

Abstract
Objectives
Very little data are known about charcoal toothpastes. The aim of this study was to counteract the missing data by determining the relative dentin abrasivity (RDA) and relative enamel abrasivity (REA) values of charcoal toothpastes.
Methods
Radioactively charged dentin and enamel samples were randomly divided into groups of eight specimens. Each group was brushed with two of total 12 charcoal toothpaste slurries and with a standard abrasive with a known RDA and REA value. The measured radioactivity in counts per minute within the slurries corresponds to the amount of dentin or enamel abraded. RDA and REA values of the charcoal toothpastes were expressed relative to the known value of the standard slurry.
Results
The RDA and REA values of the charcoal toothpastes have a broad range of 24–166 and 0–14, respectively.
Conclusions
The RDA and REA values do not differ significantly from previously tested commercially available toothpastes. However, the lack of fluoride compounds in many of the investigated charcoal toothpastes can have a less beneficial effect for the consumers. It is very important to educate patients accordingly.
Keywords: abrasivity, activated charcoal, RDA, REA, toothpaste
1. INTRODUCTION
There is evidence that the Egyptians in ancient times were the first ones, who used activated charcoal. Back then, it was mainly used for metal production, as material for cooking and for medical purposes. 1 , 2 The word activated describes that the charcoal consists of extremely small particles, which results in high porosity and thus a very large adsorbing surface. Even in today's medicine, activated charcoal is still used as an alternative treatment. The large surface area of the activated charcoal allows the adsorption of many drugs and toxins in the gastrointestinal tract. This causes the body to absorb less of these substances. For this reason, it has been used in medicine in case of acute overdoses or poisoning. 3 As far as dental care is concerned, Hippocrates discussed the possibility of combating black gums and foetor ex ore, using crushed ashes from rabbit heads and mice in ancient Greece. 4 Clean white teeth were already regarded as a status symbol by the Romans, which has not changed until today. 4 In cosmetics industry, more and more products containing activated charcoal are being marketed. The use of charcoal for oral hygiene has long been known in many cultures such as India, Malaysia, Bangladesh, Tanzania and Italy. 5 Activated charcoal is supposed to remove discoloration from the teeth and therefore should have a whitening effect. However, clinical evidence does not support these companies' claims. 2 Especially nowadays with the possibility of marketing via social media, it is important to be able to inform patients about dental care products based on evidence. Many companies advertise the natural ingredients of their charcoal toothpastes. However, this usually also means that many do not contain fluoride. 6 Fluoride is known to protect teeth against demineralization and even promote the reabsorption of minerals from saliva back into the enamel. 7 , 8 There is therefore justified concern that these toothpastes could increase the risk of tooth decay. 5 A study by Franco et al. 9 showed that the charcoal‐based toothpowder does not show any dental bleaching effect. Charcoal‐containing toothpastes initially color the oral cavity black, which increases the contrast to the white/yellowish teeth. This can lead to consumers being misled about the whitening effects of such pastes. Besides other effects, charcoal acts as an abrasive in toothpastes, but there are very few studies on the actual abrasiveness of such toothpastes. 6 A high abrasiveness can lead to excessive dental hard tissue loss. With further progression and/or in cases of gingival recession, it can affect the dentin, which can be the cause of the development of hypersensitivity. 10 , 11 , 12 The gold standard to determine the relative dentin abrasivity (RDA) and relative enamel abrasivity (REA) of toothpastes was already developed in the 1950s. 13 As implied by their names, these measurements are relative because the abrasiveness of the toothpaste to be tested is compared with that of a known standard abrasive. The RDA/REA value of this standard abrasive was set at 100 and 10, respectively, and the abrasiveness of the different toothpastes is expressed as a percentage of this. 10 , 14 If a toothpaste is twice or half as abrasive, it achieves an RDA value of 200 or 50, respectively. 10
Usually only the RDA, but not the REA value, of toothpastes is determined. Reason for this is the fact that the dentin has a lower resistance to abrasions than the enamel and is therefore more likely to be viewed as a weak point. However, since only the enamel of the oral cavity is exposed in healthy intraoral conditions, it comes into contact with the pastes the most and should therefore not be neglected. This is of special importance, since new types of used abrasives can be harder than the enamel. 15
In 2020, Hamza et al. 10 tested 20 commercially available toothpastes with diamond powder and traditional abrasives for their RDA and REA values. However, none of the toothpastes included activated charcoal, of which more and more are appearing on the market.
The aim of the present study was to determine and compare the RDA and REA values of 12 charcoal toothpastes available in Switzerland in order to be able to educate patients about their abrasive potential.
2. MATERIALS AND METHODS
2.1. Toothpastes and sample preparation
Twelve charcoal‐containing toothpastes (Table 1) were purchased online from different providers in Switzerland in 2021.
TABLE 1.
Measured RDA and REA (± SD) values in this study. Supplemented with manufacturer information on the declared RDA values, the abrasives and the fluoride content
| Toothpastes | Manufacturer | RDA measured (± SD) | REA measured (± SD) | RDA declared | Abrasives a | Fluoride [ppm F−] |
|---|---|---|---|---|---|---|
| Curaprox white is black | Curaden AG; Kriens, Switzerland |
37 (± 6) |
0 (± 0) |
50 |
Activated charcoal Hydroxyapatite (15,000 ppm, Nano) |
NaF [1450] |
| Curaprox black is white | Curaden AG; Kriens, Switzerland |
42 (± 5) |
3 (± 1) |
50 |
Activated charcoal Hydroxyapatite (15,000 ppm, Nano) |
NaF [1450] |
| Colgate natural extracts charcoal & white | GABA, Therwil, Switzerland |
53 (± 4) |
2 (± 1) |
– |
Charcoal Powder Hydrated silica |
NaF [1000] |
| Naturaline zahnpaste aktivkohle | Coop Genossen‐schaft, Basel, Switzerland |
27 (± 4) |
0 (± 0) |
– | Charcoal Powder | None |
| EcoDenta black whitening toothpaste | UAB BIOK, Vilnius, Lithuania |
64 (± 4) |
4 (± 4) |
– |
Charcoal Powder Hydrated silica |
None |
| Natural toothpaste charcoal | The Humble Co., Sundbyberg, Sweden |
67 (± 6) |
5 (± 5) |
80–90 |
Charcoal Powder Hydrated silica |
NaF [1450] |
| Zew for men toothpaste with charcoal | Eco international GmbH, Weimar, Germany |
38 (± 4) |
2 (± 1) |
– |
Charcoal Powder Hydrated silica Hydroxyapatite |
None |
| Bamboo charcoal toothpaste mint | Nanchang Smile Technology Co., Ltd, Nanchang city, China |
26 (± 3) |
2 (± 1) |
– |
Charcoal Powder Hydrated silica |
None |
| MyMagicMud whitening toothpaste | Carbon & Clay Co., Texas, USA |
97 (± 11) |
9 (± 4) |
– |
Charcoal Powder Solum Diatomeae Bentonite |
None |
| Blackwood charcoal toothpaste | SPLAT, London, England |
166 (± 9) |
11 (± 4) |
– |
Charcoal Powder Hydrated silica |
None |
| Kemphor charcoal toothpaste | Laboratorios Verkos, Pinseque, Spain |
99 (± 7) |
12 (± 2) |
– |
Charcoal Powder Hydrated silica |
NaF [1450] |
| Candida white black‐pearls | Mibelle AG, Buchs, Switzerland |
53 (± 3) |
14 (± 3) |
55 |
Charcoal Powder Hydrated silica |
NaF [1450] |
Abrasives as declared by manufacturer: Hydrated silica = SiO2 · nH2O; Hydroxyapatite = Ca5(PO4)3OH; Solum Diatomeae = Mainly SiO2 (silica); Bentonite = Mixture of different clay minerals.
Extracted and cleaned bovine permanent incisors from a slaughterhouse were used for the dentin and enamel sample preparation. The roots of the teeth were separated from the crowns using a diamond cutting disc (Isomet, low speed saw, Buehler, Illinois, USA). The roots served as dentin samples and the crowns as enamel samples. The roots and crowns were ground in half (longitudinal axis, roughly through their root canals) using a grinding machine (Tegramin‐30, Struers A/S, Ballerup, Denmark) in order to generate a straight surface for embedding in Paladur (Heraeus Kulzer GmbH, Hanau, Germany). The untreated surfaces of the samples were polished using Sof‐Lex polishing discs (3 M Oral Care, St Paul, USA) under constant water cooling. The dentin samples were polished for 1 min each with light‐blue and light‐yellow discs. The enamel samples were polished for an additional 1 min with a blue disk before they were treated in the same way as dentin samples. The contact pressure of the disc was checked using a pressure gauge (TM 503 Power Module; Tektronix Inc., Beaverton, USA) and was between 40 and 60 g. New discs were used for each sample. The appearance of the samples can be seen in the study by Hamza et al. 10
The samples were then sent to the atomic institute in Vienna (Austria) so that they could be irradiated with neutrons at a maximum temperature of 55°C. In addition to the samples, a solution with a known amount of dissolved artificial apatite was also sent. This served as a control in each of the experiments. Before starting the actual experiments, the now radioactive samples were embedded in Paladur, so that they could be clamped in the V‐8 cross‐brushing machine (Sabri Enterprises, Downers Grove, USA). The samples were each stored in tap water to protect them from dehydration. For each two different toothpastes, eight randomly selected samples were used, which resulted total of six RDA or REA sample groups.
2.2. Test procedure
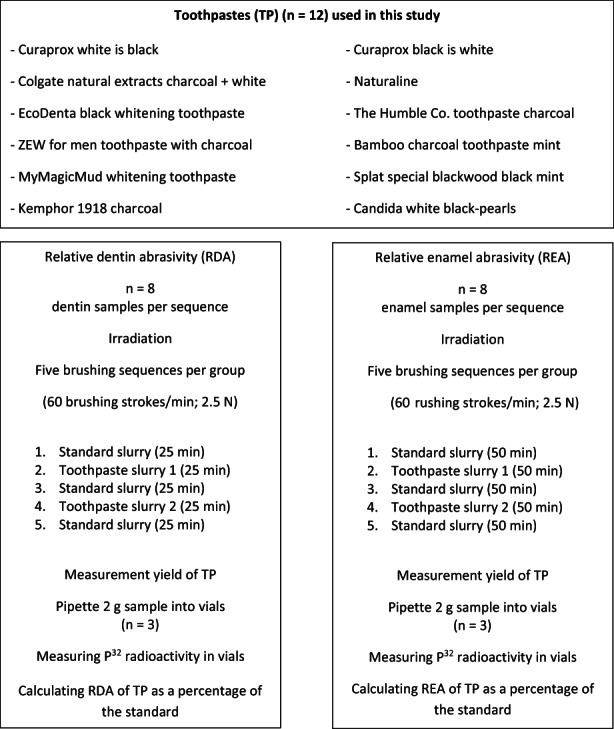
Before and after the brushing sequence with a charcoal toothpaste, a sequence was carried out using the standard abrasive. The values of the third sequence, with the standard abrasive, were used as a control brushing sequence for both pastes, which results in a total of five runs per sample group and two different charcoal toothpastes. This ‘sandwich technique’ was described in detail by Imfeld. 13 The respective standard slurry and toothpaste slurry were freshly prepared before each sequence. The standard slurry contained 90 g of silica abrasive particles (ISO‐Silica EXP 2480–1; Evonik Industries AG, Hanau‐Wolfgang, Germany), 450 g glycerol (Merck KGaA, Darmstadt, Germany) and 0.45 g silicon antifoaming agent (Sigma‐Aldrich, Saint Louis, USA). The toothpaste slurry contained 225 g of the respective charcoal toothpaste (Figure 1), 360 g of a saliva substitute with a similar buffering capacity as human saliva by Imfeld 13 and 0.45 g silicon antifoaming agent (Sigma‐Aldrich, Saint Louis, USA).
FIGURE 1.
Schematic representation of the procedure per sample group (two charcoal toothpastes).
Each day of the experiment, the slurries were freshly prepared, the samples were placed in the brushing machine and standard toothbrushes (Paro M43; Esro, Thalwil, Switzerland) were clamped in the machine. The contact pressure of the brushes was checked using a spring balance before each sequence and set to 2.5 N. The toothbrushes were replaced with new ones after each cycle. In total, 60 g of each of the corresponding slurry was filled into eight tubes and clamped in the machine, so that the samples were covered with slurry the entire time. To prevent abrasive particles from sticking to the bottom of the tube, a silicone cloth was clamped into the machine in addition to the brushes, which ensured that the slurry was constantly mixed during the brushing procedure. For the RDA measurements, the bovine dentin samples were abraded at a rate of 60 strokes per minute for 25 min (a total of 1500 strokes). One brush stroke corresponds to a complete back and forth movement of the brush over the sample. The same procedure was used for the REA measurement. However, the brushing was performed for 50 min (a total of 3000 brushstrokes). Between the sequences, all consumables were replaced with new ones, and the machine was cleaned well with distilled water. Figure 2 shows a simplified representation of the study design.
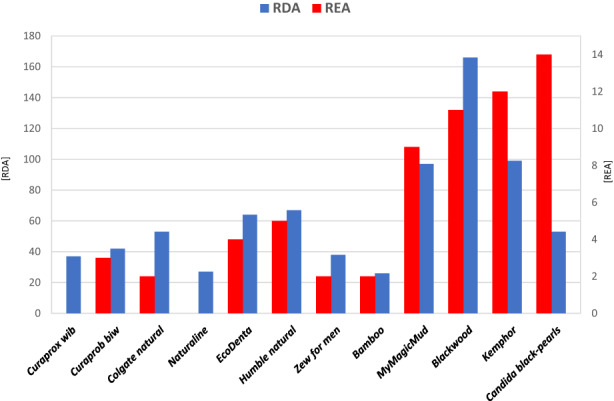
FIGURE 2.
Combined presentation of the mean RDA and REA values per paste (RDA: blue, y‐axis left, REA: red, y‐axis right). The standard deviation is not shown, and for the sake of simplicity, abbreviations were used for the paste names.
2.3. RDA and REA measurement
After the end of each sequence, the eight tubes were mixed for 1 min each (Ultra‐Turrax T25; Janke & Kunkel GmbH & Co KG, Staufen, Germany) to ensure the homogeneity of the now radioactive slurries. Two‐gram slurry from each tube was pipetted into a glass vial using an analytical balance (Sartorius Lab Instruments GmbH & Co. KG, Goettingen, Germany), and the weight was noted. This means that a total of 24 samples were produced per standard and paste to be measured. The weighed samples were each diluted with 1 ml of 2 M hydrochloric acid (AppliChem GmbH, Darmstadt, Germany) and 12 ml distilled water. The hydrochloric acid leads to the complete dissolution of the dental hard tissue contained in the samples and thus leads to the release of all the radioactivity contained in it. The samples were then stored for at least 24 h before being measured. The P32 radioactivity was measured in a Tri‐Carb A 2700 liquid scintillation analyser (Perkin Elmer, Waltham, USA). The device measures the P32 activity using counts per minute and converts it to decay per minute. However, some of the counts are lost due to the color, which should not be neglected with the dark charcoal toothpastes. For this reason, a so‐called measurement yield was carried out for each paste. For this purpose, 50 mg of the above‐mentioned artificial apatite that was sent along for irradiation was weighed into a total of five vials, and 2 g of non‐radioactive slurry was added (immediately after production). These samples were treated in the same way as already described above. Because of the known amount of radioactivity inside these samples, one ultimately knows how many counts are getting lost. This correction factor must be taken into account for the results of the samples. The results of the two sequences with the standard slurry for each sample, which were measured before and after the pastes, were averaged and normalized, respectively. The RDA and REA values of the respective charcoal toothpastes were expressed as a percentage of the values of the standard abrasive per sample, including the correction factor.
2.4. Statistical analysis
Each group contained eight samples and corresponded to a single charcoal toothpaste. The average value of all eight samples represents the RDA or REA value of the corresponding charcoal toothpaste. Due to the fact that if a statistical analysis would have been performed, the p‐values would have to be adjusted for multiple comparisons, statistical comparisons between the different charcoal toothpastes were not carried out. Comparing 12 pastes would have resulted in 66 comparisons, giving a p‐value of 0.00075. This would possibly lead to false non‐significant differences, although the RDA and REA values are clinically very different from each other.
3. RESULTS
Table 1 and Figure 2 show the RDA and REA values determined for the 12 different toothpastes within this study. In addition, the table was supplemented by the abrasives, RDA values and fluoride content specified by the manufacturers, when this information was available.
The following pastes scored the highest RDA values (± Standard deviation [SD]): Blackwood charcoal toothpaste (166 ± 9), Kemphor charcoal toothpaste (99 ± 7) and MyMagicMud whitening toothpaste (97 ± 11). And the lowest RDA values showed Bamboo charcoal toothpaste mint (26 ± 3) and Naturaline zahnpaste aktivkohle (27 ± 4).
The following pastes scored the highest REA values (± SD): Candida white black‐pearls (14 ± 3), Kemphor charcoal toothpaste (12 ± 2) and Blackwood charcoal toothpaste (11 ± 4). The lowest RDA values respectively below the detection limit showed that Curaprox white is black (0 ± 0) and Naturaline zahnpaste aktivkohle (0 ± 0).
It should be noted that charcoal‐containing toothpastes with a high RDA value also tended to have slightly higher REA values. The exception is Candida white black‐pearls with activated charcoal microgranules which had a moderate RDA value (53 ± 3), but the highest REA value (14 ± 3). The few available RDA values from the manufacturers agree well with the values determined in this study, even if they tended to be somewhat lower in this study.
According to the proposed classification by Hamza et al., 10 the various charcoal toothpastes would be classified as follows:
| RDA‐1: Low abrasion, RDA < 40 | RDA | REA‐1: Low abrasion, REA < 4 | REA |
|
Bamboo charcoal toothpaste mint Naturaline zahnpaste aktivkohle Curaprox white is black Zew for men toothpaste with charcoal |
26 ± 3 27 ± 4 37 ± 6 38 ± 4 |
Curaprox white is black Naturaline zahnpaste aktivkohle Colgate natural extracts charcoal & white Zew for men toothpaste with charcoal Bamboo charcoal toothpaste mint Curaprox black is white |
0 ± 0 0 ± 0 2 ± 1 2 ± 1 2 ± 1 3 ± 1 |
| RDA‐2: Moderate abrasion, RDA 40–80 | REA‐2: Moderate abrasion, REA 4–8 | ||
|
Curaprox black is white Colgate natural extracts charcoal & white Candida white black‐pearls EcoDenta black whitening toothpaste Natural toothpaste charcoal |
42 ± 5 53 ± 4 53 ± 3 64 ± 4 67 ± 6 |
EcoDenta black whitening toothpaste Natural toothpaste charcoal |
4 ± 4 5 ± 5 |
| RDA‐3: High abrasion, RDA > 80 | REA‐3: High abrasion, REA > 8 | ||
|
MyMagicMud whitening toothpaste Kemphor charcoal toothpaste Blackwood charcoal toothpaste |
97 ± 11 99 ± 7 166 ± 9 |
MyMagicMud whitening toothpaste Blackwood charcoal toothpaste Kemphor charcoal toothpaste Candida white black‐pearls |
9 ± 4 11 ± 4 12 ± 2 14 ± 3 |
4. DISCUSSION
Toothpastes are an important tool to mechanically remove plaque. Time and again, new and supposedly promising toothpastes find their way onto the market. Especially today in times of Instagram and so on where advertisements are practically unavoidable, the consumer is enticed with a large number of promises. The charcoal toothpastes are no exception. It is impressive how the charcoal toothpastes color the oral cavity black and then suddenly the white teeth appear while brushing your teeth. It is difficult to tell whether the teeth have really become whiter or whether the contrast between black and white is fooling us. So, do these toothpastes keep their promises, or do they even have harmful properties?
Brooks et al. 6 reported in a literature review that there are almost no or partially insufficient clinical and laboratory data on ‘charcoal‐based dentifrices’. With this study, the authors wanted to counteract the missing data by determining the RDA and REA values of such toothpastes. With these data, at least one statement can be made about the abrasiveness of such toothpastes.
The determination of RDA and REA values at the University of Zurich is a standardized procedure that was described by Imfeld in 2010. 13 Hamza et al. 10 have already discussed in a similar study with different types of toothpastes that the values can vary greatly from laboratory to laboratory. It is even the case that the determination of the same paste, in the same laboratory, but at different times, can show a deviation of 20%. 16 So even if the RDA measurement is a very standardized procedure, it would be advantageous to also indicate the laboratory where the corresponding value was determined and only compare values reported in the same study performed in the same laboratory.
In a review by Yassen et al., 17 it was noted that there are inconsistent data on whether bovine teeth are suitable substitutes for human teeth in dental research. Bovine teeth, however, have a larger surface area than human teeth and do not show any caries. This leads to an increase of the homogeneity of the samples compared with human teeth. 18 It is true that bovine and human teeth differ in some parameters, but because the RDA and REA values are each expressed relative to a known standard abrasive, this should have little impact. The question even arises, because the standard abrasive has a known value and the RDA und REA values are relative, whether it would not be even better—and more ecological—to use uniform artificial hydroxyapatite blocks, so that the comparability between the individual samples can be improved. This would also save a lot of preparation time for the creation of the samples, which makes the implementation more interesting for the user. The method certainly still has some optimization potential.
However, caution should be exercised in predicting the true clinical abrasiveness of the pastes based on their RDA and REA values. There are numerous factors that influence the true abrasiveness of the toothpastes in vivo. The brushing machine carries out uniform upward and downward movements with a set contact pressure. This brushing technique does not correspond to the situation in vivo and can lead to a modulation of the abrasivity. 10 , 19 A study by Attin et al. 20 showed that an erosive attack prior to toothbrushing results in significantly more tooth wear. But this fact alone would be too simple, because Wegehaupt et al. 15 were able to show that toothpastes containing a diamond abrasive cause more tooth wear on uneroded bovine enamel than on eroded bovine enamel. This is explained by the fact that the diamond particles cut worse through the softened substance but rather slide over it. 10 This shows the complexity and dependency of the type of abrasive contained in the various pastes. To the best of our knowledge, it has not yet been investigated whether toothpastes with activated charcoal cause more or less tooth wear after an erosive attack occurred. There are of course many other influencing factors, which will not be discussed further here. However, the RDA and REA values are only to be regarded as one of many factors that can be used to estimate the abrasiveness of toothpastes. In any case, they should not be used alone to draw conclusions about the clinical safety of toothpastes. 16 With the help of these values, no statement can be made about the cleaning performance either. It would certainly make sense to test the cleaning performance of all activated charcoal toothpastes, such as in the study by Hamza et al. 21 where the toothpaste ‘Curaprox black is white’ was already tested. The above‐mentioned study shows that the activated charcoal toothpaste showed a high cleaning efficacy (85.2%) with a moderate abrasivity (RDA = 50 specification of the manufacturer and 42 ± 5, within this study). However, some other studies showed no clinically significant whitening effect of activated charcoal powder. 5 , 9 Something must be differentiated, namely the cleaning performance is about whether the toothpaste is able to remove extrinsic (stored on the teeth; outside) stains. With bleaching, however, intrinsic discoloration embedded in the tooth is also lightened, the overall tooth color is therefore lighter. It can be somewhat misleading for the consumer if the widely used term ‘whitening effect’ on charcoal toothpastes only means the removal of extrinsic stains. In addition, activated charcoal toothpastes usually contain other abrasives, which is why it is difficult to assess the sole influence of activated charcoal.
Many of the toothpastes tested in this study also contain the abrasive hydrated silica (SiO2 · nH2O) in addition to the activated charcoal. It is therefore difficult to estimate how much of the abrasiveness has to be attributed to which abrasive. In the study by Hamza et al., 10 pastes that only contain hydrated silica have RDA values between 26 and 100 and REA values between 1 and 19. This agrees closely with the values in this study where the toothpastes with additional activated charcoal have RDA values between 26 and 99 and REA values between 2 and 14. The only outlier is the toothpaste ‘Blackwood charcoal toothpaste (SPLAT, London, England)’ with an RDA value of 166 ± 9. The explanation for the wide range of RDA and REA values probably lies in the shape and size of the abrasive particles contained. 22 , 23 , 24 If only the toothpaste that only contains activated charcoal as an abrasive (Naturaline zahnpaste aktivkohle; Coop Genossenschaft, Basel, Switzerland) is considered, an RDA value of 27 ± 4 and an REA of 0 (not in the measurable range) were detected. The question therefore arises as to whether activated charcoal has any influence, at least on the REA value. Activated charcoal is mostly carbon (>90%). Some activated charcoals are made from bamboo, while others are made from coconut shells. The influence on the origin of the activated charcoal in the pastes is unclear and probably also depends more on the processing and the corresponding size and shape of the particles. The only charcoal toothpaste which contained other abrasives such as bentonite and clay (MyMagicMud whitening toothpaste, Carbon & Clay Co., Texas, USA) resulted in rather high RDA and REA values of 97 and 9, respectively. However, these values were also achieved by other pastes that did not contain these two ingredients. The Blackwood charcoal toothpaste (SPLAT, London, England) had the highest RDA value of 166 ± 9, but with an REA value of 11 ± 4 not the highest within this study. Conversely, the Candida white black‐pearls (Mibelle AG, Buchs, Switzerland) with the highest REA value of 14 ± 3 had only a moderate RDA value of 53 ± 3. This fact clearly shows that it is very important to measure both values, as they often do not correlate with each other.
A somewhat worrying trend is the lack of fluoride compounds in many of the investigated pastes. This is largely due to the pastes being sold as natural, ecofriendly or organic. In this study, 50% of the charcoal pastes available in Switzerland are fluoride‐free. Internationally, the number of available fluoride‐free toothpastes is even higher. The systematic review by Brooks et al. 6 showed that only 8% of the charcoal toothpastes contain fluoride compounds. There are numerous studies showing the positive effects of fluoridated table salt and fluoridated dentifrices. 8 , 25 , 26 , 27 The effects of fluoride compounds are very versatile. Their influence on the dental hard tissue is the promotion of remineralization, the reduction of acid solubility, inhibition of demineralization and lowering of the critical pH value. 28 , 29 , 30 , 31 In addition, fluoride is assumed to have an influence on the bacterial metabolism, which means that there is a doubly positive caries‐preventive effect. 28 However, most of the findings on the antibacterial mechanisms of action of fluorides come from in vitro studies and have therefore not yet been clinically confirmed. 32 As Paracelsus realized as early as the 15th century and described with his world‐famous quote ‘All things are poison, and nothing is without poison; but the dose makes it clear that a thing is not a poison’, this of course also applies to fluorides. The ‘probably toxic dose (short PTD)’ of fluorides is 5.0 mg F−/kg body weight. 8 , 33 An adult with 70 kg body weight would have to intake 240 g of a toothpaste containing 1450 ppm F−; in other words, has to eat three full toothpaste tubes each with 75 g content. It is clear that this looks different with a child of just 15 kg, which is why children's toothpastes also have a lower fluoride content of 500 ppm F−.
5. CONCLUSION
In summary, it can be concluded that the charcoal toothpastes have similar RDA and REA values as already known conventional toothpastes from other studies. The ranges for the RDA and the REA values are 26–166 and 0–14, respectively. To substantiate the safety and efficacy claims of charcoal toothpastes, more studies are needed. However, the lack of fluoride compounds in many of the charcoal toothpastes can have a harmful effect for the consumers. It is very important to educate patients accordingly.
6. CLINICAL RELEVANCE
6.1. Scientific rationale for study
Activated‐charcoal‐containing toothpastes still need to be further examined. There is little literature of the mechanical properties of such pastes.
6.2. Principal findings and practical implications
Already known commercially available toothpastes and charcoal toothpastes do not differ in their range of RDA and REA values. However, it should be noted that activated charcoal is usually not the only abrasive contained and that the abrasiveness is strongly dependent on the quantity, size and shape of the abrasive particles. Many of these charcoal toothpastes, which are advertised as natural, also contain no fluoride, which can have a negative impact on the patient's caries activity.
AUTHOR CONTRIBUTIONS
Manuel J. Zoller, Wrote the manuscript, performed the experiments in fulfillment of requirements for a doctoral degree. Blend Hamza, Contributed substantially to discussion, proofread the manuscript. Claudia Cucuzza, Supported and organized the implementation of the experiments. Andrea Gubler, Supported and organized the implementation of the experiments. Thomas Attin, Research idea, contributed substantially to discussion, proofread the manuscript. Florian J. Wegehaupt, Research idea, hypothesis, experimental design, contributed substantially to discussion and writing the paper, proofread the manuscript.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
FUNDING INFORMATION
No external funding was obtained for this study.
ACKNOWLEDGEMENT
Open access funding provided by Universitat Zurich.
Zoller MJ, Hamza B, Cucuzza C, Gubler A, Attin T, Wegehaupt FJ. Relative dentin and enamel abrasivity of charcoal toothpastes. Int J Dent Hygiene. 2023;21:149‐156. doi: 10.1111/idh.12634
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- 1. Marketos SG, Androutsos G. Charcoal: from antiquity to artificial kidney. J Nephrol. 2004;17:453‐456. [PubMed] [Google Scholar]
- 2. Sanchez N, Fayne R, Burroway B. Charcoal: an ancient material with a new face. Clin Dermatol. 2020;38:262‐264. [DOI] [PubMed] [Google Scholar]
- 3. Juurlink DN. Activated charcoal for acute overdose: a reappraisal. Br J Clin Pharmacol. 2016;81:482‐487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Newsom SWB. Hygiene and the ancient romans. Br J Infect Contr. 2004;5:25‐27. [Google Scholar]
- 5. Palandi SDS, Kury M, Picolo MZD, Coelho CSS, Cavalli V. Effects of activated charcoal powder combined with toothpastes on enamel color change and surface properties. J Esthet Restor Dent. 2020;32:783‐790. [DOI] [PubMed] [Google Scholar]
- 6. Brooks JK, Bashirelahi N, Reynolds MA. Charcoal and charcoal‐based dentifrices: a literature review. J Am Dent Assoc. 2017;148:661‐670. [DOI] [PubMed] [Google Scholar]
- 7. Nakata T, Kitasako Y, Sadr A, Nakashima S, Tagami J. Effect of a calcium phosphate and fluoride paste on prevention of enamel demineralization. Dent Mater J. 2018;37:65‐70. [DOI] [PubMed] [Google Scholar]
- 8. Wegehaupt F, Menghini G. Fluoride update. Swiss Dent J. 2020;130:677‐683. [DOI] [PubMed] [Google Scholar]
- 9. Franco MC, Uehara J, Meroni BM, Zuttion GS, Cenci MS. The effect of a charcoal‐based powder for enamel dental bleaching. Oper Dent. 2020;45:618‐623. [DOI] [PubMed] [Google Scholar]
- 10. Hamza B, Attin T, Cucuzza C, Gubler A, Wegehaupt FJ. RDA and REA values of commercially available toothpastes utilising diamond powder and traditional abrasives. Oral Health Prev Dent. 2020;18:807‐814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Machla F, Mulic A, Bruzell E, Valen H, Stenhagen ISR. In vitro abrasivity and chemical properties of charcoal‐containing dentifrices. Biomater Investig Dent. 2020;7:167‐174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Addy M. Tooth brushing, tooth wear and dentine hypersensitivity ‐ are they associated. Int Dent J. 2005;55:261‐267. [DOI] [PubMed] [Google Scholar]
- 13. Imfeld T. Standard operation procedures for the relative dentin abrasion: (RDA) method used at Zurich university. J Clin Dent. 2010;21:S11‐S12. [Google Scholar]
- 14. Grabenstetter RJ, broge RW, Jackson FL, Radike AW. The measurement of the abrasion of human teeth by dentifrice abrasives: a test utilizing radioactive teeth. J Dent Res. 1958;37:1060‐1068. [DOI] [PubMed] [Google Scholar]
- 15. Wegehaupt FJ, Hoegger VGM, Attin T. Abrasion of eroded and sound enamel by a dentifrice containing diamond abrasive particles. Swiss Dent J. 2017;127:634‐639. [DOI] [PubMed] [Google Scholar]
- 16. González‐Cabezas C, Hara AT, Hefferren J, Lippert F. Abrasivity testing of dentifrices ‐ challenges and current state of the art. Monogr Oral Sci. 2013;23:100‐107. [DOI] [PubMed] [Google Scholar]
- 17. Yassen GH, Platt JA, Hara AT. Bovine teeth as substitute for human teeth in dental research: a review of literature. J Oral Sci. 2011;53:273‐282. [DOI] [PubMed] [Google Scholar]
- 18. Zoller MJ, Procopio A, Attin T, Wegehaupt FJ. Homemade modification of salad dressings to reduce their erosive potential. Oral Health Prev Dent. 2021;19:433‐440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Imfeld T, Sener B, Lutz F. Mechanische Wirkung von in der Schweiz marktführenden Zahnpasten auf Dentin. Acta Med Dent Helv. 1998;3:54‐59. [Google Scholar]
- 20. Attin T, Koidl U, Buchalla W, Schaller HG, Kielbassa AM, Hellwig E. Correlation of microhardness and wear in differently eroded bovine dental enamel. Arch Oral Biol. 1997;42:243‐250. [DOI] [PubMed] [Google Scholar]
- 21. Hamza B, Tanner M, Attin T, Wegehaupt FJ. Dentin abrasivity and cleaning efficacy of novel/alternative toothpastes. Oral Health Prev Dent. 2020;18:713‐718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Singh RP, Sharma S, Logani A, Shah N, Singh S. Comparative evaluation of tooth substance loss and its correlation with the abrasivity and chemical composition of different dentifrices. Indian J Dent Res. 2016;27:630‐636. [DOI] [PubMed] [Google Scholar]
- 23. De Boer P, Duinkerke AS, Arends J. Influence of tooth paste particle size and tooth brush stiffness on dentine abrasion in vitro. Caries Res. 1985;19:232‐239. [DOI] [PubMed] [Google Scholar]
- 24. Mahmood A, Mneimne M, Zou LF, Hill RG, Gillam DG. Abrasive wear of enamel by bioactive glass‐based toothpastes. Am J Dent. 2014;27:263‐267. [PubMed] [Google Scholar]
- 25. Menghini GD, Steiner M, Marthaler TM, Bandi A. Caries occurrence in schoolchildren of the canton of Glarus in 1974 to 1992: the effect of the use of fluoridated salt. Schweiz Monatsschr Zahnmed. 1995;105:467‐473. [PubMed] [Google Scholar]
- 26. Nordström A, Birkhed D. Preventive effect of high‐fluoride dentifrice (5,000 ppm) in caries‐active adolescents: a 2‐year clinical trial. Caries Res. 2010;44:323‐331. [DOI] [PubMed] [Google Scholar]
- 27. Moberg Sköld U, Petersson LG, Lith A, Birkhed D. Effect of school‐based fluoride varnish programmes on approximal caries in adolescents from different caries risk areas. Caries Res. 2005;39:273‐279. [DOI] [PubMed] [Google Scholar]
- 28. Buzalaf MAR, Pessan JP, Honório HM, Ten Cate JM. Mechanisms of action of fluoride for caries control. Monogr Oral Sci. 2011;22:97‐114. [DOI] [PubMed] [Google Scholar]
- 29. Rošin‐Grget K, Peroš K, Sutej I, Bašić K. The cariostatic mechanisms of fluoride. Acta Med Acad. 2013;42:179‐188. [DOI] [PubMed] [Google Scholar]
- 30. Rølla G, Saxegaard E. Critical evaluation of the composition and use of topical fluorides, with emphasis on the role of calcium fluoride in caries inhibition. J Dent Res. 1990;69 Spec No:780‐5; discussion 820;69:780‐785. [DOI] [PubMed] [Google Scholar]
- 31. Robinson C. Fluoride and the caries lesion: interactions and mechanism of action. Eur Arch Paediatr Dent. 2009;10:136‐140. [DOI] [PubMed] [Google Scholar]
- 32. Koo H. Strategies to enhance the biological effects of fluoride on dental biofilms. Adv Dent Res. 2008;20:17‐21. [DOI] [PubMed] [Google Scholar]
- 33. Whitford GM. Fluoride in dental products: safety considerations. J Dent Res. 1987;66:1056‐1060. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.