between different strategies. Given that the COVID‐19 pandemic constitutes an unprecedented multidimensional long‐term stressor of the 21st century (Goldfarb, 2020; Gruber et al., 2021), it provides ideal conditions to evaluate how flexibility may tie in with adaptive responding.
Flexibility can emerge on all levels of intrapsychic processes and has thus been studied in the context of various domains, giving rise to partially overlapping constructs. Two of these constructs that have received substantial attention in the literature are cognitive and regulatory flexibility (Haim‐Nachum & Levy‐Gigi, 2021). Cognitive flexibility is the ability to recognise multiple possible responses to a situation and to make an adaptive choice (Martin & Rubin, 1995). It is thus reflected in a wide repertoire of problem‐solving strategies, deployed according to situational demands (Kraft et al., 2020). Regulatory flexibility refers to an individual's ability to modulate emotional experience ‐ specifically to up‐ and downregulate emotional states ‐ using a repertoire of different strategies matching situational demands. Critically, both cognitive and regulatory flexibility have been linked to reduced psychopathology after trauma (Bonanno et al., 2011; Keith et al., 2015; Levy‐Gigi et al., 2016; Levy‐Gigi et al., 2020), indicating that high flexibility may buffer the potentially deleterious effects of stressful events. A recent study has further shed light on the incremental validity of cognitive flexibility and regulatory flexibility ‐ assessed in the context of emotion expression and coping with trauma ‐ in predicting current and lifetime PTSD symptoms (Haim‐Nachum & Levy‐Gigi, 2021). Although all flexibility measures were significantly correlated with PTSD symptoms, cognitive flexibility emerged as the only predictor of current PTSD symptoms with incremental validity. These results indicate that ‐ despite significant overlap—cognitive and regulatory flexibility seem to encompass unique aspects that are linked to PTSD symptoms.
Although previous findings imply a key role of flexibility in successful coping with trauma, which is informative for identifying potential predictors of adaptive responding to COVID‐19‐related stress, only a few studies have examined how flexibility may influence responses to the COVID‐19 pandemic. First studies investigating the impact of coping flexibility (i.e., trauma‐related regulatory flexibility; Cheng et al., 2021; Jordan et al., 2022; Shigeto et al., 2021) and cognitive flexibility (Kalia et al., 2020; Seiter & Curran, 2021) on responses to the COVID‐19 pandemic revealed that low flexibility is linked to more negative responses. Moreover, two studies found an association between emotion regulatory flexibility and superior mental health in Italian healthcare workers (Lenzo et al., 2021) and elderly outpatients (Sardella et al., 2021) during COVID‐19. Critically, no study to date has investigated the impact of multiple flexibility constructs (i.e. coping flexibility and cognitive flexibility) on response to COVID‐19. Such an investigation seems warranted since multifaceted flexibility is likely required for adaptive responding to the COVID‐19 pandemic as a multidimensional long‐term stressor. Alternatively, high flexibility in one facet might be more important for responding to the pandemic than flexibility in others (Haim‐Nachum & Levy‐Gigi, 2021). Moreover, the relevance of these flexibility facets may be modulated by the level of pre‐COVID‐19 stressor exposure. That is, contexts with high levels of stress or trauma exposure may increase requirements for flexible self‐regulation.
Similarly, it is important to assess responses to COVID‐19 on a cognitive, emotional and behavioural level. These levels are regarded as interconnected and interactive processes that influence each other (Russo‐Netzer & Ameli, 2021). Yet, COVID‐19‐related effects may manifest disproportionally on some level(s) and not on others. Hence, it is informative to examine responses to COVID‐19 in terms of profiles (differentiating between the cognitive, emotional and behavioural domains) rather than examining the overall response collapsed across these domains (Paudel, 2020; Pedrosa et al., 2020).
Previous studies examining response profiles during the COVID‐19 pandemic revealed the existence of mostly unaffected, moderately affected, and highly affected profiles (Fernández et al., 2020; Hynes et al., 2021; Li et al., 2021). A recent meta‐analysis found that approximately 65.7%, 25% and 17.9% of individuals fall into these categories (Kunzler et al., in press). However, to the best of our knowledge, no previous study has examined response profiles in terms of cognitive, emotional and behavioural responses.
To examine the relevance of multifaceted flexibility for responding to COVID‐19, we conducted a study assessing different flexibility constructs and responses to COVID‐19 in the general population. Responses to COVID‐19 were assessed on a cognitive, emotional and behavioural level, allowing us to examine response profiles, rather than an aggregated response score. To investigate the extent to which result patterns generalise across contexts with high and low society‐level pre‐COVID‐19 stress exposure, we collected subsamples in Israel and Germany. Israel is a country in which civilians are often exposed to interpersonal emergency situations, such as war or terror attacks (Besser & Neria, 2012). As a result, living conditions in Israel are considered to impose continuous traumatic stress (Greene et al., 2018; Pat‐Horenczyk & Schiff, 2019), while in Germany, there is no frequent exposure to such stressors (Rutter, 1987). Comparing subsamples from these countries, thus gave us the unique opportunity to assess the generalizability of result patterns across different levels of pre‐COVID‐19 stress exposure.
In line with previous research, we hypothesized that three different profiles reflecting low, moderately and highly adaptive responding to COVID‐19 would emerge. Examination of differences between these profiles in emotional, cognitive and behavioural subdomains was exploratory, though limited evidence indicates that the cognitive subdomain may be particularly affected in individuals in low‐response profiles (Torrente et al., 2022). We further expected to find significant differences between the profiles in depression and anxiety, corresponding to the level of adaptive responding. Based on the findings of Haim‐Nachum and Levy‐Gigi (2021), we further hypothesized that cognitive and coping flexibility would significantly predict profile membership, such that high levels of flexibility would be associated with highly‐adaptive responding group membership.
2. MATERIALS AND METHODS
During the spring and summer of 2020, participants from the general population were asked to complete an online study comprising measures of coping flexibility (Bonanno et al., 2011), cognitive flexibility (Martin & Rubin, 1995), and emotion regulatory flexibility 1 (Burton & Bonanno, 2016). Adaptive responding to COVID‐19 was assessed on a cognitive, emotional and behavioural level. Based on these data, we conducted latent profile analyses to investigate the existence of discernable patterns of response to the pandemic and their association with anxiety and depression symptoms. We tested the cross‐national similarity of the final class solutions following steps proposed by Morin et al. (2016). Finally, we conducted logistic regression analyses to investigate which facets of flexibility uniquely predict different response profiles while controlling for socio‐demographic characteristics and known covariates (Schäfer et al., 2020; Wang et al., 2020; Xu et al., 2020).
2.1. Participants
A total of 2330 Israelis and 743 Germans participated in this study. Participants were recruited from the general population via online platforms and (social) media advertisements. Recruitment took place from 12 April until 5 May, 2020, in Israel and from 8 May until 1 July, 2020, in Germany. Citizens of both countries had experienced the first waves of pandemic spread, related restrictions and intermittent lockdowns at this point of the pandemic (for details, see Appendix S1). Participants were informed of the study objectives, prompted for informed consent and confirmation that they were at least 18 years old and fluent in Hebrew or German speakers, respectively. Thereafter, they completed a survey comprising questions on demographic variables (age, gender and income) and instruments measuring different flexibility constructs, responses to COVID‐19, depression, anxiety, lifetime trauma exposure and perceived social support. Upon completion, participants had the opportunity to enter a raffle. All study procedures were approved by the local ethics committees.
2.2. Measures
2.2.1. Assessment of flexibility
Coping flexibility was assessed using the Perceived Ability to Cope with Trauma (PACT) scale (Bonanno et al., 2011). The PACT measures flexibility in engaging in forward‐focused (i.e., being able to focus on the present, sample item: ‘Following a potentially traumatic event, I would be able to stay focused on my current goals and plans’) and trauma‐focused (i.e., being able to reflect on the traumatic experience, sample item: ‘Following a potentially traumatic event, I would be able to reflect on the meaning of the event’) coping. It comprises 20 items that are rated on a 7‐point scale (forward focus: α = 0.86, α = 0.77; trauma focus: α = 0.83, α = 0.71; in the Israeli and German samples, respectively). In line with Bonanno et al. (2011), the PACT score was calculated as the difference between general sum and polarity (i.e., the absolute difference between the trauma‐focused score and the forward‐focused score; for details, see Bonanno et al., 2011).
Cognitive flexibility was measured using the Cognitive Flexibility Scale (CFS) developed by Martin and Rubin (1995). The scale comprises 12 items that are rated on a 6‐point scale (Israel: α = 0.81, Germany: α = 0.86). Sample item: ‘In any given situation, I am able to act appropriately’.
2.2.2. Assessment of response to the COVID‐19 pandemic
Given the lack of tools assessing responding to the COVID‐19 pandemic at the time of data collection, we developed a new scale. In developing the scale, we first defined specific facets of responding (i.e., emotional, cognitive, and behavioural). In a second step, an item pool was developed covering each facet. Of this initial item pool, four items for behavioural responding (sample item: ‘I am following the news constantly in order to stay up to date with any developments all the time.’), three items for cognitive responding (sample item: ‘As a society, we won't be able to deal with an emergency reality for a prolonged period of time.’) and three items for emotional responding (sample item: ‘I feel stressed more than usually since the outbreak of COVID‐19’.) were selected for the final scale in a process of exploratory factor analysis in half of the Israeli sample and half of the German sample, followed by a confirmatory factor analysis (CFA) in the other half of each sample, respectively. Both CFAs demonstrated good fit indices [χ2(32) = 63.79, p < 0.001, CFI = 0.97, NFI = 0.96, RMSEA = 0.05; χ2(32) = 65.83, p < 0.001, CFI = 0.95, NFI = 0.94, RMSEA = 0.06; for the Israeli and the German samples, respectively]. Each item was rated on a 5‐point scale. Internal consistency was acceptable in the Israeli (emotional: α = 0.78, cognitive: α = 0.62, behavioural: α = 0.64) and in the German samples (emotional: α = 0.79, cognitive: α = 0.62, behavioural: α = 0.73).
2.2.3. Assessment of depression and anxiety
Depression was assessed using the Beck Depression Inventory (BDI‐II; Beck et al., 1996). The BDI‐II comprises 21 items (e.g., ‘I can't get any pleasure from the things I used to enjoy.’). The sum score of all items was used for analyses (Israel: α = 0.92, Germany: α = 0.94).
Anxiety was assessed using the State version of the State‐Trait Anxiety Inventory (STAI‐S; Spielberger, 1983). The STAI‐S assesses respondents' current anxiety levels using 20 items that are rated on a 4‐point scale (e.g., ‘I feel upset’; α = 0.96, Germany: α = 0.96).
2.2.4. Assessment of potential covariates
To examine the effects of Lifetime trauma exposure on response profiles, we used the Life Events Checklist for DSM‐5 (LEC‐5; Weathers et al., 2013). The LEC‐5 contains 16 potentially traumatic events. Participants are asked to indicate their level of exposure (happened to me, witnessed it, learned about it, part of my job, not sure or does not apply). Some items refer to inter‐personal events (‘Combat or exposure to a war‐zone’), while others refer to accidental trauma (‘Natural disaster’). Following the distinction of Cloitre et al. (2018), we calculated the amount of interpersonal traumatic events (physical assault, assault with a weapon, sexual assault, other unwanted or uncomfortable sexual experiences, combat or exposure to a warzone, captivity, serious injury and/or harm and/or death you caused to someone else) to compare the context of the two countries prior to the pandemic. In the main analyses, we followed previous studies which used a general score of all items for which participants indicated direct (happened to me) or indirect (witnessed it, part of my job) exposure (Israel: α = 0.95, Germany: α = 0.94).
To assess the effects of Social support, we used the Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al., 1988). The MSPSS consists of 12 items that assess support from friends, family and one's significant other (sample item: ‘I can count on my friends when things go wrong.’). Each item is rated on a 7‐point scale (Israel: α = 0.93, Germany: α = 0.94).
2.3. Data analysis
To explore the existence of different response profiles, we conducted latent profile analyses (LPA) in each subsample using the three response subscales as indicators. LPA is a mixture modelling technique (McLachlan et al., 2019), which models participants' heterogeneous patterns of responses to latent class indicators as a mix of normal distributions within each class (Peugh & Fan, 2013). Latent class enumeration determines the number of latent classes and calculates the mean response profile in each latent class (Peugh & Fan, 2013).
According to widely used methodological recommendations (e.g., Pastor & Gagné, 2013; Peugh & Fan, 2013), models were evaluated based on Akaike's Information Criterion (AIC), the Bayesian Information Criterion (BIC), the sample‐size adjusted BIC (SABIC), as well as the adjusted and bootstrapped likelihood ratio test (ALRT and BLRT), and entropy. For AIC, BIC, and SABIC, lower values indicate a model that fits better. ALRT and BLRT test whether a more complex model fits better than a model that has one less latent class. A p‐value associated with ALRT (BLRT) below the significance level (i.e., 0.05) indicates a better fit for the more complex model compared to its simpler counterpart. Entropy is an index that quantifies the separation of latent classes and ranges between 0 and 1, with higher values indicating better class separation. Finally, we also considered the parsimony of the model, substantive interpretability of the profiles and the relative increase in model fit when selecting the final models. LPAs were conducted in Mplus, version 8.6 (Muthén & Muthén, 2021). In all LPA models, means and the variances of the profile indicators in each latent class were estimated freely. The covariances among indicators within latent classes were fixed to zero in all models.
In addition to conducting LPAs within each subsample, we used the approach described by Morin et al. (2016) to assess the similarity of profile structure across both countries. To this end, we compared model fits of models imposing configural (number of profiles), structural (within‐profile means), dispersion (within‐profile means and variability) and distributional (within‐profile means, variability and proportions) similarity. These model comparisons assess whether LPA analyses can be run on the combined overall sample (participants of both countries together), or alternatively, LPA should be run separately for each country. If the configural model has better fit indices than the more constrained three models, according to Morin et al. (2016), it is not viable to interpret the results of the LPA analysis unified across both countries rather LPAs should be conducted separately in each subsample.
To characterise individual profiles, we compared subscales across and within classes. We also investigated differences between response profiles in depression and anxiety during the pandemic. Lastly, we examined the effects of potential covariates (i.e., sociodemographic variables, social support, lifetime trauma exposure) and flexibility (i.e., cognitive and coping flexibility) on latent class membership. We used the BCH method to assess associations between profiles as independent variables and anxiety/depression outcomes as dependent variables (Asparouhov & Muthén, 2021; Bakk & Vermunt, 2016). For independent variables predicting profile membership, we used the three‐step method (multinomial logistic regression) recommended by Asparouhov and Muthén (2014) to estimate class membership in relation to these variables while accounting for misspecification bias.
3. RESULTS
3.1. Baseline characteristics
Both subsamples comprised a higher number of female than male participants (Germany: 79.54%, Israel: 82.59%), with no significant between‐sample differences (p > 0.05). Subsamples were found to differ (p < 0.05, η2 = 0.002) in mean age with German participants (M = 41.32, SD = 14.16) being younger than Israeli participants (M = 42.69, SD = 14.78). However, with a mean of 1.37 years, this difference was not substantial. Subsamples did not differ in economic status (p > 0.05, η2 = 0.001), with the majority of participants in Germany (M = 1.94, SD = 0.74) and Israel (M = 1.99, SD = 0.73) indicating that their income was around average. 2 Finally, we compared subsamples with respect to trauma history, which did not reveal any significant differences (p > 0.05, η2 = 0.001) between German (M = 4.19, SD = 2.88) and Israeli (M = 3.96, SD = 3.05) participants. Examination of interpersonal trauma exposure specifically revealed a significantly higher exposure rate (p < 0.001, η2 = 0.017) in Israeli (M = 1.54, SD = 1.49) as compared to German (M = 1.09, SD = 1.23) participants.
3.2. Latent profile analyses
In the first step of the LPA, we identified the number of classes that modelled appropriately participants' endorsement of the profile indicators. For the German subsample, p‐ALRT and p‐BLRT became non‐significant for the four‐class solution, supporting that a three‐class solution was a better fit (Table 1). For the Israeli subsample, p‐ALRT and p‐BLRT were significant for the four‐class solution, supporting a four‐class solution (Table 1). However, closer examination of the four‐class solution revealed that two of the four classes were not sufficiently distinct from each other, precluding substantive interpretability of the profiles. By contrast, the three‐class solution yielded three clearly differentiable profiles. Thus, based on parsimony and substantive interpretability, we selected the three‐class solution for the Israeli sample.
TABLE 1.
Statistical criteria associated with latent class enumeration
| Model | k | SSS | LL | AIC | BIC | SABIC | p‐ALRT | p‐BLRT | Entropy |
|---|---|---|---|---|---|---|---|---|---|
| Class Enumeration: Germany | |||||||||
| 1‐class | 1 | ‐ | −2964.36 | 5940.72 | 5968.38 | 5949.33 | ‐ | ‐ | ‐ |
| 2‐class | 2 | 336 | −2793.80 | 5607.59 | 5653.70 | 5621.94 | < 0.001 | < 0.001 | 0.858 |
| 3‐class | 3 | 175 | −2755.28 | 5538.55 | 5603.10 | 5558.65 | < 0.001 | < 0.001 | 0.848 |
| 4‐class | 4 | 128 | −2751.18 | 5538.36 | 5621.35 | 5564.20 | 0.266 | 0.280 | 0.780 |
| Class Enumeration: Israel | |||||||||
| 1‐class | 1 | ‐ | −8916.81 | 17845.62 | 17880.14 | 17861.08 | ‐ | ‐ | ‐ |
| 2‐class | 2 | 883 | −8032.19 | 16084.39 | 16141.92 | 16110.15 | < 0.001 | < 0.001 | 0.841 |
| 3‐class | 3 | 431 | −7854.64 | 15737.28 | 15817.83 | 15773.35 | 0.002 | 0.003 | 0.796 |
| 4‐class | 4 | 232 | −7765.43 | 15566.87 | 15670.43 | 15613.24 | < 0.001 | < 0.001 | 0.782 |
| Cross‐national Similarity | |||||||||
| Configural | 3 | 175 | −13100.93 | 26283.86 | 26531.10 | 26400.83 | ‐ | ‐ | 0.687 |
| Structural | 3 | 175 | −13112.58 | 26289.16 | 26482.13 | 26380.45 | ‐ | ‐ | 0.665 |
| Dispersion | 3 | 175 | −13165.41 | 26364.82 | 26467.34 | 26413.32 | ‐ | ‐ | 0.788 |
| Distributional | 3 | 175 | −13139.17 | 26314.34 | 26422.89 | 26363.70 | ‐ | ‐ | 0.788 |
Abbreviations: AIC, Akaike Information Criterion; BIC, Bayesian Information Criterion; LL, log‐likelihood; p‐ALRT, the p‐value associated with the adjusted likelihood ratio test; p‐BLRT, the p‐value associated with the bootstrapped likelihood ratio test; SABIC, sample‐size adjusted BIC; SSS, the smallest sample size associated with any of the classes identified by the given model.
Since a three‐class solution was selected for each country, configural similarity between countries was supported by the data. Thus, we conducted an LPA across both countries to investigate whether profiles can be interpreted independently of country. Based on this unified analysis, we evaluated whether the configural similarity model—assuming three classes across both countries—had an inferior model fit as compared to the structural similarity model (assuming the same class structure as well as equal means), the dispersion similarity model (assuming the same class structure as well as equal means and variances) and the distributional similarity model (assuming the same class structure as well as equal means, variances and proportions) across countries. This was not the case as reflected in model fit indices (Table 1). According to Morin et al. (2016), it is thus not viable to interpret the results of the LPA analysis unified across both countries. Hence, we continued examining LPAs conducted separately in each subsample. Mean profiles corresponding to the three classes in each subsample are presented in Figure 1 and profiles' characteristics are summarised in Table 2.
FIGURE 1.
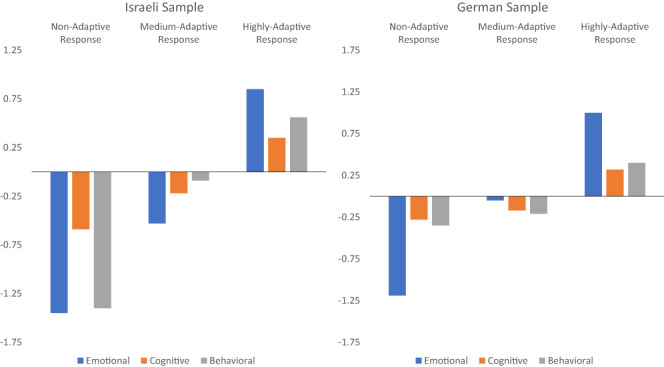
Profiles of emotional, cognitive and behavioural response to COVID‐19‐related stress.
TABLE 2.
Characteristics of individual profiles
| Country | Latent class | n | Emotional | Cognitive | Behavioural | Significant differences (p < 0.05) | |||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | ||||
| Germany | Non‐adaptive response profile | 255 | −1.19 | 0.32 | −0.28 | 0.91 | −0.35 | 0.95 | C, B > E |
| Medium‐adaptive response profile | 175 | −0.05 | 0.28 | −0.17 | 0.95 | −0.21 | 0.97 | B, C, E | |
| Highly adaptive response profile | 313 | 1.00 | 0.30 | 0.32 | 1.02 | 0.40 | 0.92 | E > B, C | |
| Israel | Non‐adaptive response profile | 431 | −1.45 | 0.34 | −0.59 | 0.85 | −1.40 | 0.74 | C > B, E |
| Medium‐adaptive response profile | 718 | −0.53 | 0.42 | −0.22 | 0.85 | −0.09 | 0.65 | B > C > E | |
| Highly adaptive response profile | 1181 | 0.85 | 0.40 | 0.35 | 1.00 | 0.56 | 0.70 | E > B > C | |
Note: This table presents standardised z‐scores for easier interpretation. Significant differences in the last column are based on post hoc Bonferroni tests within each profile following repeated measures ANOVAs.
In the German sample, a non‐adaptive response group emerged, comprising 34.32% of the entire sample (within the group, adaptivity of emotional response was lower than that of cognitive and behavioural responses). A second medium‐adaptive response group constituted 23.55% of the sample, whereas the remaining 42.13% was characterised by highly adaptive responding (within the group, adaptivity of emotional response was higher than of cognitive and behavioural responses).
In the Israeli sample, a non‐adaptive response group emerged comprising 18.50% of the entire sample (within the group, adaptivity of cognitive response was higher than of emotional and behavioural responses). A second group with medium‐adaptive responses constituted 30.82% of the sample (within the group, adaptivity of behavioural response was higher and adaptivity of emotional response was lower than adaptivity of cognitive response), whereas the remaining 51.68% was characterised by highly adaptive responding (within the group, adaptivity of emotional response was higher and adaptivity of cognitive response was lower than adaptivity of behavioural response).
3.3. Differences between profiles in depression and anxiety
Next, we examined differences among these response profiles regarding depression and anxiety. Means are presented in Table 3. In the German sample, the highly adaptive response group had significantly lower average BDI and STAI‐S scores than the medium‐adaptive response group, which in turn had significantly lower average scores than the non‐adaptive response group. The average BDI and STAI‐S scores of the non‐adaptive response group were in the clinically relevant range whereas scores in the medium‐ and highly adaptive response groups were in the non‐clinical range (Dozois et al., 1998; Kvaal et al., 2005). In the Israeli sample, the highly adaptive response group had significantly lower average BDI and STAI‐S scores than the medium‐adaptive response group, which in turn had significantly lower average scores than the non‐adaptive response group. The average BDI and STAI‐S scores of the non‐adaptive response group were in the clinically relevant range, whereas scores in the medium and highly‐adaptive response groups were in the non‐clinical range (Dozois et al., 1998; Kvaal et al., 2005).
TABLE 3.
Comparing depression and anxiety as predicted by profiles in each country
| Country | Outcome | Non‐adaptive response profile | Medium‐adaptive response profile | Highly adaptive response profile | ||||
|---|---|---|---|---|---|---|---|---|
| M | SE | M | SE | M | SE | Significant differences (p < 0.001) | ||
| Germany | Depression | 22.07 | 0.67 | 13.49 | 0.81 | 4.47 | 0.29 | P1 > P2 > P3 |
| Anxiety | 59.48 | 0.64 | 47.23 | 0.90 | 32.82 | 0.44 | P1 > P2 > P3 | |
| Israel | Depression | 25.17 | 0.63 | 13.06 | 0.37 | 6.35 | 0.20 | P1 > P2 > P3 |
| Anxiety | 63.43 | 0.58 | 48.22 | 0.46 | 34.38 | 0.29 | P1 > P2 > P3 | |
Note: Germany—BDI: P1 > P3: χ2 = 60.58, p < 0.001; P2 > P3: χ2 = 582.80, p < 0.001; P1 > P2: χ2 = 100.42, p < 0.001; STAI: P1 > P3: χ2 = 112.21, p < 0.001; P2 > P3: χ2 = 1183.29, p < 0.001; P1 > P2: χ2 = 189.03, p < 0.001; Israel—BDI: P1 > P2: χ2 = 235.35, p < 0.001; P2 > P3: χ2 = 828.63, p < 0.001; P1 > P3: χ2 = 233.44, p < 0.001; STAI: P1 > P2: χ2 = 357.85, p < 0.001; P2 > P3: χ2 = 1990.21, p < 0.001; P1 > P3: χ2 = 583.72, p < 0.001.
3.4. Predicting profile membership based on flexibility facets
Finally, we used flexibility facets to estimate class membership in multinomial logistic regression analyses. The non‐adaptive response group was used as a reference group in both samples. In the German sample, analyses revealed significant effects of gender, social support, lifetime trauma exposure, coping flexibility and cognitive flexibility. Accordingly, members of the highly adaptive response group were less likely to be female and more likely to report higher levels of social support, lower levels of lifetime trauma exposure and higher levels of cognitive flexibility and of coping flexibility compared to the non‐adaptive response group. No significant effects emerged between the low‐ and medium‐response groups (Table 4).
TABLE 4.
Predicting profiles based on socio‐demographic variables, social support, lifetime trauma exposure and flexibility facets in the German subsample
| Predictor | Medium‐adaptive response profile | Highly‐adaptive response profile | ||||
|---|---|---|---|---|---|---|
| B | OR | 95% | B | OR | 95% | |
| Age | −0.01 | 0.89 | 0.70–1.14 | 0.01 | 1.10 | 0.89–1.37 |
| Gender | −0.33 | 0.88 | 0.68–1.13 | −0.90*** | 0.71 | 0.58–0.87 |
| Economic status | 0.13 | 1.13 | 0.88–1.44 | 0.05 | 1.05 | 0.84–1.30 |
| Social support | 0.00 | 0.95 | 0.76–1.18 | 0.03** | 1.57 | 1.23–2.02 |
| Lifetime Trauma exposure | 0.02 | 1.10 | 0.87–1.39 | −0.11** | 0.73 | 0.59–0.89 |
| Coping flexibility | 0.08 | 1.14 | 0.89–1.46 | 0.18** | 1.40 | 1.12–1.75 |
| Cognitive flexibility | 0.02 | 1.22 | 0.92–1.61 | 0.12*** | 2.60 | 1.98–3.41 |
Abbreviations: OR, odds ratio; Reference, non‐adaptive response profile.
p < 0.01
p < 0.001.
For the Israeli sample, analyses revealed significant effects of gender, age, economic status, social support, lifetime trauma exposure, coping flexibility and cognitive flexibility. Results reflected that members of the highly adaptive response group were more likely to report higher age, higher economic status and cognitive flexibility and lower levels of lifetime trauma exposure than the non‐adaptive response group. Members of the highly and medium‐adaptive responding groups were less likely to be female and more likely to report higher levels of social support than the non‐adaptive response group. Finally, members of the high‐ and medium‐adaptive responding group were more likely to report higher levels of coping flexibility than members of the non‐adaptive response group (Table 5).
TABLE 5.
Predicting profiles based on socio‐demographic variables, social support, lifetime trauma exposure and flexibility facets in the Israeli subsample
| Predictor | Medium‐adaptive response profile | Highly adaptive response profile | ||||
|---|---|---|---|---|---|---|
| B | OR | 95% | B | OR | 95% | |
| Age | 0.02** | 1.29 | 1.08–1.53 | 0.04*** | 1.81 | 1.54–2.13 |
| Gender | −0.42 | 0.86 | 0.71–1.04 | −0.80*** | 0.74 | 0.62–0.88 |
| Economic status | 0.32* | 1.25 | 1.05–1.50 | 0.57*** | 1.51 | 1.28–1.78 |
| Social support | 0.02*** | 1.35 | 1.15–1.58 | 0.03*** | 1.70 | 1.45–1.99 |
| Lifetime Trauma exposure | −0.08** | 0.80 | 0.68–0.93 | −0.13*** | 0.68 | 0.59–0.79 |
| Coping flexibility | 0.23*** | 1.68 | 1.36–2.06 | 0.37*** | 2.28 | 1.87–2.78 |
| Cognitive flexibility | 0.01 | 1.05 | 0.86–1.27 | 0.03* | 1.25 | 1.04–1.50 |
Abbreviations: OR, odds ratio; Reference, non‐adaptive response profile.
p < 0.05
p < 0.01
p < 0.001;
4. DISCUSSION
The current study aimed to investigate adaptive responding during the early stage of the COVID‐19 pandemic and the possible effects of different flexibility domains. To examine cross‐national generalizability across conditions of high and low society‐level pre‐COVID‐19 stress, these objectives were assessed in Israeli and German participants. In line with previous research, analyses revealed three distinct response profiles in each country. The three profiles differed in the severity of anxiety and depression symptoms, with the non‐adaptive responding group reaching clinical symptom levels in both countries. Moreover, both cognitive flexibility and coping flexibility significantly predicted profile membership, with coping flexibility having a substantially larger impact in Israel than in Germany.
4.1. Characteristics and distribution of response profiles
In line with previous research (Kunzler et al., in press), latent profile analyses conducted separately in each country revealed the existence of three different profiles: a non‐adaptive response profile, a medium‐adaptive response profile and a high‐adaptive response profile. In line with the assumption that successful adjustment will be the modal response seen in response to the pandemic (Chen & Bonanno, 2020), the majority of Israeli (81.50%) and German (65.68%) participants showed a high‐ or medium‐adaptive response profile. Nevertheless, a substantial percentage fell into the non‐adaptive response profile, further characterised by high state anxiety and clinically relevant depressive symptoms. This finding illustrates the significant impact of the COVID‐19 pandemic on the mental health of a vulnerable subpopulation (Robinson et al., 2021; Schäfer et al., 2021).
Due to the lack of structural convergence, it is difficult to draw comparisons between countries based on profile structure. That said, we did find broadly comparable distributions of profiles in the German and Israeli samples, which could indicate a similar impact of COVID‐19 across countries. Correspondingly, previous studies comparing the mental health responses of Germans and Israelis during COVID‐19 show comparable levels of distress in both countries (Mækelæ et al., 2020; Mana et al., 2021). However, since previous studies had markedly lower sample sizes and assessed indicators of distress rather than adaptive responding to the pandemic, the current findings yield an important extension. Overall, our results may indicate that society‐level pre‐COVID‐19 stressor exposure does not result in a higher or lower rate of individuals, who struggle to respond adaptively to COVID‐19. As such, it appears to be neither an adaptivity nor a vulnerability factor in the context of the pandemic. However, this assumption needs to be confirmed by longitudinal research before strong conclusions can be drawn.
4.2. Impact of flexibility on response profiles
Regression analyses linking flexibility domains to profile membership revealed that cognitive flexibility and coping flexibility significantly predicted profile membership. In Israel, participants with higher coping flexibility and cognitive flexibility were more likely to be assigned to the medium‐ and highly adaptive responding group compared to the non‐adaptive responding group. A similar pattern was evident in the German subsample, with the exception that higher levels of coping flexibility were only associated with a higher probability of being assigned to the higher as opposed to the non‐adaptive responding group. These results align with a recent study that examined the incremental contributions of cognitive and regulatory flexibility in predicting current and lifetime PTSD symptoms (Haim‐Nachum & Levy‐Gigi, 2021). Both cognitive and coping flexibility were found to be significant predictors. Our findings thus replicate previous findings, while additionally expanding them to adaptive responding to a multidimensional long‐term stressor. As such, they underline the importance of cognitive and coping flexibility for responding to a range of different stressors (Burton et al., 2012; Palm & Follette, 2011). Critically, these flexibility domains were found to have incremental validity after controlling for several important predictors of adaptive responding such as economic status, social support and traumatic exposure.
When comparing the relative contributions of cognitive and coping flexibility in predicting profile membership, a differential pattern emerged between countries: While coping flexibility was a stronger predictor than cognitive flexibility in the Israeli sample, coping flexibility and cognitive flexibility were comparably strong predictors in the German sample. Moreover, coping flexibility emerged as a stronger predictor in Israel than in Germany and cognitive flexibility emerged as a stronger predictor in Germany than in Israel. This differential profile of flexibility domains linked to adaptive responding to COVID‐19 could be related to differences in society‐level pre‐COVID‐19 stress exposure in both countries. That is, coping flexibility may have been of greater importance in the Israeli sample due to the high rate of interpersonal trauma exposure, which provides more opportunities to practice this skill. This may result in individuals developing strong coping flexibility and thus primarily relying on it when responding to various stressors. Since the German population is not systematically subjected to such exposure, there may be a tendency to rely on both cognitive and coping flexibility. In support of this assumption, Israelis reported a higher number of traumatic events in the interpersonal trauma domain. This is consistent with the types of traumatic events that many civilians living in Israel are exposed to (e.g. missile attacks, hostiles throwing stones, stabbing attacks; Bleich et al., 2003; Weinberg et al., 2012). In further support, we compared flexibility levels across countries and found a significant interaction between country and flexibility domain. The interaction reflected a stronger difference in coping flexibility as compared to cognitive flexibility between Israeli and German participants, with Israelis reporting markedly higher coping flexibility. However, a smaller, yet significant difference in the same direction also emerged for cognitive flexibility. Hence, longitudinal studies are required to readdress whether differences in trauma exposure between countries could be related to differences in the relevance of flexibility domains.
4.3. Limitation
The current study provides new insights on adaptive responding to the pandemic, yet several limitations must be considered. First and foremost, the current study was cross‐sectional, which limits us in drawing causal inferences. Future studies should measure flexibility domains and adaptive responding continuously, to model longitudinal associations (Schäfer et al., 2021). In addition, we did not use any probabilistic sampling methods, which limit the generalizability of our results to the general population. Relatedly, our sampling strategy resulted in a substantially larger subsample from Israel as compared to Germany and we were not able to confirm structural similarity across countries. Nonetheless, both samples were found to be comparable in demographic characteristics. Moreover, result patterns were similar across countries, thus not providing any indications of biased sampling.
Additionally, we measured anxiety as a transient state. While this is a widely accepted way of measurement (e.g., Emons et al., 2019), it is possible that some participants reported anxiety was affected by other momentary anxiety‐inducing events unrelated to the pandemic. Therefore, future research might consider developing measures specific to stressful event. Moreover, due to lacking psychometric qualities, we were not able to include our measure of emotional flexibility (Burton & Bonanno, 2016) in the final analyses. Thus, our study could not shed light on the impact of regulatory flexibility on adaptive responding to COVID‐19. Future studies should reinvestigate the psychometric properties of the Hebrew version of the instrument and seek to optimise it for further use. Relatedly, in continuation of our prior research (Haim‐Nachum & Levy‐Gigi, 2021), we focused on cognitive and regulatory flexibility rather than assessing other constructs such as behavioural (Brown & Tait, 2010) or explanatory flexibility (Joseph & Gray, 2011). Future studies should consider assessing these constructs to provide a more comprehensive view of the incremental validity of individual flexibility domains.
4.4. Conclusion
Overall, the current findings support previous research in showing that COVID‐19 is a significant stressor that impacts the mental health of a subgroup of the population. Moreover, in line with previous research, we found that cognitive and coping flexibility were linked to adaptive responding to the pandemic, thus establishing these flexibility domains as predictors of dealing with a multidimensional—not necessarily traumatic—stressor. Comparisons between countries revealed different contributions of cognitive and coping flexibility in predicting successful responding. If replicated by future longitudinal studies, these findings may have important practical implications. They suggest that training cognitive and coping flexibility may help individuals to better cope with long‐term stressors such as COVID‐19. Such training could be selectively administered to a subpopulation with low levels of flexibility in these domains. Critically, our results suggest that it may be useful to adapt such training to the specifics of the respective population. That is, the focus of interventions (i.e. targeting one specific or several flexibility domains) should be based on the flexibility profile that is found to be beneficial in the respective population.
AUTHORS CONTRIBUTION
ELG conceptualised and designed the project. AH and MRS conducted the analyses and wrote the first draft of the manuscript. AH, MRS and ELG responded to the reviewers' comments. All authors reviewed, revised and approved the final version.
FUNDING INFORMATION
The study was supported by the Israel Science Foundation (grant #1128_16 to ELG).
CONFLICT OF INTEREST
We have no conflict of interest to disclose.
Supporting information
Appendix S1
Appendix S2
ACKNOWLEDGEMENTS
The authors would like to thank the Israeli Science Foundation for their support of this study and thank the participants for their time.
Hemi, A. , Sopp, M. R. , Schäfer, S. K. , Michael, T. , & Levy‐Gigi, E. (2022). Adaptive responding to prolonged stress exposure: A binational study on the impact of flexibility on latent profiles of cognitive, emotional and behavioural responses to the COVID‐19 pandemic. Health & Social Care in the Community, 30, e6163–e6174. 10.1111/hsc.14053
Alla Hemi and M. Roxanne Sopp contributed equally to this work.
Endnotes
We aimed at including three measures of flexibility in the analyses: cognitive, coping and emotional. However, the internal reliability of the emotional flexibility scale was found to be unsatisfactory in our sample. Therefore, we did not include emotional flexibility in the main analyses (for details, see Supplementary Material B).
1 = below average / 2 = average / 3 = above average / 4 = way above average
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- Asparouhov, T. , & Muthén, B. (2014). Auxiliary variables in mixture modeling: Three‐step approaches using M plus. Structural Equation Modeling: A Multidisciplinary Journal, 21(3), 329–341. [Google Scholar]
- Asparouhov, T. , & Muthén, B. (2021). Auxiliary Variables in Mixture Modeling: Using the BCH Method in Mplus to Estimate a Distal Outcome Model and an Arbitrary Secondary Model .
- Bakk, Z. , & Vermunt, J. K. (2016). Robustness of stepwise latent class modeling with continuous distal outcomes. Structural Equation Modeling: A Multidisciplinary Journal, 23(1), 20–31. [Google Scholar]
- Beck, A. T. , Steer, R. A. , & Brown, G. (1996). Beck depression inventory–II (BDI‐II) [Database record]. APA PsycTests. 10.1037/t00742-000 [DOI] [Google Scholar]
- Besser, A. , & Neria, Y. (2012). When home isn't a safe haven: Insecure attachment orientations, perceived social support, and PTSD symptoms among Israeli evacuees under missile threat. Psychological Trauma: Theory, Research, Practice, and Policy, 4(1), 34–46. 10.1037/a0017835 [DOI] [Google Scholar]
- Bleich, A. , Gelkopf, M. , & Solomon, Z. (2003). Exposure to terrorism, stress‐related mental health symptoms, and coping behaviors among a nationally representative sample in Israel. JAMA, 290(5), 612–620. [DOI] [PubMed] [Google Scholar]
- Bonanno, G. A. (2004). Loss, trauma, and human resilience: Have we underestimated the human capacity to thrive after extremely aversive events? American Psychologist, 59(1), 20–28. [DOI] [PubMed] [Google Scholar]
- Bonanno, G. A. , Pat‐Horenczyk, R. , & Noll, J. (2011). Coping flexibility and trauma: The perceived ability to cope with trauma (PACT) scale. Psychological Trauma: Theory, Research, Practice, and Policy, 3(2), 117–129. [Google Scholar]
- Brown, V. J. , & Tait, D. S. (2010). Behavioral flexibility: Attentional shifting, rule switching and response reversal. In Stolerman I. P. (Ed.), Encyclopedia of psychopharmacology (pp. 209–213). Springer. 10.1007/978-3-540-68706-1_340 [DOI] [Google Scholar]
- Burton, C. L. , & Bonanno, G. A. (2016). Measuring ability to enhance and suppress emotional expression: The flexible regulation of emotional expression (FREE) scale. Psychological Assessment, 28(8), 929–941. [DOI] [PubMed] [Google Scholar]
- Burton, C. L. , Yan, O. H. , Pat‐Horenczyk, R. , Chan, I. S. , Ho, S. , & Bonanno, G. A. (2012). Coping flexibility and complicated grief: A comparison of American and Chinese samples. Depression and Anxiety, 29(1), 16–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cañas, J. J. , Fajardo, I. , & Salmeron, L. (2006). Cognitive flexibility. International Encyclopedia of Ergonomics and Human Factors, 1, 297–301. [Google Scholar]
- Chen, S. , & Bonanno, G. A. (2020). Psychological adjustment during the global outbreak of COVID‐19: A resilience perspective. Psychological Trauma: Theory, Research, Practice, and Policy, 12(S1), S51. [DOI] [PubMed] [Google Scholar]
- Cheng, C. , Wang, H.‐Y. , & Ebrahimi, O. V. (2021). Adjustment to a “new normal”: Mental health benefits of coping flexibility during the COVID‐19 pandemic. Frontiers in Psychiatry, 12, 353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cloitre, M. , Shevlin, M. , Brewin, C. R. , Bisson, J. I. , Roberts, N. P. , Maercker, A. , Karatzias, T. , & Hyland, P. (2018). The international trauma questionnaire: Development of a self‐report measure of ICD‐11 PTSD and complex PTSD. Acta Psychiatrica Scandinavica, 138(6), 536–546. [DOI] [PubMed] [Google Scholar]
- Emons, W. H. , Habibović, M. , & Pedersen, S. S. (2019). Prevalence of anxiety in patients with an implantable cardioverter defibrillator: Measurement equivalence of the HADS‐A and the STAI‐S. Quality of Life Research, 28(11), 3107–3116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fernández, R. S. , Crivelli, L. , Guimet, N. M. , Allegri, R. F. , & Pedreira, M. E. (2020). Psychological distress associated with COVID‐19 quarantine: Latent profile analysis, outcome prediction and mediation analysis. Journal of Affective Disorders, 277, 75–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldfarb, E. V. (2020). Participant stress in the COVID‐19 era and beyond. Nature Reviews Neuroscience, 21(12), 663–664. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greene, T. , Itzhaky, L. , Bronstein, I. , & Solomon, Z. (2018). Psychopathology, risk, and resilience under exposure to continuous traumatic stress: A systematic review of studies among adults living in southern Israel. Traumatology, 24(2), 83. [Google Scholar]
- Gruber, J. , Prinstein, M. J. , Clark, L. A. , Rottenberg, J. , Abramowitz, J. S. , Albano, A. M. , Aldao, A. , Borelli, J. L. , Chung, T. , Davila, J. , Forbes, E. E. , Gee, D. G. , Hall, G. C. N. , Hallion, L. S. , Hinshaw, S. P. , Hofmann, S. G. , Hollon, S. D. , Joormann, J. , Kazdin, A. E. , … Weinstock, L. M. (2021). Mental health and clinical psychological science in the time of COVID‐19: Challenges, opportunities, and a call to action. American Psychologist, 76(3), 409–426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haim‐Nachum, S. , & Levy‐Gigi, E. (2021). The tension between cognitive and regulatory flexibility and their associations with current and lifetime PTSD symptoms [brief research report]. Frontiers in Psychology, 12(361), 1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hynes, K. C. , Tambling, R. R. , Russell, B. S. , Park, C. L. , & Fendrich, M. (2021). A latent profile analysis of the COVID‐19 stressors scale. Theory, Research, Practice, and Policy. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ionescu, T. (2012). Exploring the nature of cognitive flexibility. New Ideas in Psychology, 30(2), 190–200. [Google Scholar]
- Jordan, L. S. , Woodard, J. L. , Pena, G. S. , Arnold‐Nedimala, N. A. , Won, J. , Callow, D. D. , & Smith, J. C. (2022). Forward‐focused coping predicts better mental health outcomes in mid‐to late‐life during the COVID‐19 pandemic. Aging and Mental Health, 26(3), 554–562. [DOI] [PubMed] [Google Scholar]
- Joseph, J. S. , & Gray, M. J. (2011). The utility of measuring explanatory flexibility in PTSD research. Cognitive Therapy and Research, 35(4), 372–380. [Google Scholar]
- Kalia, V. , Knauft, K. , & Hayatbini, N. (2020). Cognitive flexibility and perceived threat from COVID‐19 mediate the relationship between childhood maltreatment and state anxiety. PLoS One, 15(12), e0243881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keith, J. , Velezmoro, R. , & O'Brien, C. (2015). Correlates of cognitive flexibility in veterans seeking treatment for posttraumatic stress disorder. The Journal of Nervous and Mental Disease, 203(4), 287–293. [DOI] [PubMed] [Google Scholar]
- Koesten, J. , Schrodt, P. , & Ford, D. J. (2009). Cognitive flexibility as a mediator of family communication environments and young adults' well‐being. Health Communication, 24(1), 82–94. [DOI] [PubMed] [Google Scholar]
- Kraft, D. , Rademacher, L. , Eckart, C. , & Fiebach, C. J. (2020). Cognitive, affective, and feedback‐based flexibility ‐ disentangling shared and different aspects of three facets of psychological flexibility. Journal of Cognition, 3(1), 21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krishnamoorthy, Y. , Nagarajan, R. , Saya, G. K. , & Menon, V. (2020). Prevalence of psychological morbidities among general population, healthcare workers and COVID‐19 patients amidst the COVID‐19 pandemic: A systematic review and meta‐analysis. Psychiatry Research, 293, 113382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lenzo, V. , Quattropani, M. C. , Sardella, A. , Martino, G. , & Bonanno, G. A. (2021). Depression, anxiety, and stress among healthcare workers during the COVID‐19 outbreak and relationships with expressive flexibility and context sensitivity. Frontiers in Psychology, 12, 348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leung, R. C. , & Zakzanis, K. K. (2014). Brief report: Cognitive flexibility in autism spectrum disorders: A quantitative review. Journal of Autism and Developmental Disorders, 44(10), 2628–2645. [DOI] [PubMed] [Google Scholar]
- Levy‐Gigi, E. , Bonanno, G. A. , Shapiro, A. R. , Richter‐Levin, G. , Kéri, S. , & Sheppes, G. (2016). Emotion regulatory flexibility sheds light on the elusive relationship between repeated traumatic exposure and posttraumatic stress disorder symptoms. Clinical Psychological Science, 4(1), 28–39. [Google Scholar]
- Levy‐Gigi, E. , Donner, R. , & Bonanno, G. A. (2020). Free your mind: Emotional expressive flexibility moderates the effect of stress on post‐traumatic stress disorder symptoms. International Journal of Molecular Sciences, 21(15), 5355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li, L. , Niu, Z. , Li, H. , Griffiths, M. D. , Mei, S. , Jiang, H. , & Xin, J. (2021). Latent profile analysis of mental health among Chinese healthcare staff during the COVID‐19 pandemic. Psychol Health Med, 29, 1–14. [DOI] [PubMed] [Google Scholar]
- Mækelæ, M. J. , Reggev, N. , Dutra, N. , Tamayo, R. M. , Silva‐Sobrinho, R. A. , Klevjer, K. , & Pfuhl, G. (2020). Perceived efficacy of COVID‐19 restrictions, reactions and their impact on mental health during the early phase of the outbreak in six countries. Royal Society Open Science, 7(8), 200644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mana, A. , Bauer, G. , Magistretti, C. M. , Sardu, C. , Juvinyà‐Canal, D. , Hardy, L. , Catz, O. , Tušl, M. , & Sagy, S. (2021). Order out of chaos: Sense of coherence and the mediating role of coping resources in explaining mental health during COVID‐19 in 7 countries. SSM‐Mental Health, 1, 100001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin, M. M. , & Rubin, R. B. (1995). A new measure of cognitive flexibility. Psychological Reports, 76(2), 623–626. [Google Scholar]
- McLachlan, G. J. , Lee, S. X. , & Rathnayake, S. I. (2019). Finite mixture models. Annual Review of Statistics and its Application, 6, 355–378. [Google Scholar]
- Morin, A. J. , Meyer, J. P. , Creusier, J. , & Biétry, F. (2016). Multiple‐group analysis of similarity in latent profile solutions. Organizational Research Methods, 19(2), 231–254. [Google Scholar]
- Palm, K. M. , & Follette, V. M. (2011). The roles of cognitive flexibility and experiential avoidance in explaining psychological distress in survivors of interpersonal victimization. Journal of Psychopathology and Behavioral Assessment, 33(1), 79–86. [Google Scholar]
- Paredes, M. R. , Apaolaza, V. , Fernandez‐Robin, C. , Hartmann, P. , & Yañez‐Martinez, D. (2021). The impact of the COVID‐19 pandemic on subjective mental well‐being: The interplay of perceived threat, future anxiety and resilience. Personality and Individual Differences, 170, 110455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pastor, D. A. , & Gagné, P. (2013). Mean and covariance structure mixture models .
- Pat‐Horenczyk, R. , & Schiff, M. (2019). Continuous traumatic stress and the life cycle: Exposure to repeated political violence in Israel. Current Psychiatry Reports, 21(8), 1–9. [DOI] [PubMed] [Google Scholar]
- Paudel, D. (2020). ABC framework of fear of COVID‐19 for psychotherapeutic intervention in Nepal: A review . 10.31234/OSF.IO/9SJ4A [DOI]
- Pedrosa, A. L. , Bitencourt, L. , Fróes, A. C. F. , Cazumbá, M. L. B. , Campos, R. G. B. , de Brito, S. B. C. S. , & Simões e Silva, A. C. (2020). Emotional, behavioral, and psychological impact of the COVID‐19 pandemic. Frontiers in Psychology, 11, 566212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peugh, J. , & Fan, X. (2013). Modeling unobserved heterogeneity using latent profile analysis: A Monte Carlo simulation. Structural Equation Modeling: A Multidisciplinary Journal, 20(4), 616–639. [Google Scholar]
- Pfefferbaum, B. , & North, C. S. (2020). Mental health and the Covid‐19 pandemic. New EnglandJjournal of Medicine, 383(6), 510–512. [DOI] [PubMed] [Google Scholar]
- Robinson, E. , Sutin, A. R. , Daly, M. , & Jones, A. (2021). A systematic review and meta‐analysis of longitudinal cohort studies comparing mental health before versus during the COVID‐19 pandemic. medRxiv . [DOI] [PMC free article] [PubMed]
- Russo‐Netzer, P. , & Ameli, M. (2021). Optimal sense‐making and resilience in times of pandemic: Integrating rationality and meaning in psychotherapy. Frontiers in Psychology, 12, 1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rutter, M. (1987). Psychosocial resilience and protective mechanisms. American Journal of Orthopsychiatry, 57(3), 316–331. [DOI] [PubMed] [Google Scholar]
- Salari, N. , Hosseinian‐Far, A. , Jalali, R. , Vaisi‐Raygani, A. , Rasoulpoor, S. , Mohammadi, M. , Rasoulpoor, S. , & Khaledi‐Paveh, B. (2020). Prevalence of stress, anxiety, depression among the general population during the COVID‐19 pandemic: A systematic review and meta‐analysis. Globalization and Health, 16(1), 1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sardella, A. , Lenzo, V. , Bonanno, G. A. , Basile, G. , & Quattropani, M. C. (2021). Expressive flexibility and dispositional optimism contribute to the elderly's resilience and health‐related quality of life during the COVID‐19 pandemic. International Journal of Environmental Research and Public Health, 18(4), 1698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schäfer, S. , Sopp, R. , Koch, M. , Göritz, A. S. , & Michael, T. (2021). The long‐term buffering effect of sense of coherence on psychopathological symptoms during the COVID‐19 pandemic: Findings from a prospective observational study. [DOI] [PMC free article] [PubMed]
- Schäfer, S. K. , Sopp, M. R. , Schanz, C. G. , Staginnus, M. , Göritz, A. S. , & Michael, T. (2020). Impact of COVID‐19 on public mental health and the buffering effect of a sense of coherence. Psychotherapy and Psychosomatics, 89(6), 386–392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seiter, J. S. , & Curran, T. (2021). Social‐distancing fatigue during the COVID‐19 pandemic: A mediation analysis of cognitive flexibility, fatigue, depression, and adherence to CDC guidelines. Communication Research Reports, 38(1), 68–78. [Google Scholar]
- Shigeto, A. , Laxman, D. J. , Landy, J. F. , & Scheier, L. M. (2021). Typologies of coping in young adults in the context of the COVID‐19 pandemic. The Journal of General Psychology, 148(3), 272–304. [DOI] [PubMed] [Google Scholar]
- Spielberger, C. D. (1983). State‐trait anxiety inventory for adults (STAI‐AD) [Database record]. APA PsycTests. 10.1037/t06496-000 [DOI] [Google Scholar]
- Torrente, F. , Yoris, A. , Low, D. M. , Lopez, P. L. , Bekinschtein, P. , Vazquez, G. , Manes, F. , & Cetkovich, M. (2022). Psychological symptoms, mental fatigue and behavioural adherence after 72 continuous days of strict lockdown during the COVID‐19 pandemic in Argentina. British Journal of Psychiatry Open, 8(1), E10. 10.1192/bjo.2021.1065 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang, Y. , Kala, M. P. , & Jafar, T. H. (2020). Factors associated with psychological distress during the coronavirus disease 2019 (COVID‐19) pandemic on the predominantly general population: A systematic review and meta‐analysis. PLoS One, 15(12), e0244630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weathers, F. , Blake, D. , Schnurr, P. , Kaloupek, D. , Marx, B. , & Keane, T. (2013). The life events checklist for DSM‐5 (LEC‐5) .
- Weinberg, M. , Besser, A. , Campeas, M. , Shvil, E. , & Neria, Y. (2012). Reactions of civilians exposed to terrorism and war trauma in Israel: The role of intra‐ and interpersonal factors. In Columbus A. M. (Ed.), Advances in psychology research (pp. 1–53). Nova Science Publishers. [Google Scholar]
- Xu, J. J. , Ou, J. Y. , Luo, S. Y. , Wang, Z. J. , Chang, E. , Novak, C. , Shen, J. Y. , Zheng, S. Y. , & Wang, Y. A. (2020). Perceived social support protects lonely people against COVID‐19 anxiety: A three‐wave longitudinal study in China. Frontiers in Psychology, 11, 66965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zimet, G. D. , Dahlem, N. W. , Zimet, S. G. , & Farley, G. K. (1988). The multidimensional scale of perceived social support. Journal of Personality Assessment, 52(1), 30–41. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1
Appendix S2
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.