

Abstract
We report the case of a 33-year-old woman who was admitted to our clinic with the diagnosis of chronic arterial occlusion of the right lower extremity. Preoperative angiography suggested an iliofemoral atherosclerotic occlusion. During surgery, multiple hydatid cysts causing iliofemoral occlusion were found and excised. Arterial reconstruction was performed using an iliofemoral bypass technique with a polytetrafluoroethylene vascular graft. This case emphasizes that, in sheep-raising countries or in patients from such countries, primary vascular echinococcosis should be considered in the differential diagnosis of chronic arterial occlusion.
Key words: Arterial occlusive diseases, echinococcosis, femoral artery, iliac artery
Hydatidosis is a rare parasitic infestation that is characterized by hydatid cysts. Echinococcus granulosus is endemic in the sheep-raising regions of the world, including countries surrounding the Mediterranean, the Middle East, Central Europe, Australia, and South America. 1–3 The adult worm is found in the small intestine of the hosts (dogs), which acquire the parasite by eating the infected remains of an intermediate host (frequently, sheep). Accidental infection of human beings occurs after ingestion of the ova excreted by the host. The ingested ova hatch in the duodenum, penetrate the intestinal mucosa and enter the portal circulation, and are transported to the liver or lung. Thus hydatid cysts most often develop in the lung or liver, 2,3 and arterial localization of the echinococcosis is uncommon. 2,4
We performed an echinococcal cystectomy in a patient who had a rare case of primary arterial hydatidosis causing chronic arterial occlusion. The surgery and the difficulties of preoperative diagnosis are discussed herein.
Case Report
A 33-year-old woman was admitted to our clinic in May 1998 with findings of chronic arterial occlusion in the right lower extremity. She had continuing malaise and intermittent claudication at 100 meters. On physical examination, the right femoral and distal arterial pulses were absent. Laboratory tests yielded the following results: the erythrocyte sedimentation rate was 10 mm/hour, and the leukocyte count was 7,200 (1.7% eosinophilic leukocytes, 30% lymphocytes, 58% polymorphonuclear leukocytes, and 10.3% monocytes). Chest radiography showed nothing out of the ordinary. Arteriography showed complete occlusion of the right iliac and femoral arteries, and the circulation to the deep and superficial femoral arteries appeared to be supplied by collateral vessels (Figs. 1 and 2). Our preliminary diagnosis was atherosclerosis of the iliac and femoral arteries.
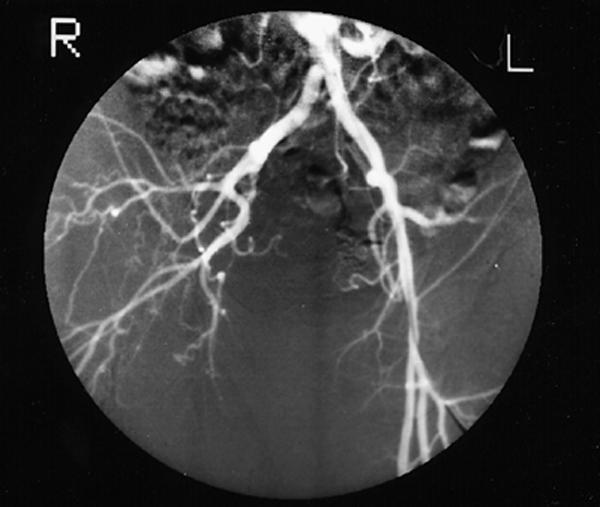
Fig. 1 Angiogram shows right iliac and femoral artery occlusion.
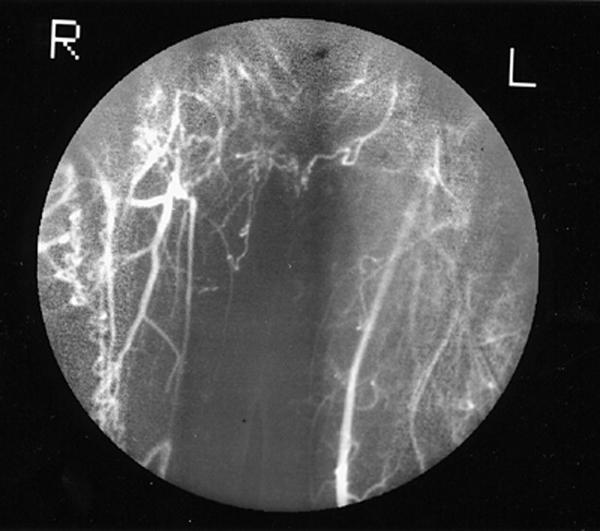
Fig. 2 The superficial femoral artery is filling by means of collateral circulation.
During surgical exploration of the groin, there was no pulse in the right iliac and femoral arteries. The arteries appeared irregular and larger than expected. The incision was extended and a pulsatile common iliac artery was reached through retroperitoneal exploration. A longitudinal arteriotomy that included the external iliac, common femoral, and superficial femoral arteries showed multiple hydatid cysts (Fig. 3), which were all removed. The distal run-off of the superficial femoral artery was normal. Iliofemoral bypass was performed with a 6-mm polytetrafluoroethylene (PTFE) ringed stretch vascular graft (W.L. Gore & Associates; Flagstaff, Ariz). Drains were placed and the wound was closed. No perioperative or early postoperative complication occurred, and the patient's symptoms arising from arterial occlusion resolved.
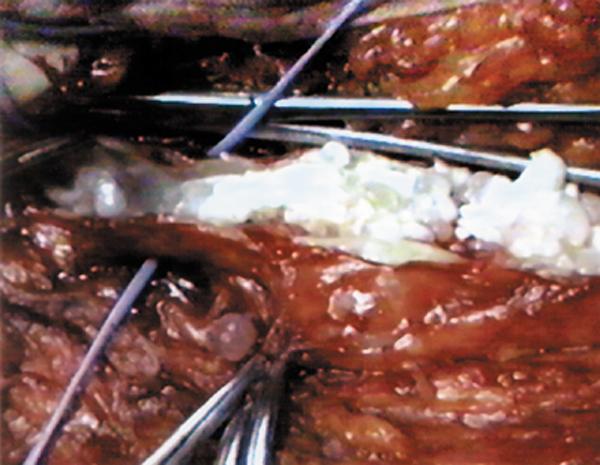
Fig. 3 Multiple hydatid cysts are seen within the lumen of the femoral artery.
The patient was given 15 mg/kg of albendazole for 30 days postoperatively. She underwent examination for cysts elsewhere in the body. Computed tomographic scans of the thorax, abdomen, and brain were performed 7 days after operation, but no primary origin of the hydatid cysts was found. Echocardiography showed a normal heart and great vessels. Therefore, the patient was discharged from the hospital on the 10th postoperative day. She was asymptomatic at 2-year follow-up physical examination.
Discussion
Hydatid cysts may appear anywhere in the human body; however, more than 90% localize in the liver (60%) and lungs (30%). 3,5 The remainder are found in other organs, such as the spleen, kidneys, pancreas, brain, and heart. 6 Arterial involvement of hydatid cysts usually develops after cardiac hydatid cyst rupture and embolization. 1,2,4 Primary arterial localization of hydatid cysts is extremely uncommon. 3,5,7 Yorukoglu and colleagues 3 presented a case of primary muscular hydatid cyst that obstructed the femoral artery and vein. They had observed apparent thrombosis of the superficial femoral artery and vein and performed a thrombectomy. Rada 5 treated a patient who had 2 hydatid cysts in the wall of the femoral artery and the adductor muscle. Papacharalambous and associates 7 described a patient who had a hydatid cyst in the lumen of the femoral artery, causing chronic arterial occlusion. Compared with the above-mentioned reports, our case is unique with respect to the number and location of the cysts.
A preoperative diagnosis of echinococcosis in locations other than the lungs and liver may be difficult—even in areas of the world where the disease is endemic—unless it is specifically considered as a possibility. Madariaga and coworkers 8 reported a case of femoral artery occlusion due to hydatid cysts, but their patient had presented with acute arterial occlusion and was diagnosed during arterial embolectomy.
The clinical presentation, chronic arterial occlusion, was different in our patient. Routine laboratory and radiographic findings were nonspecific—in particular, the eosinophilic leukocyte count and the chest X-ray. In the preoperative period, hydatidosis was not confirmed by serological testing because it was not considered as a cause of the chronic arterial occlusion. In addition, angiography supported an atherosclerotic origin of the occlusion and failed to reveal the hydatid disease. The diagnosis was finally established during the operation.
Surgical treatment of symptomatic cysts is optimal for complete cyst removal. For inoperable cysts, medical therapy with either albendazole or mebendazole provides improvement in most patients, but only about one third are completely rid of the disease. Albendazole is given to prevent dissemination and postoperative recurrence. In our patient, we administered 15 mg/kg of albendazole for 30 days after iliofemoral bypass.
Since this patient has been symptom-free for 2 years, we suggest that complete surgical excision of the cysts and arterial revascularization of the affected extremity with a bypass is an effective therapy for hydatidosis-related chronic arterial occlusion. In this patient, albendazole might also have assisted in the complete eradication of the cysts.
Footnotes
Address for reprints: Dr. Necdet Öz, Fabrikalar Mah. 3002 Sok., Güvercin AP. No:7, 07030 Antalya, Turkey
References
- 1.Panagiotis NS, Homeros A. Hydatid disease of the lung. In: Shields TW, editor. General thoracic surgery. 4th ed. Vol 2. Baltimore: William & Wilkins, 1994:1021–31.
- 2.Tuzuner A, Kuterdem E, Bac B, Oygur N, Uluoglu O, Aker H. An uncommon case of hydatid cyst localized on the endocardium causing arterial embolism. Vasa 1980;9:277–80. [PubMed]
- 3.Yorukoglu Y, Zengin M, Dolgun A, Nazliel K, Salman E, Pasaoglu E, et al. Primary muscular hydatid cyst causing arterial insufficiency: case report and literature review. Angiology 1993;44:399–401. [DOI] [PubMed]
- 4.Rosenberg T, Panayiotopoulos YP, Bastounis E, Papalambros E, Balas P. Acute abdominal aorta embolism caused by primary cardiac echinococcus cyst. Eur J Vasc Surg 1993;7: 582–5. [DOI] [PubMed]
- 5.Rada IO. Ischaemic syndrome of the lower limb produced by a hydatic cyst. J Cardiovasc Surg (Torino) 1986;27:282–5. [PubMed]
- 6.Eren EE, Aykut S, Kayihan A, Aydogan H, Dagsali S. Echinococcal cyst of the interventricular septum with right ventricular protrusion. Tex Heart Inst J 1989;16:292–5. [PMC free article] [PubMed]
- 7.Papacharalambous G, Panoussis P, Andrikopoulos V, Pappas P, Liapi G. Chronic arterial occlusion produced by hydatid cyst development in the lumen of the femoral artery. Eur J Vasc Endovasc Surg 1998;15:544–6. [DOI] [PubMed]
- 8.Madariaga I, de la Fuente A, Lezaun R, Imizcoz MA, Carmona JR, Urquia M, et al. Cardiac echinococcosis and systemic embolism. Report of a case. Thorac Cardiovasc Surg 1984;32:57–9. [DOI] [PubMed]