

Abstract
Objectives
The predictors of SARS-CoV-2 reinfection are unclear. We examined predictors of reinfection with pre-Omicron and Omicron variants among COVID-19-recovered individuals.
Methods
Randomly selected COVID-19-recovered patients (N = 1004) who donated convalescent plasma during 2020 were interviewed between August 2021 and March 2022 regarding COVID-19 vaccination and laboratory-proven reinfection. The sera from 224 (22.3%) participants were tested for antispike (anti-S) immunoglobulin G and neutralizing antibodies.
Results
The participants’ median age was 31.1 years (78.6% males). The overall reinfection incidence rate was 12.8%; 2.7% versus 21.6% for the pre-Omicron (mostly Delta) versus Omicron variants. Negative associations were found between fever during the first illness and pre-Omicron reinfection: relative risk 0.29 (95% confidence interval 0.09-0.94), high anti-N level at first illness and Omicron reinfection: 0.53 (0.33-0.85), and overall reinfection: 0.56 (0.37-0.84), as well as between subsequent COVID-19 vaccination with the BNT162b2 vaccine and pre-Omicron 0.15 (0.07-0.32), Omicron 0.48 (0.25-0.45), and overall reinfections 0.38 (0.25-0.58). These variables significantly correlated with immunoglobulin G anti-S follow-up levels. High pre-existing anti-S binding and neutralizing antibody levels against the SARS-CoV-2 Wuhan and Alpha strains predicted protection against Omicron reinfections.
Conclusion
Strong immune responses after the first COVID-19 infection and subsequent vaccination with the BNT162b2 vaccine provided cross-protection against reinfections with the Delta and Omicron variants.
Keywords: Omicron, Pre-omicron variants, Reinfection, Longitudinal study, Hybrid immunity
Introduction
Like many countries, Israel experienced several epidemic waves of COVID-19. The original SARS-CoV-2 Wuhan and the Alpha variants were the causes of the first three COVID-19 waves, while the Delta and the Omicron family variants were predominant in the fourth and fifth waves, respectively [1]. On December 19, 2020, Israel introduced the BNT162b2 mRNA vaccine in a vigorous immunization campaign, starting with the two-dose regimen, which conferred high protection against overall SARS-CoV-2 infection, COVID-19 hospitalizations, and deaths [2], [3], [4], [5]. Vaccination with one dose for COVID-19-recovered individuals at least 3 months after recovery has been recommended since March 2021. In July 2021, Israel was the first country to introduce a third vaccine dose (first booster) 5 months or more after the second dose [6] to contain the Delta variant-associated surge. A fourth injection of the BNT162b2 vaccine (second booster) was approved on December 31, 2021 for residents of long-term care facilities and later, for the general population aged 60 years or older [7,8]. The goal was to provide cross-protection against SARS-CoV-2 infections associated with the Omicron variant that surged in Israel after mid-December 2021 and prevent severe illness. Indeed, among the Israeli population aged 60 years or older, the protection conferred by the fourth BNT162b2 dose ranged from 45% to 50% against infection and 62% to 71% against severe COVID-19 1-4 weeks after vaccination compared with vaccination with three doses 4 months or earlier [7], [8], [9].
It was shown that COVID-19-recovered individuals who received one or more COVID-19 vaccine doses had a lower risk of reinfection with SARS-CoV-2 Wuhan (wild-type), Alpha, and Delta variants than recovered individuals who were not further vaccinated or individuals who received the vaccine only [10], [11], [12], [13]. Despite this evidence less is known about the short- and long-term protection conferred by hybrid immunity, namely the combined effect of naturally acquired immunity and vaccine-induced immunity against SARS-CoV-2 variants belonging to the Omicron family and how this correlates with the binding and neutralizing antibody levels against the corresponding variants [10,14,15].
The aim of this study was to examine potential predictors of reinfection with pre-Omicron and Omicron variants among individuals who recovered from COVID-19 during the first year of the pandemic. Particularly, we assessed the role of immunoglobulin (IgG) antibody response to the nucleocapsid (N) antigen after the primary SARS-CoV-2 infection, demographics and clinical indicators during the primary (first) COVID-19 episode, and subsequent COVID-19 vaccination with the BNT162b2 vaccine. Eventually, we examined whether the risk of reinfection with Omicron variants was associated with pre-existent binding and neutralizing antibody levels induced by pre-Omicron SARS-CoV-2 infection and/or vaccination with the BNT162b2 vaccine based on Wuhan strain-derived spike (S) antigen.
Materials and methods
Study population and design
COVID-19 convalescent plasma (CCP) donors (n = 5486) between April 4, 2020 and April 26, 2021 who recovered from reverse transcription-polymerase chain reaction (RT-PCR)-documented SARS-CoV-2 infection and were tested for anti-N SARS-CoV-2 antibodies were followed up. Recovery from COVID-19 was determined by two consecutive negative RT-PCR test results, at least 24 hours apart, after symptoms have resolved. An additional 14-day deferral was needed before plasma collection.
Serological testing and plasma donations were performed approximately 6 weeks after disease onset in the framework of Magen David Adom (MDA) National Blood Services. The CCP donors were males or nulliparous females [16]. Donors signed written informed consent for the CCP collection and filled-in the donor health questionnaire.
In this prospective study, a random age-stratified sample of 2158 individuals was selected among the 5486 CCP donors for a follow-up assessment comprising interviews from August 9, 2021 to December 15, 2021, capturing the Delta wave, and from December 16, 2021 to March 28, 2022, capturing Omicron waves (Supplementary Figure 1). The CCP donors interviewed were asked on the history of COVID-19 vaccination, frequency of testing, and laboratory-proven reinfection (and symptoms) occurring between the date of the primary COVID-19 illness and the date of the interview. CCP donors who agreed to participate were invited to MDA donation sites to provide a blood sample for SARS-CoV-2 serology testing. The pre-Omicron component of the study included all 1004 participants as the population at risk. The actuarial period, in which we counted new pre-Omicron SARS-CoV-2 reinfections, spanned from at least 3 months after the primary infection until December 15, 2021. The Omicron component included 473 of the 1004 participants interviewed between December 16, 2021 and March 28, 2022 as the population at risk in the actuarial period, during which we counted new SARS-CoV-2 reinfections (predominantly Omicron variants B.A.1 and B.A.2) [1].
Definitions
The outcome variables
-
1.
Reinfection with SARS-CoV-2, which was defined as a self-report on positive RT-PCR test result at least 3 months after the recovery from primary COVID-19 episode, and those with COVID-19-related symptoms were considered as having symptomatic reinfection. In the Omicron study component, SARS-CoV-2 infection confirmation was based on either RT-PCR or antigen positivity, compatible with the standard of care during this period.
-
2.
IgG anti-S antibody level as measured by the Abbott anti-S chemiluminescent immunoassay (CLIA) kit in each serum sample and expressed as geometric mean concentrations (GMCs).
-
3.
Neutralizing antibody titers as detected by the SARS-CoV-2 microneutralization assay against SARS-CoV-2 Wild-type, Alpha B.1.1.7, Delta B.1.617.2, and Omicron B.1.1.529 variants.
Exposure variables
The exposure variables included demographics (age in years and sex), fever (measured body temperature >38°C), and hospitalization (yes or no), all during the primary COVID-19 illness, as reported by the participants at the first CCP donation. Anti-N IgG antibody level (dichotomous variable) was defined as “low”, ranging from negativity to a value below 4 Signal-to-cutoff ratio (S/CO), and “high”, equal or above 4 S/CO [17], as measured before the first CCP donation. COVID-19 vaccination status was defined as self-report on the number of BNT162b2 vaccine doses received at least 3 months after the primary SARS-CoV-2 infection and until the interview date.
Laboratory methods
All primary illness CCP serum samples were tested for anti-N by CLIA, performed on the Architect i2000 SR (Abbott, Green Oaks, IL, USA) automated immunoassay analyzer [17]. A quantitative measurement of IgG anti-S antibodies was performed by the same methodology on Abbott Architect i2000 automated immunoassay analyzer, following the manufacturer's instructions. The follow-up sera were re-tested for total antibodies (including IgG) to SARS-CoV-2 N antigen using the electro-CLIA (ECLIA) (Elecsys Anti-SARS-CoV-2, Roche Diagnostics, Rotkreuz, Switzerland).
Viral isolation of the Wild-type, Beta, Delta, and Omicron variants, viral titration, and microneutralization assay were performed as previously described [18] (Supplementary Material). IgG anti-S and neutralizing antibody levels to the Wuhan (wild-type) strain were calibrated against the National Institute for Biological Standards and Control International Standard 20/136; the results we expressed in binding arbitrary units (BAU/ml) and international units/ml, respectively [19,20], which facilitates international comparisons.
Statistical analysis
Data were analyzed using IBM SPSS version 28 (IBM Corporation, Armonk, NY, USA). We calculated the cumulative incidence of SARS-CoV-2 reinfection (per 100 persons) according to the exposure variables, separately for the pre-Omicron and Omicron periods. Bivariate and multivariable analyses were performed using the negative binomial regression, with the log link model with reinfection as the dependent variable, yielding risk ratios (RRs) with corresponding 95% confidence intervals (CIs). The homogeneity of the associations between the various predictors and reinfection with pre-Omicron and Omicron SARS-CoV-2 was examined using the Breslow-Day test of homogeneity. A sensitivity analysis included a reanalysis of data using the Poisson log-linear regression, in which person-months of each participant from the primary SARS-CoV-2 infection until the reinfection was used as an offset. We also used a test-negative case-control study design, in which cases comprised participants with reinfection and the controls those who tested negative implementing logistic regression models that yielded odds ratios and 95% CI.
The IgG anti-S antibody concentrations and neutralizing antibody titers were expressed as geometric mean concentration or titer (GMC or GMT) (with 95% CI) by the exposure variables. Bivariate analyses, using Student's t-test, one-way analysis of variance, and Spearman rank correlation coefficients, and multivariate linear regression models were used to identify correlates of the concentration of anti-S antibodies. All tests were two-tailed and P-values <0.05 were considered statistically significant.
Results
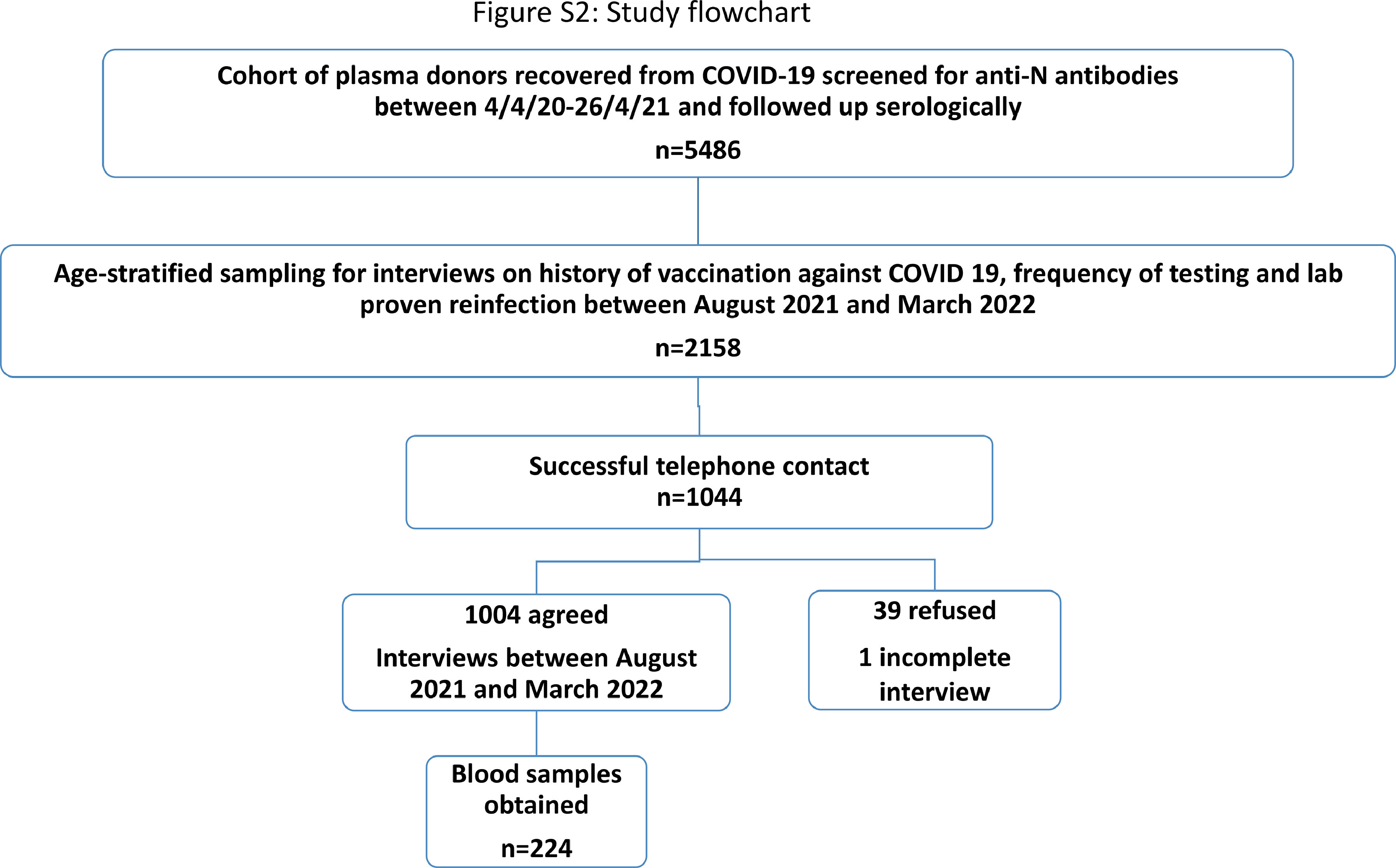
Of the 2158 randomly selected CCP donors, 1044 were successfully contacted. Of those, 1004 (median age 31.1 years, 78.6% males) agreed to participate and completed the questionnaire; 224 provided a blood sample for SARS-CoV-2 serology testing shortly after the interview (Supplementary Figure 2). A subset of 82 participants had the sera collected before the surge of the Omicron wave.
Of the 1004 participants, 60.8% had fever and 15.3% were hospitalized during the course of the primary COVID-19 episode between March 2020 and March 2021; 45.2%, 33.5%, and 7.6% subsequently received one, two, and three or more doses of the BNT162b2, respectively, and 13.7% remained unvaccinated. The participants had similar characteristics to the overall cohort of 5458 CCP donors (Table S1, Supplementary material).
Determinants of SARS-CoV-2 reinfection: the pre-Omicron study component
Overall, 27 participants (of 1004) had SARS-CoV-2 reinfections during the pre-Omicron era, (until December 15, 2021), yielding an incidence rate of 2.7% (95% CI 1.8-3.8) (Table 1 ); of those, 22 were symptomatic. These reinfections (mostly Delta variant) occurred between 4.6 and 18.0 months after the primary COVID-19 illness (median = 11.4 months; interquartile range = 6.8-13.6).
Table 1.
Determinants of reinfection with SARS-CoV-2 in the pre-Omicron and Omicron waves.
| Pre-Omicron |
Omicron |
Overall |
|||||
|---|---|---|---|---|---|---|---|
| n/total (%) | P-value⁎ | n/total (%) | P-value⁎ | n/total (%) | P-value⁎ | P for interaction | |
| Overall | 27/1004 (2.7%) | 102/473 (21.6%) | 129/1004 (12.8%) | ||||
| Age, years | |||||||
| 18-34 | 15/576 (2.6%) | 0.846 | 70/271 (25.8%) | 0.009 | 85/576 (14.8%) | 0.036 | 0.125⁎⁎ |
| ≥35 | 12/428 (2.8%) | 32/202 (15.8%) | 44/428 (10.3%) | ||||
| Sex | |||||||
| Males | 21/789 (2.7%) | 1.000 | 80/378 (21.2%) | 0.677 | 101/789 (12.8%) | 0.909 | 0.845⁎⁎ |
| Females | 6/215 (2.8%) | 22/95 (23.2%) | 28/215 (13.0%) | ||||
| Fever at primary infection | |||||||
| <38°C | 9/258 (3.5%) | 0.041 | 24/108 (22.2%) | 0.886 | 33/258 (12.8%) | 0.905 | 0.158⁎⁎ |
| ≥38°C | 4/400 (1.0%) | 46/217 (21.2%) | 50/400 (12.5%) | ||||
| Hospitalization at primary infection | |||||||
| Yes | 8/154 (5.2%) | 0.053 | 13/58 (22.4%) | 0.865 | 21/154 (13.6%) | 0.793 | 0.302⁎ |
| No | 19/850 (2.2%) | 89/415 (21.4%) | 108/850 (12.7%) | ||||
| Anti-N at primary infection | |||||||
| Negative & Positive - up to 4 | 20/603 (3.3%) | 0.164 | 74/276 (26.8%) | 0.001 | 94/603 (15.6%) | 0.001 | 0.678⁎⁎ |
| Positive 4+ | 7/401 (1.7%) | 28/197 (14.2%) | 35/401 (8.7%) | ||||
| COVID-19 vaccination status | |||||||
| 0 doses | 14/138 (10.1%) | <0.001 | 24/61 (39.3%) | <0.001 | 38/138 (27.5%) | <0.001 | 0.133⁎⁎ |
| 1+ doses | 13/866 (1.5%) | 78/412 (18.9%) | 91/866 (10.5%) | ||||
| COVID-19 vaccination status | |||||||
| 0 doses | 14/138 (10.1%) | <0.001 | 24/61 (39.3%) | 0.001 | 38/138 (27.5%) | <0.001 | 0.489# |
| 1 dose | 8/454 (1.8%) | 44/199 (22.1%) | 52/454 (11.5%) | ||||
| 2 doses | 5/336 (1.5%) | 28/162 (17.3%) | 33/336 (9.8%) | ||||
| 3+ doses | 0/76 (0%) | 6/51 (11.8%) | 6/76 (7.9%) | ||||
P-value by Fisher's exact test.
Breslow-Day test of homogeneity.
Negative binomial regression with log link models testing for interaction.
The risk of reinfection was significantly reduced by 71% (P = 0.039) in recovered individuals with fever during the primary COVID-19 episode than those without fever and by 85% (P <0.001) among individuals who were subsequently vaccinated with the BNT162b2 vaccine versus unvaccinated ones (Table 2 ). The reinfection risk reductions were similar when the vaccinees group was divided into three groups according to the number of vaccine doses received (Table 1 and 2). In the multivariable model, having fever during the primary COVID-19 illness (adjusted RR 0.23 [95% CI 0.07-0.80], P = 0.021) and subsequent COVID-19 vaccination (adjusted RR 0.07 [95% CI 0.02-0.23], P <0.001) remained significantly associated with a decreased risk of reinfection, respectively (Table S2, Supplementary material).
Table 2.
Bivariate analysis of determinants of reinfection with SARS-CoV-2 in the pre-Omicron and Omicron waves.
| Pre-Omicron |
Omicron |
Overall |
||||
|---|---|---|---|---|---|---|
| Unadjusted RR (95% CI)* | P-valuea | Unadjusted RR (95% CI)a | P-valuea | Unadjusted RR (95% CI)* | P-valuea | |
| Age, years | ||||||
| 18-34 | 1.00 (Reference) | - | 1.00 (Reference) | - | 1.00 (Reference) | - |
| ≥35 | 1.08 (0.5-2.32) | 0.851 | 0.61 (0.39-0.97) | 0.036 | 0.69 (0.47-1.02) | 0.066 |
| Sex | ||||||
| Males | 1.00 (Reference) | - | 1.00 (Reference) | - | 1.00 (Reference) | - |
| Females | 1.05 (0.42-2.63) | 0.920 | 1.09 (0.65-1.85) | 0.736 | 1.01 (0.65-1.58) | 0.940 |
| Fever at primary infection | ||||||
| <38°C | 1.00 (Reference) | - | 1.00 (Reference) | - | 1.00 (Reference) | - |
| ≥38°C | 0.29 (0.09-0.94) | 0.039 | 0.95 (0.55-1.65) | 0.865 | 0.97 (0.61-1.55) | 0.923 |
| Hospitalization at primary infection | ||||||
| Yes | 2.32 (1.00-5.40) | 0.050 | 1.05 (0.55-1.99) | 0.893 | 1.07 (0.652-1.76) | 0.781 |
| No | 1.00 (Reference) | - | 1.00 (Reference) | - | 1.00 (Reference) | - |
| Anti-N at primary infection | ||||||
| Negative & Positive-up to 4 | 1.00 (Reference) | - | 1.00 (Reference) | - | 1.00 (Reference) | - |
| Positive 4+ | 0.53 (0.22-1.26) | 0.148 | 0.53 (0.33-0.85) | 0.008 | 0.56 (0.37-0.84) | 0.005 |
| COVID-19 vaccination status | ||||||
| 0 doses | 1.00 (Reference) | - | 1.00 (Reference) | - | 1.00 (Reference) | - |
| 1+ doses | 0.15 (0.07-0.32) | <0.001 | 0.48 (0.28-0.82) | 0.007 | 0.38 (0.25-0.58) | <0.001 |
| COVID-19 vaccination status | ||||||
| 0 doses | 1.00 (Reference) | - | 1.00 (Reference) | - | 1.00 (Reference) | - |
| 1 doses | 0.17 (0.07-0.42) | <0.001 | 0.56 (0.32-0.99) | 0.049 | 0.41 (0.26-0.65) | <0.001 |
| 2 doses | 0.15 (0.05-0.42) | <0.001 | 0.44 (0.24-0.82) | 0.009 | 0.35 (0.21-0.59) | <0.001 |
| 3+ doses | - | - | 0.30 (0.11-0.79) | 0.015 | 0.28 (0.11-0.70) | 0.007 |
| Time from primary infection to interview, (months, continuous variable) | 0.93 (0.83-1.04) | 0.202 | 0.94 (0.86-1.04) | 0.234 | 1.05 (0.98-1.11) | 0.128 |
CI, confidence interval; RR, risk ratio.
RR and P-values were obtained from bivariate negative binomial with log link models, with SARS-CoV-2 reinfection as the dependent variable.
Determinants of SARS-CoV-2 reinfection during the Omicron B.A.1 and B.A.2 wave
The overall incidence of reinfection during the Omicron (December 16, 2021 to March 28, 2022) wave was 21.6% (102/473; 95% CI 18.0-25.4) (Table 1); of those, 90 (88.2%) had symptoms. These reinfections occurred between 12.7 and 22.2 months after the primary COVID-19 illness (median = 16.8 months, interquartile range = 15.7-18.4).
The risk of reinfection was significantly lower by 39% (P = 0.036) in recovered participants aged 35 years and older than in younger ones, by 47% (P = 0.008) in those with high anti-N antibody level after the primary COVID-19 episode versus those with low anti-N antibody levels, and by 52% (P = 0.007) in COVID-19 vaccinees versus unvaccinated ones (Table 2). A linear trend of decreased reinfection rate with Omicron variants (P = 0.001) was associated with the number of vaccine doses received (Tables 1 and 2). In the multivariable model, a high anti-N antibody level at the primary episode and subsequent COVID-19 vaccination were significantly associated with a lower risk of reinfection: adjusted RR 0.59 (95% CI 0.36-0.95), P = 0.031 and adjusted RR 0.47 (95% CI 0.28-0.82]), P = 0.007, respectively (Table S3, Supplementary material).
The homogeneity analysis of the associations between the various predictors and reinfection with pre-Omicron and Omicron SARS-CoV-2 variants showed no significant interactions (Table 1), enabling a pooled analysis of the predictors of reinfection incidence (Tables 1, 2 and S4).
Similar results on the association between predictors and the risk of reinfection were obtained in sensitivity analyses using the Poisson regression model and the test-negative case-control analysis (Tables S5-S12, Supplementary material).
RT-PCR or antigen testing to detect SARS-CoV-2 reinfections was similar across the exposure variables among the participants (Table S13).
Correlates of anti-S IgG levels
The characteristics of individuals who provided a blood sample at the follow-up (224/1004, 22.3%) were similar to those of the entire cohort of 1004 participants (Table S1, Supplementary material).
Tables 3 displays the serological results of anti-S IgG levels in 204 participants who had no documented reinfection during the study, showing the net effect of the independent variables on the IgG anti-S antibody level at the follow-up. A significant 3-fold increase in IgG anti-S GMTs (854 [95% CI 664-1098]) was detected in recovered individuals who had high IgG anti-N levels at their first plasma donation than those with low or undetectable levels IgG anti-N levels (234 [95% CI 147-372]), (P <0.001)]. A total of 87% percent of individuals positive for anti-N at primary infection were still positive at the follow-up measurement. Participants vaccinated after recovery from COVID-19 had an IgG anti-S GMC that was 13-fold higher than unvaccinated ones (716 [95% CI 579-885] vs 38 [95% CI 14-100], respectively, P <0.001). Moreover, a dose-response relationship, albeit not statistically significant, was found between the number of vaccine doses received and GMC levels (Table 3). The time (in months) from the first CCP donation to the follow-up serological test correlated positively with the anti-S IgG levels (Spearman r = 0.293 (P <0.001) (Table 3).
Table 3.
Bivariate analysis of the correlates of anti-S IgG antibody levels at the follow-up assessment among participants without reinfection.
| Number interviewed | Number tested for IgG anti-S | Geometric mean concentration (95% CI) | P-valuea | |
|---|---|---|---|---|
| Age, years | ||||
| 18-34 | 491 | 82 | 412 (291-583) | 0.473* |
| ≥35 | 384 | 122 | 503 (341-741) | |
| Sex | ||||
| Males | 688 | 173 | 467 (345-633) | 0.913* |
| Females | 187 | 31 | 448 (258-777) | |
| Fever at primary infection | ||||
| <38°C | 225 | 62 | 481 (274-843) | 0.433* |
| ≥38°C | 350 | 77 | 622 (428-903) | |
| Hospitalization at primary infection | ||||
| Yes | 133 | 38 | 656 (370-1164) | 0.226a |
| No | 742 | 166 | 429 (316-582) | |
| Anti-N at primary infection | ||||
| Negative & Positive - up to 4 | 509 | 96 | 234 (147-372) | <0.001a |
| Positive 4+ | 366 | 108 | 854 (664-1098) | |
| COVID-19 vaccination status | ||||
| 0 doses | 100 | 30 | 38 (14-100) | <0.001a |
| 1+ doses | 775 | 174 | 716 (579-885) | |
| COVID-19 vaccination status | ||||
| 0 doses | 100 | 30 | 38 (14-100) | <0.001b |
| 1 dose | 402 | 79 | 603 (431-844) | |
| 2 doses | 303 | 72 | 802 (578-1113) | |
| 3+ doses | 70 | 23 | 906 (551-1489) | |
| Time from 1st vaccine to anti-S testing, months | 128 | r = -0.084c | 0.345 | |
| Time from primary infection to anti-S testing, months | 194 | r = 0.293c | <0.001 | |
CI, confidence interval; Ig, immunoglobulin; S, spike.
P-value was obtained by Student's t-test or bindependent sample Kruskal-Wallis test
Spearman correlation coefficient
A stratified analysis by anti-N levels at the first donation and vaccination status showed that the highest IgG anti-S GMC of 1067.5 (95% CI 857.9-1328.3) was measured in participants with high anti-N IgG level at the first donation who subsequently were vaccinated (Table S14, Supplementary material). In a multiple linear regression model, a high anti-N IgG level at first infection (beta coefficient 0.896 [95% CI 0.433-1.359], P <0.001) and COVID-19 vaccination (beta coefficient 2.686 [95% CI 2.048-3.324], P <0.001) were significantly associated with the IgG anti-S level at the follow-up, as well as the time that elapsed between the primary COVID-19 episode and serology testing (Table S15, Supplementary material). The latter correlated with the number of vaccine doses (Spearman r = 0.16, P = 0.029, n = 187). Tables S16 and S17 (Supplementary material) display the corresponding results in all 224 participants.
Pre-existent IgG anti-S and neutralizing antibodies and reinfection with Omicron variants
Overall, 82 of the 224 participants who provided sera at the follow-up had sera collected before the surge of the Omicron wave. Participants with no subsequent reinfection during the Omicron wave had significantly higher pre-existent IgG anti-S and neutralizing antibodies to the wild-type SARS-CoV-2 and Alpha variants but not to the Delta variant versus participants with reinfections. The anti-Omicron GMTs were low in the sera collected before the Omicron wave and not related to reinfection (Table 4 ). Pre-existent ln IgG anti-S binding and log2 neutralizing antibody titers to the four variants highly correlated (r = 0.82 to 0.87; P <0.001).
Table 4.
Pre-existent IgG anti-S antibodies and neutralizing antibodies geometric mean concentration/geometric mean titer (95% confidence intervals) and reinfection with Omicron-related variants.
| Reinfection |
P-valuea | ||
|---|---|---|---|
| No (n = 54) | Yes (n = 28) | ||
| Pre-existent IgG anti-S (binding arbitrary unit/ml) | 512 (315-834) | 126 (54-293) | 0.005 |
| Pre-existent NA against: | |||
| Wild-type virus (titer) | 682 (378-1229) | 202 (70-584) | 0.030 |
| Wild-type virus (IU/ml) | 338 (191-598) | 104 (38-284) | 0.030 |
| Alpha (titer) | 450 (248-817) | 119 (37-87) | 0.026 |
| Delta (titer) | 397 (220-717) | 157 (58-429) | 0.089 |
| Omicron (titer) | 30 (13-69) | 9 (2-33) | 0.103 |
Ig, immunoglobulin; S, spike.
P-values were obtained by Student's t-test for continuous variables and the Fisher's exact test for dichotomous variables
A threshold level of 800 BAU/ml derived from the distribution of logarithmic transformed levels of pre-existing binding IgG anti-S antibodies among individuals with and without reinfection with Omicron variants was associated with 58% (95% CI 2-82%) lower risk of reinfection with Omicron variants, and a threshold level of 500 IU/ml of neutralizing antibodies against the ancestor Wuhan strain was associated with 50% lower reinfection risk (Table 5 ).
Table 5.
Thresholds of pre-existent IgG anti-S antibodies and neutralizing antibodies and estimates of protection against reinfection with Omicron-related variants.
| Total | Reinfection, n (%) | Risk ratio (95% confidence interval) | P-value | Risk reduction | |
|---|---|---|---|---|---|
| Total | 82 | 28 | - | - | - |
| Anti-S antibodies | |||||
| <800 BAU/ml | 54 | 23 (42.6%) | Reference | 0.029 | 58% (2%-82%) |
| ≥800 BAU/ml | 28 | 5 (17.9%) | 0.42 (0.18-0.98) | ||
| Neutralizing antibodies to Wuhan strains | |||||
| <500 IU/ml | 40 | 19 (47.5%) | Reference | 0.035 | 50% (4%-74%) |
| ≥500 IU /ml | 38 | 9 (23.7%) | 0.50 (0.26-0.96) | ||
BAU, binding arbitrary unit; Ig, immunoglobulin; S, spike.
Discussion
We determined the incidence of reinfection with pre-Omicron and Omicron SARS-CoV-2 variants in a cohort of 1004 COVID-19 CCP donors.
The main findings are that reinfections occurred in this highly immune population of COVID-19 recovered individuals, who mostly were vaccinated with the BNT162b2 vaccine. We found significant associations of history of post-primary infection COVID-19 vaccination and pre-existent immune response with reinfection risk.
The cumulative incidence of reinfection with Omicron variant was higher than reinfection with the pre-Omicron variants, likely due to the higher transmission, greater immune escape of Omicron, or both [21], [22], [23].
Vaccination with at least one dose of BNT162b2 vaccine conferred 85% protection against reinfection with pre-Omicron variants. Recovered individuals with fever during the primary infection had a significant 71% lower risk of reinfection during the pre-Omicron period, possibly due to more enhanced immune response during the primary infection [24].
The risk of reinfection with Omicron variant was reduced by 52% among recovered individuals vaccinated with BNT162b2 vaccine and followed a dose-response pattern. In addition, the high level of anti-N level at primary infection was associated with a 47% lower reinfection risk, thus highlighting the importance of both variables in immunity against Omicron reinfection. Although vaccination with BNT162b2 vaccine provides anti-S “booster” after the primary SARS-CoV-2 infection, anti-N level at the first infection likely reflects an extended breadth of the immune response, both cellular and humoral, including anti-S IgG binding and neutralizing antibodies [25] and possibly antibodies against other viral epitopes.
The highest anti-S GMC at the follow-up was found among recovered participants with high anti-N level at the first infection who subsequently received the BNT161b2 vaccine, followed by vaccinated ones who had a low baseline anti-N level, and finally, unvaccinated individuals, thus emphasizing the pivotal role of COVID-19 vaccination in recovered individuals to attain sufficient immunity. Gazit et al. showed that persons with confirmed-SARS-CoV-2 infection who received a single dose of BNT162b2 vaccine at least 3 months after the primary infection had an 82% reduced risk of reinfection versus recovered persons who did not receive COVID-19 vaccination [11]. This and other studies [11,14] on COVID-19-recovered individuals have captured mainly the Delta wave, and they support our findings regarding the importance of COVID-19 vaccination in recovered persons for the prevention of reinfection. A study from Qatar [10] showed that hybrid immunity resulting from previous SARS-CoV-2 infection and recent receipt of a booster dose of COVID-19 mRNA vaccine conferred the strongest protection against Omicron infection. A vaccine boost in recovered individuals reaches the highest and most stable levels of binding and functional antibodies against SARS-CoV-2 [26,27].
Importantly, in our cohort, the primary COVID-19 episode occurred during the first year of the pandemic, before the emergence of the Delta and Omicron variants, and comprised mostly of the original Wuhan strain and Alpha variant. Moreover, the BNT162B2 vaccine is based on the Wuhan strain-derived S antigen. Compared with the Wuhan strain, the SARS-CoV-2 variants of concern display mutations in the S antigen, culminating with more than 30 such mutations in the Omicron variant, resulting in significant resistance to naturally acquired or vaccine-induced immunity [21,22]. It was postulated that the heterologous protection might be achieved against Delta and Omicron variants by increasing the levels of neutralizing anti-S antibodies, and this was indeed attained by means of hybrid immunity, as demonstrated by our nested serological analysis of 82 recovered individuals with available pre-Omicron sera. We found higher levels of pre-existent anti-S IgG binding antibodies and pre-existent neutralizing antibodies to the wild-type Wuhan strain and Alpha variant among individuals without subsequent reinfection versus those with Omicron reinfection. We determined that the putative threshold levels of 800 BAU/ml IgG anti-S to the Wuhan strain associated with a 58% estimated protection against the heterologous Omicron reinfection, and a threshold titer of neutralizing antibodies of 500 IU/ml to Wuhan associated a conferred 50% protection against Omicron reinfection. Similar association and threshold levels of IgG anti-S binding antibodies were reported [28] in a comprehensive study from South Africa (668 BAU/ml IgG anti-Wild Type-Spike associated with 50% protection against Omicron in recovered and vaccinated mothers).
It follows that hybrid immunity reaching a critical pre-existing level of anti-S IgG binding and neutralizing antibodies could be sufficient to prevent reinfections with new SARS-CoV-2 variants, even with substantial genetic changes. These findings are of importance presently in populations that have been extensively exposed to both SARS-CoV-2 infections and COVID-19 vaccines, in which the segment of naïve individuals becomes limited. Moreover, under the uncertainty of the emergence of new variants of concerns, revaccination with the existent mRNA and other subunit vaccines, inducing a robust serum antibody response could be sufficient to prevent reinfections for at least a few months until modified vaccines of increased homology could be administered.
Our study has limitations. We could reestablish contact with only 48.4% of the sampled individuals. Nonetheless, the baseline characteristics of the study participants were similar to the entire cohort of CCP donors. Moreover, only 22% of the participants provided sera at the follow-up, but those who provided sera had comparable characteristics to the entire study participants. Testing for SARS-CoV-2 was similar across the different categories of the exposure variables, thus eliminating the potential differential effect of testing-seeking behavior. Lastly, the information on COVID-19 vaccination and reinfection was based on self-reports. Self-report on vaccination correlated nicely in our study with anti-S serum level, thus supporting the validity of COVID-19 vaccination reporting. Recall of SARS-CoV-2 test results and reporting COVID-19 core symptoms were also shown to be highly valid [29,30]. Our study has several strengths. Primarily, the longitudinal study design that enabled the establishment of the temporal associations between baseline characteristics and subsequent reinfections. The long-term follow-up allowed the capture of both the Delta and Omicron waves, thus enhancing the knowledge regarding the role of hybrid immunity in the heterologous protection against emergent variants of concerns. Our cohort comprised a homogeneous population of COVID-19-recovered CCP donors during the first year of the pandemic, with comparable testing-seeking behaviors. We systematically tackled factors that might affect the risk of reinfection in this cohort by combining of serological measurements together with clinical and epidemiological data, thus providing in-depth analysis of the role of vaccination and pre-existing immunity in the prevention of reinfections. Because all participants had their primary infection during the first year of the pandemic, we could assess the net effect of pre-existing immunity to the Wuhan strain and Alpha variant. Lastly, most participants were vaccinated with BNT162b2 vaccine, thus mimicking the current situation, where most people were either exposed to natural SARS-CoV-2 infection COVID-19 vaccination or both, which broaden the generalizability of our findings.
In conclusion, reinfection with emerging variants of concern occurred among COVID-19-recovered individuals, with substantially higher incidence of Omicron reinfections than Delta reinfections. Subsequent vaccination with the BNT162b2 vaccine and high anti-N levels at primary infection provided significant protection against these reinfections and induced higher anti-S binding antibodies at follow-up. Pre-existing anti-S binding antibodies and neutralizing antibody levels against the Wuhan strain and Alpha variants were inversely associated with the risk of Omicron reinfections. These findings are of broad public health importance and contribute to shaping the COVID-19 vaccination policy.
Declarations of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgments
Funding
The authors are grateful to SodaStream International Ltd and PepsiCo for the donation that supported the study in part. SodaStream and PepsiCo did not have any role in the study design, data collection and analysis, interpretation of the study findings, writing, or submitting the manuscript.
Ethical approval
The study protocol was approved by the ethics committees of the Wolfson Medical Center (no. 0074-WOMC) and Tel Aviv University (no. 0003409-1). Participants gave verbal documented consent before being interviewed by phone and those who provided blood samples signed written informed consent form.
Acknowledgments
The authors are thankful to all the volunteers who participated in the follow-up study and to the MDA personnel that assisted in the logistics of the study.
Author contribution
Study design: Dani Cohen, Khitam Muhsen, Marina Izak, Oren Zimhony, Eilat Shinar, Yasmin Maor; Data collection: Marina Izak, Evgeniy Stoyanov; Saritte Perlman, Yonatan Amir. Laboratory tests: Anya Bialik, Limor Kliker, Nofar Atari, Ruti Yshai, Yona Zaide, Michal Mandelboim; Data analysis: Sophy Goren, Dani Cohen, Khitam Muhsen; Interpretation of the findings: Dani Cohen, Khitam Muhsen, Marina Izak, Oren Zimhony, Eilat Shinar, Yasmin Maor, Hadar Marcus, Noa Madar-Balakirski, Tomer Israely, Nir Paran; Writing: Dani Cohen, Khitam Muhsen; Reviewing and critical editing: all authors.
Footnotes
Supplementary material associated with this article can be found, in the online version, at doi:10.1016/j.ijid.2023.04.395.
Appendix. Supplementary materials
{kind=link}
{kind=link}
References
- 1.Our World in Data. SARS-CoV-2 variants in analyzed sequences, Israel, https://ourworldindata.org/grapher/covid-variants-area?country=~ISR; 2022 [accessed 25 October 2022].
- 2.Muhsen K, Cohen D. COVID-19 vaccination in Israel. Clin Microbiol Infect. 2021;27:1570–1574. doi: 10.1016/j.cmi.2021.07.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Dagan N, Barda N, Kepten E, Miron O, Perchik S, Katz MA, et al. BNT162b2 mRNA Covid-19 vaccine in a nationwide mass vaccination setting. N Engl J Med. 2021;384:1412–1423. doi: 10.1056/NEJMoa2101765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chodick G, Tene L, Rotem RS, Patalon T, Gazit S, Ben-Tov A, et al. The effectiveness of the two-dose BNT162b2 vaccine: analysis of real-world data. Clin Infect Dis. 2022;74:472–478. doi: 10.1093/cid/ciab438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Haas EJ, Angulo FJ, McLaughlin JM, Anis E, Singer SR, Khan F, et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: an observational study using national surveillance data. Lancet. 2021;397:1819–1829. doi: 10.1016/S0140-6736(21)00947-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bar-On YM, Goldberg Y, Mandel M, Bodenheimer O, Freedman L, Alroy-Preis S, et al. Protection against Covid-19 by BNT162b2 booster across age groups. N Engl J Med. 2021;385:2421–2430. doi: 10.1056/NEJMoa2115926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bar-On YM, Goldberg Y, Mandel M, Bodenheimer O, Amir O, Freedman L, et al. Protection by a fourth dose of BNT162b2 against Omicron in Israel. N Engl J Med. 2022;386:1712–1720. doi: 10.1056/NEJMoa2201570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Muhsen K, Maimon N, Mizrahi AY, Boltyansky B, Bodenheimer O, Diamant ZH, et al. Association of receipt of the fourth BNT162b2 dose with Omicron infection and COVID-19 hospitalizations among residents of long-term care facilities. JAMA Intern Med. 2022;182:859–867. doi: 10.1001/jamainternmed.2022.2658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Magen O, Waxman JG, Makov-Assif M, Vered R, Dicker D, Hernán MA, et al. Fourth dose of BNT162b2 mRNA Covid-19 vaccine in a nationwide setting. N Engl J Med. 2022;386:1603–1614. doi: 10.1056/NEJMoa2201688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Altarawneh HN, Chemaitelly H, Ayoub HH, Tang P, Hasan MR, Yassine HM, et al. Effects of previous infection and vaccination on symptomatic Omicron infections. N Engl J Med. 2022;387:21–34. doi: 10.1056/NEJMoa2203965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gazit S, Shlezinger R, Perez G, Lotan R, Peretz A, Ben-Tov A, et al. The incidence of SARS-CoV-2 reinfection in persons with naturally acquired immunity with and without subsequent receipt of a single dose of BNT162b2 vaccine: a retrospective cohort study. Ann Intern Med. 2022;175:674–681. doi: 10.7326/M21-4130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gazit S, Shlezinger R, Perez G, Lotan R, Peretz A, Ben-Tov A, et al. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) naturally acquired immunity versus vaccine-induced immunity, reinfections versus breakthrough infections: a retrospective cohort study. Clin Infect Dis. 2022;75:e545–e551. doi: 10.1093/cid/ciac262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Nordström P, Ballin M, Nordström A. Risk of SARS-CoV-2 reinfection and COVID-19 hospitalisation in individuals with natural and hybrid immunity: a retrospective, total population cohort study in Sweden. Lancet Infect Dis. 2022;22:781–790. doi: 10.1016/S1473-3099(22)00143-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Goldberg Y, Mandel M, Bar-On YM, Bodenheimer O, Freedman LS, Ash N, et al. Protection and waning of natural and hybrid immunity to SARS-CoV-2. N Engl J Med. 2022;386:2201–2212. doi: 10.1056/NEJMoa2118946. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chemaitelly H, Nagelkerke N, Ayoub HH, Coyle P, Tang P, Yassine HM, et al. Duration of immune protection of SARS-CoV-2 natural infection against reinfection. J Travel Med. 2022;29:taac109. doi: 10.1093/jtm/taac109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Izak M, Gendelman V, Bransburg-Zabary S, Stoyanov E, Gat R, Cohen D, et al. Qualifying coronavirus disease 2019 convalescent plasma donors in Israel. Vox Sang. 2022;117:185–192. doi: 10.1111/vox.13162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Manalac J, Yee J, Calayag K, Nguyen L, Patel PM, Zhou D, et al. Evaluation of Abbott anti-SARS-CoV-2 CMIA IgG and Euroimmun ELISA IgG/IgA assays in a clinical lab. Clin Chim Acta. 2020;510:687–690. doi: 10.1016/j.cca.2020.09.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Nemet I, Kliker L, Lustig Y, Zuckerman N, Erster O, Cohen C, et al. Third BNT162b2 vaccination neutralization of SARS-CoV-2 Omicron infection. N Engl J Med. 2022;386:492–494. doi: 10.1056/NEJMc2119358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.NIBSC. WHO International Standard First WHO International Standard for Anti-SARS-CoV-2 Immunoglobulin (Human) NIBSC Code. Available from First WHO International Standard for anti-SARS-CoV-2 immunoglobulin (human), nibsc.org; 2020 [accessed 29 December 2022].
- 20.Saker K, Escuret V, Pitiot V, Massardier-Pilonchéry A, Paul S, Mokdad B, et al. Evaluation of commercial anti-SARS-CoV-2 antibody assays and comparison of standardized titers in vaccinated health care workers. J Clin Microbiol. 2022;60 doi: 10.1128/JCM.01746-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Liu L, Iketani S, Guo Y, Chan JF, Wang M, Liu L, et al. Striking antibody evasion manifested by the Omicron variant of SARS-CoV-2. Nature. 2022;602:676–681. doi: 10.1038/s41586-021-04388-0. [DOI] [PubMed] [Google Scholar]
- 22.Le TTB, Vasanthakumaran T, Thi Hien HN, Hung IC, Luu MN, Khan ZA, et al. SARS-CoV-2 Omicron and its current known unknowns: a narrative review. Rev Med Virol. 2023;33:e2398. doi: 10.1002/rmv.2398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Patalon T, Saciuk Y, Peretz A, Perez G, Lurie Y, Maor Y, et al. Waning effectiveness of the third dose of the BNT162b2 mRNA COVID-19 vaccine. Nat Commun. 2022;13:3203. doi: 10.1038/s41467-022-30884-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Pallett SJ, Jones R, Abdulaal A, Pallett MA, Rayment M, Patel A, et al. Variability in detection of SARS-CoV-2-specific antibody responses following mild infection: a prospective multicentre cross-sectional study, London, United Kingdom, 17 April to 17 July 2020. Euro Surveill. 2022;27 doi: 10.2807/1560-7917.ES.2022.27.4.2002076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Almendro-Vázquez P, Chivite-Lacaba M, Utrero-Rico A, González-Cuadrado C, Laguna-Goya R, Moreno-Batanero M, et al. Cellular and humoral immune responses and breakthrough infections after three SARS-CoV-2 mRNA vaccine doses. Front Immunol. 2022;13 doi: 10.3389/fimmu.2022.981350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sette A, Crotty S. Immunological memory to SARS-CoV-2 infection and COVID-19 vaccines. Immunol Rev. 2022;310:27–46. doi: 10.1111/imr.13089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Tauzin A, Gong SY, Chatterjee D, Ding S, Painter MM, Goel RR, et al. A boost with SARS-CoV-2 BNT162b2 mRNA vaccine elicits strong humoral responses independently of the interval between the first two doses. Cell Rep. 2022;41 doi: 10.1016/j.celrep.2022.111554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Zar HJ, MacGinty R, Workman L, Botha M, Johnson M, Hunt A, et al. Natural and hybrid immunity following four COVID-19 waves: a prospective cohort study of mothers in South Africa. EClinicalmedicine. 2022;53 doi: 10.1016/j.eclinm.2022.101655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.McCarthy K, Maru S, Nowlin S, Ram P, Glazer KB, Janevic T. The validity of self-reported SARS-CoV-2 results among postpartum respondents. Paediatr Perinat Epidemiol. 2022;36:518–524. doi: 10.1111/ppe.12874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Adorni F, Prinelli F, Bianchi F, Giacomelli A, Pagani G, Bernacchia D, et al. Self-reported symptoms of SARS-CoV-2 infection in a nonhospitalized population in Italy: cross-sectional study of the EPICOVID19 web-based survey. JMIR Public Health Surveill. 2020;6:e21866. doi: 10.2196/21866. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.