

Abstract
Aim
Acute pyelonephritis is one of the most common bacterial infections in childhood. This potentially serious condition can lead to renal scarring, loss of kidney function and hypertension. The aim of this study was to identify risk factors associated with pyelonephritis in children without kidney or urinary tract abnormalities.
Methods
Medical records of children aged 4–18 diagnosed with 1st time pyelonephritis from 2016 to 2021 were retrospectively analysed. Children with abnormal kidney ultrasound were excluded. In addition to demographic data, information on bladder and bowel function was extracted together with habits of fluid intake.
Results
A total of 105 patients were diagnosed with 1st time pyelonephritis. Of these, 47% were diagnosed with constipation according to the Rome IV criteria within a mean follow‐up period of 167 days after their pyelonephritis, which is markedly higher than the estimated prevalence of constipation in the background population. Constipation was positively associated with recurrent urinary tract infection (p = 0.01).
Conclusion
Constipation is associated with pyelonephritis and recurrent urinary tract infection in children (primarily girls) 4–18 years of age without evident kidney or urinary tract abnormalities. We recommend systematic evaluation of bowel and bladder function after 1st time pyelonephritis in all children >4 years.
Abbreviations
- ANOVA
Analysis of Variance
- BBD
Bladder and Bowel Dysfunction
- BC
Bladder Capacity
- DUI
Daytime Urinary Incontinence
- E. Coli
Escherichia Coli
- EBC
Expected Bladder Capacity
- EN
Enuresis Nocturna
- ICCS
International Children's Continence Society
- IQR
Interquartile Range
- LUTS
Lower Urinary Tract Symptoms
- MVV
Maximum Voided Volume
- PACCT
Paris Consensus on Childhood Constipation Terminology
- PVR
Post‐void Residual Volume
- Qmax
Maximum Flow
- SD
Standard Deviation
- US
Ultrasound
- UT
Urinary Tract
- UTI
Urinary Tract Infection
- VUR
Vesicoureteral Reflux
Key Notes.
Evidence on risk factors associated with pyelonephritis and recurrent urinary tract infection in children without kidney or urinary tract abnormalities is sparse.
In a carefully selected cohort of children 4–18 years of age without evident kidney or urinary tract abnormalities based on renal ultrasound, functional constipation was positively associated with 1st time pyelonephritis and recurrent urinary tract infection.
Systematic evaluation of bowel and bladder function should be performed in all children >4 years after 1st time pyelonephritis.
1. INTRODUCTION
Urinary tract infection (UTI) is among the most common bacterial infections in childhood affecting up to 8.4% of girls and 1.7% of boys within the first 6 years of life. 1 , 2 Pyelonephritis is defined as an upper UTI involving the upper urinary tract and kidney parenchyma. This potentially serious condition can lead to renal scarring, 3 , 4 which can further result in loss of kidney function and long‐term sequelae such as hypertension. 5 Approximately 85–95% of upper and lower UTIs are caused by Escherichia coli (E. coli). Klebsiella, Proteus, Enterococcus and Enterobacter species are other common organisms. 6
Kidney or urinary tract (UT) abnormalities, for example vesicoureteral reflux, (VUR) are well‐established risk factors associated with UTI. 3 , 7 However, our knowledge on risk factors associated with UTI in children without kidney or UT abnormalities is limited. Few studies suggest an association between the recurrence of UTI and functional constipation 8 , 9 as well as daytime urinary incontinence (DUI). 3 , 10 , 11 , 12
In the clinical setting, high‐fluid intake is recommended for UTI prevention due to the prevention of bacterial proliferation and elimination of the contaminating bacteria with frequent voiding. However, evidence on insufficient fluid intake as a risk factor associated with UTI is inconsistent, 13 and data on the paediatric population is sparse. 14
The aim of this study was to investigate risk factors for 1st time pyelonephritis and recurrent UTI in children without evident kidney or UT abnormalities.
2. MATERIALS AND METHODS
Since 2016, children >4 years diagnosed with 1st time pyelonephritis in the paediatric emergency department at Gødstrup Hospital, Denmark and Central Jutland Regional Hospital, Denmark have been offered a follow‐up visit in the outpatient clinic.
The follow‐up visit encompasses assessment of bowel function based on Rome IV criteria, transabdominal ultrasound (US) with measurement of rectal diameter and assessment of bladder function by 48‐h frequency–volume chart and uroflow measurement. The cut‐off age was chosen, as these data/measurements would not be possible in children younger than 4 years of age.
In this retrospective study, we reviewed medical records of children aged 4–18 years who presented with 1st time pyelonephritis between 1 January 2016 and 1 May 2021 at these two hospitals. The cases were evaluated for inclusion if one of the following ICD‐10 diagnostic codes was registered in the medical record: DN109C acute pyelonephritis, DN118B recurrent pyelonephritis and DN129 pyelonephritis NOS.
Inclusion criteria were a confirmed diagnosis of 1st time pyelonephritis according to guidelines with a significant growth of bacteria in a urine culture from a mid‐stream urine sample. A growth of ≥10 4 CFU/ml in two consecutive clean catch urine samples was considered positive. 15 Fever (>38.0°C) and other symptoms associated with AP such as urge, pollakisuria, dysuria, stomach or lower back pain and lethargy were required in combination with the positive urine culture.
Children with confirmed pyelonephritis had a kidney US performed within 2 months after the infection. Exclusion criteria were anatomical abnormalities diagnosed by US, prior lower urinary tract surgery and neurogenic bladder dysfunction.
A clinical database was established in REDCap electronic data capture tools hosted at Aarhus University, Aarhus, Denmark. 16
Demographic data (e.g. gender, age) were extracted along with data concerning medical history and clinical presentation at symptom onset. Method for urine sample was registered along with type of bacteria identified in the urine culture.
Constipation, DUI and enuresis nocturna (EN) was noted in accordance with the Rome IV criteria 17 and recommendations from the International Children's Continence Society (ICCS). 18 DUI and EN were registered in children from 5 years in accordance with ICCS guidelines. 18 Data on fluid intake, maximum voided volume (MVV) and micturition frequency were obtained from the 48‐h frequency–volume chart filled in by the patients before their first visit in the outpatient clinic. Expected bladder capacity (EBC) was calculated using the formula: EBC (ml) = (age(years) + 1) × 30. 18
The following data were registered from the uroflowmetry also performed at first visit in the outpatient clinic: uroflow pattern, maximum flow (Qmax), voided volume and post‐void residual volume (PVR). Only uroflowmetry curves with a voided volume > 50 ml were considered relevant for interpretation. The shape of the flow was characterised as bell, tower, plateau, staccato or interrupted in accordance with ICCS definitions. 18 For children aged 4–6 years, a single PVR >30 ml or > 21% of bladder capacity (BC) (BC = PVR + voided volume) was regarded as significant. Elevated PVR for children age ≥7 years was defined as a single PVR >20 ml or 15% BC. 18
2.1. Statistical analysis
Descriptive data were reported as mean ± standard deviation (SD) for normally distributed data and as median with interquartile range (IQR) for non‐parametric data. One‐way analysis of variance (ANOVA) was used to compare normally distributed variables and Kruskal–Wallis test was used when comparing non‐normally distributed variables. Categorical variables were reported in numbers and percentages and compared using chi‐squared test and Fisher's exact test when appropriate. A p‐value <0.05 was considered statistically significant. All statistics were calculated using STATA 17.9 (StataCorp, 2019. Stata Statistical Software: Release 17. College Station, TX: StataCorp LCC).
3. RESULTS
A total of 229 children and adolescents were identified by one of the ICD‐10 diagnostic codes: DN109C acute pyelonephritis, DN118B recurrent pyelonephritis and DN129 pyelonephritis NOS. A total of 124 patients (54%) were subsequently excluded from the analysis; in 31 (14%) patients the initial diagnosis was dismissed or not confirmed by urine culture with significant growth, 28 (12%) had kidney or UT abnormality, 3 (1%) had neurogenic bladder following damage to the spinal cord, 1 (0.4%) was diagnosed with 1st time pyelonephritis before the age of 4 and 61 (27%) were not offered a follow‐up visit or did not show up for their follow‐up appointment (Figure 1).
FIGURE 1.
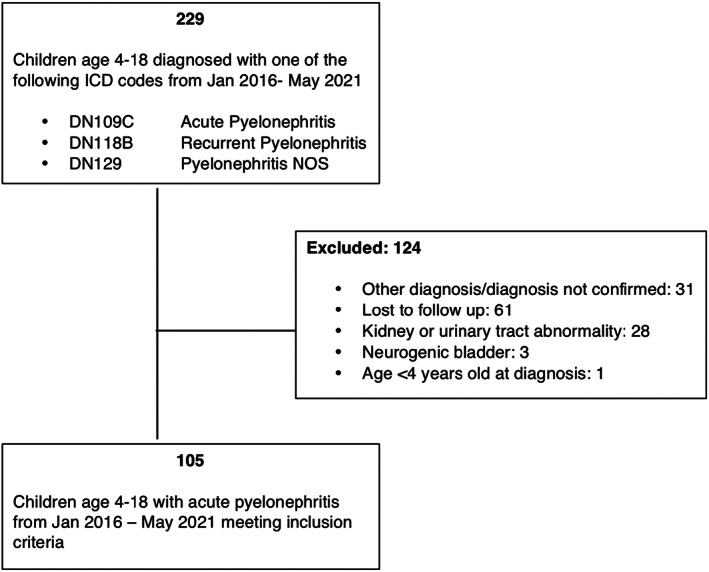
Study cohort flow diagram.
3.1. Demographic findings and clinical characteristics
A total of 105 patients met the inclusion criteria for enrolment in the study. Demographic data and clinical characteristics for the study population are presented in Table 1.
TABLE 1.
Demographic data and clinical characteristics for the study population.
| All patients with 1st time pyelonephritis 01‐Jan‐2016 to 01‐May‐2021 | n = 105 | Missing/n (%) |
|---|---|---|
| Baseline characteristics | ||
| Age (years), median (iqi) | 7 (5; 11) | 0/105 (0) |
| Sex (female), n (%) | 98 (93) | 0/105 (0) |
| Time from admission to follow‐up (days), mean (SD) | 167 (98) | 0/105 (0) |
| Microbiology | ||
| ‐ E. coli, n (%) | 100 (95) | |
| ‐ Other, n (%) | 5 (5) | |
| Bowel function | ||
| Constipation (yes), n (%) | 49 (47) | 1/105 (0.1) |
| Rectal diameter, by ultrasound, (cm), mean (SD) | 3.2 (1) | 52/105 (50) |
| Bladder diary | ||
| Fluid intake (mL), mean (SD) | 1169 (483) | 31/105 (30) |
| Voiding frequency per day, mean (SD) | 6 (2) | 48/105 (46) |
| MVV a /EBC b , mean (SD) | 1.1 (0.4) | 44/82 (54) |
| DUI c (≥5 years of age) (yes), n (%) | 40 (44) | 1/92 (1) |
| EN d (≥5 years of age) (yes), n (%) | 18 (20) | 1/92 (1) |
| Uroflow | ||
| Pattern | 12/105 (11) | |
| ‐ Normal, n (%) | 48 (52) | |
| ‐ Abnormal, n (%) | 45 (48) | |
| Total voided volume, median (iqi) | 152.5 (106; 223) | 11/105 (10) |
| Qmax e (mL/s), mean (SD) | 25.0 (10) | 13/105 (12) |
| Residual urine (yes), n (%) | 43 (46) | 12/105 (11) |
| ‐ mL, median (iqi) | 46 (30; 60) | |
| Follow‐up | ||
| More than one follow‐up (yes), n (%) | 70 (67) | 12/105 (11) |
Maximum Voided Volume.
Expected Bladder Capacity.
Daytime Urinary Incontinence.
Enuresis Nocturna.
Maximum Flow.
The majority of the patients (93%) were girls with a median age of 7 years. E. coli was cultured in 95% of the urine samples. Mean time from diagnosis to follow‐up in the outpatient clinic was 167 (SD 98) days.
Constipation was diagnosed in 47% of children at follow‐up. Data on bowel function were missing in one patient. DUI was present in 44% of children and 20% had EN. The population had a mean fluid intake of 1169 ml/day and mean voiding frequency was 6 times/day.
Uroflowmetry pattern was evaluated in accordance with ICCS guidelines. 18 A bell‐shaped curve was considered normal whereas tower‐shaped, staccato‐shaped, plateau‐shaped and interrupted curves were considered abnormal. Uroflowmetry was not performed in 12 patients, either due to technical challenges or due to the patient's inability to urinate.
In 33% of cases, no additional follow‐up was needed after the first visit in the outpatient clinic, leaving 67% of patients with one or more bowel or bladder symptoms with the need for further investigation, treatment and/or follow‐up (28% only constipation, 19% only DUI, 19% constipation and DUI).
3.2. Single episode vs. recurrent pyelonephritis
Children with recurrent UTI after their 1st time pyelonephritis were compared to children with no recurrence (Table 2).
TABLE 2.
Recurrence vs. no recurrence
| Recurrence | No Recurrence | p | |
|---|---|---|---|
| All patients, n (%) | 43 (41) | 62 (59) | |
| Baseline characteristics | |||
| Age (median), n (%) | 6 (5; 10) | 7 (6; 12) | 0.07 |
| Follow‐up time (years), mean (SD) | 3.1 (1.0) | 2.6 (1.2) | 0.03 |
| Time from 1st time pyelonephritis to 1st recurrence (days), median (iqi) | 132 (43; 297) | ||
| Bowel function | |||
| Constipation (yes), n (%) | 27 (63) | 22 (36) | 0.01 |
| Bladder diary | |||
| Fluid intake (mL), mean (SD) | 1134 (553) | 1191 (438) | 0.6 |
| DUI a (≥5 years of age) (yes), n (%) | 19 (44) | 21 (34) | 0.3 |
| EN b (≥5 years of age) (yes), n (%) | 11 (53) | 7 (47) | 0.06 |
| Uroflow | |||
| Pattern (abnormal), n (%) | 19 (50) | 26 (47) | 0.8 |
| Residual urine (yes), n (%) | 20 (54) | 23 (41) | 0.2 |
Daytime Urinary Incontinence.
Enuresis Nocturna.
Recurrences until 01 November 2021 were registered to ensure a minimum follow‐up period of 6 months for all included children. Mean follow‐up time was 2.6 years (SD 1.2) for children without recurrent infection and 3.1 years (SD 1.0) for children with recurrence (p = 0.03) Median time from 1st pyelonephritis to first recurrent infection was 132 days. A trend towards children with recurrent infection to be younger than those without further infections was observed (Mean age 6 and 7 respectively, p = 0.07). Children with one or more recurrent infections had a higher prevalence of constipation (p = 0.01). No difference in DUI or EN was observed between groups. Mean fluid intake was equal between children with and without recurrent infection. Data from uroflowmetry revealed no difference according to uroflow pattern and no difference in number of children with elevated PVR.
3.3. Children diagnosed with constipation compared to non‐constipated children
Children diagnosed with constipation according to the Rome IV criteria at the follow‐up visit in the outpatient clinic after their 1st time pyelonephritis were compared with non‐constipated children (Table 3).
TABLE 3.
Constipation vs. no constipation
| Constipation | No constipation | p | |
|---|---|---|---|
| All patients, n (%) | 49 (47) | 55 (53) | |
| Bladder diary | |||
| Fluid intake (mL), mean (SD) | 1136 (558) | 1197 (414) | 0.6 |
| DUI a (≥5 years of age) (yes), n (%) | 20 (41) | 20 (37) | 0.7 |
| EN b (≥5 years of age) (yes), n (%) | 6 (12) | 12 (22) | 0.2 |
| Uroflow | |||
| Pattern (abnormal), n (%) | 20 (49) | 24 (47) | 0.9 |
| Residual urine (yes), n (%) | 18 (44) | 25 (49) | 0.6 |
Daytime Urinary Incontinence.
Enuresis Nocturna.
According to data from bladder diary, no difference in fluid intake or prevalence of DUI or EN was observed between children with and without constipation. Delving into uroflow parameters, no difference in curve pattern or presence of PVR was observed between the two groups.
4. DISCUSSION
In a carefully selected cohort of children between 4 and 18 years of age without evident kidney or UT abnormalities accessed by US, constipation is associated with 1st time pyelonephritis and recurrent UTI.
In this study, 47% of the enrolled children were identified as being constipated which is considerably higher than the estimated prevalence of constipation in childhood (16%). 19 A relationship between constipation and UTI in childhood is generally accepted but has only been investigated in few studies and with heterogeneous results. Blethyn et al 9 found an association between constipation and the number of UTIs in children from 2–14 years old. Constipation was, however, defined as the presence of faecal impaction on radiography and not diagnosed based on the Rome IV criteria, which is considered gold standard today. Loening‐Baucke et al 8 observed a 3% rate of UTI in constipated boys and a 33% rate in constipated girls and reported that successful management of constipation resulted in disappearance of recurrent UTIs in all patients without UT abnormalities. Contrary to this, Chang et al 20 found no significant association between constipation diagnosed with Rome III criteria and the recurrence of UTI in toilet‐trained children. However, the authors suggest the small sample size of 60 enrolled children to be the cause of the statistical non‐significance. In the same study, 48,5% of the enrolled girls were diagnosed with constipation after their 1st time pyelonephritis, which is comparable to the prevalence found in our study.
More recent studies have elucidated bladder and bowel dysfunction (BBD) as a risk factor for UTI both in the presence and absence of VUR. Sjöström et al 12 found an overall BBD prevalence of 38% in preschool children with a history of pyelonephritis during their first year of life with a stronger association in girls where 46% had BBD. This is in accordance with the findings of this study, where the majority of included children are girls. However, marked differences between the two populations are worth mentioning, as Sjöström looked at children with pyelonephritis during the first year of life, which is a population with more even gender distribution and probably not comparable to our cohort of children from the age of 4 years with 1st time pyelonephritis. Furthermore, BBD was diagnosed based on a questionnaire where the scale for total scores showed a sum cut‐off score of ≥7 for BBD, but symptoms from both bowel and bladder system were not required. As children in this study presented mainly with LUT dysfunction and only 17% with constipation it is difficult to compare their results to ours.
Shaikh et al 11 investigated the prevalence of BBD in a cohort of toilet‐trained children with 1st time pyelonephritis from the age of 2 months to 6 years. Even though many of the enrolled children had their pyelonephritis before toilet training was completed, the cohort was more similar to ours, than the above‐mentioned studies. Shaikh et al found BBD to be present in 54% of all included children regardless of VUR status. In accordance with Sjöström et al, a validated questionnaire that did not differentiate between bowel and bladder symptoms was used to diagnose BBD and only 22% of the children met criteria for constipation according to the modified Paris consensus on childhood constipation terminology (PACCT) used in the study. 21 Our study suggests a more significant association between constipation and UTI than the two BBD studies. The reason for this could be the close temporal association between the pyelonephritis and screening for constipation in our study.
Although a causal relation between constipation and UTI is not fully clarified, an association between constipation and PVR should be considered as a partial explanation. Kalyoncu et al 22 found elevated PVR in 26% of constipated children compared to 3% of children with neither constipation nor lower urinary tract symptoms (LUTS). This is comparable to Chung et al 23 who found elevated PVR in 35.5% of children with severe constipation. PVR is a well‐known predictor of recurrent UTI in children. 20
In our study, we found no association between constipation and abnormal uroflow or elevated PVR, despite a significant number of children with elevated PVR in the cohort. An explanation for this could be the substantial amount of missing data on uroflow and residual urine volume and therefore a too small cohort to achieve statistical significance.
Furthermore, uroflow was only performed on one occasion and not repeated in case of a pathological curve as recommended by the ICCS, 18 increasing the risk of overestimating the prevalence of pathological curves and elevated PVR.
4.1. Recurrent UTIs
In this study, 39.4% of children had one or more recurrent UTIs after their 1st time pyelonephritis, which is in consistence with recurrence rates observed in other studies. 24 Our study suggests children with recurrence to be younger than children without further infections though statistical significance was not achieved. This association is supported by findings in previous studies 20 and is speculated to be caused by maturation of the bladder function with increased age. 25 Constipation was positively associated with recurrent UTI strengthening the hypothesis of constipation as a risk factor for UTI in children.
4.2. Fluid intake and UTI
High fluid intake is considered protective for UTI. 26 In our study, the enrolled children had a mean fluid intake of 1169 ml (SD 486) based on a two‐day diary obtained by primarily the parents, but probably more independent by the adolescents. No difference in fluid intake between children with and without relapse was observed. In clinical practice, a daily fluid intake of 1200–1500 ml is typically recommended for children with constipation and urinary incontinence. As this is consistent with the findings in our study, we cannot detect an association between decreased fluid intake and occurrence of UTIs based on our data. However, in the light of the lacking knowledge about fluid intake in a general population of children and adolescents and the difficulties in fluid assessment, further studies are needed to make more accurate conclusions on fluid intake and the association with constipation and UTIs in childhood.
4.3. Systematic follow‐up program for children with 1st time pyelonephritis—should it be advised?
In our study, we utilised the systematic follow‐up for children with 1st time pyelonephritis after the age of four to identify risk factors. We identified a large number of children with constipation; thus, we believe that a systematic follow‐up programme for children after their 1st time pyelonephritis is important to reduce the risk for further UTIs and subsequent renal scarring. Furthermore, a high incidence of both DUI and EN was observed in our cohort compared with the background population. 27 , 28 Therefore, we recommend both bowel and bladder function to be evaluated after 1st time pyelonephritis in all children.
4.4. Strengths and limitations
Our study has several limitations. This was a retrospective, observational study with no control group. We had to exclude 27% of the children because follow‐up was missing or insufficient. In some cases, the physician did not offer follow‐up, because the new guidelines were failed; in other cases, the patient failed to attend the appointment in the outpatient clinic. Children lost to follow‐up might have been less likely to have symptoms from bowel or bladder system overestimating the association between these conditions and 1st time pyelonephritis in our study.
We assumed our cohort to be without kidney or UT abnormalities based on routine US performed within 1–2 months after the pyelonephritis. However, US is limited by its ability to detect renal abnormalities, as only 40% of VUR and 50% of renal scar abnormalities are detected. 29 , 30
Another limitation is the different follow‐up period among the enrolled children. The short follow‐up period for some of the children might underestimate the risk of recurrence and can potentially underestimate the difference between the two groups as some of the children with recent 1st time pyelonephritis registered in the non‐relapse group may have relapse after the end of the study. A difference in follow‐up time was registered between children with and without recurrence. However, all children had a minimum follow‐up period of 6 months and with a median time of only 132 days from 1st pyelonephritis to first recurrent infection, the different follow‐up period is not expected to cause significant bias of the results.
The major strength of this study is the systematic follow‐up strategy for children with 1st time pyelonephritis, as the enrolled children are well characterised and have been through the same profound examination.
In conclusion, this study provides evidence that constipation is associated with pyelonephritis and recurrent UTI in primarily girls 4–18 years of age without evident kidney or UT abnormalities. It supports the strategy of systematic follow‐up for all children from the age of 4 years after their 1st time pyelonephritis in order to identify and treat risk factors and potentially reduce the risk of recurrent UTIs.
AUTHOR CONTRIBUTIONS
Luise Borch, Konstantinos Kamperis and Søren Hagstrøm contributed to the study conception and design. Sofie Axelgaard did material preparation, data collection and analysis and wrote the first draft of the manuscript. Rasmus Kristensen and Alexander Jessen contributed to data analysis. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
FUNDING INFORMATION
No funding was received to assist with the preparation of this manuscript.
CONFLICT OF INTEREST
The authors have no relevant financial or non‐financial interest to disclose.
ACKNOWLEDGEMENTS
Marie‐Louise E. Andersen, MD, Ph.D., who evaluated children with 1st time pyelonephritis in the outpatient clinic, Central Jutland Regional Hospital. Marie‐ Louise E. Andersen also helped identifying the children for the present study.
Axelgaard S, Kristensen R, Kamperis K, Hagstrøm S, Jessen AS, Borch L. Functional constipation as a risk factor for pyelonephritis and recurrent urinary tract infection in children. Acta Paediatr. 2023;112:543–549. 10.1111/apa.16608
DATA AVAILABILITY STATEMENT
The authors confirm that this manuscript is an honest and transparent account of the study being reported. The data sets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
REFERENCES
- 1. Hellström A, Hanson E, Hansson S, Hjälmås K, Jodal U. Association between urinary symptoms at 7 years old and previous urinary tract infection. Arch Dis Child. 1991;66(2):232‐234. doi: 10.1136/adc.66.2.232 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Hoberman A, Chao HP, Keller DM, Hickey R, Davis HW, Ellis D. Prevalence of urinary tract infection in febrile infants. J Pediatr. 1993;123(1):17‐23. doi: 10.1016/s0022-3476(05)81531-8 [DOI] [PubMed] [Google Scholar]
- 3. Keren R, Shaikh N, Pohl H, et al. Risk factors for recurrent urinary tract infection and renal scarring. Pediatrics. 2015;136(1):e13‐e21. doi: 10.1542/peds.2015-0409 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Breinbjerg A, Jørgensen CS, Frøkiær J, Tullus K, Kamperis K, Rittig S. Risk factors for kidney scarring and vesicoureteral reflux in 421 children after their first acute pyelonephritis, and appraisal of international guidelines. Pediatr Nephrol. 2021;36(9):2777‐2787. doi: 10.1007/s00467-021-05042-7 [DOI] [PubMed] [Google Scholar]
- 5. Patzer L, Seeman T, Luck C, Wühl E, Janda J, Misselwitz J. Day – and night‐time blood pressure elevation in children with higher grades of renal scarring. J Pediatr. 2003;142(2):117‐122. doi: 10.1067/mpd.2003.13 [DOI] [PubMed] [Google Scholar]
- 6. Chakupurakal R, Ahmed M, Sobithadevi DN, Chinnappan S, Reynolds T. Urinary tract pathogens and resistance pattern. J Clin Pathol. 2010;63(7):652‐654. doi: 10.1136/jcp.2009.074617 [DOI] [PubMed] [Google Scholar]
- 7. Nordenström J, Sillen U, Holmdahl G, Linnér T, Stokland E, Sjöström S. The Swedish infant high‐grade reflux trial – bladder function. J Pediatr Urol. 2017;13(2):139‐145. doi: 10.1016/j.jpurol.2016.10.022 [DOI] [PubMed] [Google Scholar]
- 8. Loening‐Baucke V. Urinary incontinence and urinary tract infection and their resolution with treatment of chronic constipation of childhood. Pediatrics. 1997;100(2 Pt 1):228‐232. doi: 10.1542/peds.100.2.228 [DOI] [PubMed] [Google Scholar]
- 9. Blethyn AJ, Jenkins HR, Roberts R, Verrier JK. Radiological evidence of constipation in urinary tract infection. Arch Dis Child. 1995;73(6):534‐535. doi: 10.1136/adc.73.6.534 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Sureshkumar P, Jones M, Cumming RG, Craig JC. Risk factors for urinary tract infection in children: a population‐based study of 2856 children. J Paediatr Child Health. 2009;45(3):87‐97. doi: 10.1111/j.1440-1754.2008.01435.x [DOI] [PubMed] [Google Scholar]
- 11. Shaikh N, Hoberman A, Keren R, et al. Recurrent urinary tract infections in children with bladder and bowel dysfunction. Pediatrics. 2016;137(1):e20152982. doi: 10.1542/peds.2015-2982 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Sjöström S, Sillén U, Bachelard M, et al. Bladder/bowel dysfunction in pre‐school children following febrile urinary tract infection in infancy. Pediatr Nephrol. 2021;36(6):1489‐1497. doi: 10.1007/s00467-020-04853-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Fasugba O, Mitchell BG, McInnes E, et al. Increased fluid intake for the prevention of urinary tract infection in adults and children in all settings: a systematic review. J Hosp Infect. 2020;104(1):68‐77. doi: 10.1016/j.jhin.2019.08.016 [DOI] [PubMed] [Google Scholar]
- 14. Rudaitis S, Pundziene B, Jievaltas M, Uktveris R, Kevelaitis E. Recurrent urinary tract infection in girls: do urodynamic, behavioral and functional abnormalities play a role? J Nephrol. 2009;22(6):766‐773. [PubMed] [Google Scholar]
- 15. Aspevall O, Hallander H, Gant V, Kouri T. European guidelines for urinalysis: a collaborative document produced by European clinical microbiologists and clinical chemists under ECLM in collaboration with ESCMID. Clin Microbiol Infect. 2001;7(4):173‐178. doi: 10.1046/j.1198-743x.2001.00237.x [DOI] [PubMed] [Google Scholar]
- 16. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi: 10.1016/j.jbi.2019.103208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Zeevenhooven J, Koppen IJ, Benninga MA. The new Rome iv criteria for functional gastrointestinal disorders in infants and toddlers. Pediatr Gastroenterol Hepatol Nutr. 2017;20(1):1‐13. doi: 10.5223/pghn.2017.20.1.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Austin PF, Bauer SB, Bower W, et al. The standardization of terminology of lower urinary tract function in children and adolescents: update report from the standardization committee of the international Children's continence society. NeurourolUrodyn. 2016;35(4):471‐481. doi: 10.1002/nau.22751 [DOI] [PubMed] [Google Scholar]
- 19. Mugie SM, Benninga MA, di Lorenzo C. Epidemiology of constipation in children and adults: a systematic review. Best Pract Res Clin Gastroenterol. 2011;25(1):3‐18. doi: 10.1016/j.bpg.2010.12.010 [DOI] [PubMed] [Google Scholar]
- 20. Chang SJ, Tsai LP, Hsu CK, Yang SS. Elevated postvoid residual urine volume predicting recurrence of urinary tract infections in toilet‐trained children. Pediatr Nephrol. 2015;30(7):1131‐1137. doi: 10.1007/s00467-014-3009-y [DOI] [PubMed] [Google Scholar]
- 21. Benninga M, Candy DC, Catto‐Smith AG, et al. The Paris consensus on childhood constipation terminology (PACCT) group. J Pediatr Gastroenterol Nutr. 2005;40(3):273‐275. doi: 10.1097/01.mpg.0000158071.24327.88 [DOI] [PubMed] [Google Scholar]
- 22. Kalyoncu A, Thomas DT, Abdullayev T, et al. Comparison of uroflow parameters in children with pure constipation versus constipation plus lower urinary tract symptoms. Scand J Urol. 2015;49(6):492‐496. doi: 10.3109/21681805.2015.1059358 [DOI] [PubMed] [Google Scholar]
- 23. Chung KL, Chao NS, Liu CS, Tang PM, Liu KK, Leung MW. Abnormal voiding parameters in children with severe idiopathic constipation. Pediatr Surg Int. 2014;30(7):747‐749. doi: 10.1007/s00383-014-3511-0 [DOI] [PubMed] [Google Scholar]
- 24. Conway PH, Cnaan A, Zaoutis T, Henry BV, Grundmeier RW, Keren R. Recurrent urinary tract infections in children: risk factors and association with prophylactic antimicrobials. Jama. 2007;298(2):179‐186. doi: 10.1001/jama.298.2.179 [DOI] [PubMed] [Google Scholar]
- 25. Jansson UB, Hanson M, Sillén U, Hellström AL. Voiding pattern and acquisition of bladder control from birth to age 6 years—a longitudinal study. J Urol. 2005;174(1):289‐293. doi: 10.1097/01.ju.0000161216.45653.e3 [DOI] [PubMed] [Google Scholar]
- 26. Beetz R. Mild dehydration: a risk factor of urinary tract infection? Eur J Clin Nutr. 2003;57(Suppl 2):S52‐S58. doi: 10.1038/sj.ejcn.1601902 [DOI] [PubMed] [Google Scholar]
- 27. Nieuwhof‐Leppink AJ, Schroeder RPJ, van de Putte EM, de Jong TPVM, Schappin R. Daytime urinary incontinence in children and adolescents. Lancet Child Adolesc Health. 2019;3(7):492‐501. doi: 10.1016/S2352-4642(19)30113-0 [DOI] [PubMed] [Google Scholar]
- 28. Järvelin MR, Vikeväinen‐Tervonen L, Moilanen I, Huttunen NP. Enuresis in seven‐year‐old children. Acta Paediatr Scand. 1988;77(1):148‐153. doi: 10.1111/j.1651-2227.1988.tb10614.x [DOI] [PubMed] [Google Scholar]
- 29. Mahant S, Friedman J, MacArthur C. Renal ultrasound findings and vesicoureteral reflux in children hospitalised with urinary tract infection. Arch Dis Child. 2002;86(6):419‐420. doi: 10.1136/adc.86.6.419 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Christian MT, McColl JH, MacKenzie JR, Beattie TJ. Risk assessment of renal cortical scarring with urinary tract infection by clinical features and ultrasonography. Arch Dis Child. 2000;82(5):376‐380. doi: 10.1136/adc.82.5.376 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The authors confirm that this manuscript is an honest and transparent account of the study being reported. The data sets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.