

Abstract
Background
Play is an essential component of children's development. Children with intellectual disability tend to have poor socioemotional abilities and impaired play. This study examined the effects of a medical/therapeutic clowning play intervention on the playfulness of children with intellectual disability.
Method
Two medical clowns facilitated a play intervention in a preschool classroom setting with a total of 52 children with intellectual disability. We compared before and after two groups that received the intervention: group 1 met the medical clowns once a week for 6 months (long‐intervention group) and group 2 for 3 months (short intervention group). Children's functioning was assessed using the Vineland Adaptive Behaviour Scales. Children's playfulness was scored using the Test of Playfulness observational assessment. A teachers' focus‐ group was used to gather additional information on the clowns' work.
Results
Children's playfulness increased significantly at the end of the intervention, whereas the improvement in the playfulness scores of group 1 was significantly larger than those of group 2 (t 50 = −4.82, p < .001). The teachers' focus group revealed additional benefits of the medical clowns' work.
Conclusion
The results shed light on the play and playfulness of children with intellectual disability and the possible contribution of a clowning play intervention to their development.
Keywords: children, intellectual disability, intervention, play; playfulness; medical clowns
“The most effective kind of education is that a child should play among lovely things.”
Plato
1. INTRODUCTION
Children's play is intrinsic to their well‐being. Their natural disposition to become emotionally and socially involved in the course of play lies at the foundation of their development (Golinkoff et al., 2006; Sutton‐Smith, 1997). Play is an essential part of their first experiences of the world, and vital for their ability to form relationships and tackle new learning tasks (Youell, 2008). Preschool children's play abilities predict their emotional knowledge, expressiveness, emotional regulation (Lindsey & Colwell, 2013) as well as social skills (Harris, 2000). Medical clowns are ‘experts’ at free play, aiming to create playful interaction with a variety of populations whom they work with (Sridharan & Sivaramakrishnan, 2016). In the present study we examined the possible contribution of medical clowns in promoting the playfulness of children with intellectual disability.
Intellectual disability refers to neurodevelopmental disorders characterised mainly by substantial delays in cognitive development (American Psychiatric Association, 2013). Children with intellectual disability exhibit deficits in their play that parallel their socioemotional difficulties and deficits in other areas of development (Malone & Langone, 1999; Walters & Kaufman Blane, 2000). Children with intellectual disability are less playful than their typically developing peers, and exhibit inferior play skills (Hamm, 2006; Okimoto et al., 2000), tending to solitary play and being less socially interactive (Guralnick & Groom, 1987). This is especially worrisome in light of the importance of play for children's development. If play and playfulness are not established in children's early experiences, it may compromise their emotional, psychological, and cognitive development (Youell, 2008).
Previous studies have shown that issues like affect regulation, social competence, and sense of autonomy, all of which are practiced during children's play, may be of significant importance to the adjustment of children with intellectual disabilities to the everyday world (Schuengel, & Janssen, 2006; Sigman et al., 1999). Indeed, they are likely to matter even more for children with intellectual disabilities than for typically developing children (Baker et al., 2007). Sensitive responses on the part of the caretaker, affective warmth, and following the child's lead during play have been shown to be significant for positive outcomes in children with intellectual disabilities: greater child persistence, mastery motivation, and improved social skills (Guralnick, 2016).
Medical clowns use free play as their main method to interact and bring joy, laughter, and relief to the population with whom they work with (Sridharan & Sivaramakrishnan, 2016). Since the introduction of clowns into New York City hospitals in the 1980's, the profession of medical clowning has developed and spread to a wide variety of institutions serving different functions. Consequently, at present medical clowns can be found working with children and adults suffering from diverse conditions in hospitals, geriatric and mental health centers (Warren & Spitzer, 2011; Raviv, 2018; Barkmann et al., 2013) and have joined emergency teams in communities in areas of natural disaster (Raviv, 2012). In recent years, the work of medical clowns has been accompanied by a growing number of empirical studies. A meta‐analysis of 19 studies about medical clowns has found that they play a significant role in reducing stress and anxiety levels in children admitted to hospitals as well as in their parents (Sridharan & Sivaramakrishnan, 2016).
The alliance between the clown and the hospital patient or the disabled child is based on folly, reversal of order, and self‐ridicule, the main goal being the establishment of a playful interaction with the child. Together with that, the clown interaction is characterised by sensitive and profound emotional communication that aims first and foremost to enable the other person to join the playful encounter. As play specialists, the clowns create a safe and comfortable play environment that enables children (and adults) to participate in playful interactions. Their flexibility, use of humour, play with hierarchy (i.e., ‘I am more silly than you are’), are some of the unique characteristics used to draw people in to play (Raviv, 2018). Thus, medical clowns can be seen as the ultimate agents of free play, practicing spontaneity and creativity while involving and motivating other people to join their play (Citron, 2011), and thereby may contribute to advance play and playfulness.
There is a deep resemblance between medical/therapeutic clowning and children's play, which is expressed in the natural affinity between children and clowns. Medical clowns working in paediatric units allow child patients to engage in play, enabling them to experience control, flexibility, and creativity over their painful reality (Koller & Gryski, 2008). The clowns' activity offers the children an opportunity to engage in play, free of functional purposes or didactic aims. Instead, the clown's play is aimed at mutual enjoyment. The clown's interaction facilitates verbal and non‐verbal communication, improves mood and attitude, and enhances the expression of laughter, joy, imagination, and creativity (Meiri et al., 2016).
In recent years, research has begun to examine the possible contributions of medical clowning to children with varied disabilities. A pilot study by Kingsnorth, Blain, and McKeever (2011) examined the effects of medical clowning on hospitalised children with physical and intellectual disabilities, investigating physiological signals, and behavioural and emotional responses as measures of responsiveness to the clowns. Results showed that the medical clowns had an overall positive effect on the mood and wellbeing of all children, including those with mild and profound disability, with reports of increased smiling and laughing, positive mood changes, and decreased grimacing (Kingsnorth et al., 2011). A more recent study showed that a medical clowning intervention with children with autism spectrum disorder (ASD) resulted in a significant decline in the symptomatology of ASD behaviour, including stereotypic behaviour (Shefer, et al., 2019). This is one of the few studies that examined the possible contribution of medical clowns beyond the hospital setting, on measures other than stress and anxiety. Similarly, in the present study we aimed to examine the effect of medical/therapeutic clown on the children's wider functioning as expressed via their playfulness, and beyond the parameters of mood change or anxiety reduction.
The playful essence of the clowns' interaction with children and its therapeutic effects led us to examine their possible contribution to the playfulness of children with intellectual disability. Play interventions have linked playfulness with socio‐emotional development, growth of language and motor skills, creativity, and problem solving (Hamm, 2006). Yet, research has shown that parents and educators of children with intellectual disability tend to abandon playing with them in favour of didactic and directive interactions (Al‐Yagon & Margalit, 2012; Lane & Mistrett, 1996). Unlike typically developing children or children with autism (i.e., Siller et al., 2013), there is little research on the play of children with intellectual disabilities and interventions to promote it. The present study suggests that medical/therapeutic clowning can serve as an early play intervention to promote and advance the play, playfulness, and socioemotional development of children with intellectual disability.
Playfulness refers to the disposition to engage in play (Barnett, 1991), and it captures both the child's approach and the mechanism of play (Pinchover, 2017). Bundy (1997) identified four primary characteristics of play that constitute playfulness: (a) intrinsic motivation, manifest when players play for the sake of playing, not for any external purpose or reason other than the play itself; (b) internal control, manifest when players choose and control their play: whom to play with, what to play, and the limits of the play (what is play and what is not play); (c) freedom to suspend reality, describing pretend play that is not real, and which occurs outside ordinary reality, although maintaining a relation with it (Bundy, 1997); and (d) framing, describing the ability of children to frame their play, giving and reading cues signalling that ‘this is play’ (Bateson, 1971). Bundy operationalised these four elements of playfulness, based on play theory and research, into an observation‐based assessment tool, the Test of Playfulness (ToP) (Bundy, 2010), which makes possible the examination of playfulness for typically developing children and children with disabilities (Muys et al., 2006). In the present study, we examined the possibility of enhancing playfulness among children with intellectual disability using medical clown intervention.
1.1. Hypotheses
A weekly intervention of medical/therapeutic clowning will show its positive effect on the level of playfulness of children with intellectual disability. Group 1 will receive the intervention for 6 months, (Long‐Intervention group; LIG) and group 2 for 3 months (Short‐Intervention Group; SIG):
At the end of the intervention, there will be a positive increase in children's playfulness compared to the beginning of the intervention.
The increase in the level of children's playfulness will be significantly larger in the LIG than in the SIG.
The hypothesis will be examined in light of the severity of the children's disability, as measured by their adaptive behaviour scores.
2. METHOD
2.1. Research design
To examine the possible effects of the clown intervention on preschool children with intellectual disability, we used a 2 (before and after) × 2 (two study groups each receiving different amount of intervention) design. Hence, we used a pretest‐posttest assessment using standardised measures, comparing how the two groups differ on the amount (dose) of clown intervention they received. In addition, we facilitated a focus group of the kindergarten teachers in order to get their perspective on the possible contribution of the clowns' work.
Two kindergarten centers participated in the study. One center received a 6‐month intervention and the other 3‐months. A design that compares the length of the two interventions was chosen for ethical considerations to ensure that all participating children benefit from the clown intervention. This was the design that the education authority of the kindergartens preferred.
Parents provided informed consent for their children's participation in the study. Approval was received from the University of Haifa Ethics Committee (register number 255/15 granted on 9/4/2015) and from the Chief Scientist of the Israel Ministry of Education (register number 9620 granted on 6/21/2017).
2.2. Participants
The children were recruited from two kindergarten centers for children with intellectual disability. We contacted the parents and described the research procedure and its importance. We asked parents to grant permission for their child to participate in the study, and those who agreed signed a consent form. The parents of all the children except one agreed to the participation of their child in the study. As agreed with the parents who objected their child participation, arrangements were made for the child to participate in the clown intervention, but the participation of the child was not measured or documented.
For the initial sample size calculation, we used G*Power 3.1 (Faul et al., 2009) and we were expecting a moderate to strong effect size (Cohen's d ~ .7) and a power of 0.8, using a sample of 26 participants per group.
The study included eight preschool classes at two education centers. Fifty‐two children participated in the study, of whom 23 were in the LIG (mean age = 3.91, SD = .79; 65% boys) and 29 in the SIG (mean age = 4.10, SD = 1.21; 72% boys). The range of their chronological age was 3–7 years, and all had been diagnosed with intellectual disability before entering the kindergarten, in addition to other conditions and developmental disabilities such as cerebral palsy and ASD. Furthermore, 47% of the children received medications on a regular basis because of various medical problems, and 43% received other treatments such as art therapy, hydrotherapy, and physiotherapy; 67% of the children either had only one sibling or were an only child.
Participating in the study's focus group were eight special education teachers who gave their full consent to participate in the study. Their age ranged from 28 to 66 years (M = 47.75, SD = 14.78). The native language of five of the teachers was Russian, two teachers were native Hebrew speakers, and one teacher's native language was Arabic. Six of the teachers had two or more children. All the teachers had bachelors' degrees, and five of them a master's degree. The teacher's experience at their work ranged from 7 to 38 years (M = 20, SD = 10.45). In the years in which the study was conducted, the teachers were responsible for 8–10 children per class.
2.3. Procedure
At the beginning of the study, after receiving consent forms from all the parents, we interviewed the kindergarten teachers using the Vineland Adaptive Behaviour Scales (VABS) to assess each child in their class and obtain an indication of the level of the child's functioning and adaptive behaviour. The clown intervention began after these interviews.
Two trained medical clowns interacted with up to eight children in each class in a 30‐min session once a week. The meetings lasted for 6 months for the LIG and 3 months for the SIG. The pair of clowns visited the classrooms equipped with toys, musical instruments, and props to stimulate play. The interactions with the clowns were recorded with two cameras for assessment purposes and intervention fidelity. In addition, the clowns sent weekly reports about the sessions. Three months following the intervention we conducted a focus group with the kindergarten teachers to get their impression on the effect of the clowns' work on the children and the teachers.
We analysed two 30‐min videotaped sessions from the beginning (T1) of the intervention and two sessions from the end (T2) using the ToP observational assessment for each child in both intervention and control groups.
2.3.1. Clowns' training
The clowns, one female and one male, in their early thirties, were both graduates of the Medical Clowning Academic Training Program of the Theatre Department at the University of Haifa. A year before the beginning of this study, they were interns in the same kindergarten center and developed their skills working with children with intellectual disabilities. Before the beginning of the study, the clowns underwent a 3‐day training to prepare them for working in the kindergarten as part of the present study. The children who participated in the study were not exposed to the clowns during their internship, and children who worked with the clowns during the internship were excluded from the study.
2.3.2. Clowns' activity
The activity of the clowns took place in a group setting. The clowns used various techniques aimed at engaging the children in play. In the beginning the clowns aimed at one‐on‐one interactions, gradually engaging the children in group interactions. Examples of the games and techniques used were mirroring, manipulating imaginary objects, peek‐a‐boo, ball games, games of tag, pretend play, singing a good morning song, dancing with the children and allowing each child to give a short solo performance, racing with toy cars, playing with objects, and more (for a detailed description of the medical clowns' techniques, see, Feniger‐Schaal et al., 2020).
2.3.3. Supervision
The clowns received monthly supervision by a senior medical clown and weekly supervision by a member of the kindergarten staff.
2.4. Measures
2.4.1. Vineland Adaptive Behaviour Scales (VABS) second edition: Parent/caregiver rating form (Vineland‐II; Sparrow et al., 2006)
Vineland‐II is a standardised test used to assess adaptive behaviour in four domains: communication, daily living skills, socialisation, and motor skills. It provides standard scores in each of the domains and an overall adaptive behaviour score with an average of 100 and SD of 15. In this study, the children's adaptive behaviour was assessed using the overall score. VABS has a teacher form, but it is designed for school‐aged children, whereas most of the children participating in the present study had a mental age lower than that of school children and could not be assessed using this form because of the floor effect. Therefore, we used the parent/caregiver rating form rather than the teacher's version because it is valid for children aged 6 months and older, which suited our sample.
The kindergarten schoolteachers completed the VABS at the beginning of the intervention. The adaptive behaviour score is part of the standardised assessment for intellectual disability. We used the VABS in this study because it is a relatively easy way to obtain an indication of the children's level of disability based on a structured interview with the teachers.
2.4.2. Test of playfulness version 4.2 (ToP; Bundy, 2010)
ToP is a standardised observational assessment intended to evaluate and score children at play from the age of 6 months to 18 years. The ToP comprises 30 items rated on a 4‐point scale (0–3) that reflect the extent (ext.), intensity (int.), and skill of the child at free play. The ToP assesses the children's playfulness comprehensively by operationalising four elements of playfulness, based on play theory and research: motivation for play, control of play, use of pretence, and framing. For example, the children's motivation is examined based on their engagement and participation (ext. and int.), as well as their positive affect during play (int.), reflecting the intrinsic fun of play. The children's control and choices at play are assessed by their ability to initiate (skill) and modify (skill) the games, as well as their ability to socially interact at play (ext., int., and skill), support (skill), and share (skill) with others. The children's ability to use pretence (skill) is expressed also through the use of humour (skill) and mischief (skill). The framing of the play is measured through the children's use of signalling and giving cues to others (ext. and skill) and their ability to read cues (skill) (Skard & Bundy, 2008). The diverse items scored on the ToP offer a multidimensional assessment of the complex nature of a child's playfulness. Studies have established the reliability and validity of the ToP for use with children with various disabilities: physical disabilities (Harkness & Bundy 2001; Hess & Bundy 2003), intellectual disability, developmental disabilities, cerebral palsy (Hamm, 2006; Okimoto et al., 2000), and ASD (Bass & Mulick, 2007). The reliability and validity of ToP have been established according to the Rasch measurement model (Wright & Stone, 1979) for children with and without disabilities (Hamm, 2006; Okimoto, Bundy, & Hanzlik, 2000). ToP has been used to measure the effectiveness of adult‐led play interventions (Muys et al., 2006).
To assess each child's playfulness during the clown intervention in the classroom, we scored two different videotaped 30‐min group sessions from the beginning and end of the intervention (a total of four sessions for each child), verifying that an adequate amount of interaction was observed for each child (originally, ToP is scored based on a single 15‐minute play episode). Hence, it may be that one video record portrayed all the children in a specific kindergarten in an adequate way but it can also be that we needed to choose a different video that gets a better view of a certain child, either from the second camera or from a different session.
We made several adaptations to the ToP for the present study. Seven items were deemed inapplicable or irrelevant to all the clown interactions and therefore removed: safe (ext.), process (ext.), enters (skill), creative use of objects (ext. and skill), and interaction with objects (int. and skill). ToP is tolerant of missing data, and items that are removed do not affect the scoring or validity of ToP (Fischer & Molenaar, 1995). Because of the heterogeneity of the participants, we modified the skillfulness scale to allow the most disabled children, in view of their limited abilities, to receive credit for their attempts to participate. Passivity is a prevalent characteristic of children with developmental intellectual disabilities (Niccols et al., 2012), therefore, to acknowledge the children's playfulness, however minimal and limited it may be, we chose to give children a positive score even when they were passively engaged by the clowns. The skillfulness scores (0–3) were adapted as follows: 0—Unskilled, 1—The child shows slight skill (most of the time participating passively), 2—The child shows moderate skill (participating actively some of the time), and 3—Highly skilled (the child participates actively most of the time). This change was applied to the following items scored for skillfulness: actively engaged; modifies activity; engages in playful mischief; engages in social play; supports play of others; responds to other's cues; and transitions from one play activity to another (the guidelines for the ToP adaptation can be obtained from the first author).
To avoid bias, the tapes were scored in random order and tapes from the same class were not scored consecutively. The coders were blind to whether the observation took place before or after the intervention. The ToP ratings for each child were entered into the ToP Keyform, an Excel form that converts the ratings into a total playfulness score based on the relative difficulty of each item (the Keyform was obtained from Bundy, the developer of ToP), established by previous research using ToP (Skard & Bundy, 2008). The raters watched each video twice, taking notes about the interactions between the clowns and the children. After watching two of the videos involving each child, the raters scored the ToP score sheet (Bundy, 2010).
2.5. Interrater reliability
We compared the coding of two raters on 20% of the ToP videotapes and determined interrater reliability using the interclass correlation coefficient (ICC) for consistency of independent ratings (McGraw & Wong, 1996). Interrater reliability was 0.83, with 95% confidence intervals.
2.6. Focus group
Three months after the end of the intervention, eight of the kindergarten teachers met to serve as a focus group and discuss their impressions of the clowns' work. The focus group was co‐conducted by the two leading researchers of the study, who have extensive experience in facilitating focus groups. The group members were asked the following questions:
Can you tell us your impression of the clowns' work?
In your opinion, was there any specific effect of their work on the children or on you?
Is there anything else you would like to share regarding your encounter with the clowns when they worked in your class?
The focus group lasted 90 min. We recorded the discussion and transcribed it.
The thematic analysis approach (Braun & Clarke, 2006) was applied to the text in order to identify subjects and themes (more recently referred to as reflexive thematic analysis; Braun & Clark, 2019). The analysis process six stages: (1) Familiarisation with the data; (2) Generating preliminary codes; (3) Searching for themes that contain significant information related to the research question; (4) Reviewing the themes; (5) Defining and naming of themes which involves identifying the essence of each theme using quotes from the text; (6) Writing and reporting, and presenting a coherent summary of the findings (Braun & Clarke, 2006, 2019). Two coders were involved in identifying the themes that emerged.
3. RESULTS
3.1. Change in observed playfulness following the clown interventions
To assess the change in observed playfulness following the interventions, we first examined the difference between the ToP scores at T1 and T2, in each group separately. Table 1 presents the descriptive statistics for each group.
TABLE 1.
Descriptive statistics for the study groups
| ToP T1 | ToP T2 | Difference in ToP | Adaptive behaviour | |||||
|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | |
| Long intervention | −1.64 | 0.60 | 0.55 | 0.71 | 2.19 | 0.80 | 52.75 | 13.07 |
| Short intervention | −1.18 | 0.68 | −0.03 | 0.59 | 1.15 | 0.75 | 49.02 | 19.53 |
For the LIG, ToP at T2 was significantly higher than at T1 (t 22 = −13.10, p < .001, Cohen's d = 2.73, 95% CI [−2.54, −1.85]). Similarly, for the SIG, ToP at T2 was significantly higher than the mean of observed playfulness at T1 (t 28 = −8.30, p < .001, Cohen's d = 1.54, 95% CI [−1.44, −0.87]).
Figure 1 presents the changes in the two groups, comparing T1 and T2.
FIGURE 1.
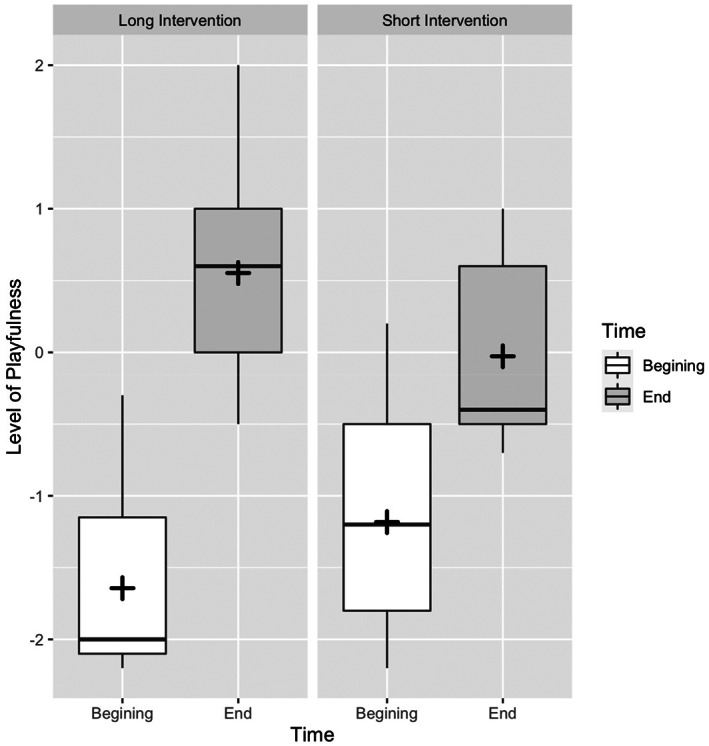
Difference between the LIG and SIG at the beginning and the end of the intervention. The middle line of the boxplot is the group median, and the cross is the group mean. The upper and lower boundaries of the box are the third and first quartiles, respectively. Whiskers mark the minimum and maximum values of the group
3.1.1. Differences between groups in intervention effectiveness
To assess the effects of the interventions without being biased by their baseline levels, we calculated the T2‐T1 difference of the ToP scores for each group. We found that the ToP difference score in the LIG was significantly larger than in the SIG (t 50 = −4.82, p < .001).
Gender and group differences. To examine whether the difference between groups may be due to gender‐related differences in the effects of the interventions, we compared the ToP difference scores of boys (M = 1.56, SD = 0.89) and girls (M = 1.74, SD = 1.02), which were found to be non‐significant (t 50 = −0.66, p > .05).
3.1.2. Adaptive behaviour and group differences
Examining the relation between the children's adaptive behaviour scores and playfulness level, we found no significant correlations between children's Vineland scores (M = 50.35, SD = 17.42) and ToP scores across groups at T1 (r = .25, p > .05), at T2 (r = .19, p > .05), and with respect to the ToP difference score (r = −.03, p > .05).
To examine the effect of differences in adaptive functioning on the ToP difference score, in both groups, we performed an ANCOVA with the type of group (long or short intervention) as the independent variable, the adaptive behaviour score as a covariate, and the difference in ToP scores as the dependent variable. We found a significant main effect of the type of group (long or short intervention) on the difference in ToP scores after controlling for the adaptive behaviour score (F(1,39) = 19.48, p < .001). Conversely, the main effect of the adaptive behaviour score was not significant (F 1,39 = 0.52, p > .05). The difference between groups in their adaptive behaviour score (see Table 1 for descriptive statistics) was not significant (t 40 = −0.66, p > .05).
In summary, we found that the effect of the clown intervention on the participants' playfulness level was more significant in the group that received the intervention for a longer period of time than in the group that received the intervention for a shorter period of time, even when controlling for the adaptive behaviour score.
3.2. Focus group
The following themes were identified from the discussion of the focus group, illustrated by excerpts:
A general positive effect of the clowns: ‘It was so lovely to see the children laughing so much’. (Teacher 3) ‘I fell in love with the clowns, I hope this project continues, it had such a positive effect on all of us’. (Teacher 6)
Something unusual happened during or as a result of the encounter with the clowns: ‘I was so surprised that he (child) engaged in the competitive game with the clowns, he's usually so passive…’ (Teacher 1) ‘When D asked the clown to sit next to him, I was surprised. He never asked anyone to sit next to him. Since then, he began initiating such things with others as well’. (Teacher 3) ‘With the clowns I saw her initiating and laughing out loud… I never saw her like this’ . (Teacher 8) ‘I tried to teach them to play with the ball for a long time, with no success, then Yoyo [the clown] came in and just did it. How did he do that?!’ (Teacher 3)
There was a positive effect of the clown on a child's specific difficulty: ‘The clowns found a way to connect with R. To get him out of his “bubble,” so he participated in the activity…’ (Teacher 4) ‘When the clowns approached a different kid, she would make sounds to call them to come back to her; that was unusual for her…’ (Teacher 5) ‘He is usually very shy. With the clowns I could see his confidence growing, they provided a safe place for him to play’. (Teacher 7)
The clowns affected or changed the teacher's practice: ‘I learned to do stupid things, to let the children “go wild,” the repertoire of our games expanded’. (Teacher 8) ‘I learned from the clowns to mirror them, to follow the child's ideas’. (Teacher 4) ‘I saw that doing foolish things jokingly and having fun has a significant effect on the children, in a way I could not imagine. I began laughing more with the children…’ (Teacher 1) ‘Their [the clowns'] responses were much more effective than mine. With all my pedagogic knowledge and years of experience, they know better…’ (Teacher 3) ‘I never thought they [the children] can play such imaginative games…’ (Teacher 6)
The clowns' effect was shown beyond the time of the meetings with the clowns: ‘A few months after the clowns are no longer here, the children are still asking that we play the games they used to play with the clowns’. (Teacher 8) ‘The clowns had an effect at the group level. The children didn't play as a group before. Since the clowns were here, the children began playing with each other much more’. (Teacher 5)
4. DISCUSSION
In the present study, we examined the change in the playfulness of children with intellectual disability, following a medical/therapeutic clown intervention. The results indicate that children with intellectual disability benefitted from the medical/therapeutic clown intervention, and their playfulness improved. The participating children showed improvement in their motivation to play, ability to initiate and engage in play, use of pretend play, imagination, humour, and engagement with others in play. The significant difference we found between the two study groups shows that the longer the intervention lasted, the greater the effect of the intervention was. Teachers' focus group provides a glimpse into the unique contribution of the clowns to the children's playfulness and their broader influence on children with intellectual disabilities: creating a safe, engaging, explorative and fun environment in which to practice playfulness.
The sample included children with a range of adaptive behaviour levels. Nevertheless, we found no correlation between adaptive behaviour and playfulness scores in baseline. Furthermore, we found no correlation between the improvement in playfulness scores and level of adaptive behaviour. This finding is significant because it points to a surprising aspect of the clown intervention: higher functioning children did not necessarily improve more than lower functioning ones. This result is similar to that of another study which found no significant correlation between the ability of children with intellectual disability to play and their IQ level (Messier et al., 2008). Children with different levels of disability can equally benefit from the clown intervention‐improving and enhancing their playfulness.
The play intervention described in this study is new both to the treatment of children with intellectual disability and to the profession of medical clowning. Previous studies on medical clowning emphasised the contribution of the clowns primarily to lowering anxiety and other negative emotions in medical circumstances (Sridharan & Sivaramakrishnan, 2016). Our study is the first known to us to examine the contribution of medical clowning to the playfulness of children with intellectual disabilities. People with intellectual disabilities may experience social injustice and disempowered social position (Walmsley, & Johnson, 2003; Baker & Donelly, 2001). Likewise, they may experience a lack of control and motivation, as well as a low sense of autonomy and self‐determination (Lachapelle et al., 2005) and therefore may benefit from psychological empowerment (Martin, 2006). The unique characteristics of the clowns' work provide novel conditions for the improvement of children's playfulness: The clowns' play allows children to be ‘themselves’ while playing as equal partners to the children, without expectations or didactic agenda; unlike teachers and most adults, who assume a pedagogic stance when playing with children with intellectual disabilities adopting either the role of the audience or of a ‘play director’ (Meacham, et al., 2014). The clowns are attentive to subtle communication and are flexible‐ready to adopt and improvise with any action offered by the child with intellectual disability; working with the child as a partner, while remaining open to what develops in the ‘here and now’ and the flow of the play. The clown's total engagement in playful interaction is exactly what succeeds in drawing the children in. Furthermore, the clowns make themselves as vulnerable as the children, preferring humour, grand mistakes and failures over success and didactics, thereby empowering the children and encouraging them to engage and take risks. All of these unique characteristics of the clowns' play foster a sense of freedom and joy that is so essential for children with intellectual disability, as for any other children.
4.1. Limitations of the study
The playfulness score, as measured by the ToP, showed a general improvement in children's playfulness. Nevertheless, the ToP was not able to capture the specific effects of the clown intervention because it was not designed for child‐clown‐group interaction, but rather for the one‐on‐one interaction of the child with another child or adult. Another limitation following from the method chosen to assess the children's playfulness (based on two interactions at the beginning and two at the end of the intervention) is that it did not allow to analyse all of the sessions throughout the intervention. Some of the children may have been more playful or expressed different qualities of playfulness in sessions other than those chosen for assessment. Our study used the ToP to assess children with severe and profound intellectual disability, however further exploration is needed to adapt and validate the test in this population.
The study's main limitation lies in the inability to measure the results of the intervention beyond the interactions with the clowns, not allowing us to generalise how the intervention affected the children outside the clown's interactions, or to evaluate abilities other than playfulness. The teachers' responses, however, provide an indication of the broader contribution of the clowns to the children and staff. Additional focus groups of teachers could increase the strength of this data.
This pioneering study can be extended in future studies to explore the contribution of medical clowns to advancing other areas in the development of children with intellectual disability. Moreover, the study sample included children with various levels of disability. Future studies need to control more closely the variability in the sample of children to be able to draw more robust conclusions about the effect of medical clowns on children with intellectual disability.
Finally, in the present study we chose to compare the groups on the basis of the duration of intervention received by each group. This time variable was chosen mainly because of pragmatic and ethical reasons, as the educational authorities of the kindergarten did not allow offering the clown intervention only to some of the children, therefore it was not possible to create a ‘no intervention’ group. We had to start the year giving all the children the opportunity to enjoy the clowns' work. This limitation is part of the difficulties in conducting a ‘naturalistic’ study as opposed to a laboratory one, where variables can be more easily chosen and controlled. Nevertheless, conducting the study in a natural setting was one of the strengths of the present study for providing a fertile interface between academic study and the community. At the same time, the absence of a more robust control group makes it impossible to pinpoint the unique contribution of the clowns by comparison with other treatments offered in the kindergarten.
5. CONCLUSION
The significance of the study lies in its contribution to the limited research on the playfulness of children with intellectual disability. The new intervention for children with intellectual disability described in this study was proven to be effective in improving the children's playfulness. The study supports the introduction of medical clowning into educational institutions for children with intellectual disabilities, and proposes a clowning approach in playing with children with intellectual disability based on free play and humour, which can be adopted by parents and the educational staff. Further research on this topic should focus on investigating the specific effects of the clown intervention on children's playfulness and its contribution to their socio‐emotional development.
FUNDING INFORMATION
This work was supported by the Keren Shalem fund.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
INFORMED CONSENT
All participants gave their full consent to participate in the study.
ACKNOWLEDGEMENTS
We thank Prof. Atay Citron for his support, inspiration, and guidance, Anwar Sabichat for her assistance in the data collection and analysis, Tali Koenig, the staff and families at the Flora preschool center for making this study possible, and last but not least the most talented and funny clowns: Esti Mittelberg, Yuval Ben‐Ami and Yaron‐Sancho Goshen.
Feniger‐Schaal, R. , Stern, A. , & Elizarov, E. (2023). The effect of medical/therapeutic clowns on the playfulness of children with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, 36(1), 186–195. 10.1111/jar.13049
Funding information Shalem fund, Grant/Award Number: 890‐68
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
REFERENCES
- Al‐Yagon, M. , & Margalit, M. (2012). Parental coping, emotional resources, and children's adjustment: Theory, empirical evidence, and interventional implications. In Molinelli B. & Grimaldo V. (Eds.), Handbook of the psychology of coping: New research (pp. 59–84). Nova Science Publisher's. [Google Scholar]
- American Psychiatric Association . (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Author. [Google Scholar]
- Baker, J. K. , Fenning, R. M. , Crnic, K. A. , Baker, B. L. , & Blacher, J. (2007). Prediction of social skills in 6‐year‐old children with and without developmental delays: Contributions of early regulation and maternal scaffolding. American Journal on Mental Retardation, 112(5), 375–391. 10.1352/0895-8017(2007)112[0375:POSSIY]2.0.CO;2 [DOI] [PubMed] [Google Scholar]
- Baker, K. , & Donelly, M. (2001). The social experiences of children with disability and the influence of environment: A framework for intervention. Disability & Society, 16(1), 71–85. 10.1080/713662029 [DOI] [Google Scholar]
- Barkmann, C. , Siem, A. K. , Wessolowski, N. , & Schulte‐Markwort, M. (2013). Clowning as a supportive measure in paediatrics‐a survey of clowns, parents and nursing staff. BMC Pediatrics, 13(1), 166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barnett, L. A. (1991). Characterizing playfulness: Correlates with individual attributes and personality traits. Play and Culture, 4(4), 371–393. [Google Scholar]
- Bass, J. D. , & Mulick, J. A. (2007). Social play skill enhancement of children with autism using peers and siblings as therapists. Psychology in the Schools, 44(7), 727–735. 10.1002/pits.20261 [DOI] [Google Scholar]
- Bateson, G. (1971). The message, ‘this is play’. In Herron R. E. & Sutton‐Smith B. (Eds.), Child's play (pp. 261–269). Wiley & Sons. [Google Scholar]
- Braun, V. , & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. [Google Scholar]
- Braun, V. , & Clarke, V. (2019). Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise and Health, 11(4), 589–597. [Google Scholar]
- Bundy, A. (2010). Test of playfulness. University of Sydney. [Google Scholar]
- Bundy, A. C. (1997). Play and playfulness: What to look for. In Parham L. D. & Fazio L. S. (Eds.), Play in occupational therapy for children (pp. 52–66). Mosby. [Google Scholar]
- Citron, A. (2011). Medical clowning and performance theory. In Harding J. & Rosenthal C. (Eds.), The rise of performance studies: Rethinking Richard Schechner's broad spectrum (pp. 248–263). Palgrave Macmillan. [Google Scholar]
- Faul, F. , Erdfelder, E. , Buchner, A. , & Lang, A.‐G. (2009). Statistical power analyses using G*power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41, 1149–1160. [DOI] [PubMed] [Google Scholar]
- Feniger‐Schaal, R. , Citron, A. , Mittlelberg, E. , & Ben Eli, Y. (2020). Intervention of medical (therapeutic) clowns in a kindergarten for children with intellectual disability: A case study. International Journal of Disability, Development and Education, 67(3), 293–305. [Google Scholar]
- Fischer, G. H. , & Molenaar, I. W. (Eds.). (1995). Rasch models: Foundations, recent developments and applications. Springer‐Verlag. [Google Scholar]
- Golinkoff, R. M. , Hirsh‐Pasek, K. , & Singer, D. G. (2006). Why play=learning: A challenge for parents and educators. In Singer D. G., Golinkoff R. M., & Hirsh‐Pasek K. (Eds.), Play = learning (pp. 3–12). Oxford University Press. [Google Scholar]
- Guralnick, M. J. (2016). Early intervention for children with intellectual disabilities: An update. Journal of Applied Research in Intellectual Disabilities, 30(2), 211–222. [DOI] [PubMed] [Google Scholar]
- Guralnick, M. J. , & Groom, J. M. (1987). The peer relations of mildly delayed and nonhandicapped preschool children in mainstreamed playgroups. Child Development, 58(6), 1556. 10.2307/1130695 [DOI] [PubMed] [Google Scholar]
- Hamm, E. M. (2006). Playfulness and the enviromental support of play in children with and without developmental disabilities. OTJR; Occupation, Participation and Health, 26(3), 88–96. [Google Scholar]
- Harkness, L. , & Bundy, A. C. (2001). The test of playfulness and children with physical disabilities. The Occupational Therapy Journal of Research, 21(2), 73–89. [Google Scholar]
- Harris, P. L. (2000). The work of the imagination. Blackwell Publishers. [Google Scholar]
- Hess, L. M. , & Bundy, A. C. (2003). The association between playfulness and coping in adolescents. Physical & Occupational Therapy in Pediatrics, 23(2), 5–17. [PubMed] [Google Scholar]
- Kingsnorth, S. , Blain, S. , & McKeever, P. (2011). Physiological and emotional responses of disabled children to therapeutic clowns: A pilot study. Evidence‐Based Complementary and Alternative Medicine, 2011, 2011–2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koller, D. , & Gryski, C. (2008). The life threatened child and the life enhancing clown: Towards a model of therapeutic clowning. Evidence‐based Complementary and Alternative Medicine, 5(1), 17–25. 10.1093/ecam/nem033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lachapelle, Y. , Wehmeyer, M. L. , Haelewyck, M. C. , Courbois, Y. , Keith, K. D. , Schalock, R. , Verdugo, M. A., & Walsh, P. N. (2005). The relationship between quality of life and self‐determination: An international study. Journal of Intellectual Disability Research, 49(10), 740–744. 10.1111/j.1365-2788.2005.00743.x [DOI] [PubMed] [Google Scholar]
- Lane, S. J. , & Mistrett, S. G. (1996). Play and assistive technology issues for infants and young children with disabilities: A preliminary examination. Focus on Autism and Other Developmental Disabilities, 11(2), 96–104. [Google Scholar]
- Lindsey, E. , & Colwell, M. (2013). Pretend and physical play: Links to preschoolers' affective social competence. Merrill‐Palmer Quarterly, 59(3), 330–360. [Google Scholar]
- Malone, D. M. , & Langone, J. (1999). Teaching object‐related play skills to preschool children with developmental concerns. International Journal of Disability, Development and Education, 46(3), 325–336. [Google Scholar]
- Martin, R. (2006). A real life–A real community: The empowerment and full participation of people with an intellectual disability in their community. Journal of Intellectual & Developmental Disability, 31(2), 125–127. 10.1080/13668250600681511 [DOI] [PubMed] [Google Scholar]
- McGraw, K. O. , & Wong, S. P. (1996). Forming inferences about some intraclass correlation coefficients. Psychological Methods, 1(1), 30–46. [Google Scholar]
- Meacham, S. , Vukelich, C. , Han, M. , & Buell, M. (2014). Preschool teachers’ questioning in sociodramatic play. Early Childhood Research Quarterly, 29(4), 562–573. 10.1016/j.ecresq.2014.07.001 [DOI] [Google Scholar]
- Meiri, N. , Ankri, A. , Hamad‐Saied, M. , Konopnicki, M. , & Pillar, G. (2016). The effect of medical clowning on reducing pain, crying, and anxiety in children aged 2–10 years old undergoing venous blood drawing—A randomized controlled study. European Journal of Pediatrics, 175(3), 373–379. [DOI] [PubMed] [Google Scholar]
- Messier, J. , Ferland, F. , & Majnemer, A. (2008). Play behavior of school age children with intellectual disability: Their capacities, interests and attitude. Journal of Developmental and Physical Disabilities, 20(2), 193–207. [Google Scholar]
- Muys, V. , Rodger, S. , & Bundy, A. C. (2006). Assessment of playfulness in children with autistic disorder: A comparison of the children's playfulness scale and the test of playfulness. OTJR: Occupation, Participation and Health, 26(4), 159–170. [Google Scholar]
- Niccols, A. , Thomas, K. , & Schmidt, L. A. (2012). Socioemotional and brain development in children with genetic syndromes associated with developmental delay. In Burack J. A., Hodapp R. M., Iarocci G., & Zigler E. (Eds.), The oxford handbook of intellectual disability and development (pp. 254–274). Oxford University Press. [Google Scholar]
- Okimoto, A. M. , Bundy, A. , & Hanzlik, J. (2000). Playfulness in children with and without disability: Measurement and intervention. American Journal of Occupational Therapy, 54(1), 73–82. [DOI] [PubMed] [Google Scholar]
- Pinchover, S. (2017). The relation between teachers' and children's playfulness: A pilot study. Frontiers in Psychology, 8, 2214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raviv, A. (2012). Still the best medicine, even in a war zone: My work as a medical clown. TDR/The Drama Review, 56(2), 169–177. [Google Scholar]
- Raviv, A. (2018). Medical clowning: The healing performance. Seagull books. [Google Scholar]
- Schuengel, C. , & Janssen, C. G. (2006). People with mental retardation and psychopathology: Stress, affect regulation and attachment: A review. International Review of Research in Mental Retardation, 32, 229–260. 10.1016/S0074-7750(06)32008-3 [DOI] [Google Scholar]
- Shefer, S. , Attia, O. L. , Rosenan, R. , Wald, O. A. , Ende, H. , & Gabis, L. V. (2019). Benefits of medical clowning in the treatment of young children with autism spectrum disorder. European Journal of Pediatrics, 178(8), 1283–1289. [DOI] [PubMed] [Google Scholar]
- Sigman, M. , Ruskin, E. , Arbelle, S. , Corona, R. , Dissanayake, C. , Espinosa, M. , & Robinson, B. F. (1999). Continuity and change in the social competence of children with autism, Down syndrome, and developmental delays. Monographs of the Society for Research in Child Development, 64(1), 1–114 https://www.jstor.org/stable/3181510 [DOI] [PubMed] [Google Scholar]
- Siller, M. , Hutman, T. , & Sigman, M. (2013). A parent‐mediated intervention to increase responsive parental behaviors and child communication in children with ASD: A randomized clinical trial. Journal of Autism and Developmental Disorders, 43(3), 540–555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Skard, G. , & Bundy, A. (2008). Test of playfulness. In Parham L. D. & Fazio L. S. (Eds.), Play in occupational therapy for children (pp. 71–93). Mosby Elsevier. [Google Scholar]
- Sparrow, S. S. , Cicchetti, D. V. , & Balla, D. A. (2006). Vineland adaptive behavior scales. In Parent/caregiver rating form manual (2nd ed.). Pearson. [Google Scholar]
- Sridharan, K. , & Sivaramakrishnan, G. (2016). Therapeutic clowns in pediatrics: A systematic review and meta‐analysis of randomized controlled trials. European Journal of Pediatrics, 175(10), 1353–1360. [DOI] [PubMed] [Google Scholar]
- Sutton‐Smith, B. (1997). The ambiguity of play: Rhetorics of fate. In The performance studies reader. Routledge. [Google Scholar]
- Walmsley, J. , & Johnson, K. (2003). Normalizing, emancipating and making a stand. In Inclusive research with people with learning disabilities: Past, present and futures (pp. 44–60). Jessica Kingsley Publishers. [Google Scholar]
- Walters, A. S. , & Kaufman Blane, K. (2000). Mental retardation. In Zeanah C. (Ed.), Handbook of Infant Mental Health (2nd ed., pp. 271–281). Guilford Press. [Google Scholar]
- Warren, B. , & Spitzer, P. (2011). Laughing to longevity—The work of elder clowns. The Lancet, 378(9791), 562–563. [DOI] [PubMed] [Google Scholar]
- Wright, B. D. , & Stone, M. H. (1979). Best test design. MESA Press. [Google Scholar]
- Youell, B. (2008). The importance of play and playfulness. European Journal of Psychotherapy and Counselling, 10(2), 121–129. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.