

Abstract
One Health is a collaborative approach that requires synergies between human, animal and environmental health sectors, other key sectors, and partners supporting these capacity‐building efforts. Multiple One Health capacity‐building tools are available that can be used independently or together. Two tools that have been used in sequence to inform each other include the US Centers for Disease Control and Prevention's One Health Zoonotic Disease Prioritization (OHZDP) Process and University of Minnesota/US Department of Agriculture's One Health Systems Mapping and Analysis Resource Toolkit™ (OH‐SMART). In August 2017, a workshop was held in Islamabad, Pakistan, that integrated these two tools for the first time. In this integrated workshop, we used the OHZDP to develop a list of priority zoonotic diseases for Pakistan and OH‐SMART™ to conduct a partner assessment and disease‐specific gap analysis. Both tools were used to identify areas for One Health collaboration for the priority zoonotic diseases. Additionally, we trained 11 in‐country facilitators representing the human and animal health sectors on both tools. This manuscript describes the integration of these two tools—using the Pakistan workshop as a process case study—to inform future efforts to implement One Health tools synergistically. Implementation of the technical and logistical aspects of the integrated workshop was detailed: (1) workshop preparation, (2) facilitator training, (3) workshop implementation and (4) workshop outcomes. Sixteen months after the workshop, we conducted an in‐country facilitator survey to follow‐up on the utility of both tools and the training for facilitators. We evaluated facilitator survey results using a qualitative analysis software atlas.ti. Using the OHZDP Process and OH‐SMART™ together achieved continuity between the two processes and provided a professional development opportunity for in‐country facilitators. Based on the success of this integrated workshop, partners developing and implementing One Health tools should recognize the importance of collaboration to maximize outcomes.
Keywords: One Health, operational tools, prioritization, systems mapping, zoonoses
Impacts.
The OHZDP Process and OH‐SMART™ are two One Health tools that have been implemented independently to inform capacity‐building efforts; integrating the implementation of these tools can maximize time, resources and outcomes.
Using the OHZDP Process and OH‐SMART™ together achieved continuity between the two processes by identifying priority zoonotic diseases using a multisectoral, evidence‐based and repeatable process and by allowing for a more in‐depth assessment to identify existing gaps and action steps for each of the prioritized zoonotic diseases.
The integrated OHZDP Process and OH‐SMART™ facilitator training provided a professional development opportunity for in‐country facilitators and enhanced capacity and knowledge for future One Health activities.
1. INTRODUCTION
A One Health approach for the prevention and control of zoonotic diseases requires collaboration among multidisciplinary partners from the various health sectors (human, animal, environment, etc.) as well as synergies between other key sectors and partners supporting these country capacity‐building efforts. Multiple tools are available for countries to use to strengthen One Health capacity at the national level (Burkle, 2015; Machalaba et al., 2018; Operationalizing One Health, 2017; Pelican et al., 2019; WHO‐OIE Operational Framework, 2021). Many of these can be used independently or together to maximize efforts towards strengthening zoonotic disease prevention and control, and strengthening One Health coordination between sectors (Pelican et al., 2019). Additionally, aligning the workshop goals with pre‐existing plans maximizes time and improves overall outcomes to enhance One Health capacity. Too often, however, the outcomes of these tools may not be aligned and opportunities to maximize time and resources can be missed. Two tools that have been used in sequence to inform each other include the US Centers for Disease Control and Prevention's (CDC) One Health Zoonotic Disease Prioritization (OHZDP) Process (CDC, One Health Zoonotic Disease Prioritization, 2021; Rist et al., 2014) and the One Health Systems Mapping and Analysis Resource Toolkit™ (OH‐SMART; Pelican et al., 2019; Vesterinen et al., 2019).
Centers for Disease Control and Prevention's One Health Office developed the OHZDP Process to assist countries using a One Health approach to prioritize zoonotic diseases of greatest concern and develop next steps and action plans for these priorities. To date, the OHZDP Process has been conducted in 37 locations at the regional, national and subnational level to help focus One Health activities around zoonotic disease prevention and control (CDC, Completed OHZDP Workshops, 2021). Outcomes from the OHZDP Process have been integrated into WHO Joint External Evaluations and National Action Plans for Health Security conducted to meet International Health Regulation (IHR) capacities (WHO, Strengthening the IHR Through a One Health Approach, 2022; WHO‐OIE Operational Framework, 2021). OHZDP outcomes have also informed One Health systems development, and zoonotic disease‐specific efforts globally such as IHR‐PVS Bridging Workshops, the World Organization for Animal Health (OIE) Performance of Veterinary Services (PVS) Pathway and the FAO Surveillance Evaluation Tool (CDC, One Health Zoonotic Disease Prioritization, & One Health Systems Mapping and Analysis Resource Toolkit™, 2017; Pelican et al., 2019; Salyer et al., 2017). The OHZDP Process may be repeated approximately every 5 years to reassess zoonotic disease priorities and progress for enhanced One Health capacity.
OH‐SMART™ co‐developed by the University of Minnesota (UMN) and the US Department of Agriculture (USDA) was created to map multisectoral coordination and collaboration and then develop specific action plans to improve One Health systems. To date, OH‐SMART™ has been used successfully in 18 countries. The OH‐SMART™ systems mapping process first identifies key partners involved in the One Health challenge being analysed. These partners then analyse the existing One Health system for gaps in multisectoral coordination and communication. OH‐SMART™ is flexible and has been applied to strengthen One Health systems needing improvement to address One Health issues such as zoonotic diseases including surveillance, laboratory capacity, outbreak response and workforce development (Errecaborde et al., 2017; Vesterinen et al., 2019).
While these two One Health tools have been implemented to inform capacity‐building efforts in 10 overlapping countries (Pelican et al., 2019); the workshops were conducted in sequence and independently; therefore, an opportunity to combine workshops exists to streamline efforts for planning and implementation while still providing the intended outcomes (Pelican et al., 2019). In 2017, this opportunity arose when the government of Pakistan requested that both the OHZDP Process and OH‐SMART™ be implemented in Pakistan to help identify priority zoonotic diseases and identify areas to strengthen their One Health capacity to prevent, detect and respond to these diseases. Given this request, CDC, UMN and USDA collaborated to plan and implement an integrated workshop instead of two stand‐alone workshops, combining both One Health tools during the same workshop for the first time. The goal of this integrated workshop was to use both well‐established One Health tools to identify a list of priority zoonotic diseases and next steps to address those disease through One Health collaboration in Pakistan, while piloting the concept that there is a benefit to integrating One Health tools and a logical progression in implementing the OHZDP Process and OH‐SMART™ together.
This manuscript describes the integration of these two One Health tools, using the Pakistan integrated workshop as a process case study to inform future efforts to implement One Health tools synergistically. This process case study focuses on the technical and logistical aspects of conducting the workshop. Detailed information on the workshop outcomes can be found in the workshop report, One Health Zoonotic Disease Prioritization and One Health Systems Mapping and Analysis Resource Toolkit for Multisectoral Engagement in Pakistan.
2. MATERIALS AND METHODS
2.1. Contributing tools
The OHZDP Process brings together representatives from human, animal and environmental health sectors, as well as other relevant partners, to prioritize zoonotic diseases using a mixed methods approach (CDC, One Health Zoonotic Disease Prioritization, 2021; Rist et al., 2014). The OHZDP Process is typically implemented in a workshop style format with steps conducted before, during, and after the workshop. Before the OHZDP workshop, a core planning team with representatives from key sectors is identified to conduct all logistical and technical components of the preparation steps. Three groups of participants are identified by the core planning team: (1) in‐country facilitators, (2) voting members from the government sectors actively involved in zoonotic disease prevention and control (with equal representation from each) and (3) advisors representing other key sectors and partners who provide advice and expertise to voting members and support post‐workshop collaborative activities. Workshop components and participants are detailed in Table 1. During the OHZDP workshop, participants finalize the list of zoonotic diseases for prioritization, develop criteria and questions, rank criteria, prioritize zoonotic diseases and discuss next steps and action plans for multisectoral, One Health engagement. After the OHZDP workshop, a final report approved by all partners is produced, and partners advocate for and implement the recommended next steps and action plans for the priority zoonotic diseases (CDC, Completed OHZDP Workshops, 2021).
TABLE 1.
Comparison of workshop implementation elements detailed and evaluated across the individual (OHZDP and OH‐SMART™) and the integrated One Health workshop: (1) workshop preparation, (2) facilitator training, (3) workshop implementation and (4) workshop outcomes.
| Tool elements | OHZDP a | OH‐SMART™ b | Integrated OHZDP/OH‐SMART™ in Pakistan |
|---|---|---|---|
| Elements of workshop preparation | |||
| Duration of workshop preparation | Approximately 3 months | 1–2 months | >3 months |
| Number of master facilitators identified | Minimum of three experienced master facilitators | Three master facilitators | Six master facilitators identified; four facilitators implemented the integrated workshop with one cross‐trained on both tools |
| Number of in‐country facilitators | 3–5 | 10–15 | 11 |
| Identification and criteria for in‐country facilitator selection |
|
|
11 local facilitators trained who were Field Epidemiology and Lab Training Program fellows and alumni (5 from the animal health sector, 6 from the human health sector). For details see OHZDP Workshop Report and Table 2 |
| Identification and criteria for participant selection |
Voting members: Represent government human health, animal health and environment sectors; in a technical leadership role with the ability to make decisions; ability to finalize and approve the priority zoonotic disease list and next step discussions; willing to carry the results of the OHZDP workshop forward. Advisors or observers: Key partners who represent organizations that are active in zoonotic disease work. The government recommends the appropriate advisors for the workshop and they may include non‐governmental partners |
OH‐SMART™ is flexible and adaptable to including participants from various sectors or other partners depending on the goal of the workshop and the system to be addressed | Participants included 27 Voting Members and 18 Advisors. For details see OHZDP Workshop Report and Table 2 |
| Literature review | A country‐specific, regional, and global literature review is conducted for the zoonoses on the initial zoonotic disease list. These reviews are extensive and typically cover approximately 40 zoonotic diseases | May include a synthesis of existing national‐level workforce assessments, strategies and reports | 221 articles were collected and reviewed according to typical OHZDP literature review process |
| Logistics requirements | The CDC One Health Office, US Government agencies, national government partners, funding partners, and other relevant partners may be part of a core planning team that work to prepare for the workshop and arrange logistics | Local team members work with OH‐SMART™ team to arrange logistics based on budget available | CDC One Health Office, in‐country CDC staff, US Government Agencies, Pakistan government partners, OH‐SMART™ facilitators worked with in‐country partner for the preparation of the workshop and to coordinate logistics |
| Elements of facilitator training | |||
| Duration | 2 days | 2 days | 3 days |
| Number trained | 3–5 | 10–15 | 11 |
| Lectures in technical components | OHZDP Master Facilitators train local facilitators on each step of the OHZDP Process on training through interactive exercises | Review of One Health and role in addressing complex problems. Depends on needs/desires of host organization. | Trainees received interactive training on each step of the OHZDP and OH‐SMART™ processes including the technical components of the OHZDP analytical hierarchy process for decision‐making |
| Facilitation and presentation skills | Trainees are required to undergo a mock simulation exercise to practice presentation and facilitation skills, covering all steps of the OHZDP Process during training Day 2. Trainees further lead or co‐lead the actual workshop with assistance from the OHZDP Master Facilitators, where needed | Shared leadership skills to include self‐awareness, active listening, and facilitation. | Training materials were integrated so that the shared leadership development exercises were incorporated into the OHZDP portion of the training. The trainees completed a mock simulation exercise during the training and co‐lead both the OHZDP and OH‐SMART™ components of the actual workshop |
| Elements of workshop implementation | |||
| Duration | 2 days | 2 days | 4 days |
| Number of participants | 12 voting members and 15–20 advisors | OH‐SMART™ is flexible and adaptable to include the number of participants as needed depending on the goal of the workshop |
70 total participants including voting members, advisors, facilitators, and others who attended the workshop as an observer or gave remarks. 27 voting members were grouped by sector at the federal level and by province for 11 voting groups for the OHZDP portion of the workshop while 18 people participated as observers; All participants developed the disease‐specific maps as part of the OH‐SMART process |
| Workshop steps |
Before the workshop:
During the workshop:
After the workshop:
|
Shared leadership skills development
|
Before the workshop:
During the workshop:
After the workshop:
|
| Partner identification | Before the Workshop: Partners are identified prior to the inception of the workshop | Step 1 of the OH‐SMART™: Workshop participants identify partner networks for identified zoonotic disease of interest | Government partners active on One Health priorities for zoonotic disease prevention and control in Pakistan were identified prior to the integrated workshop and invited to participate. During the OH‐SMART™ portion of the workshop, participants discussed additional relevant partners |
| Partner engagement | During the OHZDP Workshop: A mixed methods prioritization process is used to engage partners collaboratively to develop criteria and questions, rank criteria, and score questions to develop a ranked zoonotic disease list | Step 2 of the OH‐SMART™: Partners are interviewed to understand the system being examined, current state of One Health collaboration within their country and to determine additional partners that need to be included |
The OHZDP mixed method prioritization was used to engage partners during the OHZDP portion of the workshop. Partner interviews were conducted during step 2 of the OH‐SMART™ portion of the workshop with the focus on the prioritized zoonotic diseases |
| Prioritization | During the OHZDP Workshop: Quantitative methods are used to develop a ranked zoonotic disease list using decision tree analysis. Voting members are then presented with the ranked list and a qualitative, facilitated discussion occurs for the final priority zoonotic disease list | N/A | The OHZDP process for prioritization was used |
| Process mapping | N/A | Step 3 of the OH‐SMART™: The goals of this process are to map the current status of collaboration between sectors for One Health challenges | OHZDP outcomes informed step 3 of the OH‐SMART process which was used to visualize existing systems for flow of information, decisions, or actions taken between identified partners during an outbreak scenario |
| Analysis | During the OHZDP Workshop: A ranked list is presented to partners which is discussed, validated, and approved. Then a next steps discussion is held to identify areas for multisectoral, One Health collaboration around collaboration, surveillance, laboratory, outbreak response, preparedness, workforce, and other areas | Step 4–5 of the OH‐SMART™: Maps are analysed to identify opportunities for system improvement through partner discussion groups | The OHZDP process for validating and approving a rank list of prioritized zoonotic diseases was used. steps 4–5 of OH‐SMART™ were used to analyse system maps and identify opportunities for action planning |
| Action planning | During the OHZDP Workshop: Discussion based—partners identify specific next steps to address identified gaps and improve multisectoral, One Health collaboration for the priority zoonotic diseases | Step 6 of the OH‐SMART™: Partners identify specific next steps to address identified gaps and improve multisectoral, One Health collaboration | An action plan was developed in line with step 6 of OH‐SMART™ and as would be completed through a discussion at the end of an OHZDP workshop. This included general next steps around multisectoral collaboration, laboratory capacity, surveillance, outbreak response, and workforce. Then specific next steps for each represented sector were also agreed upon |
| Elements of workshop outcomes | |||
|
|
All of the OHZDP and OH‐SMART outcomes plus a final workshop report that includes specific country action plans for improving the prioritized zoonotic disease challenge mapped and analysed. | |
One Health Zoonotic Disease Prioritization (OHZDP).
One Health Systems Mapping and Analysis Resource Toolkit (OH‐SMART™).
OH‐SMART™ involves a six‐step process that facilitates multiple sectors to analyse their multisectoral coordination and collaboration, identify gaps and agree upon action steps to address the gaps in a detailed action plan (Vesterinen et al., 2019). The six OH‐SMART™ steps include (1) partner identification, (2) focus group interviews, (3) multisectoral systems mapping, (4) system analysis, (5) identification of opportunities for improvement and (6) action plan development.
Both the OHZDP Process and OH‐SMART™ are designed to be supported and delivered by local facilitators, trained through a pre‐workshop facilitator training. The local facilitators for both tools are selected based on similar criteria including having a technical role in human, animal or environmental health or familiarity with the concept of One Health (see Table 1 for facilitator criteria details). For the OHZDP Process, this involves a 2‐day training where government One Health sector trainees are taught the OHZDP Process, given an opportunity to conduct a simulation of the workshop and then co‐facilitate the actual workshop while being supported and mentored by the master facilitation team. For OH‐SMART™, this training is delivered in a 1‐ to 2‐day workshop to introduce the tool and practice the processes. OH‐SMART™ facilitator training also includes exercises in shared leadership and communication to build trainee facilitation skills.
Detailed methods for these tools have been previously described (CDC, One Health Zoonotic Disease Prioritization, 2021; Errecaborde et al., 2017; Rist et al., 2014; Vesterinen et al., 2019).
2.2. Comparison and integration of workshop elements
To describe the technical and logistical aspects of this process, we detailed and compared the following workshop implementation elements between Pakistan's integrated workshop and what would typically occur in a stand‐alone OHZDP and OH‐SMART™ workshop: (1) workshop preparation, (2) facilitator training, (3) workshop implementation and (4) workshop outcomes (Table 1).
2.3. Facilitator survey
We deployed a facilitator survey 16 months following the workshop to all 11 trained in‐country facilitators. This survey aimed to determine: (1) how and the frequency the two tools were used following the workshop; (2) the facilitator's knowledge and practice of One Health in their country following the workshop; (3) the facilitator's understanding and engagement of the multiple relevant sectors following the workshop; and (4) if the workshop expanded or enriched the facilitator's One Health network in the short and long term. The quantitative and qualitative questions were taken from a previously developed OH‐SMART™ facilitator survey (Sarode, 2018), which was modified to cover elements of the OHZDP Process and the integrated workshop. Survey timing allowed an assessment of long‐term impact of the training and time to conduct some of the follow‐up activities around the prioritized zoonotic diseases identified during the integrated workshop. There was no baseline data collected for survey domains 2 through 4.
We summarized data from these surveys using atlas.ti qualitative analysis software (Atlas.ti Scientific Software Development Product GmbH version 7.0.82.0). We used an inductive content analysis approach that employed a descriptive first cycle coding and a thematic analysis for the second cycle coding (Hsieh & Shannon, 2005; Qualitative Data Analysis, 2019). Code frequencies and co‐occurrence of emerging themes were used to provide context to the analysis (Ryan & Bernard, 2003). The intensity of the co‐occurrence between two codes (c‐coefficient) was calculated using the Co‐Occurrence Atlas.ti function. The c‐coefficient is a number between 0 and 1 and, like a correlation coefficient, shows the strength of association between two codes. The Atlas.ti Code Co‐occurrence matrix tool was used to identify co‐occurrence and sequence patterns from a list of codes generated from the responses.
3. RESULTS
3.1. Integrated workshop implementation and evaluation of workshop elements
Successful workshop implementation required close collaboration among CDC, UMN, USDA and in‐country partners in all phases of preparation, delivery and follow‐up activities. The OHZDP Process took place first to develop a priority zoonotic disease list that would inform the mapping, analysis, and action planning components of the OH‐SMART™ application. The integrated workshop was conducted in two phases; a 3‐day facilitator training led by OHZDP Process and OH‐SMART™ master facilitators, followed by a 4‐day workshop supported by both the newly trained local facilitators and master facilitators (Figure 1). Both phases integrated OHZDP Process and OH‐SMART™ methods (Table 1).
FIGURE 1.
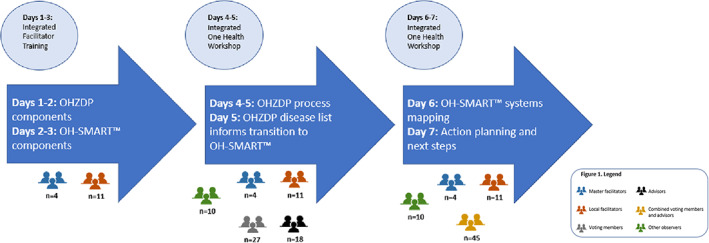
Timeline of events for integrated One Health Zoonotic Disease Prioritization (OHZDP) and One Health Systems Mapping and Analysis Resource Toolkit™ (OH‐SMART™) facilitator training and workshop, August 19–25th, 2017 Islamabad, Pakistan.
3.1.1. Workshop preparation
We initiated workshop planning in early 2017 starting with the selection of a core planning team to support the technical and logistical preparations. The core planning team consisted of 17 experienced organizers from CDC (4), UMN (5) and USDA (4), in‐country staff from CDC (3) and USDA (1), and the implementing partner, CABI. It took approximately 3 months to combine training and workshop materials.
Timing
A typical stand‐alone OHZDP Process or OH‐SMART™ workshop is 4 days, including 2 days of in‐country facilitator training and 2 days for each workshop. For the Pakistan‐integrated workshop, we dedicated 3 days to facilitator training and allotted 4 days for the workshop for a total of 7 days (Figure 1), 1 day less than would typically be expected for each workshop alone. The core planning team modified the combined workshop agenda to account for this. The core planning team also developed an integrated master slide deck to optimize workshop and facilitator training content and streamline transitions between the two One Health tools.
Participant selection
The selection of facilitators and participants for the integrated workshop was the same composition as a typical OHZDP workshop (One Health Zoonotic Disease Prioritization, 2021). The national government of Pakistan invited participants representing the human health, animal health and environment/wildlife health sectors, and other identified partners. However, the number of participants required for an OHZDP workshop and a OH‐SMART™ does vary. Typically, an OHZDP workshop has up to 12 voting members and 15–20 advisors (Table 1; CDC, One Health Zoonotic Disease Prioritization, 2021). To conduct a thorough partner mapping analysis for the OH‐SMART™ portion of the workshop, UMN/USDA requested an increased number of workshop participants and facilitators. Therefore, the Pakistan‐integrated workshop included 27 voting members and 18 advisors for a total of 45 participants. For a typical OHZDP workshop, we train only three to six in‐country facilitators (CDC, One Health Zoonotic Disease Prioritization, 2021). A typical OH‐SMART™ facilitator training includes 10–15 trainees. This ensures there is at least one facilitator available to work with each breakout group during each step of the process and sufficient diversity to capture the complexity of the One Health system. For this integrated workshop, we trained 11 in‐country facilitators on both the OHZDP Process and OH‐SMART™.
Literature review
As part of the preparatory phase, the core planning team reviewed over 221 articles using the same methodology for a typical OHZDP workshop (Table 1; CDC, One Health Zoonotic Disease Prioritization, 2021; Rist et al., 2014). The literature review was used during the OHZDP Process to score the initial list of 33 zoonotic diseases based on criteria and questions developed during the workshop.
Logistics
All logistics were managed as they typically would be for an OHZDP Process or OH‐SMART™ (Table 1).
3.1.2. Facilitator training
We trained 11 in‐country facilitators during the first 3 days of the workshop using an integrated version of the OHZDP Process and OH‐SMART™ facilitator trainings (Figure 1). The Pakistan national and provincial level governments selected trainees using criteria as described in Table 1. Typically, an OHZDP facilitator training is 2 full days, but the second day was condensed to allow for initial training on the OH‐SMART™.
The first day of the training agenda was structured similarly to a stand‐alone OHZDP facilitator training. Modifications included introducing both the OHZDP Process and OH‐SMART™ and adding elements of the OH‐SMART™ training, including facilitation skills and shared leadership to allow the facilitators to use those skills throughout. Other sections of the typical OHZDP facilitator training agenda for the first day were shortened in length of time to accommodate these additions (including developing the criteria, question development, ranking the criteria and scoring the zoonotic diseases), but the content remained the same.
The second day began with an exercise to simulate an OHZDP workshop with an abbreviated training on how to lead the next step discussion that would usually be included in the facilitator training for an OHZDP Process. This was replaced by a transition to OH‐SMART™, which would be used to conduct a gap analysis and to focus next steps planning to address identified gaps. The rest of the second day and the third day were dedicated to training on OH‐SMART™.
3.1.3. Workshop implementation
Following the facilitator training, the newly trained facilitator team supported by four master OHZDP and OH‐SMART™ facilitators together led a 4‐day integrated OHZDP and OH‐SMART™ workshop (Figure 1). For the integrated workshop, we divided 27 voting members into 11 voting groups representing the eight provincial departments of health, livestock and dairy development and the three national‐level ministries of agriculture, health, and environment. An additional 18 partners served as advisors to voting members and provided input during open discussion (Table 2).
TABLE 2.
Roles and represented organizations for the workshop participants
| Participant | Total number | Workshop participation | Organizations represented | Sectors represented (human health, animal health, environmental health) | Role |
|---|---|---|---|---|---|
| Local facilitator | 11 |
Facilitator training Integrated One Health Workshop |
NIH a Provincial HD b Provincial L&DD c Army Medical Core in Rawalpindi |
Human health Animal health |
Trained to implement both One Health tools Facilitated integrated workshop |
| Voting member | 27 | Participated throughout the Integrated One Health Workshop |
NIH Ministry of National Health Services, Regulations, and Coordination Ministry of Climate Change Ministry of National Food Security and Research NARC d Provincial HD Provincial L&DD |
Human health Animal health Environment |
Made decisions on priority zoonotic disease list and next steps |
| Advisors | 18 | Advised voting members during the OHZDP e Process portion and participated during the OH‐SMART™ f portion of the Integrated One Health Workshop |
Food and Agriculture Organization OIE g Public Health England WHO‐Pakistan CDC‐Pakistan US Department of Agriculture‐Pakistan US Agency for International Development US Department of State |
Human health Animal health Environment |
Provided subject matter expertise during open discussion |
| Master facilitator | 4 |
Facilitator Training Integrated One Health Workshop |
CDC University of Minnesota/Indonesian One Health University Network |
Public health Animal health |
Led facilitator training Facilitated integrated workshop |
| Other | 10 | Observed during the OHZDP Process portion and observed during the OH‐SMART™ portion of the Integrated One Health Workshop |
NIH Field Epidemiology Training Project‐ NARC Provincial HD Provincial L&DD |
Human health Animal health |
Observed workshop Provided opening and closing address |
Note: For a full list of participants, workshop organizers, and implementing partners with associated organizations see the One Health Zoonotic Disease Prioritization & One Health Systems Mapping and Analysis Resource Toolkit™ for multisectoral engagement in Pakistan report (CDC, 2017).
National Institute of Health (NIH).
Provincial Health Directorates (HD).
Provincial Livestock and Dairy Development (L&DD).
National Agricultural Research Center (NARC).
One Health Zoonotic Disease Prioritization (OHZDP).
One Health Systems Mapping and Analysis Resource Toolkit (OH‐SMART™).
World Organization for Animal Health (OIE).
An initial list of 33 zoonotic diseases were identified to go through the OHZDP Process. The voting members developed five criteria and questions, ranked the criteria for quantitative ranking of these 33 zoonotic diseases as per standard methods (CDC, One Health Zoonotic Disease Prioritization, & One Health Systems Mapping and Analysis Resource Toolkit™, 2017). The voting members discussed and voted on a final priority list of six zoonotic diseases: zoonotic influenza, brucellosis, salmonellosis, rabies, Crimean Congo Hemorrhagic Fever and anthrax (CDC, One Health Zoonotic Disease Prioritization, & One Health Systems Mapping and Analysis Resource Toolkit™, 2017).
The key step to integration of the two One Health tools occurred on Day 2 when the workshop transitioned from OHZDP to OH‐SMART™. In a typical OHZDP Workshop, the next step discussion occurs on Day 2, after the priority zoonotic disease list has been agreed upon. Typically, this discussion is driven by the facilitators through a series of questions starting with general plans and recommendations that leads to an agreed upon set of next steps for each sector and partner organizations. For this workshop, once the priority zoonotic diseases were agreed upon, we used the six steps of OH‐SMART™ to analyse existing One Health systems in Pakistan and to identify gaps and areas for improvement around the priority zoonotic diseases (Figure 1).
Voting members and advisors all participated equally in OH‐SMART™. The core planning team specified four groups by province and included both human and animal health representation. Participants were also assigned based on their area of expertise where relevant. The fifth group included human, animal and environmental health representatives from the ministry level (Table 2). Each group focused on evaluating the existing coordination, communication and collaboration within the outbreak response system for an assigned prioritized zoonotic disease. Initially, the ministry‐level group was split into two groups to cover two prioritized zoonotic diseases, influenza viruses and anthrax; however, in the final steps, the group elected to focus solely on zoonotic influenza viruses for the mapping exercise due to limited time.
3.1.4. Workshop outcomes
Outcomes included a finalized list of priority zoonotic diseases and areas identified for multisectoral, One Health engagement in developing prevention and control strategies around these zoonotic diseases (CDC, One Health Zoonotic Disease Prioritization, & One Health Systems Mapping and Analysis Resource Toolkit™, 2017). The OH‐SMART™ process included mapping the current and ideal state of the existing coordination, communication and collaboration within the outbreak response system for five of the six prioritized diseases. Workshop participants worked in five groups assigned to one of the six priority zoonotic diseases and mapped the process from identification of an outbreak through resulting response activities, noting gaps in multisectoral coordination and communication, existing surveillance systems, existing laboratory capacity to diagnose the disease in humans and animals, and any gaps. Participants discussed recommendations and further actions to address identified gaps. Recommendations included developing a national framework and strategic plan for One Health in Pakistan (CDC, One Health Zoonotic Disease Prioritization, & One Health Systems Mapping and Analysis Resource Toolkit™, 2017). More detail on these outcomes are in the final workshop report (CDC, One Health Zoonotic Disease Prioritization, & One Health Systems Mapping and Analysis Resource Toolkit™, 2017).
3.2. Facilitator survey results
Nine of the 11 trained facilitators participated in the follow‐up survey. Respondents represented both national and provincial level government institutions from both the human health (68%) and animal health sectors (32%) currently engaged in Technical, Senior Technical and Senior Management positions.
The results of the facilitator survey revealed thematic clustering around the understanding of and advocacy for One Health among the respondents as a result of the workshop (Tables 3 and 4). The co‐occurrence codes with the highest frequency were One Health, shared understanding, respondent perceived value of tools and skills gained, and partner diversity (Table 3).
TABLE 3.
Code Co‐occurrence showing intensity of association between codes
| One Health | Shared understanding | Tools and skills a | Partners | Shared leadership | Collaboration | Culture change | Shared vision | Tools application b | Tools training c | |
|---|---|---|---|---|---|---|---|---|---|---|
| One Health | 0.31 | 0.22 | 0.45 | 0.18 | 0.05 | 0.18 | 0.18 | 0.06 | 0.05 | |
| Shared understanding | 0.31 | 0.21 | 0.31 | 0.11 | 0.24 | 0.27 | 0.06 | 0.05 | ||
| Tools and skills a | O.22 | 0.21 | 0.29 | 0.22 | 0.05 | 0.07 | 0.07 | 0.33 | 0.16 | |
| Partners | 0.45 | 0.31 | 0.29 | 0.07 | 0.13 | 0.14 | ||||
| Shared leadership | 0.18 | 0.11 | 0.22 | 0.11 | 0.18 | 0.18 | 0.13 | |||
| Collaboration | 0.05 | 0.24 | 0.05 | 0.07 | 0.11 | 0.08 | 0.05 |
The codes with the highest intensity of association are bolded.
Respondent perceived value of the tools and skills acquired (focused on perception of internal and external tool validity by respondent).
Respondent application of OH‐ZDPT and OH‐SMART™ Toolkits within their institution or geographic jurisdictions (an account of where tools were implemented).
Respondent perceived practical, flexible and complimentary nature of tools (OH‐ZDPT/OH‐SMART™) and training (shared leadership and facilitation skills) and its ease of comprehension (focused on the training process).
TABLE 4.
Facilitator survey results.
| Description of item | N | Yes (%) | No (%) | Standard error (%) |
|---|---|---|---|---|
| Workshop helped you better understand One Health | 9 | 100 | 00 | 0.00 |
| Workshop changed your perception of other One Health organizations | 9 | 100 | 00 | 0.00 |
| Used tools from training | 9 | 90 | 10 | 9.00 |
| Used workshop outputs after workshop | 9 | 89 | 11 | 10.00 |
| Did the workshop help you professionally? | 9 | 89 | 11 | 10.00 |
| Formal or informal changes in your organization | 9 | 78 | 22 | 14.00 |
| Improved influence on interactions with sectors represented at the training | 9 | 78 | 22 | 14.00 |
| Used tools in your work | 9 | 67 | 33 | 16.00 |
| Improved influence on interactions with sectors not represented at the training | 9 | 56 | 44 | 16.00 |
| Used tools in additional training in Pakistan | 9 | 22 | 78 | 14.00 |
This thematic clustering aligned with the content analysis of respondent's feedback that revealed three major themes: perceived value of the training, implementation drivers and implementation barriers. Facilitator survey respondents identified learning to use and implement the OHZDP Process (100% of respondents) and the OH‐SMART™ tools (77% of respondents) as the most useful parts of the training (Table 4). Respondents described the tools as simple, practical, flexible and easy to apply towards translating One Health knowledge into action such as policy, training and national One Health strategic planning efforts. Sentiments shared by the trained facilitators in survey responses reveal this enthusiasm:
Different priority lists had been circulating around for some time but were unable to convince the majority of partners. This tool however was way more convincing and acceptable as it covered majority of areas significant for prioritization of zoonotic diseases. Its weighted scores for different factors allowed comparison of bacterial and viral pathogens without creating much hindrance.
The trained facilitators appreciated the access to a suite of flexible and practical tools that could be easily modified and applied towards multisectoral, One Health action planning at the institutional, regional and national level, as evidenced by these survey responses:
I have been constantly using it for different activities including stakeholder's interviews, action planning etc. although with minor modifications according to my own requirements.
I applied the same procedure and skills learnt during workshop to prioritize 5 new diseases to be included in DEWS Surveillance being conducted by my organization.
Great experience with great trainers…We need such workshops at the provincial level to increase the awareness about the One Health Approach.
The integrated workshops' emphasis on the development of flexible teams who understand their key roles in establishing a multisectoral course of action resonated well with the survey respondents. They attributed this to the practical nature of both tools and to shared leadership skills that emphasize action and responsibility by all partners regardless of disciplinary or hierarchical barriers. Respondents highlighted their ability to have an impact using available resources within their spheres of influence. Survey respondent comments summarize this sense of empowerment generated as a result of the training, such as:
I was able to convince my colleagues on [the] importance of effective disease surveillance and outbreak investigation and as a result was assigned disease surveillance related activities at my office…
After the workshop I am able to play my role as One Health moderator and support my government in doing synergistic efforts towards disease prioritization and planning on[in] controlling disease of local and national priorities.
Respondents identified drivers that facilitated the implementation of their newly acquired tools and training. These revolved around the process of disciplinary integration, development of a shared understanding of other partners' goals, systems and capacities, and identification of common ground that would allow shared action despite disparate mandates in the control of zoonotic diseases. Respondents were careful to remind us of the importance of ‐an enabling environment at various government levels and funding opportunities that can help operationalize One Health.
We have become more open to collaborative work, however that may not only be attributed to this sole workshop although it definitely played the part. Poultry research institute currently is running several collaborative projects with provincial and federal institutes.
The successes described were not without challenges. Respondents cited barriers that prevented implementation of workshop processes, such as challenges unique to the combined delivery of the two tools, challenges due to the lack of harmonized systems across departments. Respondents also cited challenges such as the limited time to cover all aspects of the training.
4. DISCUSSION
This integrated workshop supported Pakistan's One Health work by enabling representatives from the national and provincial ministries associated with human, animal and environmental health to prioritize zoonotic diseases of greatest concern using the OHZDP Process. This was followed by OH‐SMART™ to review and visualize the procedures and processes for existing coordination, communication and collaboration within the outbreak response system for each prioritized disease and to develop specific action plans to address identified gaps. Prioritizing zoonotic diseases allowed Pakistan to meet Joint External Evaluation and other global frameworks' (WHO, Joint External Evaluation of IHR Core Capacities of the Islamic Republic of Pakistan, 2017; WHO, Strengthening the IHR Through a One Health Approach, 2022; WOAH, IHR‐PVS National Bridging Workshop, 2017) recommendations for priority actions and provided a multisectoral forum to openly discuss the needs and challenges in controlling zoonotic diseases.
Several next steps were accomplished towards strengthening One Health in Pakistan as a result of this integrated workshop. Following the workshop in 2017, the Ministry of National Health Services Regulation and Coordination notified the prioritized zoonotic diseases as a national priority which resulted in the inclusion of these diseases in the national Infectious Disease Surveillance and Response (IDSR) system. This inclusion requires regular reporting of human cases of these diseases through routine surveillance. Several follow‐up activities were conducted around strengthening rabies and brucellosis prevention and control. This included a WHO‐supported joint risk assessment for rabies at the human–animal–environment interface supported in November 2017 and again in 2019. A follow‐up meeting was held in 2018 to conduct a Stepwise Approach to Rabies Elimination (SARE) and to pilot the Staged Tool for the Elimination of Brucellosis (STEB) using a One Health approach. Subsequently, the Food and Agriculture Organization of the United Nations (FAO) supported the development of a national action plan for rabies engaging the human and animal health sectors. At the provincial level, the Government of Punjab developed a canine population control policy using a capture, neuter, vaccinate and release method. One outcome of the STEB was the development of a 5‐year national brucellosis control strategic plan for 2018 through 2023. Additionally, the Global Health Development fund supported joint One Health brucellosis surveillance efforts. Finally, the Government of Pakistan drafted a One Health Strategic Plan for the national level that included goals and objectives to strengthen One Health efforts for the prioritized zoonotic diseases and One Health coordination to prevent antimicrobial resistance. Thus, the integrated workshop catalysed a series of actions and plan development within the following 2 years.
In addition to the positive outcomes and next steps that were accomplished towards strengthening One Health in Pakistan as a result of the workshop, the integration process taught us a lot about combining One Health tools. These lessons learned are useful for future activities because this workshop demonstrated a logical progression in implementing the OHZDP Process and OH‐SMART™ together (Pelican et al., 2019). In locations where a stand‐alone OH‐SMART™ is conducted before an OHZDP workshop, zoonotic diseases are selected by an information gathering and synthesis phase to identify outcomes of prior needs assessments conducted in the country (Pelican et al., 2019). In the case that a OH‐SMART™ is conducted after an OHZDP Process in the same location, the OHZDP workshop report is used to focus the OH‐SMART™ on the list of prioritized zoonotic diseases determined during the OHZDP. In this integrated workshop, the OHZDP Process added a multisectoral, evidence‐based and repeatable process for identifying the prioritized zoonotic diseases at the start of the OH‐SMART™. Integration allowed for a quicker progression from identification of the most pressing zoonotic diseases of greatest concern to identifying and agreeing to action steps to address existing gaps within a One Health system.
The additional workshop time allowed participants to examine information sharing processes between human, animal and environmental health sectors, the roles of each sector, and areas of strengths and weaknesses during an outbreak. This benefitted the next steps development, including the visualization of the systems around five of the six priority zoonotic diseases through mapping (CDC, One Health Zoonotic Disease Prioritization and One Health Systems Mapping and Analysis Resource Toolkit™, 2017), allowing participants to better understand the complexity of the priority zoonotic diseases, and the important contributions of various partners in addressing these challenges.
In addition to a professional development opportunity for in‐country facilitators and strengthened local capacity and knowledge on these One Health tools, the integration of the facilitator training helped identify areas that were lacking in the stand‐alone training materials. Leadership skill development aimed to enable new facilitators to be more confident and effective in leading both portions of the workshop. Facilitators felt empowered by the development of shared leadership skills because it emphasized action and responsibility by all partners regardless of disciplinary or hierarchical barriers. A future area of evaluation of the training may include understanding whether and how the integrated training affected facilitator readiness as compared to facilitators in countries that had separate, full‐length trainings.
Streamlined logistics were an additional benefit of the integrated workshop, saving participant and facilitator travel time and resources (Häsler et al., 2014). CDC and UMN facilitators were dually trained on the OH‐SMART™, resulting in fewer facilitators travelling to Pakistan to conduct both the OHZDP Process and OH‐SMART™. However, some logistical challenges arose due to the extended workshop. While the integrated workshop was shorter than two stand‐alone workshops, the facilitator training and combined workshop were 7 days for the facilitators and 4 days for voting members and advisors. Four to 7 days may be a long time to ask participants to be away from their regular duties, versus 2–4 days in a stand‐alone workshop. The amount of material that was covered with the integration of both tools for the facilitator training and the workshop was almost double as well. In spite of the extended time for a next steps discussion through use of the OH‐SMART™, there was not sufficient time for systems mapping of all six prioritized zoonotic diseases with the participants divided into five groups. In this case, the participants themselves decided to forgo mapping of one priority disease. While it is not required to conduct systems mapping for every priority disease, this could be an area of improvement for future integrated workshops—to divide participants into smaller groups to cover all diseases in the time allotted. Other improvements for future integrated workshops might include allowing more time for the facilitator training, managing the workshop schedule to avoid facilitator and participant fatigue, and further streamlining the materials to avoid redundancies. Considering whether a gap between workshops would be useful for participants to address key action items before coming together to make further plans may also impact the decision to hold an integrated workshop or not.
A challenge of integrating these two processes was that the standard number of participants varies between workshops. In a stand‐alone OHZDP workshop, there are about 35–40 people (including voting members, advisors, facilitators and others who may attend and observe the workshop) on average. The nature of OH‐SMART™ does not have a specific number of people required to participate. The combined Pakistan workshop had 45 voting members and advisors alone, which required additional modifications for the implementation. The OHZDP voting portion was modified to accommodate the increase in voting members and the decentralization of Pakistan's government structure to allow for provincial representation. One possible limitation of this arrangement was that multisectoral, regional and national voting groups may have led to the dilution of individual votes or perspectives.
The success of this integrated workshop towards meeting the shared goals of both the OHZDP and OH‐SMART™ and the Government of Pakistan illustrates that implementing One Health tools collaboratively can lead to successful outcomes for countries. The coordination of the OHZDP Process and OH‐SMART™ tools was formalized through the planning process; however, there is still a need for more systematic ways to collaborate when One Health tools are implemented (Pelican et al., 2019). Partners developing and implementing One Health tools should recognize the importance of collaboration to maximize outcomes by regularly communicating to share information such as implementation timelines, outcomes and lessons learned. Together one process can inform the next, and identify opportunities for synergy (Pelican et al., 2019). By working collaboratively, One Health partners can help countries select the most relevant tools for the greatest impact on One Health systems and capacity building.
CONFLICT OF INTERESTS
The authors declare that they have no competing interests.
ACKNOWLEDGEMENTS
This study was acknowledged by Pakistan ministries and provincial departments; integrated workshop facilitators such as Hina Ali, Ambreen Chaudhry, Saima Dil, Ibrar‐ul‐Hussain, Zakir Hussain, Jhangir Khan, Mumtaz Ali Khan, Muhammad Wasif Malik, Eisha Mansoor, Asif Sayed and M. Farooq Tahir; and implementing partners such as CABI, USDA Pakistan, US CDC‐Pakistan and US CDC One Health Office.
Varela, K. , Goryoka, G. , Suwandono, A. , Mahero, M. , Valeri, L. , Pelican, K. , & Salyer, S. J. (2023). One health zoonotic disease prioritization and systems mapping: An integration of two One Health tools. Zoonoses and Public Health, 70, 146–159. 10.1111/zph.13015
The views and opinions expressed in this article are those of the authors and are not necessarily the official views of US CDC or University of Minnesota.
DATA AVAILABILITY STATEMENT
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
REFERENCES
- Burkle, F. M. (2015). Global Health security demands a strong international health regulations treaty and leadership from a highly resourced World Health Organization. Disaster Medicine and Public Health Preparedness, 9(5), 568–580. 10.1017/dmp.2015.26 [DOI] [PubMed] [Google Scholar]
- CDC . (2021). Completed OHZDP workshops | one health . https://www.cdc.gov/onehealth/what‐we‐do/zoonotic‐disease‐prioritization/completed‐workshops.html
- CDC . (2021). One health zoonotic disease prioritization (OHZDP) | one health . https://www.cdc.gov/onehealth/what‐we‐do/zoonotic‐disease‐prioritization/index.html [DOI] [PMC free article] [PubMed]
- CDC . (2017). One Health zoonotic disease prioritization & one health systems mapping and analysis resource toolkit™ for multisectoral engagement in Pakistan .
- Errecaborde, K. M. , Pelican, K. M. , Kassenborg, H. , Prasarnphanich, O. O. , Valeri, L. , Yuuzar, E. , Fauzi, R. P. S. , Budayanti, N. S. , Suwandono, A. , Artama, W. T. , Adisasmito, W. , & Dutcher, T. (2017). Piloting the one health systems mapping and analysis resource toolkit in Indonesia. EcoHealth, 14(1), 178–181. 10.1007/s10393-017-1207-3 [DOI] [PubMed] [Google Scholar]
- Häsler, B. , Cornelsen, L. , Bennani, H. , & Rushton, J. (2014). A review of the metrics for one health benefits. Revue Scientifique et Technique, 33(2), 453–464. 10.20506/rst.33.2.2294 [DOI] [PubMed] [Google Scholar]
- Hsieh, H. F. , & Shannon, S. E. (2005). Three approaches to qualitative content analysis. Qualitative Health Research, 15(9), 1277–1288. 10.1177/1049732305276687 [DOI] [PubMed] [Google Scholar]
- Machalaba, C. C. , Salerno, R. H. , Barton Behravesh, C. , Benigno, S. , Berthe, F. C. J. , Chungong, S. , Duale, S. , Echalar, R. , Karesh, W. B. , Ormel, H. J. , Pelican, K. , Rahman, M. , Rasmuson, M. , Scribner, S. , Stratton, J. , Suryantoro, L. , & Wannous, C. (2018). Institutionalizing one health: From assessment to action. Health Security, 16(S1), S37–S43. 10.1089/hs.2018.0064 [DOI] [PubMed] [Google Scholar]
- Operationalizing One Health . (2017). One health tools in the context of Global Health security . https://www.abstractsonline.com/pp8/#!/4395/session/12
- Pelican, K. , Salyer, S. J. , Barton Behravesh, C. , Belot, G. , Carron, M. , Caya, F. , De La Rocque, S. , Errecaborde, K. M. , Lamielle, G. , Latronico, F. , Macy, K. W. , Mouille, B. , Mumford, E. , Shadomy, S. , Sinclair, J. R. , & Dutcher, T. (2019). Synergising tools for capacity assessment and one health operationalisation. Revue Scientifique et Technique (International Office of Epizootics), 38(1), 71–89. 10.20506/rst.38.1.2942 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Qualitative Data Analysis | SAGE Publications Inc . (2019). https://us.sagepub.com/en‐us/nam/qualitative‐data‐analysis/book246128
- Rist, C. L. , Arriola, C. S. , & Rubin, C. (2014). Prioritizing zoonoses: A proposed one health tool for collaborative decision‐making. PLoS One, 9(10), e109986. 10.1371/journal.pone.0109986 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ryan, G. W. , & Bernard, H. R. (2003). Techniques to identify themes. Field Methods, 15(1), 85–109. 10.1177/1525822X02239569 [DOI] [Google Scholar]
- Salyer, S. J. , Silver, R. , Simone, K. , & Behravesh, C. B. (2017). Prioritizing zoonoses for global health capacity building—Themes from one health zoonotic disease workshops in 7 countries, 2014–2016. Emerging Infectious Diseases, 23, S57–S64. 10.3201/eid2313.170418 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sarode, T. (2018). Domestic OH‐SMART(TM) activities, evaluation summary [unpublished report] .
- Vesterinen, H. M. , Dutcher, T. V. , Errecaborde, K. M. , Mahero, M. W. , Macy, K. W. , Prasarnphanich, O. O. , Kassenborg, H. , Yulizar, E. , Fauzi, R. P. , Budayanti, N. S. , Suwandono, A. , Artama, W. T. , Valeri, L. , & Pelican, K. M. (2019). Strengthening multi‐sectoral collaboration on critical health issues: One health systems mapping and analysis resource toolkit (OH‐SMART) for operationalizing one health. PLoS One, 14(7), e0219197. 10.1371/journal.pone.0219197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- WHO . (2017). Joint external evaluation of IHR core capacities of the Islamic Republic of Pakistan . http://www.who.int/ihr/publications/WHO‐WHE‐CPI‐2017.9/en/
- WHO . (2021). WHO‐OIE Operational Framework for Good governance at the human‐animal interface . https://www.who.int/ihr/publications/WHO‐OIE_Operational_Framework/en/
- WHO . (2022). Strengthening the IHR through a one health approach . https://www.who.int/activities/strengthening‐global‐health‐security‐at‐the‐human‐animal‐interface/strengthening‐the‐IHR‐through‐a‐one‐health‐approach
- WOAH . (2017). IHR‐PVS National Bridging Workshop | strategic partnership for IHR and health security (SPH). https://extranet.who.int/sph/ihr‐pvs‐bridging‐workshop
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.