

A patient undergoing a right pneumonectomy for bronchogenic cancer also underwent tangential resection of the superior vena cava (SVC), which had been partly infiltrated by the tumor. The surgical procedure included intrapericardial ligation of both pulmonary veins and complete isolation of the SVC, from the atrium to the brachiocephalic trunks; this involved freeing the SVC at the point of its connection with the pericardium. The absence of these 3 right points of fixation (the SVC and the pulmonary veins at their pericardial junctions) presumably enabled the heart to slip through the pericardial window and to rotate its tip to the right. In spite of this cardiac displacement, the hemodynamic condition of the patient remained acceptable, so the problem was not discovered for a couple of hours, at which point standard postoperative chest radiography revealed it (Fig. 1). The cardiac torsion was confirmed by external echocardiography. The patient then underwent repeat thoracotomy, heart repositioning, and right pericardial reconstruction with a Gore-Tex® patch.
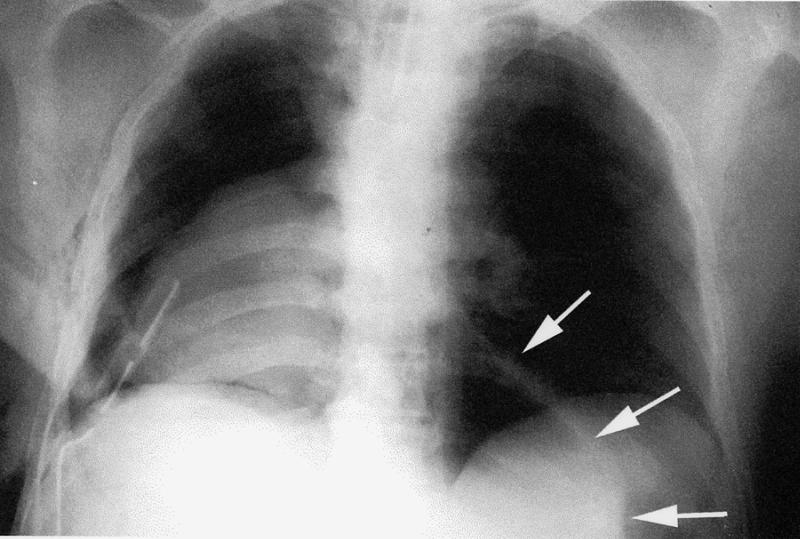
Fig. 1 Chest radiograph shows 180° rightward rotation of the heart. Arrows outline the empty pericardial sac.
Cardiac herniation after partial pericardiectomy during pneumonectomy is not a rare occurrence. Thoracic surgeons need to remember to repair the pericardial window at the time of right pneumonectomy. In fact, the heart—displaced through the pericardial window by increased abdominal pressure or by increased right hemithorax negative pressure (i.e., improper drainage)—might actually rotate its tip, as in our patient. In cases of left pneumonectomy, it may be sufficient to enlarge the pericardial defect in order to prevent strangulation, should herniation occur.
Footnotes
Address for reprints: S. Nazari, MD, Residenza Parco 152, 20080 Milano 3-Basiglio, Italy
*Dr. Semler has an interest in a company that manufactures a mechanical compression device.