

Abstract
Introduction
Drooling in Parkinson's disease (PD) is frequent but often goes underrecognized. Our aim was to examine the prevalence of drooling in a PD cohort and compare it with a control group. Specifically, we identified factors associated with drooling and conducted subanalyses in a subgroup of very early PD patients. Patients and Methods. PD patients who were recruited from January 2016 to November 2017 (baseline visit; V0) and evaluated again at a 2-year ± 30-day follow-up (V2) from 35 centers in Spain from the COPPADIS cohort were included in this longitudinal prospective study. Subjects were classified as with or without drooling according to item 19 of the NMSS (Nonmotor Symptoms Scale) at V0, V1 (1-year ± 15 days), and V2 for patients and at V0 and V2 for controls.
Results
The frequency of drooling in PD patients was 40.1% (277/691) at V0 (2.4% (5/201) in controls; p < 0.0001), 43.7% (264/604) at V1, and 48.2% (242/502) at V2 (3.2% (4/124) in controls; p < 0.0001), with a period prevalence of 63.6% (306/481). Being older (OR = 1.032; p = 0.012), being male (OR = 2.333; p < 0.0001), having greater nonmotor symptom (NMS) burden at the baseline (NMSS total score at V0; OR = 1.020; p < 0.0001), and having a greater increase in the NMS burden from V0 to V2 (change in the NMSS total score from V0 to V2; OR = 1.012; p < 0.0001) were identified as independent predictors of drooling after the 2-year follow-up. Similar results were observed in the group of patients with ≤2 years since symptom onset, with a cumulative prevalence of 64.6% and a higher score on the UPDRS-III at V0 (OR = 1.121; p = 0.007) as a predictor of drooling at V2.
Conclusion
Drooling is frequent in PD patients even at the initial onset of the disease and is associated with a greater motor severity and NMS burden.
1. Introduction
Sialorrhea, commonly referred to as drooling, is defined as excessive saliva beyond the margin of the lip. Drooling can be a complication of Parkinson's disease (PD) and is one of the most prevalent complaints of patients, but it is often underrecognized and undertreated [1]. A wide prevalence range has been reported in the literature, ranging from 10 to 84%, with no significant variation across ethnic groups [2–15]. However, when studies compared PD patients with controls, drooling only occurred in 6–15% of people without PD [5, 6, 15, 16]. The broad range in PD patients is likely due to the lack of a standard definition of and diagnostic criteria for sialorrhea and the differences in the PD population studied and the methods used. Despite these obstacles, drooling has still been found to negatively impact the quality of life (QoL) of both patients and caregivers [5, 12, 13, 17–19]. Sialorrhea may bring repercussions for the psychosocial health of the person who drools and added burden for the caregiver as well (e.g., odor, stained clothes, constant wiping, restricted social life, etc.) [1]. Moreover, drooling is associated with an increased risk of dry mouth, impact on bolus formation, loss of antibacterial effects of saliva, perioral dermatological changes, ulceration, tooth decay, gingivitis, dehydration, candidiasis, halitosis, and increased speech difficulties [20–22]. Drooling in PD patients appears to be primarily related to reduced swallowing efficiency and not to an increase in saliva production [20, 23], as dysphagia is the strongest factor associated with drooling [7, 12, 23]. Other reported factors associated with drooling are orofacial rigidity/hypomimia, lingual bradykinesia, aging, male gender, cognitive impairment, hallucinations, nontremor dominant PD phenotype, longer disease duration, and more advanced disease stage [3–8, 11–14, 23–26].
Although many studies have analyzed the frequency of drooling in PD, there is less information about its prevalence and associated factors in early PD patients and how it impacts QoL and change over time. Some studies have reported a prevalence of about 20% in de novo and untreated PD patients and that prevalence increases in the long term [27, 28]. Our hypothesis was that the prevalence of drooling in early PD patients would be high and would negatively impact QoL. The aim of the current study was to examine the prevalence of drooling, and its progression, in a PD cohort and assess its impact on QoL. Furthermore, we compared the frequency of drooling in PD patients with a control group and analyzed all these aspects in a subgroup of patients from the cohort with a short disease duration of ≤2 years since the onset of the symptoms. Moreover, we identified in both groups, the entire cohort and the subgroup with early PD, factors associated with not only drooling but also drooling severity as well.
2. Materials and Methods
PD patients who were recruited from January 2016 to November 2017 (baseline visit; V0) and evaluated again at a 2-year ± 30-day follow-up (V2) from 35 centers in Spain from the COPPADIS cohort [29] were included in this study. The methodology of the COPPADIS-2015 study can be consulted in https://bmcneurol.biomedcentral.com/articles/10.1186/s12883-016-0548-9 [30]. This is a multicenter, observational, longitudinal prospective, and 5-year follow-up study designed to analyze disease progression in a Spanish population of PD patients. All patients included were diagnosed according to the UK PD Brain Bank criteria [31].
Information on sociodemographic aspects, factors related to PD, comorbidity, and treatment were collected. Motor status, nonmotor symptoms (NMS), QoL, and disability were assessed at V0 and at V2 using different validated scales: Hoehn and Yahr (H&Y), UPDRS-III and UPDRS-IV, Freezing of Gait Questionnaire (FOGQ)), Parkinson's Disease Cognitive Rating Scale (PD-CRS), Nonmotor Symptoms Scale (NMSS), Beck Depression Inventory-II (BDI-II), Parkinson's disease sleep scale (PDSS), Neuropsychiatric Inventory (NPI), Questionnaire for impulsive-compulsive disorders in Parkinson's Disease-Rating Scale (QUIP-RS), visual analog scale-pain (VAS-Pain), Visual Analog Fatigue Scale (VAFS)), the 39-item Parkinson's Disease Questionnaire (PDQ-39), the EUROHIS-QOL 8-item index (EUROHIS-QOL8), and ADLS (Schwab and England Activities of Daily Living Scale) [30]. In patients with motor fluctuations, the motor assessment was made during the OFF state (without medication in the last 12 hours) and during the ON state. The assessment was only performed without medication in patients without motor fluctuations. The same evaluation as for the patients, except for the motor assessment, was performed in control subjects at V0 and at V2 (2 years ± 1 month). Furthermore, motor (H&Y, UPDRS-III, and UPDRS-IV) and nonmotor assessment (NMSS and ADLS) was conducted in PD patients at 1 year ± 1 month (V1) [30]. LEED was calculated based on the literature [32].
Subjects were classified as with or without drooling according to item 19 of the NMSS [33]. This item is one of the 30 items on this scale and is included in domain 6 (gastrointestinal tract). This question asks about drooling: “Does the patient dribble saliva during the day?.” The score range is from 0 (without the symptom) to 12 (the most frequent and severe). Subjects with an NMSS-item 19 score = 0 were considered “without drooling,” whereas subjects with an NMSS-item 19 score ≥1 (from 1 to 12) were considered “with drooling.” Drooling was identified at V0, V1, and V2 in patients and at V0 and V2 in controls. The drooling burden was also calculated for PD patients. The score at V0, V1, and V2 and the sum of the score from the three visits (NMSS-DroolingV0+V1+V2, from 0 to 36) were calculated. Patients reporting drooling during the three visits were defined as patients with “persistent drooling.” The same method was used to define dysphagia (item 20 of the NMSS) [34] and hypomimia (item 19 of the UPDRS-III during the OFF state) [35].
2.1. Statistical Analysis
Data were processed using SPSS 20.0 for Windows. For comparisons between PD patients in the control group and PD patients with and without drooling, the Student's t-test, Mann–Whitney U test, chi-square test, or Fisher test were used as appropriate (distribution for variables was verified by one-sample Kolmogorov–Smirnov test).
Binary and linear regression models were used for determining independent factors associated with drooling (drooling as the dependent variable) and drooling severity (NMSS-DroolingV0+V1+V2 score as the dependent variable), respectively. Variables with univariate associations with p values <0.20 were included in a multivariable model, and a backward selection process was used to remove variables individually until all remaining variables were significant at the 0.10 level. For exploring the association between drooling and QoL, linear regression models were used with PDQ-39SI (health-related QoL) and EUROHIS-QOL8 (global QoL) as dependent variables. The total domain scores of the PDQ-39 were expressed as a percentage of the corresponding maximum possible score, and a summary index was obtained as an average of the domain scores (PDQ-39SI). The effect was controlled by age, gender, disease duration, LEDD, comorbidities (total number of non-anti-Parkinsonian drugs [36]), motor (H&Y, UPDRS-III, UPDRS-IV, and FOGQ) and nonmotor (NMSS) status, cognitive function (PC-CRS total score), dysphagia, hypomimia, and autonomy for ADL (ADLS), which were included as covariates in the model [36].
For PD patients, analyses were conducted in the entire cohort and in the subgroup of patients with ≤2 years of disease duration since symptoms' onset (PD ≤ 2 y) at the baseline. The p value was considered significant for all analyses when it was <0.05.
2.2. Standard Protocol Approvals, Registrations, and Patient Consents
For this study, we received approval from the Comité de Ética de la Investigación Clínica de Galicia in Spain (2014/534; 02/DEC/2014). Written informed consents from all participants in this study were obtained. COPPADIS-2015 was classified by the AEMPS (Agencia Española del Medicamento y Productos Sanitarios) as a postauthorization prospective follow-up study with the code COH-PAK-2014-01.
3. Results
At the baseline, 691 PD patients (62.59 ± 8.92 years old; 60.2% males; mean disease duration 5.5 ± 4.37 years) and 206 patients in the control group (60.98 ± 8.34 years old; 50% males) were considered valid for the analysis. The frequency of drooling in PD patients was 40.1% (277/691) at V0; 43.7% (264/604) at V1; 48.2% (242/502) at V2 (Figure 1(a)). At V0 and V2, drooling was significantly less frequent (p < 0.0001) in the control group than in PD patients (2.4% at V0 and 3.2% at V2 in controls). In the patients (N = 481; 62.62 ± 8.54 years old, from 35 to 75; 59.2% males) with assessments carried out during all visits (V0, V1, and V2), 63.6% (306/481) of them reported drooling at least once during the study (period prevalence). Specifically, 18.9% (91/481) in only one visit, 19.1% (92/481) in two out of the three visits, and 25.6% (123/481) in all three visits (i.e., persistent drooling) (Figure 1(b)). In the PD ≤ 2 y group (62.22 ± 8.33 years old; 57.3% males; mean disease duration 1.29 ± 0.37 years), the frequency of drooling was 34.8% (64/184) at V0, 37.5% at V1 (60/160), and 50.4% (66/131) at V2. After the 2-year follow-up, the cumulative prevalence of drooling in this group was 64.6% (21.3% in 1 visit, 23.6% in 2 visits, and 19.7% in all visits) (Figure 1(b)).
Figure 1.
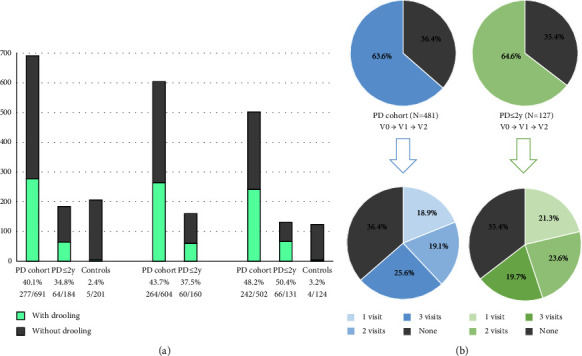
(a) Percentage of patients (the whole cohort and the group with no more than 2 years since symptom onset (PD ≤ 2 y) and controls reporting drooling at different visits: V0, V1, and V2. (b) Prevalence of drooling during the follow-up period in all patients and in the PD ≤ 2 y group who completed the three visits (V1, V2, and V3) and percentage of cases presenting drooling in only 1 visit, 2 visits, and all visits. PD cohort vs. controls at V0, p < 0.0001; PD cohort vs. controls at V2, p < 0.0001; PD ≤ 2 y group vs. controls at V0, p < 0.0001; PD ≤ 2 y group vs. controls at V2, p < 0.0001. PD: Parkinson's disease. PD ≤ 2 y group: patients with ≤2 years since symptom onset.
Regarding drooling burden in PD patients, as expected, the NMSS-DroolingV0+V1+V2 score was higher in patients with persistent drooling (p < 0.0001): drooling in one visit, 1.95 ± 1.67 (N = 91); drooling in two out of the three visits, 4.22 ± 2.95 (N = 92); persistent drooling, 10.36 ± 6.12 (N = 123). Drooling was more frequent in patients with dysphagia than in those without dysphagia: 60% (96/160) vs. 34.1% (181/531) (p < 0.0001) at V0; 57.9% (99/171) vs. 38.1% (165/433) (p < 0.0001) at V1; 55.9% (76/136) vs. 45.4% (60/166/366) (p = 0.023) at V2 (Figure 2(a)). Drooling burden (NMSS-item 19 total score) correlated with dysphagia burden (NMSS-item 20 total score) at V0 (N = 691; r = 0.322; p < 0.0001), at V1 (N = 604; r = 0.344; p < 0.0001), at V2 (N = 502; r = 0.198; p < 0.0001), and after considering all visits together (N = 481; r = 0.292; p < 0.0001). Drooling was also more frequent in patients with hypomimia than in those without hypomimia at V0 (43% vs. 31%; p = 0.011), at V1 (48.4% vs. 30.9%; p = 0.001), and at V2 (51.9% vs. 33.8%; p = 0.002) (Figure 2(a)). A significant correlation was observed between drooling burden and hypomimia burden at V0 (r = 0.197; p < 0.0001), at V1 (r = 0.149; p < 0.0001), at V2 (r = 0.189; p < 0.0001), and after considering all visits (r = 0.213; p < 0.0001). Similar results were observed in the PD ≤ 2 y group, with significant correlations between drooling burden and dysphagia burden (r = 565; p < 0.0001) and between drooling burden and hypomimia burden (r = 0.360; p < 0.00001) after considering the sum of the burden of all visits during the follow-up. Drooling was more frequent in patients with dysphagia at V0 and at V1 and with hypomimia at V2 than in those patients with these symptoms in the PD ≤ 2 y group (Figure 2(b)). Regarding the treatment, none of the patients were receiving botulinum toxin at any of the 3 visits (V0, V1, and V2).
Figure 2.
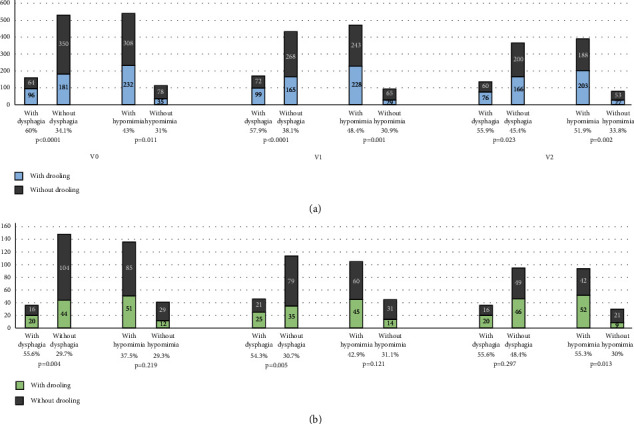
(a) Number of patients reporting drooling at V0, V1, and V2 when they were divided in patients with vs. without dysphagia and with vs. without hypomimia (the whole cohort). A comparison between the percentage is shown for each analysis. (b) Number of patients from the PD ≤ 2 y group reporting drooling at V0, V1, and V2 when they were divided in patients with vs. without dysphagia and with vs. without hypomimia. A comparison between the percentage is shown for each analysis. PD: Parkinson's disease. PD ≤ 2 y group: patients with ≤2 years since symptom onset.
At the baseline, drooling was associated with gender (males, 69% vs. 54.3%; p < 0.0001), older age (63.79 ± 8.21 vs. 61.8 ± 9.29; p = 0.008), and a higher LEDD (646.01 ± 410.21 vs. 512.73 ± 409.22; p < 0.0001) (Table 1). Patients with drooling were worse in terms of motor (UPDRS-III; UPDRS-IV; FOGQ) and nonmotor (PD-CRS; NMSS; BDI-II; NPI; PDSS; VAS-PAIN; VASF-physical; VASF-mental) status, QoL (PDQ-39SI; EUROHIS-QOL8; Figure 3), and autonomy for activities of daily living (ADLS) when compared to those without drooling (Table 1). In the PD ≤ 2 y group, drooling was associated with gait problems (FOGQ), a greater motor severity (UPDRS-III) and NMS burden (NMSS) including mood and other neuropsychiatric symptoms (BDI-II; NPI), pain (VAS-PAIN) and mental fatigue (VASF-mental), and a worse QoL (PDQ-39SI; EUROHIS-QOL8) (Table 1). Compared to patients without drooling, the frequency of major depression, freezing of gait, and falls in the subgroup of PD ≤ 2 y patients with drooling was roughly double (Table 1).
Table 1.
Disease-related characteristics, motor and nonmotor symptoms, and autonomy for activities of daily living and quality of life in patients with and without drooling at the baseline in the entire cohort (n = 691) and in PD ≤ 2 y (N = 184).
| Without drooling entire cohort (N = 414) |
With drooling entire cohort (N = 277) |
p | Without drooling PD ≤ 2 y (N = 120) |
With drooling PD ≤ 2 y (N = 64) |
p | |
|---|---|---|---|---|---|---|
| Age | 61.8 ± 9.29 | 63.79 ± 8.21 | 0.008 | 61.68 ± 8.54 | 63.39 ± 7.84 | 0.252 |
| Males (%) | 54.3 | 69 | <0.0001 | 55 | 60.9 | 0.269 |
| Weight (kgs) | 75.37 ± 13.83 | 76.56 ± 13.34 | 0.341 | 75.84 ± 14.75 | 75.75 ± 11 | 0.755 |
| Disease duration (years) | 5.31 ± 4.24 | 5.8 ± 4.55 | 0.136 | 1.33 ± 0.73 | 1.22 ± 0.75 | 0.332 |
| L-dopa eq. daily dose (mg) | 512.73 ± 409.22 | 646.01 ± 410.21 | <0.0001 | 303.51 ± 242.63 | 343.11 ± 256.34 | 0.296 |
| Number of non antip. drugs | 2.45 ± 2.43 | 2.79 ± 2.62 | 0.106 | 2.72 ± 2.44 | 2.94 ± 2.66 | 0.680 |
| Motor phenotype (%) | 0.899 | 0.995 | ||||
| Tremoric dominant | 45.6 | 44.9 | 58.8 | 57.8 | ||
| PIGD | 39.1 | 38.4 | 27.7 | 29.7 | ||
| Indeterminate | 15.3 | 16.7 | 13.4 | 12.5 | ||
| Hoehn and Yahr-OFF | 2 [1.5, 2] | 2 [2, 2] | 0.031 | 2 [1.5, 2] | 2 [1.5, 2] | 0.186 |
| Stage from 3 to 5 (%) | 8.6 | 10.5 | 0.257 | 2.9 | 1.7 | 0.526 |
| UPDRS-III-OFF | 20.97 ± 10.56 | 25.17 ± 11.59 | <0.0001 | 17.56 ± 8.46 | 21.69 ± 9.68 | 0.005 |
| Hypomimia (%) | 79.8 | 86.9 | 0.011 | 74.6 | 81 | 0.219 |
| UPDRS-IV | 1.79 ± 2.34 | 2.33 ± 2.48 | <0.0001 | 0.86 ± 1.38 | 1.16 ± 1.54 | 0.136 |
| Motor fluctuations (%) | 29.1 | 38.3 | 0.008 | 6.7 | 12.5 | 0.148 |
| Dyskinesia (%) | 17.5 | 21.2 | 0.137 | 2.6 | 6.6 | 0.190 |
| FOGQ | 3.3 ± 4.36 | 4.53 ± 4.78 | <0.0001 | 1.75 ± 2.81 | 3.05 ± 3.66 | 0.031 |
| Patients with FOG (%) | 30.1 | 42 | 0.001 | 16.7 | 31.2 | 0.019 |
| Patients with falls (%) | 10.8 | 17.2 | 0.011 | 6.6 | 15.6 | 0.034 |
| PD-CRS total score | 92.52 ± 15.97 | 89.36 ± 15.25 | 0.006 | 92.18 ± 15.44 | 88.09 ± 13.73 | 0.077 |
| NMSS | 37.69 ± 32.09 | 57.28 ± 42.55 | <0.0001 | 32.85 ± 28.08 | 56.4 ± 37.17 | <0.0001 |
| Dysphagia (%) | 15.5 | 34.7 | <0.0001 | 13.3 | 31.2 | 0.004 |
| BDI-II | 8.12 ± 7.18 | 9.64 ± 7.43 | 0.002 | 7.15 ± 6.98 | 10.81 ± 7.51 | <0.0001 |
| Major depression (%) | 13.3 | 20.2 | 0.010 | 11.7 | 25 | 0.018 |
| NPI | 5.12 ± 6.99 | 7.58 ± 9.36 | 0.001 | 4.2 ± 6.52 | 7.34 ± 6.95 | <0.0001 |
| QUIP-RS | 3.96 ± 7.63 | 4.97 ± 9.07 | 0.254 | 3.42 ± 7.66 | 2.93 ± 7.46 | 0.312 |
| PDSS | 116.83 ± 25.32 | 111.98 ± 28.8 | 0.027 | 119.45 ± 25.19 | 111.22 ± 32.04 | 0.110 |
| VAS-PAIN | 2.51 ± 2.94 | 2.9 ± 2.93 | 0.046 | 2.37 ± 2.9 | 3.18 ± 2.79 | 0.046 |
| VASF − physical | 2.83 ± 2.79 | 3.2 ± 2.68 | 0.038 | 2.55 ± 2.9 | 2.78 ± 2.43 | 0.211 |
| VASF – mental | 1.93 ± 2.5 | 2.47 ± 2.58 | 0.002 | 1.85 ± 2.51 | 2.56 ± 2.51 | 0.035 |
| ADLS | 89.49 ± 10.64 | 86.85 ± 10.15 | <0.0001 | 92.08 ± 8.39 | 89.22 ± 10.12 | 0.053 |
| Functional dependency (%) | 8.2 | 10.5 | 0.186 | 4.2 | 7.8 | 0.238 |
| PDQ-39SI | 15.15 ± 12.6 | 20.11 ± 14.33 | <0.0001 | 12.4 ± 11.33 | 19.01 ± 13.91 | <0.0001 |
| EUROHIS-QOL8 | 3.83 ± 0.54 | 2.71 ± 0.56 | 0.005 | 3.91 ± 0.56 | 3.64 ± 0.48 | 0.001 |
The results represent percentages, mean ± SD, or median (p25, p75). The chi-squared and Mann-Whitney-Wilcoxon tests were applied for comparisons between patients with and without drooling at the baseline. Data about H&Y and UPDRS-III are during the OFF state (first thing in the morning without taking medication in the previous 12 hours). ADLS: Schwab and England Activities of Daily Living Scale); antip.: antiparkinsonian; BDI: Beck Depression Inventory-II; NMSS: Nonmotor Symptoms Scale; NPI: Neuropsychiatric Inventory; PD: Parkinson's disease; PD ≤ 2 y: PD with ≤2 years from symptom onset; PD-CRS: Parkinson's Disease Cognitive Rating Scale; PDSS: Parkinson's Disease Sleep Scale; PIGD: Postural Instability Gait Difficulty; QUIP-RS: Questionnaire for Impulsive-Compulsive Disorders in Parkinson's Disease-Rating Scale; UPDRS: Unified Parkinson's Disease Rating Scale; VAFS: Visual Analog Fatigue Scale; VAS-Pain: Visual Analog Scale-Pain.
Figure 3.
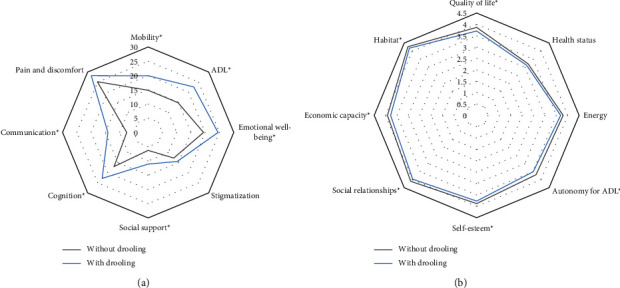
(a) Mean score on each domain of the PDQ-39 at the baseline in PD patients from the entire cohort with vs. without drooling; p < 0.0001 for all analysis except for “emotional well-being” (p = 0.001), “stigmatization” (p = 0.129), and “pain and discomfort” (p = 0.063). (b) Mean score on each domain of the EUROHIS-QOL8 at the baseline in PD patients from the entire cohort with vs. without drooling; “quality of life,” p = 0.005; “health status,” p = 0.178; “energy,” p = 0.183; “autonomy for ADL,” p = 0.011; “self-esteem,” p = 0.033; “social relationships,” p = 0.032; “economic capacity,” p = 0.020; “habitat,” p = 0.046. EUROHIS-QOL8, EUROHIS-QOL 8-item index; PD, Parkinson's disease; PDQ-39, 39-item Parkinson's disease quality of life questionnaire.
To be older (OR = 1.025; 95% CI, 1.004–1.046; p = 0.019), to be male (OR = 2.165; 95% CI, 1.486–3.153; p < 0.0001), to have a higher score on the UPDRS-III (OR = 1.018; 95% CI, 1.001–1.037; p = 0.047) and the NMSS (OR = 1.011; 95% CI, 1.005–1.016; p < 0.0001), and to have dysphagia (OR = 2.274; 95% CI, 1.476–3.505; p < 0.0001) were independent factors associated with drooling at the baseline (Table 2). In the PD ≤ 2 y group, a higher NMSS total score was the only independent factor associated with drooling at the baseline (OR = 1.017; 95% CI, 1.005–1.029; p = 0.001). Like as seen with baseline predictions, being older (OR = 1.032; 95% CI, 1.007–1.057; p = 0.012), being male (OR = 2.333; 95% CI, 1.540–3.536; p < 0.0001), having a greater NMS burden at the baseline (NMSS total score at V0; OR = 1.020; 95% CI, 1.011–1.030; p < 0.0001), and having a greater increase in the NMS burden from V0 to V2 (change in the NMSS total score from V0 to V2; OR = 1.012; 95% CI, 1.006–1.019; p < 0.0001) were identified as independent predictors of drooling after the 2-year follow-up (Table 3). When NMS burden at the baseline was considered as a categorical variable in the model, to have a very severe NMS burden at V0 (NMSS total score >70) increased the probability of drooling at V2 more than double (OR = 2.696; 95% CI, 4.248–10.729; p < 0.0001). Moreover, to have drooling at the baseline multiplied by 6 (OR = 6.751; 95% CI, 1.011–1.030; p < 0.0001), the probability of drooling at V2 after adjustment must be receiving anticholinergic drugs and the other covariates of the model. In the PD ≤ 2 y group, a higher UPDRS-III score at V0 was the only predictor of drooling at V2 identified (OR = 1.093; 95% CI, 1.025–1.166; p = 0.007) (Table 3). Specifically, to have at V0 a score on the UPDRS-III higher than 20 points increased the probability of drooling at V2 by 3-fold (OR = 3.671; 95% CI, 1.350–9.986; p = 0.011). Finally, to have a greater NMS burden at the baseline (β = 0.492; 95% CI, 0.052–0.089; p < 0.0001) and a greater increase in the NMS burden from V0 to V2 (β = 0.221; 95% CI, 0.020–0.048; p < 0.0001) were the most significant factors associated with drooling severely at V2 in the entire cohort, whereas to have at the baseline, a greater score on the UPDRS-III (β = 0.272; 95% CI, 0.038–0.204; p = 0.005) and the NMSS (β = 0.272; 95% CI, 0.009–0.049; p = 0.005) were in the PD ≤ 2 y group (Table 4). Similar results were observed when the item-19 score was excluded from the NMSS total score.
Table 2.
Factors associated with drooling at the baseline in the entire cohort (n = 691) and in the PD ≤ 2 y group (N = 184).
| ORa | ORb | 95% CIa | 95% CIb | p a | p b | |
|---|---|---|---|---|---|---|
| Entire cohort | ||||||
| Age | 1.026 | 1.025 | 1.008–1.044 | 1.004–1.046 | 0.004 | 0.019 |
| Male | 1.806 | 2.165 | 1.308–2.493 | 1.486–3.153 | <0.0001 | <0.0001 |
| LEDD | 1.001 | 1.000 | 1.001–1.002 | 1.000–1.001 | <0.0001 | 0.172 |
| UPDRS-III | 1.035 | 1.018 | 1.020–1.050 | 1.001–1.037 | <0.0001 | 0.047 |
| NMSS | 1.015 | 1.011 | 1.010–1.019 | 1.005–1.016 | <0.0001 | <0.0001 |
| Dysphagia | 2.901 | 2.274 | 2.016–4.173 | 1.476–3.505 | <0.0001 | <0.0001 |
| PD ≤ 2 y group | ||||||
| UPDRS-III | 1.052 | 1.034 | 1.014–1.090 | 0.994–1.076 | 0.006 | 0.096 |
| NMSS | 1.022 | 1.017 | 1.012–1.033 | 1.005–1.029 | <0.0001 | 0.004 |
| Dysphagia | 2.995 | 2.002 | 1.401–6.229 | 0.858–4.672 | 0.004 | 0.108 |
Dependent variable: drooling at V0 (NMSS-item 19 ≥ 1). OR (odds ratio) and 95% ICare shown. aunivariate analysis; bmultivariate analysis; entire cohort, R2 = 0.19; Hosmer and Lemeshow test, p = 0.226; PD ≤ 2 y, R2 = 0.19; Hosmer and Lemeshow test, p = 0.774. LEED: levodopa equivalent daily dose (mg/day); NMSS: Nonmotor Symptoms Scale; PD ≤ 2 y: PD with ≤2 years from symptom onset; UPDRS: Unified Parkinson's Disease Rating Scale.
Table 3.
Predictors of drooling after the 2-year follow-up in the entire cohort (N = 481) and in the PD ≤ 2 y group (N = 127).
| ORa | ORb | 95% CIa | 95% CIb | p a | p b | |
|---|---|---|---|---|---|---|
| Entire cohort | ||||||
| Age | 1.033 | 1.032 | 1.011–1.056 | 1.007–1.057 | 0.003 | 0.012 |
| Male | 2.023 | 2.333 | 1.396–2.932 | 1.540–3.536 | <0.0001 | <0.0001 |
| UPDRS-III at V0 | 1.028 | 1.016 | 1.010–1.047 | 0.995–1.038 | 0.002 | 0.097 |
| NMSS at V0 | 1.010 | 1.020 | 1.005–1.016 | 1.011–1.030 | <0.0001 | <0.0001 |
| PDQ-39SI at V0 | 1.016 | 0.978 | 1.002–1.031 | 0.955–1.002 | 0.024 | 0.069 |
| Change from V0 to V2 in NMSS | 1.006 | 1.012 | 1.001–1.011 | 1.006–1.019 | 0.042 | <0.0001 |
| PD ≤ 2 y group | ||||||
| Age | 1.037 | 1.037 | 0.994–1.082 | 0.984–1.092 | 0.096 | 0.098 |
| Male | 1.707 | 2.064 | 0.845–3.450 | 0.886–4.810 | 0.136 | 0.093 |
| UPDRS-III at V0 | 1.121 | 1.093 | 1.056–1.191 | 1.025–1.166 | <0.0001 | 0.007 |
| NMSS at V0 | 1.019 | 1.013 | 1.007–1.032 | 0.998–1.032 | 0.128 | 0.082 |
Dependent variable: drooling at V2 (NMSS-item 19 ≥ 1). OR (odds ratio) and 95% IC are shown. aunivariate analysis; bmultivariate analysis; entire cohort, R2 = 0.33; Hosmer and Lemeshow test, p = 0.163; PD ≤ 2 y, R2 = 26; Hosmer and Lemeshow test, p = 0.788. LEED: levodopa equivalent daily dose (mg/day); NMSS: Nonmotor Symptoms Scale; PD ≤ 2 y: PD with ≤2 years from symptom onset; PDQ-39SI: 39-item Parkinson's disease Questionnaire Summary Index; UPDRS: Unified Parkinson's Disease Rating Scale.
Table 4.
Factors associated with drooling severity after the 2-year follow-up in the entire cohort (N = 481) and in the PD ≤ 2 y group (N = 127).
| β a | β b | 95% CIa | 95% CIb | p a | p b | |
|---|---|---|---|---|---|---|
| Entire cohort | ||||||
| Age | 0.114 | 0.083 | 0.015–0.127 | −0.001–0.109 | 0.013 | 0.052 |
| Male | 0.112 | 0.136 | 0.252–2.199 | 0.568–2.445 | 0.014 | 0.002 |
| UPDRS-III at V0 | 0.207 | 0.087 | 0.060–1.054 | −0.003–0.093 | <0.0001 | 0.068 |
| NMSS at V0 | 0.359 | 0.492 | 0.039–0.063 | 0.052–0.089 | <0.0001 | <0.0001 |
| PDQ-39SI at V0 | 0.240 | −0.110 | 0.063–1.135 | −0.098–0.007 | <0.0001 | 0.087 |
| Change from V0 to V2 in NMSS | 0.073 | 0.221 | −0.003–0.125 | 0.020–0.048 | 0.110 | <0.0001 |
| PD ≤ 2 y group | ||||||
| UPDRS-III at V0 | 1.121 | 0.272 | 1.056–1.191 | 0.038–0.204 | <0.0001 | 0.005 |
| NMSS at V0 | 1.019 | 0.272 | 1.007–1.032 | 0.009–0.049 | <0.0001 | 0.005 |
Dependent variable: droolingV0+V1+V2 score. β standardized coefficient and 95% IC are shown. aunivariate analysis; bmultivariate analysis; entire cohort, R2 = 0.21; Durbin–Watson test = 1.92; PD ≤ 2 y, R2 = 22; Durbin–Watson test = 1.94. NMSS: Nonmotor Symptoms Scale; PD ≤ 2 y: PD with ≤2 years from symptom onset; PDQ-39SI: 39-item Parkinson's disease Questionnaire Summary Index; UPDRS: Unified Parkinson's Disease Rating Scale.
With regard to QoL, drooling was associated with a worse health-related QoL (PDQ-39SI as the dependent variable) at V0 (β = 0.180; 95% CI, 2.928–6.992; p < 0.0001) and at V2 (β = 0.131; 95% CI, 1.409–7.115; p = 0.003) and also with a worse global QoL (EUROHIS-QOL8 as dependent variable) at V0 (β = −0.118; 95% CI, −0.218 to −0.050; p = 0.002) and at V2 (β = −0.128; 95% CI, −0.251 to −0.047; p = 0.004). In the PD ≤ 2 y group, drooling was associated with a worse health-related QoL at V0 (β = 0.249; 95% CI, 2.855–10.362; p = 0.001) and at V2 (β = 0.306; 95% CI, 4.193–14.327; p < 0.0001) and with a worse global QoL at V0 (β = −0.238; 95% CI, −0.438 to −0.110; p = 0.001) as well. However, after adjustment to covariates defined in the methods, the association between drooling and both health-related and global QoL at V0 and at V2 was not significant, not even when persisting drooling or the NMSS-DroolingV0+V1+V2 score was considered in the model. A correlation was observed between the NMSS-DroolingV0+V1+V2 score and the score on both PDQ-39SI and EUROHIS-QOL8 at V2 in the entire cohort (PDQ-39SI, r = 0.234 (p < 0.0001); EUROHIS-QOL8, r = −0.222 (p < 0.0001)) and in the PD ≤ 2 y group (PDQ-39SI, r = 0.483 (p < 0.0001); EUROHIS-QOL8, r = −0.304 (p = 0.001)). QoL at V2 was worse in patients with persistent drooling in both the entire cohort (PDQ-39SI, 25.18 ± 19.14 vs. 18.4 ± 14.81 (p < 0.0001); EUROHIS-QOL8, 3.64 ± 0.51 vs. 3.8 ± 0.59 (p < 0.005)) and in the PD ≤ 2 y group (PDQ-39SI, 28.58 ± 22.71 vs. 14.03 ± 11.35 (p = 0.001); EUROHIS-QOL8, 3.54 ± 0.53 vs. 3.88 ± 0.57 (p = 0.006)). Finally, by domains, drooling was an independent factor associated with a worse “Activities of daily living” (β = 0.086; 95% CI, 0.654–5.925; p = 0.015; R2 = 0.43) and “Communication” (β = 0.088; 95% CI, 0.297–5.075; p = 0.028; R2 = 0.28) at V0 in the entire cohort.
4. Discussion
The present study represents one of the largest cohorts of PD patients in whom the prevalence of drooling was reported using a validated global NMS scale. We observed that drooling was common in PD patients, clearly much more frequent than in the control group, and was associated with the male gender, older age, and a greater motor and nonmotor severity. In addition, patients with drooling had a worse global and health-related QoL, although the effect of drooling on QoL was not significant after adjusting to other covariates. Importantly, we observed that drooling was also a very frequent symptom at the beginning of the disease, as seen in the very early PD patients, suggesting the clinical importance of asking for the presence of drooling at the beginning of the patient's follow-up.
About 2 out of every 3 patients from the Spanish cohort COPPADIS reported drooling over a 2-year follow-up. This cumulative prevalence is in line with the previously published data [11]. However, due to the lack of a standard definition and criteria for diagnosing drooling in PD patients, estimates of its prevalence vary considerably with a wide range from 10% to 84% [2–15]. This is partly due to different tools such as the UPDRS-II, SCOPA-AUT (Scale for Outcomes in Parkinson's disease for Autonomic Symptoms), PD-NMSQuest (Parkinson's Disease Nonmotor Symptoms Questionnaire), NMSS, or different types of screening questionnaires have been used to screen drooling in PD cohorts with different characteristics also [1, 3, 11]. Some specific scales to assess drooling have been designed, but they have been poorly used in studies with PD patients [37]. Using the NMSS-item 19 for detecting drooling like us, van Wamelen et al. [23] detected in a cohort of 728 PD patients with a mean disease duration of 5.6 years a prevalence of 37.2% at the baseline and 40.1% after a mean follow-up of 3.3 years (range 0.5–7.2 years). In many cross-sectional studies, the prevalence of drooling in PD is between 40% and 50% [2, 6–8, 11, 23, 24, 38, 39], which is in agreement with our findings. An interesting finding is that like in other studies [5, 13], drooling was not related to disease duration and in fact, the prevalence at each year (from 35% to 50%) and the cumulative prevalence after the 2-year follow-up (65%) was similar in those patients with no more than 2 years since symptom onset compared to the whole cohort. Drooling is frequent even in de novo patients. Erro et al. [27] reported in 61 de novo PD patients a frequency of drooling of 19.4% at the baseline and 15.3% after a 2-year follow-up, whereas Picillo et al. [28] found in 86 men and 48 women de novo PD patients a frequency of drooling at the baseline and after a 2-year follow-up of 23.3% and 25% and 10.4% and 4.1%, respectively. The Picillo study, in addition to ours and other studies, suggests that drooling could be more frequent in males [3, 11, 28, 40]. Although specifically well-designed studies to analyze the prevalence of drooling using specific validated scales [37, 41] in large cohorts are required, all these data suggest a recommendation to rule out drooling in PD patients at the beginning and throughout follow-up since its presence is associated with a worse QoL and it is potentially treatable. Consideration is especially valid in elderly men for which the prevalence of drooling is more frequent. Despite this, drooling is an underrecognized and undertreated symptom in PD [1]. Of note, no patient from our cohort was receiving botulinum toxin injections.
In addition to male gender, many other variables have been associated with drooling in PD patients such as dysphagia [1, 42], dysarthria [1, 43], hypomimia [14, 17], lingual bradykinesia [14, 17], cognitive status [15, 24], hallucinations [5], aging [3, 23], more advanced disease stage [16, 24], orthostatic hypotension [1], camptocormia [44], and a history of using antidepressants [6]. Drooling in PD patients can be in part due to the inability to maintain saliva in the mouth (i.e., hypomimia, abnormal flexed posture, etc.) and impairment of salivary clearance (i.e., lingual bradykinesia, oropharyngeal dysphagia, and upper esophageal dysmotility), as dysphagia is the strongest factor associated with drooling [7, 12, 23]. We identified dysphagia as a factor that doubles the probability of drooling independently of other variables, even though it was measured through patient-reported outcomes. Moreover, not only dysphagia burden but also hypomimia burden correlated with drooling burden in the entire cohort and the very early PD group as well. On the other hand, some recent studies comprehensively evaluating many features of the disease found an association between drooling and late onset of the disease, a higher LEDD, fluctuations, depression, higher motor scores, and a greater NMS burden [13–15, 23, 45]. In this Spanish cohort, we identified a greater motor severity (UPDRS-III) and a greater NMS burden (NMSS) as independent factors associated with drooling and/or also predictors of drooling after a 2-year follow-up. Specifically, a worse status in terms of motor and NMS predicted a greater drooling severity as well. This could explain why drooling was associated with a worse QoL but was not an independent predictor of it. Karakoc et al. [46] reported drooling in 65% of 63 people with PD but no independent significant correlation of drooling severity with QoL. However, as in our case, they measured the latter from the total PDQ-39 score, rather than with a tool that measures drooling impact. In contrast, when we used the PDQ-39 domains, we identified drooling as an independent factor associated with a worse autonomy for ADL (PDQ-39 domain 2) and communication (PDQ-39 domain 7). Psychosocially, PD droolers had worse QoL and had more difficulty speaking, eating, and socially interacting compared to PD nondroolers [3, 5, 11]. In addition, drooling patients affect their caregivers by increasing their burden, depression, and anxiety and reducing their QoL [47]. For all these reasons, therapeutic options should be evaluated more intensively in patients with PD and drooling [1, 11].
The present study has some important limitations. Drooling was considered based on an answer to a simple clinical question from the NMSS and not after using a specific scale [37, 41]. However, this methodology is the most frequent in most studies [2, 3, 6, 7, 11, 24, 40, 47, 48]. The sample size in the group of PD patients with no more than 2 years since the onset of the symptoms was small and clearly smaller than that of the entire cohort. In the 2-year follow-up group, there was a 30% loss in participants, although this has been observed in other cohorts, with retention rates of 71% [23], 67% [27], or 67% [28]. The logistic regression models used to identify the independent factors associated with drooling and predictors of drooling only explain 20–30% of the variance in our analysis, but it was either also low or not provided in other studies [6, 7, 13, 23]. For some variables, the information was not collected in all cases. Instead of a specific tool for assessing comorbidity, like the Charlson index or others, the total number of non-anti-Parkinsonian medications was used as a surrogate marker of comorbidity [36], and the role of possible comorbidities inducing drooling was not considered. Finally, our sample was not fully representative of the PD population due to inclusion and exclusion criteria (i.e., age limit, no dementia, no severe comorbidities, no second-line therapies, etc.) [49]. Nonetheless, the strengths of our study include a very thorough assessment, a prospective longitudinal follow-up design, and the extensive clinical and demographic information recorded. Data about drooling severity and PDQ-39 domains are novel.
In conclusion, this study observes a high prevalence of drooling in PD patients, clearly much more so than in control subjects, and that this feature is frequent even at the first stages of the disease as well. Dysphagia is associated with drooling, and a higher motor score and a greater NMS burden are predictors of drooling. PD patients with drooling have a worse QoL, and drooling is also an independent factor associated with communication problems. Thus, drooling screening and therapeutic options should be considered in clinical practice.
Acknowledgments
COPPADIS and the present study were developed with the help of Fundación Española de Ayuda a la Investigación en Enfermedades Neurodegenerativas y/o de Origen Genético (https://fundaciondegen.org/) and Alpha Bioresearch (https://www.alphabioresearch.com). Also, The authors received grants from the Spanish Ministry of Economy and Competitiveness [PI16/01575] co-founded by ISCIII (Concesión de subvenciones de Proyectos de Investigación en Salud de la convocatoria 2020 de la Acción Estratégica en Salud 2017–2020 por el proyecto “PROGRESIÓN NO MOTORA E IMPACTO EN LA CALIDAD DE VIDA EN LA ENFERMEDAD DE PARKINSON”) to develop a part of the COPPADIS project. The authors would like to thank all patients and their caregivers who collaborated in this study. They would also like to thank Fundación Española de Ayuda a la Investigación en Enfermedades Neurodegenerativas y/o de Origen Genético (https://fundaciondegen.org/) and Alpha Bioresearch (https://www.alphabioresearch.com) and other institutions for helping them.
Abbreviations
- ADLS:
Schwab & England activities of daily living scale
- BDI-II:
Beck depression inventory-II
- EUROHIS-QOL8:
EUROHIS-QOL 8-item index
- FOG-Q:
Freezing of gait questionnaire
- LEDD:
Levodopa equivalent daily dose
- NMS:
Non-motor symptoms
- NMSS:
Non-motor symptoms scale
- NPI:
Neuropsychiatric inventory
- PD:
Parkinson's disease
- PD-CRS:
Parkinson's disease cognitive rating scale
- PDQ-39SI:
39-item Parkinson's disease quality of life questionnaire summary index
- PDSS:
Parkinson's disease sleep scale
- QoL:
Quality of life
- QUIP-RS:
Questionnaire for impulsive-compulsive disorders in Parkinson's disease-rating scale
- UPDRS:
Unified Parkinson's disease rating scale
- VAFS:
Visual analog fatigue scale
- VAS-Pain:
Visual analog scale-pain.
Appendix
A. Coppadis Study Group
Adarmes AD, Almeria M, Alonso Losada MG, Alonso Cánovas A, Alonso Frech F, Alonso Redondo R, Álvarez The authors, Álvarez Sauco M, Aneiros Díaz A, Arnáiz S, Arribas S, Ascunce Vidondo A, Aguilar M, Ávila MA, Bernardo Lambrich N, Bejr-Kasem H, Blázquez Estrada M, Botí M, Borrue C, Buongiorno MT, Cabello González C, Cabo López The authors, Caballol N, Cámara Lorenzo A, Canfield Medina H, Carrillo F, Carrillo Padilla FJ, Casas E, Catalán MJ, Clavero P, Cortina Fernández A, Cosgaya M, Cots Foraster A, Crespo Cuevas A, Cubo E, de Deus Fonticoba T, de Fábregues-Boixar O, Díez-Fairen M, Dotor García-Soto J, Erro E, Escalante S, Estelrich Peyret E, Fernández Guillán N, Gámez P, Gallego M, García Caldentey J, García Campos C, García Díez C, García Moreno JM, Gastón The authors, Gómez Garre MP, Gómez Mayordomo V, González Aloy J, González-Aramburu The authors, González Ardura J, González García B, González Palmás MJ, González Toledo GR, Golpe Díaz A, Grau Solá M, Guardia G, Hernández Vara J, Horta-Barba A, Idoate Calderón D, Infante J, Jesús S, Kulisevsky J, Kurtis M, Labandeira C, Labrador MA, Lacruz F, Lage Castro M, Lastres Gómez S, Legarda The authors, López Ariztegui N, López Díaz LM, López Domínguez D, López Manzanares L, López Seoane B, Lucas del Pozo S, Macías Y, Mata M, Martí Andres G, Martí MJ, Martínez Castrillo JC, Martinez-Martin P, McAfee D, Meitín MT, Mendoza Plasencia Z, Menéndez González M, Méndez del Barrio C, Mir P, Miranda Santiago J, Morales Casado MI, Moreno Diéguez A, Nogueira V, Novo Amado A, Novo Ponte S, Ordás C, Pagonabarraga J, Pareés The authors, Pascual-Sedano B, Pastor P, Pérez Fuertes A, Pérez Noguera R, Planas-Ballvé A, Planellas L, Prats MA, Prieto Jurczynska C, Puente V, Pueyo Morlans M, Puig Daví A, Redondo Rafales N, Rodríguez Méndez L, Rodríguez Pérez AB, Roldán F, Ruíz De Arcos M, Ruíz Martínez J, Sánchez Alonso P, Sánchez-Carpintero M, Sánchez Díez G, Sánchez Rodríguez A, Santacruz P, Santos García D, Segundo Rodríguez JC, Seijo M, Sierra Peña M, Solano Vila B, Suárez Castro E, Tartari JP, Valero C, Vargas L, Vela L, Villanueva C, Vives B (Table 5).
Table 5.
COPPADIS study group.
| Name (last name, first name) | Location | Role | Contribution |
|---|---|---|---|
| Astrid Adarmes, Daniela | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator | Evaluation of participants and/or data management |
| Almeria, Marta | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Neuropsychologist; evaluation of participants |
| Alonso Losada, Maria Gema | Hospital Álvaro Cunqueiro, Complejo Hospitalario Universitario de Vigo (CHUVI), Vigo, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Alonso Cánovas, Araceli | Hospital Universitario Ramón y Cajal, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Alonso Frech, Fernando | Hospital Universitario Clínico San Carlos, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Alonso Redondo, Ruben | Hospital Universitario Lucus Augusti (HULA), Lugo, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Aneiros Díaz, Ángel | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Álvarez, Ignacio | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Álvarez Sauco, María | Hospital General Universitario de Elche, Elche, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Arnáiz, Sandra | Complejo Asistencial Universitario de Burgos, Burgos, Spain | Site investigator | Evaluation of participants and/or data management |
| Arribas, Sonia | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Neuropsychologist; evaluation of participants |
| Ascunce Vidondo, Arancha | Complejo Hospitalario de Navarra, Pamplona, Spain | Site investigator | Evaluation of participants and/or data management |
| Aguilar, Miquel | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Ávila Rivera, Maria Asunción | Consorci Sanitari Integral, Hospital General de L´Hospitalet, L´Hospitalet de Llobregat, Barcelona, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Bernardo Lambrich, Noemí | Hospital de Tortosa Verge de la Cinta (HTVC), Tortosa, Tarragona, Spain | Site investigator | Evaluation of participants and/or data management |
| Bejr-Kasem, Helena | Hospital de Sant Pau, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Blázquez Estrada, Marta | Hospital Universitario Central de Asturias, Oviedo, Spain | Site investigator | Evaluation of participants and/or data management |
| Botí González, Maria Ángeles | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Neuropsychologist; evaluation of participants |
| Borrué, Carmen | Hospital Infanta Sofía, Madrid, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Buongiorno, Maria Teresa | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Nurse study coordinator |
| Cabello González, Carolina | Complejo Hospitalario de Navarra, Pamplona, Spain | Site investigator | Scheduling of evaluations |
| Cabo López, Iria | Complejo Hospitalario Universitario de Pontevedra (CHOP), Pontevedra, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Caballol, Nuria | Consorci Sanitari Integral, Hospital Moisés Broggi, Sant Joan Despí, Barcelona, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Cámara Lorenzo, Ana | Hospital Clínic de Barcelona, Barcelona, Spain | Site investigator | Nurse study coordinator |
| Canfield Medina, Héctor | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Evaluation of participants and/or data management |
| Carrillo, Fátima | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator | Evaluation of participants and/or data management |
| Carrillo Padilla, Francisco José | Hospital Universitario de Canarias, San Cristóbal de la Laguna, Santa Cruz de Tenerife, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Casas, Elena | Complejo Asistencial Universitario de Burgos, Burgos, Spain | Site investigator | Evaluation of participants and/or data management |
| Catalán, Maria José | Hospital Universitario Clínico San Carlos, Madrid, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Clavero, Pedro | Complejo Hospitalario de Navarra, Pamplona, Spain | Site investigator | Evaluation of participants and/or data management |
| Cortina Fernández, A | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Coordination of blood extractions |
| Cosgaya, Marina | Hospital Clínic de Barcelona, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Cots Foraster, Ana | Institut d' Assistència Sanitària (IAS) - Instituí Cátala de la Salud. Girona, Spain | Site investigator | Evaluation of participants and/or data management |
| Crespo Cuevas, Ane | Hospital del Mar, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Cubo, Esther | Complejo Asistencial Universitario de Burgos, Burgos, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| De Deus Fonticoba, Teresa | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Nurse study coordinator evaluation of participants and/or data management |
| De Fábregues-Boixar, Oriol | Hospital Universitario Vall d´Hebron, Barcelona, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Díez Fairen, M | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Dotor García-Soto, Julio | Hospital Universitario Virgen Macarena, Sevilla, Spain | Site investigator/PI | Evaluation of participants and/or data management |
| Erro, Elena | Complejo Hospitalario de Navarra, Pamplona, Spain | Site investigator | Evaluation of participants and/or data management |
| Escalante, Sonia | Hospital de Tortosa Verge de la Cinta (HTVC), Tortosa, Tarragona, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Estelrich Peyret, Elena | Institut d' Assistència Sanitària (IAS) - Instituí Cátala de la Salud. Girona, Spain | Site investigator | Evaluation of participants and/or data management |
| Fernández Guillán, Noelia | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Neuroimaging studies |
| Gámez, Pedro | Complejo Asistencial Universitario de Burgos, Burgos, Spain | Site investigator | Evaluation of participants and/or data management |
| Gallego, Mercedes | Hospital La Princesa, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| García Caldentey, Juan | Centro Neurológico Oms 42, Palma de Mallorca, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| García Campos, Cristina | Hospital Universitario Virgen Macarena, Sevilla, Spain | Site investigator | Evaluation of participants and/or data management |
| García Díez, Cristina | Complejo Hospitalario Universitario de Pontevedra (CHOP), Pontevedra, Spain | Site investigator (from MAY/22) | Neuropsychologist; evaluation of participants |
| García Moreno, José Manuel | Hospital Universitario Virgen Macarena, Sevilla, Spain | Site investigator/PI (until MAR/21) | Coordination at the center evaluation of participants and/or data management |
| Gastón, Itziar | Complejo Hospitalario de Navarra, Pamplona, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Gómez Garre, María del Pilar | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator | Genetic studies coordination |
| Gómez Mayordomo, Víctor | Hospital Clínico San Carlos, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| González Aloy, Javier | Institut d' Assistència Sanitària (IAS) - Instituí Cátala de la Salud. Girona, Spain | Site investigator | Evaluation of participants and/or data management |
| González Aramburu, Isabel | Hospital Universitario Marqués de Valdecilla, Santander, Spain | Site investigator | Evaluation of participants and/or data management |
| González Ardura, Jessica | Hospital Universitario Lucus Augusti (HULA), Lugo, Spain | Site investigator/PI (until FEB/21) | Evaluation of participants and/or data management |
| González García, Beatriz | Hospital La Princesa, Madrid, Spain | Site investigator | Nurse study coordinator |
| González Palmás, Maria Josefa | Complejo Hospitalario Universitario de Pontevedra (CHOP), Pontevedra, Spain | Site investigator | Evaluation of participants and/or data management |
| González Toledo, Gabriel Ricardo | Hospital Universitario de Canarias, San Cristóbal de la Laguna, Santa Cruz de Tenerife, Spain | Site investigator | Evaluation of participants and/or data management |
| Golpe Díaz, Ana | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Laboratory analysis coordination |
| Grau Solá, Mireia | Consorci Sanitari Integral, Hospital Moisés Broggi, Sant Joan Despí, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Guardia, Gema | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Hernández Vara, Jorge | Hospital Universitario Vall d´Hebron, Barcelona, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Horta Barba, Andrea | Hospital de Sant Pau, Barcelona, Spain | Site investigator | Neuropsychologist; evaluation of participants |
| Idoate Calderón, Daniel | Complejo Hospitalario Universitario de Pontevedra (CHOP), Pontevedra, Spain | Site investigator (until MAY/22) | Neuropsychologist; evaluation of participants |
| Infante, Jon | Hospital Universitario Marqués de Valdecilla, Santander, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Jesús, Silvia | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator | Evaluation of participants and/or data management |
| Kulisevsky, Jaime | Hospital de Sant Pau, Barcelona, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Kurtis, Mónica | Hospital Ruber Internacional, Madrid, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Labandeira, Carmen | Hospital Álvaro Cunqueiro, Complejo Hospitalario Universitario de Vigo (CHUVI), Vigo, Spain | Site investigator | Evaluation of participants and/or data management |
| Labrador Espinosa, Miguel Ángel | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator | Neuroimaging data analysis |
| Lacruz, Francisco | Complejo Hospitalario de Navarra, Pamplona, Spain | Site investigator | Evaluation of participants and/or data management |
| Lage Castro, Melva | Complejo Hospitalario Universitario de Pontevedra (CHOP), Pontevedra, Spain | Site investigator | Evaluation of participants and/or data management |
| Lastres Gómez, Sonia | Complejo Hospitalario Universitario de Pontevedra (CHOP), Pontevedra, Spain | Site investigator | Neuropsychologist; evaluation of participants |
| Legarda, Inés | Hospital Universitario Son Espases, Palma de Mallorca, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| López Ariztegui, Nuria | Complejo Hospitalario de Toledo, Toledo, Spain | Site investigator/PI | Evaluation of participants and/or data management |
| López Díaz, Luis Manuel | Hospital Da Costa de Burela, Lugo, Spain | Site investigator | Evaluation of participants and/or data management |
| López Domínguez, Daniel | Institut d' Assistència Sanitària (IAS) - Instituí Cátala de la Salud. Girona, Spain | Site investigator | Evaluation of participants and/or data management |
| López Manzanares, Lydia | Hospital La Princesa, Madrid, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| López Seoane, Balbino | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Neuroimaging studies |
| Lucas del Pozo, Sara | Hospital Universitario Vall d´Hebron, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Macías, Yolanda | Fundación Hospital de Alcorcón, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Mata, Marina | Hospital Infanta Sofía, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Martí Andres, Gloria | Hospital Universitario Vall d´Hebron, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Martí, Maria José | Hospital Clínic de Barcelona, Barcelona, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Martínez Castrillo, Juan Carlos | Hospital Universitario Ramón y Cajal, Madrid, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Martinez-Martin, Pablo | Centro Nacional de Epidemiología y CIBERNED, Instituto de Salud Carlos III. Madrid | Collaborator in statistical and methods analysis | Methods and statistical reviewer |
| McAfee, Darrian | University of Pennsylvania, Philadelphia | Collaborator in English style | English style reviewer |
| Meitín, Maria Teresa | Hospital Da Costa de Burela, Lugo, Spain | Site investigator | Evaluation of participants and/or data management |
| Menéndez González, Manuel | Hospital Universitario Central de Asturias, Oviedo, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Méndez del Barrio, Carlota | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator | Evaluation of participants and/or data management |
| Mendoza Plasencia, Zebenzui | Hospital Universitario de Canarias, San Cristóbal de la Laguna, Santa Cruz de Tenerife, Spain | Site investigator | Evaluation of participants and/or data management |
| Mir, Pablo | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Miranda Santiago, Javier | Complejo Asistencial Universitario de Burgos, Burgos, Spain | Site investigator | Evaluation of participants and/or data management |
| Morales Casado, Maria Isabel | Complejo Hospitalario de Toledo, Toledo, Spain | Site investigator | Evaluation of participants and/or data management |
| Moreno Diéguez, Antonio | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Neuroimaging studies |
| Nogueira, Víctor | Hospital Da Costa de Burela, Lugo, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Novo Amado, Alba | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Neuroimaging studies |
| Novo Ponte, Sabela | Hospital Universitario Puerta de Hierro, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Ordás, Carlos | Hospital Rey Juan Carlos, Madrid, Spain, Madrid, Spain | Site Investigator | Evaluation of participants and/or data management |
| Pagonabarraga, Javier | Hospital de Sant Pau, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Pareés, Isabel | Hospital Ruber Internacional, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Pascual-Sedano, Berta | Hospital de Sant Pau, Barcelona, Spain | Site Investigator | Evaluation of participants and/or data management |
| Pastor, Pau | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Pérez Fuertes, Aída | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Blood analysis |
| Pérez Noguera, Rafael | Hospital Universitario Virgen Macarena, Sevilla, Spain | Site investigator | Evaluation of participants and/or data management |
| Planas-Ballvé, Ana | Consorci Sanitari Integral, Hospital Moisés Broggi, Sant Joan Despí, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Planellas, Lluís | Hospital Clínic de Barcelona, Barcelona, Spain | Site investigator (until DEC/19) | Evaluation of participants and/or data management |
| Prats, Marian Ángeles | Institut d' Assistència Sanitària (IAS) - Instituí Cátala de la Salud. Girona, Spain | Site investigator | Evaluation of participants and/or data management |
| Prieto Jurczynska, Cristina | Hospital Rey Juan Carlos, Madrid, Spain, Madrid, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Puente, Víctor | Hospital del Mar, Barcelona, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Pueyo Morlans, Mercedes | Hospital Universitario de Canarias, San Cristóbal de la Laguna, Santa Cruz de Tenerife, Spain | Site investigator | Evaluation of participants and/or data management |
| Puig Daví, Arnau | Hospital de Sant Pau, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Redondo, Nuria | Hospital La Princesa, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Rodríguez Méndez, Luisa | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Blood analysis |
| Rodríguez Pérez, Amparo Belén | Hospital General Universitario de Elche, Elche, Spain | Site investigator | Evaluation of participants and/or data management |
| Roldán, Florinda | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator | Neuroimaging studies |
| Ruíz de Arcos, María | Hospital Universitario Virgen Macarena, Sevilla, Spain | Site investigator | Evaluation of participants and/or data management |
| Ruíz Martínez, Javier | Hospital Universitario Donostia, San Sebastián, Spain | Site investigator | Evaluation of participants and/or data management |
| Sánchez Alonso, Pilar | Hospital Universitario Puerta de Hierro, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Sánchez-Carpintero, Macarena | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Neuroimaging studies |
| Sánchez Díez, Gema | Hospital Universitario Ramón y Cajal, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Sánchez Rodríguez, Antonio | Hospital Universitario Marqués de Valdecilla, Santander, Spain | Site investigator | Evaluation of participants and/or data management |
| Santacruz, Pilar | Hospital Clínic de Barcelona, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Santos García, Diego | CHUAC, Complejo Hospitalario Universitario de A Coruña | Coordinator of the project | Coordination of the COPPADIS-2015 |
| Segundo Rodríguez, José Clemente | Complejo Hospitalario de Toledo, Toledo, Spain | Site investigator | Evaluation of participants and/or data management |
| Seijo, Manuel | Complejo Hospitalario Universitario de Pontevedra (CHOP), Pontevedra, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Sierra, María | Hospital Universitario Marqués de Valdecilla, Santander, Spain | Site investigator | Evaluation of participants and/or data management |
| Solano, Berta | Institut d' Assistència Sanitària (IAS) - Instituí Cátala de la Salud. Girona, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Suárez Castro, Ester | Complejo Hospitalario Universitario de Ferrol (CHUF), Ferrol, A Coruña, Spain | Site investigator | Evaluation of participants and/or data management |
| Tartari, Juan Pablo | Hospital Universitari Mutua de Terrassa, Terrassa, Barcelona, Spain | Site investigator | Evaluation of participants and/or data management |
| Valero, Caridad | Hospital Arnau de Vilanova, Valencia, Spain | Site investigator | Evaluation of participants and/or data management |
| Vargas, Laura | Hospital Universitario Virgen del Rocío, Sevilla, Spain | Site investigator | Evaluation of participants and/or data management |
| Vela, Lydia | Fundación Hospital de Alcorcón, Madrid, Spain | Site investigator/PI | Coordination at the center evaluation of participants and/or data management |
| Villanueva, Clara | Hospital Universitario Clínico San Carlos, Madrid, Spain | Site investigator | Evaluation of participants and/or data management |
| Vives, Bárbara | Hospital Universitario Son Espases, Palma de Mallorca, Spain | Site investigator | Evaluation of participants and/or data management |
Data Availability
The protocol and the statistical analysis plan are available on request. Deidentified participants data are not available for legal and ethical reasons.
Disclosure
This manuscript is a preprint already in https://www.mdpi.com/2075-4418/12/5/1147/htm.
Conflicts of Interest
Santos García D. has received honoraria for educational presentations and advice service by Abbvie, UCB Pharma, Lundbeck, KRKA, Zambon, Bial, Italfarmaco, Teva, Archímedes, Esteve, Stada, and grants from the Spanish Ministry of Economy and Competitiveness [PI16/01575] co-founded by ISCIII (Concesión de subvenciones de Proyectos de Investigación en Salud de la convocatoria 2020 de la Acción Estratégica en Salud 2017–2020 por el proyecto “PROGRESIÓN NO MOTORA E IMPACTO EN LA CALIDAD DE VIDA EN LA ENFERMEDAD DE PARKINSON”). De Deus Fonticoba T.: None. Cores Bartolomé C. has received honoraria for educational presentations and advice service by Lundbeck and UCB Pharma. Feal Painceiras M. J.: None. Íñiguez Alvarado MC: None. Jesús S. has received honoraria from AbbVie, Bial, Merz, UCB, and Zambon and holds the competitive contract “Juan Rodés” supported by the Instituto de Salud Carlos III. She has received grants from the Spanish Ministry of Economy and Competitiveness (PI18/01898) and the Consejería de Salud de la Junta de Andalucía (PI-0459-2018). Buongiorno M. T.: Planellas LL.: None. Cosgaya M.: None. García Caldentey J. has received honoraria for educational presentations and advice service by Qualigen, Nutricia, Abbvie, Italfarmaco, UCB Pharma, Lundbeck, Zambon, Bial, and Teva. Caballol N. has received honoraria from Bial, Italfarmaco, Qualigen, Zambon, UCB, Teva, and KRKA and sponsorship from Zambon, TEVA, and Abbvie for attending medical conferences. Legarda I. has received honoraria for educational presentations and advice service by Abbvie, UCB Pharma, Zambon, Bial, and Teva. Hernández Vara J. has received travel bursaries and educational grants from Abbvie and has received honoraria for educational presentations from Abbvie, Teva, Bial, Zambon, Italfarmaco, and Sanofi-Genzyme. Cabo I. has received honoraria for educational presentations and advice service by Abbvie, Zambon, and Bial. López Manzanares L.: Compensated advisory services, consulting, research grant support, or speaker honoraria: AbbVie, Acorda, Bial, Intec Pharma, Italfarmaco, Pfizer, Roche, Teva, UCB, and Zambon. González Aramburu I.: None. Ávila Rivera MA. has received honoraria from Zambon, UCB Pharma, Qualigen, Bial, and Teva and sponsorship from Zambon and Teva for attending conferences. Gómez Mayordomo V.: None. Nogueira V.: None. Puente V. has served as consultant for Abbvie and Zambon; has received grant/research from Abbvie. Dotor García-Soto J.: Compensated advisory services, consulting, research grant support, or speaker honoraria: Merck, Sanofi-Genzyme, Allergan, Biogen, Roche, UCB, and Novartis. Borrué C.: None. Solano Vila B. has received honoraria for educational presentations and advice service by UCB, Zambon, Teva, Abbvie, and Bial. Álvarez Sauco M. has received honoraria for educational presentations and advice service by Abbvie, UCB Pharma, Zambon, Bial, and Teva. Vela L. has received honoraria for educational presentations and advice service by Abbvie, UCB Pharma, Lundbeck, KRKA, Zambon, Bial, and Teva. Escalante S. has received honoraria for educational presentations and advice service by Abbvie, Zambon, and Bial. Cubo E.: Travel grants: Abbvie, Allergan, Boston; Lecturing honoraria: Abbvie, International Parkinson´s disease Movement Disorder Society. Carrillo Padilla F. has received honoraria from Zambon (SEN Congress assistance). Martínez Castrillo JC. has received research support from Lundbeck, Italfarmaco, Allergan, Zambon, Merz, and Abbvie. He has received speaking honoraria from AbbVie, Bial, Italfarmaco, Lundbeck, Krka, TEVA, UCB, Zambon, Allergan, Ipsen, and Merz. Sánchez Alonso P. has received honoraria for educational presentations and advice service by Abbvie, UCB Pharma, Lundbeck, KRKA, Zambon, Bial, and Teva. Alonso Losada M. G. has received honoraria for educational presentations and advice service by Zambon and Bial. López Ariztegui N. has received honoraria for educational presentations and advice service by Abbvie, Italfarmaco, Zambon, and Bial. Gastón I. has received research support from Abbvie and Zambon and has served as a consultant for Abbvie, Exelts, and Zambon. Kulisevsky J.: (1) Consulting fees: Roche, Zambon; (2) Stock/allotment: No; (3) Patent royalties/licensing fees: No; (4) Honoraria (e.g. lecture fees): Zambon, Teva, Bial, UCB; (5) Fees for promotional materials: No; (6) Research funding: Roche, Zambon, Ciberned; Instituto de SaludCarlos III; FundacióLa Maratóde TV3; (7) Scholarship from corporation: No; (8) Corporate laboratory funding: No; (9) Others (e.g. trips, travel, or gifts): No. Blázquez Estrada M. has received honoraria for educational presentations and advice service by Abbvie, Abbott, UCB Pharma, Allergan, Zambon, Bial, and Qualigen. Seijo M. has received honoraria for educational services from KRKA, UCB, Zambon, Bial; travel grants from Daiichi and Roche. Ruiz Martínez J. has received honoraria for educational presentations, attending medical conferences, and advice service by Abbvie, UCB Pharma, Zambon, Italfarmaco, Bial, and Teva. Valero C. has received honoraria for educational services from Zambon, Abbvie, and UCB. Kurtis M. has received honoraria from Bial, the Spanish Neurology Society, and the International and Movement Disorders Society. de Fábregues O. has received honoraria for educational presentations and advice service by Bial, Zambon, Abbvie, KRKA, and Teva. González Ardura J. has recieved honoraria for speking from italofarma, Krka, Genzyme, UCB, Esteve, Psyma iberica marketing research SL and Ferrer, course grant from Teva and travel grant from Merck. Alonso Redondo R.: None. Ordás C.: None. López Díaz L. M. has received honoraria from UCB, Lundbeck, and KRKA. McAfee D.: None. Martínez-Martin P. has received honoraria from National School of Public Health (ISCIII), Editori-al Viguera and Takeda Pharmaceuticals for lecturing in courses, and from the International Parkinson and Movement Disorder Society (MDS) for management of the Program on Rating Scales. Mir P. has received honoraria from AbbVie, Abbott, Allergan, Bial, Merz, UCB, and Zambon and have received grants from the Spanish Ministry of Economy and Competitiveness [PI16/01575] co-founded by ISCIII (Subdirección General de Evaluación y Fomento de la Investigación) and by Fondo Europeo de Desarrollo Regional (FEDER), the Consejería de Economía, Innovación, Ciencia y Empleo de la Junta de Andalucía [CVI-02526, CTS-7685], the Consejería de Salud y Bienestar Social de la Junta de Andalucía [PI-0437-2012, PI-0471-2013], the Sociedad Andaluza de Neurología, the Jacques and Gloria Gossweiler Foundation, the Fundación Alicia Koplowitz, the Fundación Mutua Madrileña.
Authors' Contributions
Santos García D. performed conception, organization, and execution of the project, as well as statistical analysis, writing of the first draft of the manuscript, and recruitment and/or evaluation of participants. De Deus Fonticoba T. conducted review and critique as well as recruitment and/or evaluation of participants. Cores Bartolomé C. carried out collaboration in the preparation of the manuscript as well as review and critique. Feal Painceiras M. J. conducted collaboration in the preparation of the manuscript alongside review and critique. Íñiguez Alvarado M. C. performed collaboration in the preparation of the manuscript alongside review and critique. Jesús S. performed review and critique as well as recruitment and/or evaluation of participants. Buongiorno M. T. carried out review and critique and recruitment and/or evaluation of participants. Planellas LL. executed review and critique as well as recruitment and/or evaluation of participants. Cosgaya M. conducted review and critique as well as recruitment and/or evaluation of participants. García Caldentey J. conducted review and critique as well as recruitment and/or evaluation of participants. Caballol N. executed review and critique as well as recruitment and/or evaluation of participants. Legarda I. executed review and critique as well as recruitment and/or evaluation of participants. Hernández Vara J. executed review and critique and recruitment and/or evaluation of participants. Cabo I. performed review and critique and recruitment and/or evaluation of participants. López Manzanares L. performed review and critique and recruitment and/or evaluation of participants. González Aramburu I. performed review and critique and recruitment and/or evaluation of participants. Ávila Rivera M. A. performed review and critique and recruitment and/or evaluation of participants. Gómez Mayordomo V. performed review and critique and recruitment and/or evaluation of participants. Nogueira V. conducted review and critique and recruitment and/or evaluation of participants. Puente V. conducted review and critique and recruitment and/or evaluation of participants. Dotor García-Soto J. conducted review and critique and recruitment and/or evaluation of participants. Borrué C. conducted review and critique and recruitment and/or evaluation of participants. Solano Vila B. conducted review and critique and recruitment and/or evaluation of participants. Álvarez Sauco M. performed review and critique and recruitment and/or evaluation of participants. Vela L. carried out review and critique and recruitment and/or evaluation of participants. Escalante S. executed review and critique and recruitment and/or evaluation of participants. Cubo E. executed review and critique and recruitment and/or evaluation of participants. Carrillo Padilla F. executed review and critique and recruitment and/or evaluation of participants. Martínez Castrillo J. C. conducted review and critique and recruitment and/or evaluation of participants. Sánchez Alonso P. conducted review and critique and recruitment and/or evaluation of participants. Alonso Losada M. G. executed review and critique and recruitment and/or evaluation of participants. López Ariztegui N. executed review and critique and recruitment and/or evaluation of participants. Gastón I. executed review and critique and recruitment and/or evaluation of participants. Kulisevsky J. executed review and critique and recruitment and/or evaluation of participants. Blázquez Estrada M. executed review and critique and recruitment and/or evaluation of participants. Seijo M. executed review and critique and recruitment and/or evaluation of participants. Ruiz Martínez J. executed review and critique and recruitment and/or evaluation of participants. Valero C. conducted review and critique and recruitment and/or evaluation of participants. Kurtis M. conducted review and critique and recruitment and/or evaluation of participants. de Fábregues O. conducted review and critique and recruitment and/or evaluation of participants. González Ardura J. conducted review and critique and recruitment and/or evaluation of participants. Alonso Redondo R. conducted review and critique and recruitment and/or evaluation of participants. Ordás C. conducted review and critique and recruitment and/or evaluation of participants. López Díaz L. M. conducted review and critique and recruitment and/or evaluation of participants. McAfee D. conducted review and critique and review of English style. Martínez-Martin P. conducted review and critique and supervision. Mir P. executed review and critique and recruitment and/or evaluation of participants.
References
- 1.Miller N., Walshe M., Walker R. W. Research and Reviews in Parkinsonism . 2019;9:17–28. doi: 10.2147/jprls.s177409. [DOI] [Google Scholar]
- 2.Scott B., Borgman A., Engler H., Johnels B., Aquilonius S. M. Gender differences in Parkinson’s disease symptom profile. Acta Neurologica Scandinavica . 2000;102(1):37–43. doi: 10.1034/j.1600-0404.2000.102001037.x. [DOI] [PubMed] [Google Scholar]
- 3.Kalf J. G., Swart B. J. M., Borm G. F., Bloem B. R., Munneke M. Prevalence and definition of drooling in Parkinson’s disease: a systematic review. Journal of Neurology . 2009;256(9):1391–1396. doi: 10.1007/s00415-009-5098-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.van der Marck M. A., Kalf J. G., Sturkenboom I. H., Nijkrake M. J., Munneke M., Bloem B. R. Multidisciplinary care for patients with Parkinson’s disease. Parkinsonism & Related Disorders . 2009;15(3):S219–S223. doi: 10.1016/s1353-8020(09)70819-3. [DOI] [PubMed] [Google Scholar]
- 5.Leibner J., Ramjit A., Sedig L., et al. The impact of and the factors associated with drooling in Parkinson’s disease. Parkinsonism & Related Disorders . 2010;16:475–477. doi: 10.1016/j.parkreldis.2009.12.003. [DOI] [PubMed] [Google Scholar]
- 6.Muller B., Larsen J. P., Wentzel-Larsen T., Skeie G. O., Tysnes O. B., ParkWest Study G. Autonomic and sensory symptoms and signs in incident, untreated Parkinson’s disease: frequent but mild. Movement Disorders . 2011;26(1):65–72. doi: 10.1002/mds.23387. [DOI] [PubMed] [Google Scholar]
- 7.Perez-Lloret S., Negre-Pages L., Ojero-Senard A., et al. Oro-buccal symptoms (dysphagia, dysarthria, and sialorrhea) in patients with Parkinson’s disease: preliminary analysis from the French COPARK cohort. European Journal of Neurology . 2012;19(1):28–37. doi: 10.1111/j.1468-1331.2011.03402.x. [DOI] [PubMed] [Google Scholar]
- 8.Kalf J. G., Bloem B. R., Munneke M. Diurnal and nocturnal drooling in Parkinson’s disease. Journal of Neurology . 2012;259(1):119–123. doi: 10.1007/s00415-011-6138-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cersosimo M. G., Raina G. B., Pecci C. Gastrointestinal manifestations in PD: prevalence and occurrence before motor symptoms. Journal of Neurology . 2013;260:133–138. doi: 10.1007/s00415-012-6801-2. [DOI] [PubMed] [Google Scholar]
- 10.Nicaretta D. H., Rosso A. L., Mattos J. P. D., Maliska C., Costa M. M. B. Dysphagia and sialorrhea: the relationship to Parkinson’s disease. Arquivos de Gastroenterologia . 2013;50(1):42–49. doi: 10.1590/s0004-28032013000100009. [DOI] [PubMed] [Google Scholar]
- 11.Srivanitchapoom P., Pandey S., Hallett M. Drooling in Parkinson’s disease: a review. Parkinsonism & Related Disorders . 2014;20(11):1109–1118. doi: 10.1016/j.parkreldis.2014.08.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ou R., Guo X., Wei Q., et al. Prevalence and clinical correlates of drooling in Parkinson disease: a study on 518 Chinese patients. Parkinsonism & Related Disorders . 2015;21(3):211–215. doi: 10.1016/j.parkreldis.2014.12.004. [DOI] [PubMed] [Google Scholar]
- 13.Ou R. W., Guo X. Y., Wei Q. Q., et al. Diurnal drooling in Chinese patients with Parkinson’s disease. Journal of the Neurological Sciences . 2015;353(1-2):74–78. doi: 10.1016/j.jns.2015.04.007. [DOI] [PubMed] [Google Scholar]
- 14.Fereshtehnejad S. M., Skogar O., Lokk J. Evolution of orofacial symptoms and disease progression in idiopathic Parkinson’s disease: longitudinal data from the jönköping Parkinson registry. Parkinson’s Disease . 2017;2017:8. doi: 10.1155/2017/7802819.7802819 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nienstedt J. C., Buhmann C., Bihler M. Drooling is no early sign of dysphagia in PD. Neuro-Gastroenterology and Motility . 2018;30:p. 4. doi: 10.1111/nmo.13259. [DOI] [PubMed] [Google Scholar]
- 16.Edwards L. L., Pfeiffer R. F., Quigley E. M. M., Hofman R., Balluff M. Gastrointestinal symptoms in Parkinson’s disease. Movement Disorders . 1991;6(2):151–156. doi: 10.1002/mds.870060211. [DOI] [PubMed] [Google Scholar]
- 17.Kalf J. G., Smit A. M., Bloem B. R., Zwarts M. J., Munneke M. Impact of drooling in Parkinson’s disease. Journal of Neurology . 2007;254(9):1227–1232. doi: 10.1007/s00415-007-0508-9. [DOI] [PubMed] [Google Scholar]
- 18.Rajiah K., Maharajan M. K., Yeen S. J., Lew S. Quality of life and caregivers’ burden of Parkinson’s disease. Neuroepidemiology . 2017;48(3-4):131–137. doi: 10.1159/000479031. [DOI] [PubMed] [Google Scholar]
- 19.Barone P., Antonini A., Colosimo C., et al. The PRIAMO study: a multicenter assessment of nonmotor symptoms and their impact on quality of life in Parkinson’s disease. Movement Disorders . 2009;24(11):1641–1649. doi: 10.1002/mds.22643. [DOI] [PubMed] [Google Scholar]
- 20.Saleh J., Figueiredo M. A. Z., Cherubini K., Salum F. G. Salivary hypofunction: an update on aetiology, diagnosis and therapeutics. Archives of Oral Biology . 2015;60:242–255. doi: 10.1016/j.archoralbio.2014.10.004. [DOI] [PubMed] [Google Scholar]
- 21.Barbe A. G., Ludwar L., Scharfenberg I., et al. Circadian rhythms and influencing factors of xerostomia among Parkinson’s disease patients. Oral Diseases . 2019;25(1):282–289. doi: 10.1111/odi.12942. [DOI] [PubMed] [Google Scholar]
- 22.Barbe A. G., Bock N., Derman S. H. M., Felsch M., Timmermann L., Noack M. J. Self-assessment of oral health, dental health care and oral health-related quality of life among Parkinson’s disease patients. Gerodontology . 2017;34(1):135–143. doi: 10.1111/ger.12237. [DOI] [PubMed] [Google Scholar]
- 23.van Wamelen D. J., Leta V., Johnson J., et al. Drooling in Parkinson’s disease: prevalence and progression from the non-motor international longitudinal study. Dysphagia . 2020;35(6):955–961. doi: 10.1007/s00455-020-10102-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Rana A. Q., Khondker S., Kabir A., Owalia A., Khondker S., Emre M. Impact of cognitive dysfunction on drooling in Parkinson’s disease. European Neurology . 2013;70(1-2):42–45. doi: 10.1159/000348571. [DOI] [PubMed] [Google Scholar]
- 25.Fukuoka T., Ono T., Hori K., et al. Tongue pressure measurement and videofluoroscopic study of swallowing in patients with Parkinson’s disease. Dysphagia . 2019;34(1):80–88. doi: 10.1007/s00455-018-9916-5. [DOI] [PubMed] [Google Scholar]
- 26.Mao C. J., Xiong Y. T., Wang F., et al. Motor subtypes and other risk factors associated with drooling in Parkinson’s disease patients. Acta Neurologica Scandinavica . 2018;137(5):509–514. doi: 10.1111/ane.12893. [DOI] [PubMed] [Google Scholar]
- 27.Erro R., Picillo M., Vitale C., et al. The non-motor side of the honeymoon period of Parkinson’s disease and its relationship with quality of life: a 4-year longitudinal study. European Journal of Neurology . 2016;23(11):1673–1679. doi: 10.1111/ene.13106. [DOI] [PubMed] [Google Scholar]
- 28.Picillo M., Erro R., Amboni M., et al. Gender differences in non-motor symptoms in early Parkinson’s disease: a 2-years follow-up study on previously untreated patients. Parkinsonism & Related Disorders . 2014;20(8):850–854. doi: 10.1016/j.parkreldis.2014.04.023. [DOI] [PubMed] [Google Scholar]
- 29.Santos García D., Jesús S., Aguilar M., et al. COPPADIS-2015 (COhort of Patients with Parkinson’s DIsease in Spain, 2015): an ongoing global Parkinson’s disease project about disease progression with more than 1000 subjects included. Results from the baseline evaluation. European Journal of Neurology . 2019;26(11):1399–1407. doi: 10.1111/ene.14008. [DOI] [PubMed] [Google Scholar]
- 30.Santos-García D., Mir P., Cubo E., et al. COPPADIS-2015 (COhort of Patients with Parkinson’s DIsease in Spain, 2015), a global--clinical evaluations, serum biomarkers, genetic studies and neuroimaging--prospective, multicenter, non-interventional, long-term study on Parkinson’s disease progression. BMC Neurology . 2016;16(1):p. 26. doi: 10.1186/s12883-016-0548-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Hughes A. J., Daniel S. E., Kilford L., Lees A. J. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. Journal of Neurology, Neurosurgery & Psychiatry . 1992;55(3):181–184. doi: 10.1136/jnnp.55.3.181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Schade S., Mollenhauer B., Trenkwalder C. Levodopa equivalent dose conversion factors: an updated proposal including opicapone and safinamide. Mov Disord Clin Pract . 2020;7(3):343–345. doi: 10.1002/mdc3.12921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Chaudhuri K. R., Martinez-Martin P., Brown R. G., et al. The metric properties of a novel non-motor symptoms scale for Parkinson’s disease: results from an international pilot study. Movement Disorders . 2007;22(13):1901–1911. doi: 10.1002/mds.21596. [DOI] [PubMed] [Google Scholar]
- 34.Sampedro F., Martínez-Horta S., Horta-Barba A., et al. Clinical and structural brain correlates of hypomimia in early-stage Parkinson’s disease. European Journal of Neurology . 2022;29(12):3720–3727. doi: 10.1111/ene.15513. [DOI] [PubMed] [Google Scholar]
- 35.Santos García D., de Deus Fonticoba T., Cores C., et al. Falls predict acute hospitalization in Parkinson’s disease. Journal of Parkinson’s Disease . 2021;13(1):105–124. doi: 10.3233/JPD-212539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Santos García D., de Deus Fonticoba T., Suárez Castro E., et al. Non-motor symptoms burden, mood, and gait problems are the most significant factors contributing to a poor quality of life in non-demented Parkinson’s disease patients: results from the COPPADIS Study Cohort. Parkinsonism & Related Disorders . 2019;66:151–157. doi: 10.1016/j.parkreldis.2019.07.031. [DOI] [PubMed] [Google Scholar]
- 37.Nascimento D., Carmona J., Mestre T., Ferreira J. J., Guimarães I. Drooling rating scales in Parkinson’s disease: a systematic review. Parkinsonism & Related Disorders . 2021;91:173–180. doi: 10.1016/j.parkreldis.2021.09.012. [DOI] [PubMed] [Google Scholar]
- 38.Martinez-Martin P., Schapira A. H., Stocchi F., et al. Prevalence of nonmotor symptoms in Parkinson’s disease in an international setting; study using nonmotor symptoms questionnaire in 545 patients. Movement Disorders . 2007;22(11):1623–1629. doi: 10.1002/mds.21586. [DOI] [PubMed] [Google Scholar]
- 39.Siddiqui M. F., Rast S., Lynn M. J., Auchus A. P., Pfeiffer R. F. Autonomic dysfunction in Parkinson’s disease: a comprehensive symptom survey. Parkinsonism & Related Disorders . 2002;8(4):277–284. doi: 10.1016/s1353-8020(01)00052-9. [DOI] [PubMed] [Google Scholar]
- 40.Cheon S. M., Ha M. S., Park M. J., Kim J. W. Nonmotor symptoms of Parkinson’s disease: prevalence and awareness of patients and families. Parkinsonism & Related Disorders . 2008;14(4):286–290. doi: 10.1016/j.parkreldis.2007.09.002. [DOI] [PubMed] [Google Scholar]
- 41.Evatt M. L., Chaudhuri K. R., Chou K. L., et al. Dysautonomia rating scales in Parkinson’s disease: sialorrhea, dysphagia, and constipation--critique and recommendations by movement disorders task force on rating scales for Parkinson’s disease. Movement Disorders . 2009;24(5):635–646. doi: 10.1002/mds.22260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Nóbrega A. C., Rodrigues B., Torres A. C., Scarpel R. D., Neves C. A., Melo A. Is drooling secondary to a swallowing disorder in patients with Parkinson’s disease? Parkinsonism & Related Disorders . 2008;14(3):243–245. doi: 10.1016/j.parkreldis.2007.08.003. [DOI] [PubMed] [Google Scholar]
- 43.Miller N. Swallowing in Parkinson’s disease: clinical issues and management. Neurodegenerative Disease Management . 2017;7(3):205–217. doi: 10.2217/nmt-2017-0006. [DOI] [PubMed] [Google Scholar]
- 44.Ou R. W., Guo X. Y., Song W., et al. Characteristics of non-motor symptoms in patients with Parkinson’s disease exhibiting camptocormia. Gait & Posture . 2014;40(3):447–450. doi: 10.1016/j.gaitpost.2014.05.011. [DOI] [PubMed] [Google Scholar]
- 45.Tjaden K. Speech and swallowing in Parkinson’s disease. Topics in Geriatric Rehabilitation . 2008;24(2):115–126. doi: 10.1097/01.tgr.0000318899.87690.44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Karakoc M., Yon M. I., Cakmakli G. Y., et al. Pathophysiology underlying drooling in Parkinson’s disease: oropharyngeal bradykinesia. Neurological Sciences . 2016;37(12):1987–1991. doi: 10.1007/s10072-016-2708-5. [DOI] [PubMed] [Google Scholar]
- 47.Damian A., Adler C. H., Hentz J. G., et al. Autonomic function, as self-reported on the SCOPA-autonomic questionnaire is normal in essential tremor but not in Parkinson’s disease. Parkinsonism & Related Disorders . 2012;18(10):1089–1093. doi: 10.1016/j.parkreldis.2012.06.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Santos-García D., de Deus Fonticoba T., Bartolomé C. C., et al. Motor fluctuations development is associated with non-motor symptoms burden progression in Parkinson’s disease patients: a 2-year follow-up study. Diagnostics . 2022;12(5):p. 1147. doi: 10.3390/diagnostics12051147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Bloem B. R., Okun M. S., Klein C. Parkinson’s disease. The Lancet . 2021;397:2284–2303. doi: 10.1016/s0140-6736(21)00218-x.10291 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The protocol and the statistical analysis plan are available on request. Deidentified participants data are not available for legal and ethical reasons.