

Abstract
School‐age children on the autism spectrum who are minimally verbal (MVAS) use a limited repertoire of spontaneous communicative spoken words and reveal large heterogeneity in cognitive functioning. Despite the challenges to form peer social engagement posed by their unique social‐communicative profile, few interventions have targeted peer interactions in the MVAS population. This study explored predictors of individual differences in treatment response among 54 school‐age minimally verbal autistic children (8–16 years) following an RCT “school‐based peer social intervention” (S‐PSI) that compared two peer‐oriented intervention modalities (conversation versus collaboration) versus a waitlisted control group. We examined autistic‐symptom severity, age, verbal and nonverbal IQ, executive functions, and sensory‐processing profile for their contribution to children's ability to form relevant spontaneous communication exchanges with a peer partner. Main findings revealed that larger deficits in sensory‐processing (sensory‐avoidance and sensory low‐registration) and in executive functions contributed to greater growth in “relevant” (i.e., adequately attuned, participatory, reciprocal) communication following both interventions, but not for the waitlisted controls. Additionally, older participants with lower verbal and nonverbal IQ improved communication's relevancy more after the conversation intervention, whereas the collaboration intervention was more beneficial for younger participants. Lower autistic‐symptom severity contributed to larger growth in relevancy for all groups. By identifying individual‐level predictors of spontaneous, attuned, participatory, and reciprocal (i.e., “relevant”) communication exchanges with peers, we optimized S‐PSI personalization for this uniquely nonverbal, heterogeneous MVAS population. These new channels for tailoring peer interventions to better meet individuals' needs may result in reduced social isolation and loneliness and enhanced well‐being.
Keywords: communication exchanges, individual differences, minimally verbal ASD, peer interaction, school‐based peer social intervention, treatment response
Lay Summary
We examined cognitive‐developmental‐sensory and diagnostic predictors of individual differences in children's ability to form relevant spontaneous peer communication exchanges, following “school‐based peer‐social intervention” (S‐PSI) targeting minimally verbal autistic children (<30 words). Unexpectedly, treated children with greater sensory‐processing and executive‐function challenges made larger magnitude of progress. S‐PSI may influence implicit cognitive/sensory skills, thus increasing social engagement.
INTRODUCTION
Minimally verbal autism spectrum—Definition
School‐age children on the autism spectrum who are “minimally verbal” (MVAS) are characterized by difficulties in spoken language, displaying a repertoire of 0 to 30 spontaneous words (Tager‐Flusberg & Kasari, 2013). This paucity in spontaneous speech poses ongoing challenges for children's communication exchanges—their initiations and responses toward peers—during social engagement (Kasari et al., 2013; Pecukonis et al., 2019; Tager‐Flusberg et al., 2017). Prolonged difficulties in cooperating and conversing with peers can often lead to social isolation and lower well‐being, which implies the likelihood of poor long‐term prognosis for social adjustment (Howlin et al., 2000). Moreover, this minimally verbal subgroup poses challenges to both theoreticians and interventionists due to its heterogenous cognitive and language profiles (Bal et al., 2016; Kasari et al., 2013; Tager‐Flusberg & Kasari, 2013). Cognitive functioning in MVAS may range from profound impairment to average intelligence, with 16% showing a nonverbal IQ of 70 or more. Receptive language may also vary from severe impairment to intact vocabulary, but most MVAS children show nonverbal IQ scores (as measured by Raven's Colored Progressive Matrices; Raven et al., 1998) that exceed their receptive vocabulary scores (Peabody Picture Vocabulary Test‐III; Dunn & Dunn, 1997).
Prior peer‐interaction intervention
Despite its clear importance, peer‐to‐peer interaction has only rarely been targeted explicitly by interventions for school‐age MVAS children. To date, most interventions on this population utilized child‐adult rather than child–child interaction—while targeting speech production (with/without augmentative/alternative communication devices), prompting requests, responses, questions, and information sharing. In such child‐adult interventions, children's speech‐production improvement was associated with higher baseline levels of joint attention (Kasari et al., 2014) and symbolic play skills (Chang et al., 2018), as well as higher child‐caregiver communication exchanges (DiStefano et al., 2016) and lower severity of autism (Chenausky et al., 2018). The few intervention studies that focused directly on peer interaction in school‐age MVAS children yielded optimistic results such as increased communication abilities (e.g., Bahrami et al., 2016) and social skills like joining activities and sharing experiences or information (Plavnick et al., 2015). Children retained these gains from 2 weeks to 4 months after treatment, but these two studies were not RCTs and had relatively small sample sizes.
Recently, Bauminger‐Zviely et al. (2020) conducted an extensive RCT study for a sample of 54 school‐age MVAS children ages 8–16 years, investigating the effectiveness of the “school‐based peer social intervention” (S‐PSI) designed to increase social engagement in minimally verbal peer dyads on the autism spectrum (Bauminger‐Zviely et al., 2015). Throughout the S‐PSI intervention, children were taught to engage with peers either by conversing or collaborating in ways that offered alternatives to spoken words. Children could use any available communication channels including sign language, gestures, handwriting, drawing, touch, facial expression, kinesthetic movement in space, and digital tools. Efficacy of each intervention modality—conversation and collaboration—was also compared to a waitlisted (control) group.
At the group level, significant pretest‐to‐posttest improvement emerged for both intervention groups' spontaneous free conversation exchanges (mostly nonverbal) and for the collaboration group's spontaneous free play, showing increases in peer‐dyad members' key social behaviors such as initiations toward the peer partner and relevancy of peers' communicative exchanges during social‐engagement situations (Bauminger‐Zviely et al., 2020). No such improvement emerged for the control group, highlighting the potential efficacy of peer‐oriented intervention for populations with MVAS.
However, a closer look at the RCT findings at the individual level suggested that children's outcomes varied within each of the three groups. Namely, following peer‐oriented intervention or while waiting for treatment, some individual MVAS children exhibited growth in social engagement, while other individuals showed little or no gain. This raises an important question that may be linked to the inherent heterogeneity of the MVAS population: What personal child characteristics may predict better or poorer growth as a result of peer‐oriented intervention? Considering the vital importance of peer engagement for child's development and well‐being, the present study aimed to identify endogenous predictors of individual differences in children's growth as a result of peer‐oriented S‐PSI conversation and collaboration interventions (Bauminger‐Zviely et al., 2020).
Individual differences contributing to social engagement and functioning: Potential endogenous factors
Individual differences in social engagement resulting from peer‐interaction interventions have rarely been examined in the autism spectrum and even less so in MVAS. The few endogenous factors that previous studies did identify as contributing to social functioning have mainly been investigated to date with preverbal toddlers and verbally fluent children on the autism spectrum. Additionally, only some of the rare prior research conducted interventions, but most did not. In this section, we review those identified endogenous factors, namely: autistic‐symptom severity, age, cognitive variables (i.e., verbal IQ, nonverbal IQ, executive functions), and sensory‐processing profile. All of these have demonstrated strong evidence as influencing the ability to socially engage and communicate among children on the autism spectrum (Bertollo & Yerys, 2019; Kojovic et al., 2019; Ruble & McGrew, 2013; Strauss et al., 2014). We will specify those cases referring to MVAS participants or to treatment outcomes.
Elevated severity of autistic symptoms has been consistently linked to poorer adaptive skills across ages and cognitive abilities (e.g., Chan et al., 2017; Miranda et al., 2020; Tillmann et al., 2019) and to lower progress following child‐teacher social‐skills intervention (Ruble & McGrew, 2013).
The contribution of development (i.e., age) to children's social engagement was less consistent. Younger age was related with progress in social engagment (Morrier & Ziegler, 2018) and in joint attention and peer‐interaction initiation (Strauss et al., 2014), following treatment. But specific studies on MVAS showed that social behaviors (eye contact, gestures, initiatives, responses, etc.) were not related to age among 78 MVAS children (M = 6.19 years, SD = 1.29) following child‐adult play‐based social‐skills intervention (Grzadzinski, 2018). Likewise, age did not correlate with adaptive skills (communication or socialization domains on the Vineland adaptive scale) among 333 MVAS children (M = 5.95 years, SD = 1.53) (Frost et al., 2017). Thus, the role played by age in peer interaction among MVAS requires further examination.
Verbal and nonverbal IQ—were found to predict language development, adaptive social behavior, and social impairment in individuals on the autism spectrum across a wide range of ages and functioning levels (Ben‐Itzchak & Zachor, 2020; Chan et al., 2017; Charman et al., 2017; Tager‐Flusberg & Kasari, 2013). Several studies looking mainly at MVAS children and adolescents found that higher verbal IQ predicted better socialization skills (Zou et al., 2018), and higher nonverbal IQ correlated with better adaptive skills (Bertollo & Yerys, 2019; Frost et al., 2017), language development (Kasari et al., 2013), and social skills like imitation and play (Pecukonis et al., 2019). Notably, Plesa Skwerer et al. (2016) found that in MVAS children and adolescents' (6–21 years), verbal IQ (i.e., Peabody) scores were lower than nonverbal IQ scores (i.e., Raven). This calls for their separate examination in the social‐communication context for MVAS.
Cognitive abilities may also contribute to social functioning through children's executive functioning skills. Executive cognitive operations like initiation, planning, working memory, self‐monitoring, and environmental organization enable children's performance of purposeful and socially acceptable behavior (Bertollo & Yerys, 2019; Friedman & Sterling, 2019). Executive difficulties in autistic persons have been linked with difficulties in language, communication, mentalization of others' feelings and thoughts (i.e., theory of mind), social interaction, collaboration during social play, imagination, and creativity (Bauminger‐Zviely, 2013; Bednarz et al., 2020; Friedman & Sterling, 2019; Kimhi et al., 2014; Pugliese et al., 2015). Interestingly, in Bertollo and Yerys (2019), executive deficits in self‐monitoring, as well as older age and lower nonverbal IQ, contributed to lower adaptive skills (communication, socialization) in school‐age children with low IQ levels (IQ < 75).
Finally, sensory‐processing challenges are considered a defining symptom of individuals on the autism spectrum (American Psychiatric Association, 2013), with 50%–70% of them characterized by hyposensitivity, sensory‐seeking, and/or hypersensitivity and up to 90% characterized by sensory‐avoidance. These patterns may appear in any of the senses (Dellapiazza et al., 2019, 2020; Hilton et al., 2010; Sanz‐Cervera et al., 2017; Thye et al., 2018).
Several studies demonstrated links between sensory‐processing and social functioning. For example, larger impairments in sensory processing among children on the autism spectrum (3–6 years) were correlated with greater social difficulties, lower socialization skills, and poorer adaptive daily living skills (Kojovic et al., 2019). Also, children on the autism spectrum who had more sensory issues in registration of sensory cues, sensation‐seeking, and auditory‐filtering dimensions demonstrated more divergent gaze patterns in dynamic visual exploration of social scenes, compared to typically developing children. Dellapiazza et al.'s (2019) study of 197 children on the autism spectrum (3–11 years) found that those with difficulties in sensory‐seeking profile showed lower adaptive functioning (socialization, communication) than those with a typical sensory‐seeking profile. Yet, interestingly, children on the autism spectrum who had an irregular sensory‐avoidant profile showed higher adaptive communication skills than those with a typical sensory‐avoidant profile. This surprising finding may suggest that children on the autism spectrum who are irregular in their sensory avoidance may attend more to language and communication components. However, these associations diminished when controlling for IQ. In their review, Williams et al. (2018) suggested that atypical sensory‐processing along with cognitive abilities may affect opportunities for significant social experiences, thereby subsequently impeding development of broader social‐communicative adaptive skills and behaviors.
Study rationale and objectives
The importance of social interactions with peers for the well‐being and adaptive skills of children on the autism spectrum has been well established, and initially promising results emerged at the group level from our recent RCT study applying peer‐oriented intervention to promote social interactions among a heterogeneous and potentially vulnerable population of school‐age MVAS children (Bauminger‐Zviely et al., 2020). However, as seen in the review above, the frequent exclusion of school‐age MVAS children from prior research (Koegel et al., 2020; Tager‐Flusberg & Kasari, 2013) is not conducive to drawing conclusions about possible child characteristics that may contribute to children's growth from peer intervention. Predictors of social functioning may manifest differently in this sub‐population on the autism spectrum, due to their unique characteristics reflected in large heterogeneity of cognitive and language functioning (Bauminger‐Zviely et al., 2020), and, most noticeably, their paucity of spontaneous speech (Koegel et al., 2020).
Thus, the present study conducted a novel examination of school‐age MVAS children to determine whether endogenous factors previously identified for other subgroups on the autism spectrum (e.g., preverbal toddlers, verbally fluent) may contribute to these children's variability in social engagement growth from peer‐oriented intervention. Identification of possible endogenous predictors of individual differences in children's growth during the S‐PSI conversation and collaboration interventions (Bauminger‐Zviely et al., 2020) was expected to expand existing empirical and clinical knowledge about this population, thus promoting personalization of intervention programs to better fit each child's unique profile and needs.
The S‐PSI intervention included several observational outcomes to evaluate spontaneous peer interaction in MVAS. For the purpose of this study focusing on individual‐level progress in social engagement, we used the “relevancy” measure, which reflects children's adequately attuned, participatory, and reciprocal communicative‐exchange behaviors. More specifically, we explored five endogenous variables' contribution to positive pretest‐to‐posttest progress in the relevancy of peer exchanges: (a) severity of autistic symptoms (social‐communicative, restricted/repetitive); (b) chronological age; (c) verbal IQ (Peabody) and nonverbal IQ (Raven); (d) executive functions; and (e) sensory‐profile scales (sensation‐seeking, sensory‐sensitivity, sensory‐avoiding, and sensory low‐registration). We hypothesized that younger age and higher verbal and nonverbal IQ would predict higher change scores in exchange's relevancy, whereas high autistic‐symptom severity, executive functioning difficulties, and irregular sensory‐processing would predict smaller progress following S‐PSI (lower change scores in relevancy).
METHOD
This study was part of a broader RCT‐based project examining S‐PSI efficacy. Appendix A describes the two interventions' principles and content. For full information on methods and procedures, see Bauminger‐Zviely et al. (2020).
Participants
Participants were 54 school‐age MVAS children recruited from nine special‐education schools. Inclusion criteria were: (a) formal clinical ASD diagnosis, based on the Diagnostic and Statistical Manual of Mental Disorders criteria (4th ed., text rev.; American Psychological Association, 2000), given by a licensed psychologist unassociated with this study as mandatory for inclusion into these special education schools according to Israeli Ministry of Education policy; (b) verification of the child's ASD formal clinical diagnosis (scores above the autism cutoff) by a parent's report on the Social Communication Questionnaire (Rutter et al., 2003); (c) IQ ≥ 35 using the Peabody (Dunn & Dunn, 1997) for verbal IQ and the Raven (Raven et al., 1998) for nonverbal IQ; and (d) no more than 30 spontaneously spoken words (reported by teachers) per the MVAS definition (Tager‐Flusberg & Kasari, 2013). The study received permission from the chief scientist of the Ministry of Education.
To create the sample, eligible children from 37 classes in nine schools were randomly assigned into three groups: two intervention groups (conversation, collaboration) and one control (delayed‐intervention) group. In six of the schools, student numbers and teacher availability permitted children's initial random allocation to all three conditions within each school. In the three schools where student numbers or teacher availability were insufficient to initially allocate children to all three conditions in the same school, randomization was performed across schools. Allocation continued randomly across schools until all participants were assigned (for full details, see Bauminger‐Zviely et al., 2020).
Each of the three groups comprised 18 children in nine fixed dyads, matched by their preferred minimally verbal or nonverbal communication mode. At baseline (Time1), participants were 8–16 years, with verbal IQ score range of 37–101 (M = 56.26, SD = 16.22) and nonverbal IQ score range of 41–125 (M = 62.56, SD = 21.02). See Table 1 for pretest characteristics of study participants by group. Preliminary independent‐samples t‐test revealed significantly higher nonverbal IQ for the intervention groups than the control group, t(52) = −2.143, p < 0.05, and significantly higher restricted/repetitive behaviors in the conversation than the collaboration group, t(34) = −2.17, p < 0.05. However, these endogenous factors had no significant correlation with the S‐PSI outcome measure: pre‐post change scores in exchanges' relevancy.
TABLE 1.
Pretest characteristics of study participants (N = 54) with MVAS by group
| Study group | |||||
|---|---|---|---|---|---|
| Conversation (n = 18) | Collaboration (n = 18) | Control (n = 18) | Group differences | ||
| Boys/girls | 15/3 | 16/2 | 13/5 | ||
| Chronological age in months | M (SD) | 122.61 (18.61) | 134.76 (28.56) | 136.17 (22.52) | ns |
| Range | 96–162 | 92–181 | 94–182 | ||
| No. of spoken words (Social Conversation Scale) | M (SD) | 6.44 (6.90) | 10.33 (10.25) | 8.22 (8.14) | ns |
| Range | 0–25 | 0–30 | 0–30 | ||
| Communication channels | |||||
|
Limited speech only iPad with/without limited speech Communications board with/without limited speech Sign language + limited speech Sign language + writing |
5 7 6 0 0 |
12 5 1 0 0 |
4 6 6 1 1 |
||
| ASD diagnostic verification score (Social Communication Questionnaire) | M (SD) | 22.56 (3.57) | 22.00 (4.10) | 21.67 (3.38) | ns |
| Mothers' education a | M (SD) | 3.16 (0.85) | 3.44 (1.50) | 3.00 (1.37) | ns |
A 6‐point scale ranging from elementary school (1) to graduate degree or higher (6).
Measures
Relevancy: The S‐PSI outcome measure
This study on individual differences in treatment response examined a change score of Time2 (after treatment) minus Time1 (before treatment) regarding one outcome measure for “relevancy.” As operationalized in the RCT study, relevancy was the child's adequacy of attunement toward a peer partner and participation in reciprocal communication chains. At each time for each child, relevancy was rated during a 6‐min videotaped free social “conversation” situation within the same fixed peer‐dyads. During the first 3 min of the free‐“talk” situation, a familiar teacher provided structured support to assist the fixed peer‐dyads to begin communicating interactively using their preferred nonverbal/minimally‐verbal channels. In the ensuing 3 min, the teacher only encouraged the dyad to continue their “conversation” exchange. For example,” relevant” exchanges might include: Partner A listens and looks at Partner B's communication (e.g., board/gesture/speech) while Partner B communicates (writes/gestures/speaks) a question for Partner A; then Partner A replies by showing a word/picture using their preferred channel.
Raters of relevancy used Capps et al.'s (1998) Social Conversation Scale, as adapted by Bauminger‐Zviely et al. (2020) to the MVAS population's nonverbal communication channels (e.g., gestures, social smile, eye contact, initiations, responses). Two raters, experts in special education (masked to participants' group assignment) counted each child's frequency of relevant, adequate communicative behaviors toward the communicative partner during each 10‐s interval across the 6 min. Relevant behavior was scored 1, and nonrelevant behavior was scored 0, yielding a possible total relevancy score ranging between 0 and 36. This relevancy rating scale showed high reliability (α = 0.88). Raters obtained high intraclass correlation coefficients (ICC) on independent coding of 25% of videotapes, randomly selected from the three groups (ICC = 0.88 on free‐conversation coding).
Endogenous factors: Individual difference measures
Autistic‐symptom severity. The Social Responsiveness Scale (Constantino & Gruber, 2012), commonly used in studies on the autism spectrum for ages 4–18 years (Chan et al., 2017; Jones et al., 2017; Tillmann et al., 2019), assessed teacher‐rated severity of children's autistic symptoms. Two subscales corresponded with DSM‐5 symptom domains (American Psychiatric Association, 2013): social communication and interaction (SCI; 53 items) and restricted interests and repetitive behaviors (RRB; 12 items). Higher scores indicated more severe impairment. The scale showed high reliability (α = 0.97).
IQ. The Peabody and Raven IQ tests assessed children's verbal and nonverbal cognitive abilities, respectively.
Executive function. Teachers assessed children's executive functions using the behavior rating inventory of executive function (BRIEF; Gioia et al., 2000). The BRIEF, for children ages 5–18 years on the autism spectrum and/or intellectual disabilities (Bednarz et al., 2020), has high test–retest reliability (Gioia et al., 2000). The 86‐item generalized executive function score included behavioral regulation (e.g., inhibition, shifting, emotional control) and metacognition (e.g., planning, organization, monitoring). Higher scores indicated more severe impairment. The scale showed high reliability (α = 0.93).
Sensory profile. Teacher‐rated Sensory Profile School Companion Questionnaire (Dunn, 2006) assessed four of children's sensory patterns: sensory low‐registration (22 items; e.g., missing sensory cues that others notice easily), sensation‐seeking (19 items; e.g., needing more sensory input, staying more alert), sensory‐sensitivity (19 items; e.g., putting hands over ears), and sensory‐avoiding (20 items; e.g., moving away from activities, choosing to work alone). Higher scores indicated more normative (typical) sensory‐processing behavior. The scale showed high reliability (α = 0.86) and suitability for children with or without autism spectrum ages 3–12 years (Brown & Dunn, 2010). Although some current participants were older, their mental age fit this age range.
Data analysis
To explore the endogenous factor set's contribution to explanations of individual growth in relevancy of spontaneous communication exchanges with the peer partner as a result of the S‐PSI, we calculated a change score (Time2 minus Time1) for all study participants. Then, we conducted comparisons for two analytic conditions. Condition 1 (n = 54) examined the whole sample, comparing those who did versus those who did not undergo an intervention (i.e., the control group versus both the collaboration and conversation groups together). Condition 2 (n = 36) compared the two intervention groups to one another (i.e., collaboration vs. conversation), to understand each modality's possible differential contribution.
These comparisons were examined within a two‐part modeling approach using the Mplus V.8.3 statistical package (Muthén et al., 2016). In this approach, a binary (logistic or‐ probit) regression evaluates across all participants the probability of making positive progress (coded as 1) or of making no progress or negative progress (coded as 0). Simultaneously, a linear (continuous) regression examines only those who made positive progress, calculating the extent of their progress based on their actual change score, as controlled by their probability of making positive progress (Farewell et al., 2017; Sauzet et al., 2019). In this study of relevancy outcomes, we expanded the two‐part modeling to include the random effect of dyads within the two‐level analytical framework (Blozis et al., 2020). Individual participants were measured at the subject‐level, while the dyadic level was set for the peer‐coupled response. Due to the small sample, the random effect was expressed in the dyadic intercept, an intercept that varied by dyads. All analyses included the following predictors (see Figure 1): baseline relevancy score, group, each Time1 endogenous factor score, and its interaction with group.
FIGURE 1.
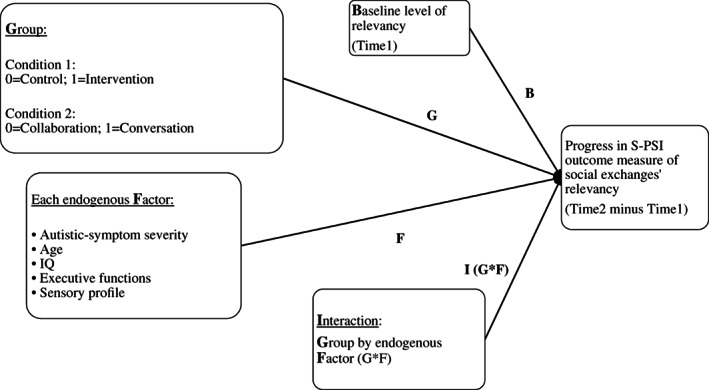
Regression model for peer communication Exchanges' relevancy outcomes. S‐PSI, school‐based peer social intervention
RESULTS
Preliminary descriptive statistics
Groups' pretest and posttest scores for relevancy (range: 0–36) were: Conversation—Time1: M = 6.49, SD = 1.89; Time2: M = 12.91 SD = 2.17; Collaboration—Time1: M = 11.25, SD = 2.08; Time2: M = 20.19, SD = 2.08; and Control—Time1: M = 13.23, SD = 1.46; Time2: M = 12.90, SD = 1.86.
The truncation procedure yielded 40 positive responders to treatment (74% of the sample)—those participants with positive pre‐post change in peer exchanges' relevancy. Table 2 presents percentages of positive responders by group, for each analytic condition. Chi‐square goodness‐of‐fit test was performed to determine whether the proportion of positive responders was equal between groups. As seen in the table, the percentage of positive responders was significantly higher in the intervention groups than the control group (Condition 1), without significant conversation versus collaboration differences (Condition 2). In line with the linear model, Table 2 also presents descriptive statistics for each group's extent of positive progress in relevancy scores, by analytic condition, showing non‐significant group differences in both conditions.
TABLE 2.
Group differences for percentages of positive treatment responders (n = 40) and descriptive data for change scores by analytic condition
| Condition 1 (n = 54) | Condition 2 (n = 36) | ||||||
|---|---|---|---|---|---|---|---|
| Both intervention groups | Control group | Collaboration group | Conversation group | ||||
| Positive responders (showing positive change in relevancy) | N | 33 | 7 | 16 | 17 | ||
| % of group | 91.6 | 38.9 | 88.9 | 94.4 | |||
| df | 1 | 1 | |||||
| χ 2 | 17.40 | 0.36 | |||||
| p | 0.00 | 0.55 | |||||
| Change scores (Time2 minus Time1) | M (SD) | 8.45 (5.56) | 6.43 (4.72) | 9.50 (5.51) | 7.47 (5.58) | ||
| Range | 1–24 | 2–15 | 3–24 | 1–22 | |||
| df | 38 | 31 | |||||
| t | −0.09 | 1.05 | |||||
| p | 0.38 | 0.30 | |||||
The two‐part series of regression analyses (binary and linear) examined endogenous factors' effects on positive progress in relevancy. Table 3 separately presents coefficients (β for linear and B for binary) for each endogenous factor's effects and interactions with group; see Figure 2 for only significant effects. Sensory‐seeking and sensory‐sensitivity profiles did not contribute significantly to relevancy in either model. The other effects are described below.
TABLE 3.
Coefficients from linear and binary modeling for endogenous predictors of relevancy outcomes by analytic condition
| Endogenous factors | Condition 1 (n = 54): Control (0) versus both interventions (1) | Condition 2 (n = 36): Collaboration (0) versus conversation (1) | ||||
|---|---|---|---|---|---|---|
| Linear β | Binary B (odds) | Linear β | Binary B (odds) | |||
| Autistic‐symptom severity | Social communication/interaction (SCI) | SCI | −0.516 * | 0.041 (1.042) | −0.110 | 0.018 (1.018) |
| Group* SCI | 0.873 | −0.042 (0.959) | 0.441 | −0.064 (0.938) | ||
| Restricted/repetitive behavior (RRB) | RRB | −0.517 * | 0.046 (1.047) | −0.111 | 0.399 (1.491) | |
| Group* RRB | 0.556 | 0.124 (1.132) | 0.396 | −0.497 (0.608) | ||
| Chronological age | Age | 0.121 | 0.014 (1.014) | 0.201 | −0.053 ** (0.948) | |
| Group* Age | 1.261 | −0.045 (0.956) | 1.763 ** | 0.067 * (1.070) | ||
| Age* (Group = 1) | — | — | 0.863 *** | 1.014 *** | ||
| Cognitive functioning | Verbal IQ (VIQ) | VIQ | −0.446 | −0.022 (0.979) | −0.003 | 0.011 (1.011) |
| Group* VIQ | 0.251 | 0.035 (1.035) | −1.432 ** | 0.019 (1.019) | ||
| VIQ* (Group = 1) | — | −0.747 *** | — | |||
| Nonverbal IQ (NVIQ) | NVIQ | −0.200 | 0.072 * (1.074) | −0.187 | 0.118 (1.125) | |
| Group* NVIQ | 0.037 | −0.06 (0.942) | 0.112 | 0.166 ** (0.847) | ||
| NVIQ* (Group = 1) | — | — | — | 0.953 *** | ||
| Executive functions (EF) | EF | −0.021 | −0.178 (0.837) | 0.485 * | −0.223 * (0.800) | |
| Group* EF | 1.411 | −0.028 (0.973) | −0.350 | 0.107 (1.112) | ||
| Sensory profile | Sensory low‐registration (SLR) | SLR | 0.336 ** | 0.039 * (1.040) | −0.778 *** | 0.038 (1.038) |
| Group* SLR | −1.478 ** | −0.009 (0.991) | 0.999* | 0.035 (1.036) | ||
| SLR* (Group = 1) | −0.325* | — | −0.314* | — | ||
| Sensory‐avoidance (SA) | SA | 0.538 | −0.009 (0.991) | −0.282 | 0.081 * (1.084) | |
| Group* SA | −1.855 ** | 0.082 * (1.085) | 0.058 | −0.016 (0.984) | ||
| SA* (Group = 1) | −0.337 *** | 1.075 *** | — | — | ||
Note: Values in bold are significant. The rejection criterion was adjusted using Holm‐Bonferroni correction (Cangur et al., 2016), which relates to the p‐value ranking of the multiple hypothesis test results. The cases in which the null‐hypothesis was rejected remained unchanged, except for two cases that were as close as 0.0002 to rejection. Group = 1 in cases of significant interactions refers to: the additional endogenous factor effect (the simple slope) for the intervention group versus this effect for the control group in Condition 1 and for the conversation group versus this effect for the collaboration group in Condition 2, both for binary and linear analyses.
p < 0.05;
p < 0.01;
p < 0.001.
FIGURE 2.
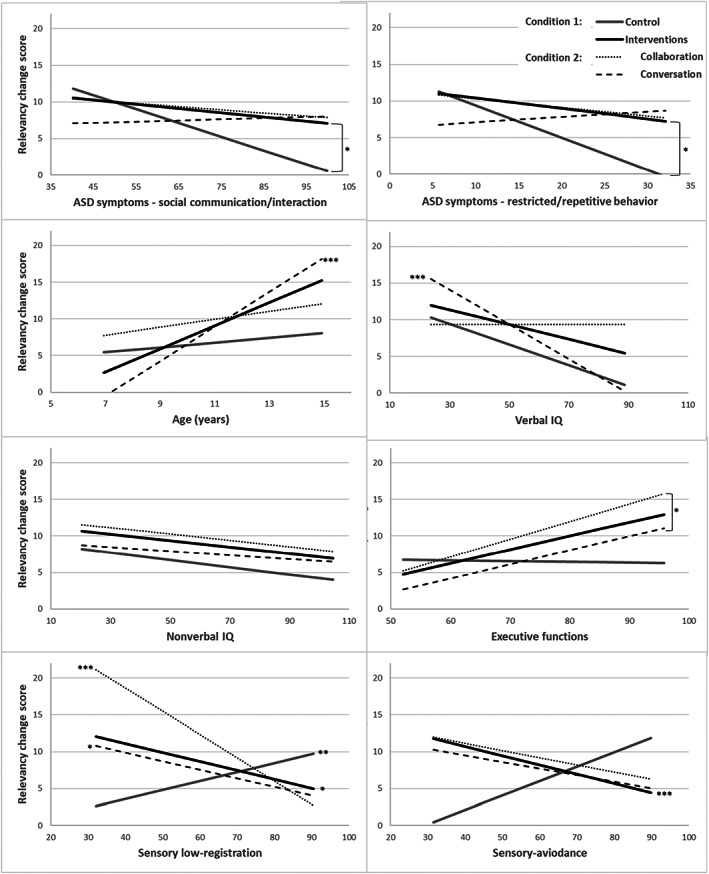
Linear modeling slopes for relevancy Progress by group as a function of endogenous factors. The nonverbal IQ predictor yielded only a significant binary effect. *p < 0.05. **p < 0.01. ***p < 0.001
Relevancy progress predictors in Condition 1 (intervention vs. control)
For Condition 1 comparing both interventions to controls (n = 54), the binary regression model predicting the odds of positive treatment responses (i.e., positive relevancy change scores) revealed a significant negative binary association with initial baseline relevancy scores, after adjusting for dyad. The odds of being positive responders decreased by 14.7% for every 1‐point increase on baseline relevancy scores (b = 0.159, p < 0.01, Odds = 0.853). Namely, children who initially demonstrated more relevant spontaneous social exchanges had lower odds of showing positive change than children who initially showed lower relevancy. The linear regression model for baseline relevancy was non‐significant (β = 0.065, p = 0.65). Also, study group revealed a significant binary effect on relevancy progress (b = 2.85, p < 0.001, Odds = 17.29), beyond endogenous predictors' effects. Thus, intervention participants were 17 times more likely to show positive progress than waitlisted children. The linear regression model for group was non‐significant (β = 1.91, p = 0.33).
Regarding endogenous predictors in Condition 1 (see Table 3), binary and linear effects for relevancy progress were nonsignificant for age, verbal IQ, and executive functioning skills. As detailed next and presented in Figure 2, five endogenous variables did contribute significantly: both autistic‐symptom severity scales (SCI, RRB), nonverbal IQ, and two sensory‐profile subscales (sensory‐avoidance, sensory low‐registration).
Specifically, both autistic‐symptom subscales revealed significant negative linear effects. Namely, as hypothesized, more intact social‐communication/interaction abilities and fewer restricted/repetitive behaviors predicted participants' larger growth in relevancy. Additionally, in line with our hypothesis, nonverbal IQ showed a significant positive binary effect; the odds of being positive responders increased by 7.4% for every 1‐point increase on nonverbal IQ.
Sensory low‐registration revealed a significant binary effect; the odds of being positive responders increased by 4.0% per 1‐point increase in adaptive sensory low‐registration scores. Moreover, examination of the significant linear interaction effect between sensory low‐registration and group suggested that larger magnitude of relevancy progress was demonstrated by intervention participants with less adaptive sensory low‐registration (lower scores) and by control group participants with more adaptive sensory low‐registration (higher scores).
Sensory‐avoidance showed significant interactions with group in both binary and linear models. Interactions indicated that these effects were nonsignificant for the control group but significant for the intervention groups. The significant binary effect for intervention participants suggested that the odds of being positive responders increased by 7.5% per 1‐point increase in adaptive sensory‐avoidance scores. The significant linear effect indicated that among intervention participants who were positive responders, less adaptive sensory‐avoidance (lower scores) contributed to larger magnitude of progress.
Relevancy progress predictors in Condition 2 (collaboration vs. conversation)
Overall, the two‐part regression analyses for Condition 2 comparing the two intervention types (n = 36) yielded nonsignificant binary (b = −0.108, p = 0.13, Odds = 0.898) and linear (β = 0.072, p = 0.56) effects for baseline relevancy scores. In addition, intervention type (collaboration versus conversation groups) also yielded non‐significant binary (b = 0.75, p = 0.535, Odds = 2.13) and linear (β = −2.05, p = 0.26) effects on progress (change score) in relevancy. Regarding endogenous predictors for Condition 2 (see Table 3), binary and linear effects were nonsignificant for both autistic‐symptom severity scales, but six endogenous variables did contribute significantly to relevancy progress (see Figure 2): age, verbal and nonverbal IQ, executive functioning skills, and two sensory‐profile subscales (sensory low‐registration, sensory‐avoidance).
Children's age showed a significant interaction with group on both binary and linear models, indicating that age effect on relevancy progress differed by intervention type. Following the conversation intervention, older participants made larger magnitude of progress than younger ones, and the odds of being positive responders increased by 1.4% per 1‐month increase in age. In contrast, in the collaboration intervention, the odds of being positive responders decreased by 5.2% per 1‐month increase in age.
Regarding IQ scores, the significant negative linear interaction effect between verbal IQ and group suggested that intervention participants with lower verbal IQ made larger magnitude of progress than those with higher verbal IQ, but only in the conversation group. Furthermore, the significant binary interaction effect of nonverbal IQ with group indicated that the odds of being positive responders decreased by 4.7% per 1‐point increase on nonverbal IQ, but again only in the conversation group.
Executive functioning skills showed a significant binary effect for both intervention groups; the odds of being positive responders decreased by 20% per 1‐point increase in executive dysfunction. A significant linear effect indicated that among positive responders in both interventions, larger executive dysfunction was associated with larger growth in relevancy.
Sensory low‐registration's significant linear interaction with group suggested that less adaptive registration of sensory cues predicted larger growth in relevancy for both groups, although this effect was stronger for the collaboration than the conversation group. Sensory‐avoidance revealed a significant binary effect; participants with more adaptive sensory‐avoidance scores had 8.4% higher odds of being positive responders, beyond intervention type.
DISCUSSION
This study's findings identified individual‐level predictors of spontaneous, attuned, participatory, and reciprocal (i.e., “relevant”) communication exchanges with peers following S‐PSI intervention applied to minimally verbal school‐age children on the autism spectrum, thereby extending Bauminger‐Zviely et al.'s (2020) group‐level RCT outcomes. Following discussion of each endogenous predictor, we suggest implications for optimizing S‐PSI personalization for this uniquely nonverbal, widely heterogeneous population.
Autistic symptoms
As hypothesized, for both intervention and control groups, greater baseline social‐communication impairment and restricted/repetitive behaviors (based on the Social Responsiveness Scale) predicted poorer progress in peer exchanges' relevancy. These results for our MVAS sample ages 8–16 years with heterogeneous IQ scores extended previous studies that correlated social‐interaction symptoms with pragmatic deficits (Miranda et al., 2020) and with shorter eye‐contact during adult‐child conversation (Jones et al., 2017), among children on the autism spectrum having IQ > 70 ages 4–13 years old. The present data suggest that severity of social‐communication/interaction difficulties contributed to communication relevancy even among these children who all lacked adequate verbal speech, and even at older ages. This highlights the importance of nonverbal components in peer‐communication exchanges across ages and functioning levels.
Interestingly, while previous research did not link restricted/repetitive behaviors with peer‐communicative exchanges, in our study this association was even stronger than for social‐communication/interaction symptoms. Perhaps such stereotyped, fixated, idiosyncratic, or ritualized behaviors play a larger role for MVAS children, who must rely more on body language and physical objects compared with more verbal children on the autism spectrum. Possibly, restricted/repetitive behaviors may interfere with the acquisition and exhibition of communication behaviors.
Chronological age
Differently from our expectations, findings demonstrated specific age patterns for each intervention. In the collaboration group, as hypothesized, younger participants had higher odds of making progress than older ones. Previous studies also demonstrated the link between younger ages and larger growth in physical proximity, joint attention, and initiation of interaction following peer‐oriented play‐based interventions for young children (2.0–6.5 years old) on the autism spectrum and their typically developing peers (Morrier & Ziegler, 2018; Strauss et al., 2014). However, in the conversation intervention, older participants unexpectedly exhibited better odds for growth than younger ones. This different age pattern may stem from the two interventions' differing contents and activities, despite their shared format, principles, and aims. The conversation intervention, targeting language‐pragmatics capabilities via board/memory games and visual symbols/signs, was inherently more pedagogically structured than the collaboration intervention targeting joint action and companionship via motoric activities and musical games. Perhaps the more structured, didactic pragmatics‐based conversation intervention offered more benefit to older MVAS children, prompting better progress on communicational exchanges based on social conversation, whereas the more playful sensorimotor‐based collaboration intervention offered better fit with the needs of younger school‐age MVAS participants. This calls for further examination.
IQ and executive functions
One unexpected finding was the negative association found for executive functioning with children's growth in exchanges' relevancy following each S‐PSI intervention. Both conversation and collaboration participants demonstrated better progress when they began with larger executive functioning impairments.
Considering this trend for both interventions, the S‐PSI appeared not only to address cognitive deficits in MVAS but also may have strengthened some executive functioning abilities. Perhaps the interventions' demanding conceptual learning and social‐interaction skill practice (see Appendix A and Bauminger‐Zviely et al., 2020) helped children to organize, plan, and monitor their thoughts and actions toward the self and others. The same trend was found for IQ, but only for the conversation group, in which those participants that started initially with lower verbal IQ manifested larger relevancy growth and those with nonverbal IQ were more likely to make progress in exchanges' relevancy.
Previously, higher cognitive abilities (e.g., executive functions, verbal and nonverbal IQ) were widely associated with better social‐adaptive abilities, including specific communication and social‐engagement behaviors, among individuals with ASD with diverse verbal, functional, and cognitive abilities (Bertollo & Yerys, 2019; Frost et al., 2017; Kasari et al., 2013; Pecukonis et al., 2019; Ruble & McGrew, 2013; Soorya et al., 2015). However, these prior findings mostly described child‐adult interaction and/or verbally fluent participants, and only two reported treatment outcomes. This paucity of peer‐oriented social‐skills intervention studies, alongside the difficulties in conducting reliable cognitive assessments for school‐age MVAS (Courchesne et al., 2015, 2019; Plesa Skwerer et al., 2016), highlights the crucial need for further investigation of the role played by verbal and nonverbal IQ for social functioning in this population.
In addition, when comparing both interventions to the control group, a group‐independent binary effect indicated that higher baseline nonverbal IQ increased the odds of making progress in relevancy, beyond group. This may partially reflect that, in the absence of intervention, the control group participants' progress in social behavior depends on higher IQ, as expected.
Sensory‐processing
Unexpectedly, in both intervention groups, children's less adaptive sensory‐processing profiles (lower scores on sensory‐avoidance and sensory low‐registration) contributed to larger growth in exchanges' relevancy. However, as hypothesized, control group participants' smaller sensory low‐registration deficits contributed to larger growth. Overall, this trend corresponds with that found for executive functioning in both intervention groups and for verbal and nonverbal IQ in the conversation group, where higher baseline deficits predicted greater capitalization on intervention alongside smaller progress in the absence of intervention. Taken together, natural progress in social‐communication behavior among MVAS children, without any intervention, appears to be hindered by greater sensory and/or cognitive difficulties. Yet, more importantly, we suggest that S‐PSI intervention can lead to progress in social‐engagement behaviors by overcoming sensory barriers as it offers diverse interaction modalities that might address the different sensory channels of school‐age MVAS participants.
Furthermore, as with the cognitive predictors (executive functions, IQ), these findings are not in line with earlier research including children on the autism spectrum ages 3–12 years, which reported sensory‐processing deficits' broad associations with greater social impairment, poorer adaptive skills (Dellapiazza et al., 2019; Kojovic et al., 2019), fewer joint play behaviors, and briefer cooperative play (Corbett et al., 2016; Williams et al., 2018), although these were not intervention studies. The current findings showing sensory difficulties' contribution to treatment progress suggest that our intervention promoting regulation and organization may lead to more socially adaptive behavior among those with larger sensory barriers.
Who benefits from S‐PSI?
Overall, our findings suggest that untreated school‐age MVAS children (controls) seemed to best progress in their social‐engagement skills if initially they had lower autistic‐symptom severity and demonstrated higher nonverbal IQ and more adaptive sensory low‐registration behavior. Among children who participated in one of the two treatments, those having lower autistic symptomatology and greater difficulties in executive functioning and sensory processing made larger progress. Notably, progress in exchanges' relevancy was affected by the endogenous factors more for the conversation than the collaboration group. Younger children seemed to benefit most from the collaboration‐based intervention, which offered them physical‐motor and musical activities and games. This intervention may have been more age‐appropriate and motivational for the younger school‐age MVAS participants. Finally, children who were older and who revealed lower verbal and nonverbal IQ seemed to benefit most from the conversation‐based language‐pragmatic intervention, which appeared to offer them a more demanding didactic experience. Both interventions, particularly the conversation one, appeared to influence implicit cognitive and sensory skills that are associated with conversational skills: regulation, planning, organization, and monitoring.
Study limitations and implications
The original sample size was decreased by focusing on positive treatment responders in the linear model, thus possibly reducing potential associations between variables. Small sample size also precluded examination of multiple endogenous factors in each regression analysis, thereby limiting investigation of their more complex associations and joint effects. Also, it prevented the ability to account for nesting within schools in addition to the dyadic design of the experiment. Further studies should consider larger samples to enable such analyses. Also, due to the paucity of prior intervention studies for promoting peers' social engagement in this population, additional studies are needed to replicate the current novel findings and their possible implications. It would also be interesting to expand beyond the current fixed dyads by examining peer interactions with an additional partner, to elucidate interventions' generalizability to other peer relationships.
This study holds empirical and clinical implications. First, some unexpected associations emerged between endogenous factors in school‐age MVAS children and their ability to capitalize on the two S‐PSI modalities that offered alternatives to spoken words to improve communicational exchanges in peer dyads. Future researchers should explore how specific intervention features directed to this population's core social‐deficit and unique nonverbal characteristics may contribute optimally to treatment outcomes. For example, perhaps the structured didactic format of the conversational‐pragmatic intervention helps children compensate for executive and sensory difficulties, thus achieving better social‐engagement skills.
Moreover, growth in relevancy is related to the ability to hold, maintain, and develop the chains of communication, which are important to enhance children's capacity to become involved in meaningful interactions thereby potentially reducing the risk for social isolation. The real‐world meaning of these findings, then, is, that those children who had more sensory challenges such as irregular patterns of registration and/or avoidance, and those who had executive issues such as lack of organization and planning, were able to overcome their barriers and show growth in their coordinated peer‐to‐peer interaction. This is an optimistic finding about pathways toward developmental growth despite personal barriers.
In addition, variability in treatment responses to the various endogenous predictors indicate individual differences in participants' needs, emphasizing the necessity to maximize treatment–person fit and tailor intervention modalities to children's individual characteristics. Furthermore, the current findings on this under‐investigated population (Tager‐Flusberg & Kasari, 2013) suggest that school‐age MVAS children can make progress in social engagement despite increasing age, cognitive and sensory difficulties, and, most importantly, lack of spoken words. Hence, these children need experiences promoting peer engagement alongside their other training domains such as academic and daily‐living skills. In conclusion, personalizing interventions to better improve social‐engagement skills may result in reduced social isolation and loneliness and enhanced well‐being.
ETHIC STATEMENT
All procedures for data collection were approved by the chief scientist of the Ministry of Education.
ACKNOWLEDGMENTS
Special thanks are extended to Yael Estrugo, Karen Samuel‐Magal, Avner Friedlin, Lior Heishrik, Dror Koren and Shahar Bar–Yehuda for their contribution to the S‐PSI intervention's development and evaluation. We express our appreciation to Dee B. Ankonina for her editorial contribution and to Dr. Gabi Liberman and Amir Hefetz for their statistical consultation.
APPENDIX A.
S‐PSI Interventions' Principles and Content
| Context shared by both interventions a | Both of the manualized S‐PSI treatment conditions (conversation and collaboration) included 60 lessons delivered to each peer dyad separately by special education teachers. Dyads were extracted from class for 1‐h lessons held four times per week over 15 weeks in their educational settings during school hours. Interventionists were supervised and guided by the research team every second week. | |
| Principles shared by both interventions |
Emphasis was on peer‐peer interaction, with the special education teacher mediating the intervention. The special education teacher presented the activity and then faded out while the two children interacted with each other. Activities used many repetitions. Contents comprised fun activities and games; visual stimuli and symbols; musical, rhythmic, and movement tasks/games, Activities were chosen based on children's chronological/mental age. Every lesson included learning and practicing. Gestures were taught, such as touching your partner's arm to draw attention and pointing at an object. |
|
|
Differing contents over 7 intervention units |
S‐PSI: Conversation | S‐PSI: Collaboration |
|
Units 1–2: Conceptual understanding (what is a social conversation?) and rules for conversation (e.g., taking turns, maintaining eye contact, listening) Units 3–5: Conversational components: initiating a conversation; topics of conversation; and developing and maintaining conversation adequately (conveying information, emotions, and content; switching between topics) Unit 6: Asking questions Unit 7: Ending a conversation and closure activities |
Unit 1: Creating “team spirit” (get‐acquainted games, group name, group rules) Units 2–3: Experiencing and understanding shared tasks with emphasis on mutual planning and joint action Units 4–6: Developing prosocial skills: sharing, helping, encouraging Unit 7: Closure activities |
|
|
Lesson example |
What is a conversation?
Gradually, each dyad expanded its communication board with contents related to conversation (possible topics, opening sentences, sentences to use for switching between topics, WH‐questions, elaborations, closure sentences). |
What is collaboration?
Gradually, each dyad expanded its communication board with contents related to collaboration (giving and getting help, comforting, collaborating, and sharing). |
Note: Context for the control group: Peer dyads continued treatment‐as‐usual in their educational settings, which did not include any specific intervention targeted to facilitate peer interaction.
Kedar, M. , & Bauminger‐Zviely, N. (2023). Predictors of individual differences in minimally verbal peer communication exchanges following peer‐oriented social intervention. Autism Research, 16(1), 230–244. 10.1002/aur.2852
DATA AVAILABILITY STATEMENT
Data sharing is not available due to restriction of the country's ministry of education on children's information.
REFERENCES
- American Psychological Association. (2000). Diagnostic and statisticalmanual of mental disorders (4th ed., text rev.). Washington, DC: American Psychological Association. [Google Scholar]
- American Psychiatric Association . (2013). Diagnostic and statistical manual of mental disorders (DSM‐5). American Psychiatric Publishing. 10.1176/appi.books.9780890425596.744053 [DOI] [Google Scholar]
- Bahrami, F. , Movahedi, A. , Marandi, S. M. , & Sorensen, C. (2016). The effect of karate techniques training on communication deficit of children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 46(3), 978–986. 10.1007/s10803-015-2643-y [DOI] [PubMed] [Google Scholar]
- Bal, V. H. , Katz, T. , Bishop, S. L. , & Krasileva, K. (2016). Understanding definitions of minimally verbal across instruments: Evidence for subgroups within minimally verbal children and adolescents with autism spectrum disorder. Journal of Child Psychology and Psychiatry, 57(12), 1424–1433. 10.1111/jcpp.12609 [DOI] [PubMed] [Google Scholar]
- Bauminger‐Zviely, N. (2013). Social and academic abilities in children with high‐functioning autism spectrum disorders (Vol. 14, pp. 274–275). Guilford Press. 10.1111/1471-3802.12082 [DOI] [Google Scholar]
- Bauminger‐Zviely, N. , Estrugo, Y. , Samuel‐Magal, K. , & Friedlin, A. (2015). The school‐based peer social intervention (S‐PSI) [unpublished protocol]. School of Education. Bar‐Ilan University. [Google Scholar]
- Bauminger‐Zviely, N. , Estrugo, Y. , Samuel‐Magal, K. , Friedlin, A. , Heishrik, L. , Koren, D. , & Bar‐Yehuda, S. (2020). Communicating without words: School‐based RCT social intervention in minimally verbal peer dyads with ASD. Journal of Clinical Child & Adolescent Psychology, 49, 837–853. 10.1080/15374416.2019.1660985 [DOI] [PubMed] [Google Scholar]
- Bednarz, H. M. , Trapani, J. A. , & Kana, R. K. (2020). Metacognition and behavioral regulation predict distinct aspects of social functioning in autism spectrum disorder. Child Neuropsychology, 26(7), 953–981. 10.1080/09297049.2020.1745166 [DOI] [PubMed] [Google Scholar]
- Ben‐Itzchak, E. , & Zachor, D. A. (2020). Toddlers to teenagers: Long‐term follow‐up study of outcomes in autism spectrum disorder. Autism, 24(1), 41–50. 10.1177/1362361319840226 [DOI] [PubMed] [Google Scholar]
- Bertollo, J. R. , & Yerys, B. E. (2019). More than IQ: Executive function explains adaptive behavior above and beyond nonverbal IQ in youth with autism and lower IQ. American Journal on Intellectual and Developmental Disabilities, 124(3), 191–205. 10.1352/1944-7558-124.3.191 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blozis, S. A. , McTernan, M. , Harring, J. R. , & Zheng, Q. (2020). Two‐part mixed‐effects location scale models. Behavior Research Methods, 52(5), 1836–1847. 10.3758/s13428-020-01359-7 [DOI] [PubMed] [Google Scholar]
- Brown, N. B. , & Dunn, W. (2010). Relationship between context and sensory processing in children with autism. American Journal of Occupational Therapy, 64(3), 474–483. 10.5014/ajot.2010.09077 [DOI] [PubMed] [Google Scholar]
- Cangur, S. , Ankarali, H. , & Pasin, O. (2016). Comparing performances of multiple comparison methods in commonly used 2 × C contingency tables. Interdisciplinary Sciences: Computational Life Sciences, 8, 337–345. 10.1007/s12539-015-0128-5 [DOI] [PubMed] [Google Scholar]
- Capps, L. , Kehres, J. , & Sigman, M. (1998). Conversational abilities among children with autism and children with developmental delays. Autism, 2, 325–344. 10.1177/1362361398024002 [DOI] [Google Scholar]
- Chan, W. , Smith, L. E. , Hong, J. , Greenberg, J. S. , & Mailick, M. R. (2017). Validating the social responsiveness scale for adults with autism. Autism Research, 10(10), 1663–1671. 10.1002/aur.1813 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chang, Y. C. , Shih, W. , Landa, R. , Kaiser, A. , & Kasari, C. (2018). Symbolic play in school‐aged minimally verbal children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 48(5), 1436–1445. 10.1007/s10803-017-3388-6 [DOI] [PubMed] [Google Scholar]
- Charman, T. , Loth, E. , Tillmann, J. , Crawley, D. , Wooldridge, C. , Goyard, D. , Ahmad, J. , Auyeung, B. , Ambrosino, S. , Banaschewski, T. , Baron‐Cohen, S. , Baumeister, S. , Beckmann, C. , Bölte, S. , Bourgeron, T. , Bours, C. , Brammer, M. , Brandeis, D. , Brogna, C. , … Buitelaar, J. K. (2017). The EU‐AIMS longitudinal European autism project (LEAP): Clinical characterisation. Molecular Autism, 8(1), 27. 10.1186/s13229-017-0145-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chenausky, K. , Norton, A. , Tager‐Flusberg, H. , & Schlaug, G. (2018). Behavioral predictors of improved speech output in minimally verbal children with autism. Autism Research, 11(10), 1356–1365. 10.1002/aur.2006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Constantino, J. N. , & Gruber, C. P. (2012). Social responsiveness scale: SRS‐2. Western Psychological Services. [Google Scholar]
- Corbett, B. A. , Muscatello, R. A. , & Blain, S. D. (2016). Impact of sensory sensitivity on physiological stress response and novel peer interaction in children with and without autism spectrum disorder. Frontiers in Neuroscience, 10, 278. 10.3389/fnins.2016.00278 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Courchesne, V. , Girard, D. , Jacques, C. , & Soulières, I. (2019). Assessing intelligence at autism diagnosis: Mission impossible? Testability and cognitive profile of autistic preschoolers. Journal of Autism and Developmental Disorders, 49(3), 845–856. 10.1007/s10803-018-3786-4 [DOI] [PubMed] [Google Scholar]
- Courchesne, V. , Meilleur, A. A. S. , Poulin‐Lord, M. P. , Dawson, M. , & Soulières, I. (2015). Autistic children at risk of being underestimated: School‐based pilot study of a strength‐informed assessment. Molecular Autism, 6(1), 12. 10.1186/s13229-015-0006-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dellapiazza, F. , Michelon, C. , Oreve, M.‐J. , Robel, L. , Schoenberger, M. , Chatel, C. , Vesperini, S. , Maffre, T. , Schmidt, R. , Blanc, N. , Vernhet, C. , Picot, M.‐C. , & Baghdadli, A. (2019). The impact of atypical sensory processing on adaptive functioning and maladaptive behaviors in autism spectrum disorder during childhood: Results from the ELENA cohort. Journal of Autism and Developmental Disorders, 50(6), 2142–2152. 10.1007/s10803-019-03970-w [DOI] [PubMed] [Google Scholar]
- Dellapiazza, F. , Michelon, C. , Vernhet, C. , Muratori, F. , Blanc, N. , Picot, M. C. , & Baghdadli, A. (2020). Sensory processing related to attention in children with ASD, ADHD, or typical development: Results from the ELENA cohort. European Child & Adolescent Psychiatry, 30(2), 283–291. 10.1007/s00787-020-01516-5 [DOI] [PubMed] [Google Scholar]
- DiStefano, C. , Shih, W. , Kaiser, A. , Landa, R. , & Kasari, C. (2016). Communication growth in minimally verbal children with ASD: The importance of interaction. Autism Research, 9(10), 1093–1102. 10.1002/aur.1594 [DOI] [PubMed] [Google Scholar]
- Dunn, L. M. , & Dunn, L. M. (1997). Examiner's manual for the Peabody picture vocabulary test (Third ed.). American Guidance Service. [Google Scholar]
- Dunn, W. (2006). Sensory profile school companion user's manual. Psych Corp Harcourt Assessment. [Google Scholar]
- Farewell, V. , Long, D. , Tom, B. , Yiu, S. , & Su, L. (2017). Two‐part and related regression models for longitudinal data. Annual Review of Statistics and Its Application, 4(1), 283–315. 10.1146/annurev-statistics-060116-054131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedman, L. , & Sterling, A. (2019). A review of language, executive function, and intervention in autism spectrum disorder. Seminars in Speech and Language, 40(4), 291–304. 10.1055/s-0039-1692964 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frost, K. M. , Hong, N. , & Lord, C. (2017). Correlates of adaptive functioning in minimally verbal children with autism spectrum disorder. American Journal on Intellectual and Developmental Disabilities, 122(1), 1–10. 10.1352/1944-7558-122.1.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gioia, G. A. , Isquith, P. K. , Guy, S. C. , & Kenworthy, L. (2000). Behavior rating inventory of executive function. Child Neuropsychology, 6, 235–238. 10.1076/chin.6.3.235.3152 [DOI] [PubMed] [Google Scholar]
- Grzadzinski, R. L. (2018). Measuring change in social communication behaviors: Reliability, validity, and application [Unpublished doctoral dissertation]. Columbia University. 10.7916/D8WT09ZN [DOI] [Google Scholar]
- Hilton, C. L. , Harper, J. D. , Kueker, R. H. , Lang, A. R. , Abbacchi, A. M. , Todorov, A. , & Lavesser, P. D. (2010). Sensory responsiveness as a predictor of social severity in children with high functioning autism spectrum disorders. Journal of Autism and Developmental Disorders, 40(8), 937–945. 10.1007/s10803-010-0944-8 [DOI] [PubMed] [Google Scholar]
- Howlin, P. , Mawhood, L. , & Rutter, M. (2000). Autism and developmental receptive language disorder—A follow‐up comparison in early adult life. II: Social, behavioural, and psychiatric outcomes. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 41(5), 561–578. 10.1111/1469-7610.00643 [DOI] [PubMed] [Google Scholar]
- Jones, R. M. , Southerland, A. , Hamo, A. , Carberry, C. , Bridges, C. , Nay, S. , Stubbs, E. , Komarow, E. , Washington, C. , Rehg, J. M. , Lord, C. , & Rozga, A. (2017). Increased eye contact during conversation compared to play in children with autism. Journal of Autism and Developmental Disorders, 47(3), 607–614. 10.1007/s10803-016-2981-4 [DOI] [PubMed] [Google Scholar]
- Kasari, C. , Brady, N. , Lord, C. , & Tager‐Flusberg, H. (2013). Assessing the minimally verbal school‐aged child with autism spectrum disorder. Autism Research, 6(6), 479–493. 10.1002/aur.1334 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kasari, C. , Kaiser, A. , Goods, K. , Nietfeld, J. , Mathy, P. , Landa, R. , Murphy, S. , & Almirall, D. (2014). Communication interventions for minimally verbal children with autism: A sequential multiple assignment randomized trial. Journal of the American Academy of Child & Adolescent Psychiatry, 53(6), 635–646. 10.1016/j.jaac.2014.01.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kimhi, Y. , Shoam‐Kugelmas, D. , Agam Ben‐Artzi, G. , Ben‐Moshe, I. , & Bauminger‐Zviely, N. (2014). Theory of mind and executive function in preschoolers with typical development versus intellectually able preschoolers with autism spectrum disorder. Journal of Autism and Developmental Disorders, 44(9), 2341–2354. 10.1007/s10803-014-2104-z [DOI] [PubMed] [Google Scholar]
- Koegel, L. K. , Bryan, K. M. , Su, P. L. , Vaidya, M. , & Camarata, S. (2020). Definitions of nonverbal and minimally verbal in research for autism: A systematic review of the literature. Journal of Autism and Developmental Disorders, 50, 2957–2972. 10.1007/s10803-020-04402-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kojovic, N. , Ben Hadid, L. , Franchini, M. , & Schaer, M. (2019). Sensory processing issues and their association with social difficulties in children with autism spectrum disorders. Journal of Clinical Medicine, 8(10), 1508. 10.3390/jcm8101508 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miranda, A. , Berenguer, C. , Roselló, B. , & Baixauli, I. (2020). Relationships between the social communication questionnaire and pragmatic language, socialization skills, and behavioral problems in children with autism spectrum disorders. Applied Neuropsychology: Child, 9(2), 141–152. 10.1080/21622965.2018.1550403 [DOI] [PubMed] [Google Scholar]
- Morrier, M. J. , & Ziegler, S. M. T. (2018). I wanna play too: Factors related to changes in social behavior for children with and without autism spectrum disorder after implementation of a structured outdoor play curriculum. Journal of Autism and Developmental Disorders, 48(7), 2530–2541. 10.1007/s10803-018-3523-z [DOI] [PubMed] [Google Scholar]
- Muthén, B. O. , Muthén, L. K. , & Asparouhov, T. (2016). Regression and mediation analysis using Mplus. Muthén & Muthén. [Google Scholar]
- Pecukonis, M. , Plesa Skwerer, D. , Eggleston, B. , Meyer, S. , & Tager‐Flusberg, H. (2019). Concurrent social communication predictors of expressive language in minimally verbal children and adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders, 49(9), 3767–3785. 10.1007/s10803-019-04089-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plavnick, J. B. , Kaid, T. , & Mac Farland, M. C. (2015). Effects of a school‐based social skills training program for adolescents with autism spectrum disorder and intellectual disability. Journal of Autism and Developmental Disorders, 45(9), 2674–2690. 10.1007/s10803-015-2434-5 [DOI] [PubMed] [Google Scholar]
- Plesa Skwerer, D. , Jordan, S. E. , Brukilacchio, B. H. , & Tager‐Flusberg, H. (2016). Comparing methods for assessing receptive language skills in minimally verbal children and adolescents with autism spectrum disorders. Autism, 20(5), 591–604. 10.1177/1362361315600146 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pugliese, C. E. , Anthony, L. , Strang, J. F. , Dudley, K. , Wallace, G. L. , & Kenworthy, L. (2015). Increasing adaptive behavior skill deficits from childhood to adolescence in autism spectrum disorder: Role of executive function. Journal of Autism and Developmental Disorders, 45(6), 1579–1587. 10.1007/s10803-014-2309-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raven, J. , Raven, J. C. , & Court, J. H. (1998). Raven manual: Section 4, advanced progressive matrices. Oxford Psychologists Press. 10.1007/978-1-4614-2332-4 [DOI] [Google Scholar]
- Ruble, L. , & McGrew, J. H. (2013). Teacher and child predictors of achieving IEP goals of children with autism. Journal of Autism and Developmental Disorders, 43(12), 2748–2763. 10.1007/s10803-013-1884-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rutter, M. , Bailey, A. , & Lord, C. (2003). Social Communication Questionnaire (SCQ). Western Psychological Services. [Google Scholar]
- Sanz‐Cervera, P. , Pastor‐Cerezuela, G. , González‐Sala, F. , Tárraga‐Mínguez, R. , & Fernández‐Andrés, M. I. (2017). Sensory processing in children with autism spectrum disorder and/or attention deficit hyperactivity disorder in the home and classroom contexts. Frontiers in Psychology, 8, 1772. 10.3389/fpsyg.2017.01772 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sauzet, O. , Razum, O. , Widera, T. , & Brzoska, P. (2019). Two‐part models and quantile regression for the analysis of survey data with a spike: The example of satisfaction with health care. Frontiers in Public Health, 7, 146. 10.3389/fpubh.2019.00146 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soorya, L. V. , Siper, P. M. , Beck, T. , Soffes, S. , Halpern, D. , Gorenstein, M. , Kolevzon, A. , Buxbaum, J. , & Wang, A. T. (2015). Randomized comparative trial of a social cognitive skills group for children with autism spectrum disorder. Journal of the American Academy of Child & Adolescent Psychiatry, 54(3), 208–216. 10.1016/j.jaac.2014.12.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strauss, K. , Esposito, M. , Polidori, G. , Vicari, S. , Valeri, G. , & Fava, L. (2014). Facilitating play, peer engagement and social functioning in a peer group of young autistic children: Comparing highly structured and more flexible behavioral approaches. Research in Autism Spectrum Disorders, 8(4), 413–423. 10.1016/j.rasd.2014.01.002 [DOI] [Google Scholar]
- Tager‐Flusberg, H. , & Kasari, C. (2013). Minimally verbal school‐aged children with autism spectrum disorder: The neglected end of the spectrum. Autism Research, 6(6), 468–478. 10.1002/aur.1329 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tager‐Flusberg, H. , Plesa Skwerer, D. , Joseph, R. M. , Brukilacchio, B. , Decker, J. , Eggleston, B. , Meyer, S. , & Yoder, A. (2017). Conducting research with minimally verbal participants with autism spectrum disorder. Autism, 21(7), 852–861. 10.1177/1362361316654605 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thye, M. D. , Bednarz, H. M. , Herringshaw, A. J. , Sartin, E. B. , & Kana, R. K. (2018). The impact of atypical sensory processing on social impairments in autism spectrum disorder. Developmental Cognitive Neuroscience, 29, 151–167. 10.1016/j.dcn.2017.04.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tillmann, J. , San José Cáceres, A. , Chatham, C. H. , Crawley, D. , Holt, R. , Oakley, B. , Banaschewski, T. , Baron‐Cohen, S. , Bölte, S. , Buitelaar, J. K. , Durston, S. , Ham, L. , Loth, E. , Simonoff, E. , Spooren, W. , Murphy, D. G. , Charman, T. , Ahmad, J. , Ambrosino, S. , … Zwiers, M. P. (2019). Investigating the factors underlying adaptive functioning in autism in the EU‐AIMS longitudinal European autism project. Autism Research, 12(4), 645–657. 10.1002/aur.2081 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams, K. L. , Kirby, A. V. , Watson, L. R. , Sideris, J. , Bulluck, J. , & Baranek, G. T. (2018). Sensory features as predictors of adaptive behaviors: A comparative longitudinal study of children with autism spectrum disorder and other developmental disabilities. Research in Developmental Disabilities, 81, 103–112. 10.1016/j.ridd.2018.07.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zou, M. , Sun, C. , Wang, J. , Kang, J. , Xu, Z. , Ma, Y. , Chen, L. , Zhang, X. , Xia, W. , & Wu, L. (2018). Factors influencing the severity of behavioral phenotype in autism spectrum disorders: Implications for research. Psychiatry Research, 261, 290–297. 10.1016/j.psychres.2017.12.084 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing is not available due to restriction of the country's ministry of education on children's information.