

ABSTRACT
Anecdotal evidence indicated some British military dive support boat personnel suffer from uncomfortably cold hands and feet, which could impair their performance and be associated with reductions in core body temperature. This study collected preliminary data on thermal stress and cognitive performance of personnel taking part in a cold-weather training exercise. Six men were monitored during four boat transits in a range of climatic conditions (air temperature +1.2°C to −10.5°C, wind chill −4.5°C to 19.3°C). Core body temperature was measured with a radio pill and 12 skin sites (ISO 9886 plus hand, finger, foot and toe) with iButtons or thermistors. Self-reported thermal comfort and thermal sensation was also recorded. Reaction time and selective attention were measured pre- and post-transit. Participants’ physical characteristics and personal clothing ensembles were recorded. No participant became hypothermic. Most participants’ hand, foot and digit temperatures fell to below 15°C, indicating a risk of impaired dexterity, in addition to that arising from gloves. During the trial, hand and digit temperatures occasionally fell below 10°C. The limited data collected showed personal clothing choices could provide adequate thermal protection for these conditions and temperatures, and highlighted inter-individual variation and the need to allow for significant variation of day-to-day environmental conditions.
KEYWORDS: Non-freezing cold injury, cold stress, thermal stress, Military, support personnel, maritime exercise
Introduction
Military divers are often required to operate in cold environments for long periods of time. During British military diver training, supporting personnel will transit in a support boat to act in supervisory and stand by role throughout the dive duration. In this role, personnel can be exposed to air temperatures below that of the water where wind chill is likely to be experienced. These conditions could reduce the physical and cognitive performance of these personnel as well as increase the risk of thermal injury. Whilst the military has guidance on the minimum operating temperatures (−20°C with wind chill) and cold weather clothing for personnel in place, anecdotal reports indicated that some personnel still report feeling uncomfortably cold during cold weather exercises. An individual exposed to a cold environment is at risk of systemic (i.e. hypothermia) and local cold injury. Thermal strain, be it systemic or local, is known to reduce task performance [1], and military populations may be at further risk of performance detriments, through the presence of additional stressors such as lack of sleep, underfeeding and strenuous physical activity [2] or prolonged periods of inactivity, e.g. sentry duty [3].
Local cold injuries are classified as freezing-cold injury (FCI) or non-freezing-cold injury (NFCI) and are prevalent amongst the military population. FCI is defined, “as the damage sustained by tissues while subject to temperatures below their freezing point at approximately −0.55°C” [4]. Heil, Oakley, and Wood (2015) undertook a review of cases of UK military FCI between 2002 and 2014 [5]. Of the 149 patients with a positive FCI diagnosis that were identified for a follow-up study, Royal Marine personnel represented over 50% of patients and Arctic training in Norway accounted for over two-thirds of the total cases. Additionally, the authors noted that the extremities were the predominant area affected by FCI and those of junior rank were disproportionally affected. NFCI is prevalent amongst the military population and occurs when tissue temperature remains low, typically between 1°C and 15°C [6], for a prolonged period of time. The body areas most susceptible to NFCI are the extremities [7]. Of the 54 individual Marines who suffered cold injuries following a training exercise in Norway, 72% were in the feet, 25% in the hands with the remaining injuries sustained in other skin sites [8]. A similar pattern of injuries was seen over a 10-year review (1994–2003) of Israeli Defence Forces cold injuries [9], of the 110 peripheral cold injuries cases, 88 cases (80%) affected the feet and 22 cases (20%) affected the hands.
Current evidence indicates that exposure to cold temperatures can negatively impact cognitive functions such as inhibitory control and selective attention [10]. The inhibition function of working memory refers to an individual’s ability to deliberately impede/inhibit automatic or dominant responses [11]. Yang et al. exposed six male participants to cold (−10°C) for 30 min [12]. Participants then completed a number of cognitive tests, including Stroop, which is a cognitive test that is commonly used to assess selective attention and inhibition performance. The study found that acute cold exposure reduced selective attention and inhibition performance. Consequently, during an operational environment, the ability to make a timely and accurate “shoot” or “no shoot” decision could be critical and therefore have a high degree of military relevance. The purpose of the study was to assess the effect of typical sea transits in a cold environment on body temperature (core body and skin temperature) and cognitive performance (reaction time and selective attention) in the dive support boat personnel.
Objectives
Assess thermal strain by measuring core body temperature, skin temperature, thermal comfort and thermal sensations in a cold-weather environment.
Describe the effect on cognitive workload and reaction time when operating in a cold-weather environment.
Method
Participants
Twelve male participants were recruited for the study and provided informed consent, one was withdrawn prior to the start following medical considerations. Due to personnel scheduling and mechanical issues caused by adverse weather; cold weather data from boat transits were collected from six participants (age, 32 ± 6 years). The study protocol was submitted to the Ministry of Defence Research Ethics Committee (MODREC) and received favourable opinion (935/MODREC/18).
Physical characteristics
Height (m) and body mass (kg) were measured with a portable stadiometer (SECA 213, Germany) and electronic scales (SECA 875, Germany), respectively. An accredited ISAK level 1 practitioner conducted eight site skinfold assessments (triceps, subscapular, biceps, iliac crest, supraspinale, abdominal, front thigh and medial calf) using calibrated skinfold callipers (Harpenden, Baty International, UK). Hand volume and foot volume were recorded by using the water-displacement plethysmography technique with specialised hand and foot volumetric oedema gauges (Baseline evaluation instruments, USA) and weighing the displaced water (Salter − 1036, BKSSDR, UK). Physical characteristic data were collected from five participants who were recruited in the UK but only three participants were instrumented due to personnel role rotations and delays to the exercise. Additional British military participants were recruited in Canada to increase the opportunity for instrumentation and as a result complete physical characteristic information was not obtained for the three additional participants due to the sensitive measurement devices not being carried overseas. A total of six participants were instrumented, four participants completed a single transit with participants 3 and 4 both completing two transits (Table 1).
Table 1.
Participants instrumented during each transit.
| Transit number | Participants |
|---|---|
| 1 | P2 |
| 2 | P3, P4, |
| 3 | P1, P3, P4, P5, |
| 4 | P4, P6 |
Note: P denotes participant.
Clothing
The participants wore a variety of issued and non-issued clothing during the trial. This is permitted and routine in this population during training exercises. All participants employed a layering system and wore hats and waterproof boots/shoes, with all but two participants reporting wearing gloves. The following layers were worn by the participants: underwear, socks, base-layer (top), base-layer (bottom), mid-layer (top), trousers, jumper/fleece, jacket, waterproof outer-layer (top), waterproof outer-layer (bottom), waterproof boots/shoes (Table 2). Only one participant chose to remove a layer (base-layer [bottom]) when they went out on a second and third transit. The materials of the clothing and footwear also were varied (man-made and natural) with the following observed by the study team or reported by the participants:
Table 2.
List of materials and fabrics observed or reported for each clothing layer worn by participants undertaking small boat transits (n=6).
| Layer | Material/fabric observed (main component of garment) |
|---|---|
| Hat | Wool, polyester, acrylic |
| Footwear | Leather, water-resistant suede, Gore-Tex® |
| Gloves | Pertex®, polyester |
| Underwear | Cotton |
| Socks | Merino wool, cotton |
| Base-layer (top) | Polyester, eastane |
| Base-layer (bottom) | Polyester, elastane |
| Mid-layer (top) | Cotton, elastane |
| Trousers | Elastane, polyester, cotton, water-resistant fabric/treatment |
| Jumper/fleece | Polyester |
| Jacket | Polyamide, polyester, water-resistant fabric, Gore Windstopper® |
| Waterproof outer-layer (top) | Polyamide, polyester, water-resistant fabric, polyurethane, acrylic |
| Waterproof outer-layer (trousers) | Polyamide, polyester, water-resistant fabric |
All participants wore a mixture of specialist outdoor brands that are designed for hiking, sailing, outdoor swimming and generic outdoor pursuits. Additionally, all participants wore at least one outer layer that was waterproof or water-resistant and those participants, who were older, wore less total layers than the younger participants. Interestingly, two experienced participants wore hooded poncho-style water-resistant robes as their main outer layer.
Empirical measures
The British military exercises took place in Halifax, Nova Scotia, Canada. and were based from a Main Support Vessel during February/March 2022. The participants were comprised of up to two instrumented support boat personnel per boat with up to two boats available. The boats had a sheltered helm on three sides with the rest of the boat unprotected from wind and rain. Due to the nature of the activities and duration of the transits, it was not possible to observe or record the tasks performed by the dive support boat personnel during transits. Participants were instrumented with the core temperature pill on waking at least 3 hours prior to scheduled boat transit on the Main Support Vessel. All external sensors and pre-cognitive tests were instrumented following the morning/afternoon brief in a warm room below deck. Cold weather clothing was donned in a partially heated boat hanger prior to moving to the open deck. All boat transits commenced from craft that were lowered into the water from the deck of the support vessel and participants climbed down ladders to board. All data was recorded off-line on data loggers and downloaded on their return.
Temperature
Core body temperature was recorded using a telemetric core temperature pill (eCelsius performance capsule, BodyCAP, France, accuracy ±0.2°C, resolution 0.01°C) that was activated and consumed at least 3 hours preceding a boat transit. Participants were required to wear a wrist band to indicate the risk of Magnetic Resonance Imaging from the time of the first consumption and for 3 days following the last pill consumption. Core body temperature data was downloaded using a performance monitor (eViewer Performance monitor, Equivital, UK) held close to the abdominal region. Skin temperature was recorded in 12 sites, with 8 sites in accordance with BS EN ISO 9886 [13] using a combination of both wired (Grant Thermistors, Grant Instruments Ltd., UK) and wireless iButton skin thermistors (iButtons, Maxim Integrated Inc., USA). Finger, hand, foot and toe sites were also recorded with wired thermistors due to their lower profile and an Eltek data logger (Gen II, Eltek, UK, accuracy ±0.4°C, resolution 0.2°C) used to record the data. The data logger with connected wires was placed in a waist pouch and placed around the participant’s waist on top of their base layers but under their outerwear. The other eight sights (forehead, neck, shoulder, upper arm, lower arm, thigh and calf) were measured with iButtons (accuracy ±1°C, resolution 0.125°C), with all thermistors secured to the skin using medical tape. All temperature sensors were calibrated and verified by the manufacturer prior to purchase. Participants did not go outside the vessel onto the open deck prior to being instrumented or wearing their outerwear due to the cold environmental conditions. Skin and core temperature were measured once every minute to accommodate extended transit durations and limitations with data storage. Ambient conditions were also sourced from the local weather station in Halifax due to partial data loss from the external iButton.
Heart rate
Heart rate (HR) was recorded using a chest strap (H10, Polar, Finland) and the data was logged using a smart watch (Fenix 6, Garmin, US) placed in a waist pouch under their outer jacket. Heart rate was sampled every second and averaged once per minute.
Perceptual scales
Thermal Sensation and Thermal Comfort were measured on separate scales, pre- and post-transit. Participants were shown the scales by the researchers and asked to rate their thermal sensation, ranging from “Very Hot” to “Very Cold” and their thermal comfort, ranging from “Very Comfortable” to “Very Uncomfortable” (Figure 4).
Figure 4.
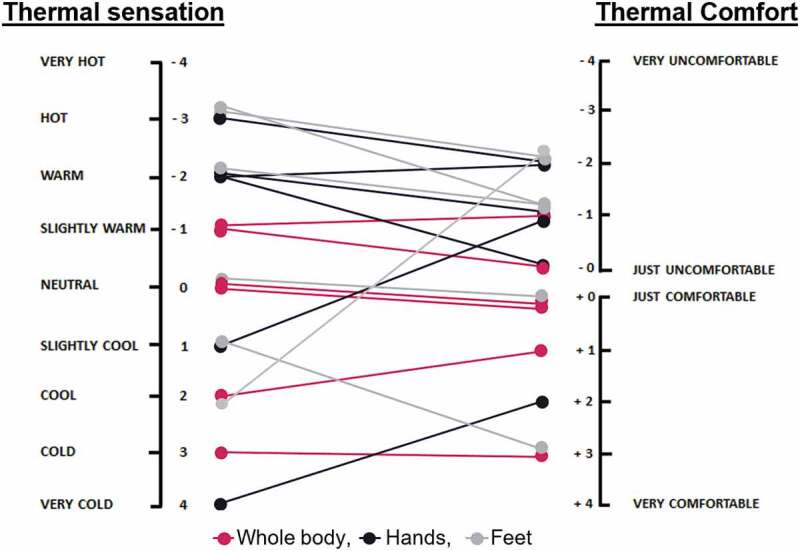
Individual thermal sensation and comfort scores for whole body, hands and feet following the cold weather sea transits. Data comprised from transit 1–3 cold weather transits across five participants with repeat scores for P3. Subjective scale data were not collected from transit four or P4 during transit three due to access to participants.
Cognitive measures
Two cognitive tasks, “Speed” and “Stroop”, were used to assess the effects of exposure to cold on reaction time and selective attention, respectively. These tasks were performed on an iPad® using the application suite “BrainBaseline”. During the Speed test, participants held the iPad® with two hands and selected one of the “hit me” buttons as soon as a coloured circle appeared in the middle of the screen. Two buttons were present on either side of the touchscreen and only one button was required to be pressed allowing participants to either use their dominant hand or alternate. The Stroop task presented participants with a word in the middle of the screen and they were required to select the correct button which related to the ink colour of the word as quickly and as accurately as possible. To make a selection, participants held the iPad in both hands and used their thumbs to select from four buttons labelled “R” for the colour red, “G” for green, “B” for Blue and “Y” for yellow on the side of the screen. The words varied between neutral (non coloured words), e.g dog and colour words that either matched or conflicted with their ink colour. Participants completed each task twice as a familiarisation the day before their first transit to reduce the training effect, this task was performed in training mode and the data were not recorded. The pre-transit Speed and Stroop tests were performed below deck without gloves using the digits to make the touchscreen selection. The tests were repeated within 10 min of returning to the Support Vessel in the partially heated hanger. Tests were completed in the hanger to reduce the rewarming effects and to allow the participants to remain in their outdoor clothing to reduce the time between cold exposure and performing the tests.
Data analysis
Due to the low sample size, variable transit duration and environmental conditions only descriptive statistics have been presented. Mean and standard deviation as well as the visual representations were calculated and depicted using Microsoft Excel.
Results
The mean environmental conditions in Halifax, Nova Scotia, during data collection were (mean ±1 standard deviation); air temperature −3 ± 5°C, relative humidity 67 ± 22%, wind speed 22 ± 7 km.h−1 and wind chill index −9 ± 6°C (Table 3) according to the local weather station. This placed the conditions on 2 to 4 on the Beaufort wind scale [14]. A total of 31 hours of exposure data were recorded across four boat transits and a combination of six participants.
Table 3.
Environmental conditions during boat transits from the local weather station.
| Time (min) | Temperature (°C) | Relative humidity (%) | Wind speed (km.h−1) | Wind chill (°C) | |
|---|---|---|---|---|---|
| Transit 1 (n=1) | 191 | −5.5 ± 1.1 | 37.8 ± 3.3 | 11.2 ± 2.9 | −10.0 ± 1.9 |
| Transit 2 (n=2) | 179 | 1.2 ± 1.4 | 97.5 ± 0.6 | 26.0 ± 2.4 | −4.5 ± 1.9 |
| Transit 3 (n=4) | 242 | 0.9 ± 2.0 | 77.7 ± 4.1 | 27.2 ± 4.1 | −4.5 ± 2.7 |
| Transit 4 (n=2) | 174 | −10.5 ± 1.6 | 59.3 ± 3.4 | 25.0 ± 2.6 | −19.3 ± 2.1 |
| Average | 197 | −3.1 ± 5.0 | 67.5 ± 22.4 | 22.3 ± 7.4 | −9.1 ± 6.2 |
*Note: Mean ± SD.
Physiological and perceptual data
Core body temperature
The overall core body temperature tended to increase at the beginning of the transits and reduce towards the end, with all staying above the ≤35°C hypothermia definition (Figure 1). Participant 4 recorded the lowest core temperature of 36.2°C 14 min into transit 4 (pink line in Figure 1). Participant 4 also tended to record the lowest core temperature across all of their transits (T3, T4 and T5) compared to the other participants and at times their changes in the core temperature were greater compared to the other participants. Participant 1 recorded the largest peak in core body temperature of 39.1°C, 50 min into transit 3 which was a 1.7°C increase compared to their starting temperature.
Figure 1.
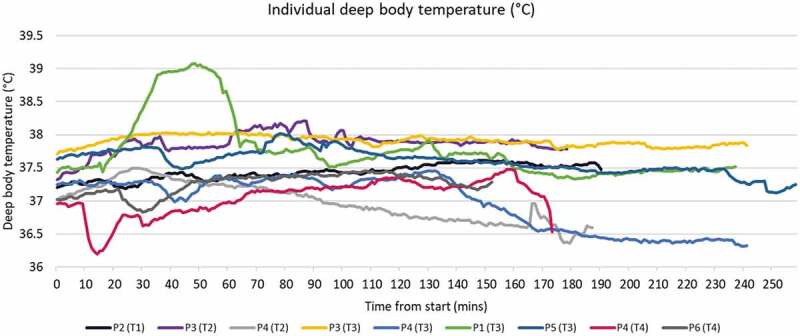
Individual core body temperature. Note: P=participant, T=transit.
Skin temperatures
Generally, skin temperature tended to fluctuate the most in the distal locations; fingers, hands, toes and feet compared to the torso, thigh and arm. The fingers and hands showed the greatest level of fluctuation, whereas the toes and feet tended to be more consistent. Despite the feet and toes being sheltered and the temperature more consistent than the hands, they tended to demonstrate gradual decline during the course of a transit (Figure 2). The forehead location was reasonably consistent and tended to be maintained during the majority of transits except during transit 4 when the wind chill index was at its lowest average temperature. The mean forehead temperature for transit 4 (n=2) was 25 ± 6°C with lows of 12°C.
Figure 2.
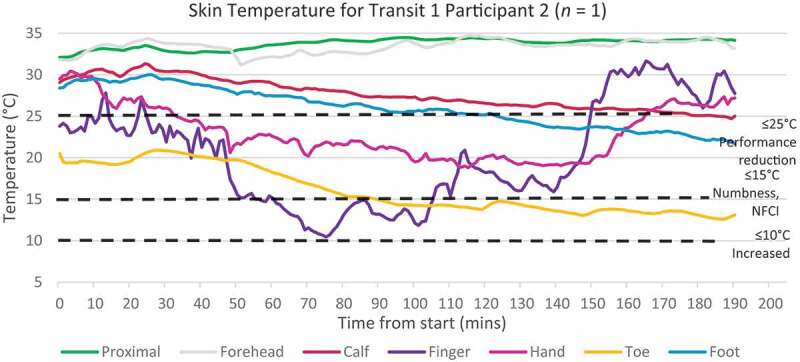
Example of skin temperature during transit 1. Note: Proximal includes, chest, back, neck, thigh, upper arm and lower arm.
Distal skin temperatures (fingers and toes) ≤25°C have been found to cause minor performance impairments. Skin temperatures <15°C are considered to be the threshold for NFCI risk due to the sharp decrease in finger dexterity and maximal vasoconstriction [6, 15]. The “hunters response” occurs at ≤10°C which is a protective mechanism where vasoconstriction remains but with intermittent cold induced vasodilation; however, there is a large inter-individual variability [16] and this lower temperature further increases the risk of NFCI. When combining all skin temperature data across all four sea transits, the percentage of total time spent below 25°C for the finger and toes was 77% and 68%, respectively (Table 4). 1% and 0.2% respectively of the transit time.
Table 4.
Total number of minutes spent within each temperature band across all participants and all four exercises.
| Forehead | Neck | Chest | Back | Upper arm | Lower arm | Thigh | Calf | Hand | Finger | Foot | Toe | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 25–15.1°C | 217 | 0 | 0 | 0 | 0 | 0 | 175 | 490 | 945 | 909 | 566 | 932 |
| 15–10.1°C | 11 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 144 | 474 | 0 | 330 |
| ≤10°C | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 15 | 21 | 0 | 5 |
| Total (min) | 228 | 0 | 0 | 0 | 0 | 0 | 175 | 490 | 1119 | 1425 | 566 | 1272 |
Heart rate
Average heart rate during transit 1–3 tended to be higher at the start and be at its lowest towards the end of the transit, with heart rate during transit 4 tending to increase as the transit continued with a peak of 144 bpm (Figure 3). Transit 1, which only had one participant had the lowest average heart rate of 74 bpm.
Figure 3.
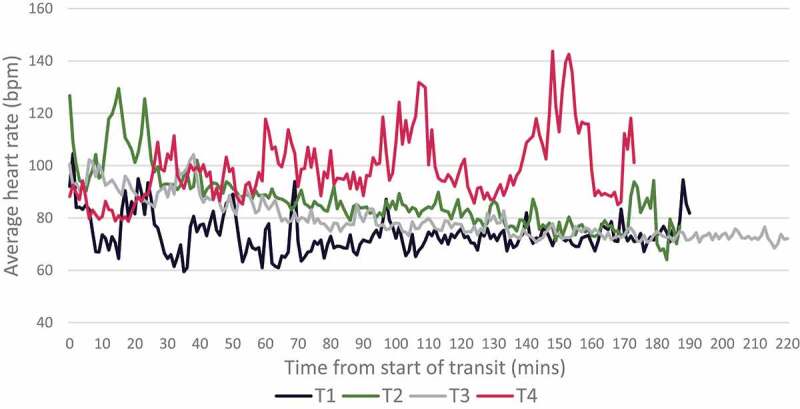
Average heart rate across each sea transit. Transit 1 (T1) n=1, Ttransit 2 (T2) n=2, transit 3 (T3) n=4, transit 4 (T4) n=2. Data were averaged between transits to demonstrate the overall trend.
Thermal sensation and comfort
Whole-body thermal sensation following a cold weather sea transit ranged from slightly warm to cold, and thermal comfort remained largely within the comfortable range, with one participant reporting that they felt slightly uncomfortable from feeling too warm (Figure 4). Hand thermal sensation had a greater spread of scores ranging from very cold to hot. Only two participants reported that their hands felt colder than neutral following sea transit with one reporting that they felt marginally uncomfortable (−1) and the other quite comfortable (+2). Foot thermal sensation was mostly rated as neutral to hot following sea transit and this feeling tended to be rated as uncomfortable. One participant reported that their feet were cool and quite uncomfortable (−2) on the thermal comfort scale.
Cognitive test data
Group mean speed task results suggest that reaction time was largely unaffected following sea transits with cold weather exposure (pre-mean reaction time; 287 ± 49 ms, post-mean reaction time 328 ± 35 ms) as the change was within the variation of the data. Visual inspection of individual data for the Speed task when presented as individual transits from P1, P2, P5, P6 and combining transits from P3 and P4 indicated that performance was not consistent between participants. Figure 5, indicates that P1, P2 and P6 reaction times remained relatively consistent, whereas P3 and P4 reaction times showed a marked decline following cold exposure.
Figure 5.
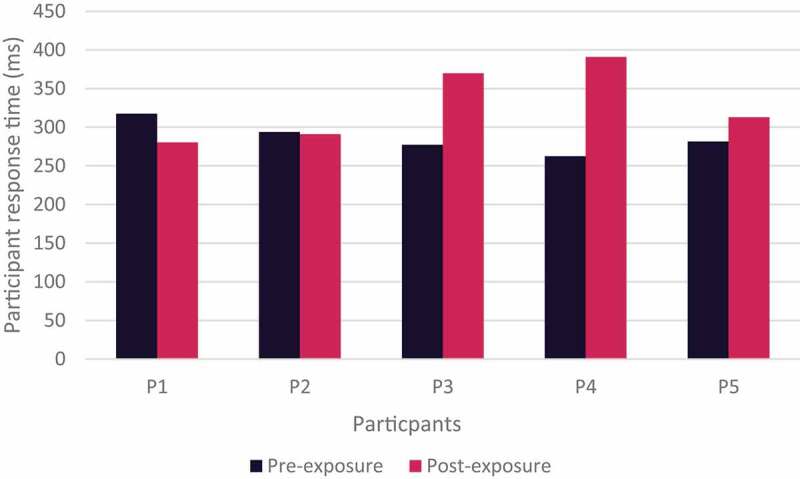
Individual reaction time during speed task pre- and post- sea transit.
Group mean Stroop performance data suggested that response time remained overall relatively consistent between pre- and post-cold weather sea transit (pre-mean response time; 825 ± 265 ms, post-mean reaction time 874 ± 299 ms). Stroop performance data when presented as individual transits from P1, P2, P5 and P6 and combining transits from P3 and P4 indicated that response time between pre- and post-transits remained similar following cold exposure (Figure 6). However, there was variance in the data which when combined with a small sample size, it is difficult to determine meaningful change.
Figure 6.
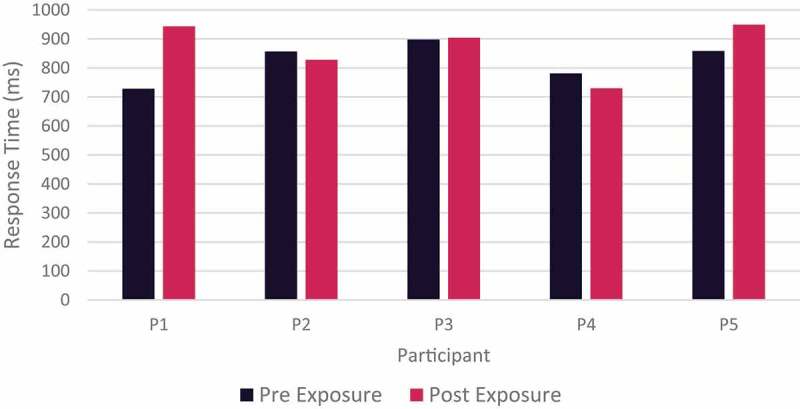
Individual participants response time during Stroop task by participant pre- and post- cold weather exposure.
Discussion
This preliminary study reported real-time skin and core body temperature of six personnel undertaking their dive support role in conditions with a wind chill index from −19.3 to −4.5°C. A key finding is that instrumentation and data collection did not hinder training objectives and was minimally invasive for personnel, demonstrating that it is possible to record core body, skin temperature, heart rate, subjective scales and conduct short cognitive tests in a field and training environment with this population. The trend for core temperature to increase initially can be partly explained by a higher metabolic activity at the beginning of the sea transits as indicated by a moderately elevated heart rate, and an average downward metabolic trend as the sea transit continued. Anecdotally, on the return journeys the wind direction was reported to be less favourable as they moved up wind, increasing the effect of wind chill. During transit 4 the lowest core body temperature was recorded by participant 4, they also had a marked reduction in their reaction time despite the participant wearing the greatest amount of layered clothing and having an average heart rate of 103 bpm for 174 min. Participant 1, who recorded the largest increase in core body temperature, had a heart rate that was slightly elevated at the beginning of the transit (average of 97 bpm for the first 30 min), but they also reported taking a nicotine pouch placed under the lip prior to the transit which may have contributed to the rise in body temperature through an acute increase in metabolic rate [17]. Specific task and behavioural observations were not possible during the study and therefore confounding effects of food, drink ingestion, adjustment of clothing layers and position on the boat all could have influenced core body temperature. Similarly, skin temperature was likely influenced by the variability in environmental conditions, exposure to wind chill, differences in physical tasks, clothing choice, body composition and size. The fingers and hands showed a greater level of fluctuation compared to the feet and toes which is likely explained by the feet being sheltered from wind chill within the boat and the participants all wearing wind and water resistant boots/shoes. Conversely, there was higher variability in the level of reported hand protection (n=2 reported no gloves, n=2 thin gloves, n=2 thick gloves, n=2 mitten/gloves), and the hands and fingers having a higher level of wind exposure compared to the feet and toes. While the feet and toes were reasonably sheltered, this didn’t stop a gradual and steady decline in skin temperature increasing the risk of cold injury on longer duration transits. During the coldest transit conditions (T4), there was a risk at the forehead of tissue damage due to very low skin temperatures [6], highlighting the importance of protecting all areas of the body, especially where the skin is exposed. Finger and toes temperature were below 25°C for the majority of the time, this has been reported as causing minor performance impairments [15]. However, there was little change in their ability to use the iPad®s when completing the “Speed” and “Stroop” tests, and on only one occasion did a participant report that their hands were very cold and their feet slightly cool on the thermal sensation scale. Participants 3 and 4 had a marked trend for their average post-transit Speed scores to be slower in comparison to their pre-scores. Only P4 had a marked lower core temperature compared to the other participants but tended to report whole body, hand and foot sensation as neutral to warm with rating of comfort to uncomfortable. P3 tended to have the highest core temperature and therefore it is difficult to determine if there is a small effect as a result of the environmental exposure. The Stroop results were quite similar within participant regardless of transit with the largest trend for a reduction in performance in participant 1, they reported cool and uncomfortable feet with hands slightly cool and marginally uncomfortable, but they had a relatively warm core temperature. The difficulties with interpreting the results of the cognitive tests stem around two possible effects: the first being cold exposure and the second the result of cognitive fatigue from being in a dive supervisory role for an average of 197 min. Baseline data in a temperate climate would assist with future interpretation in this research population. The majority of the reports of discomfort during transits were related to feeling too warm or hot as participants were asked to recall how they felt overall for the duration and not how they felt at the end of the transit. Perhaps in future it would be beneficial to obtain thermal sensation and comfort scores during boat transit as well as immediately post-transit, while still in the outdoor environment. It is important to note that the cognitive tests were not completed in a standardised environment or at the same time of day and therefore noise, distraction and circadian variations were not controlled and could have confounded the results.
Conclusion
Overall, despite participants being exposed to cold environmental conditions with Force 2 to 4 on the Beaufort wind scale, the participants were well prepared with personal protective equipment and their physiological responses were able to mitigate the risk of large changes in core body temperature. However, on an individual basis and during the colder conditions, improvements could be made to mitigate potential performance decrements and reduce the risk of extremity injury for the hands, fingers and toes. This report also highlighted large inter-individual variation, with certain participants being at higher risk than others and suggests that layered clothing particularly when sedentary should be considered on an individual basis. Conducting instrumented cold weather field research within a military exercise is likely to result in small sample sizes and therefore we would like to encourage other nations to consider creating a collaborative database to allow method and data sharing. Perhaps in future it would be beneficial to have the capability to be able to observe live deep body temperature as well as finger and toe temperature in order to prevent injury and enable prompt intervention during cold exposure. This population would also benefit from longer-term surveillance regarding NFCI and clothing choice due to their repeated exposure to cold temperatures in the extremities. Finally, improvements to field thermistors, particularly on distal locations to eliminate wires and improve waterproofing would assist with instrumentation and participant encumbrance.
Acknowledgments
This work was supported by the UK Ministry of Defence.
Funding Statement
The work was supported by the Ministry of Defence.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- [1].Pilcher JJ, Nadler E, Busch C.. Effects of hot and cold temperature exposure on performance: a meta-analytic review. Ergonomics. 2002;45(10):682–9. [DOI] [PubMed] [Google Scholar]
- [2].Lieberman H, Castellani J, Young A. Cognitive function and mood during acute cold stress after extended military training and recovery. Aviat space environ med. 2009;80(7):629–636. [DOI] [PubMed] [Google Scholar]
- [3].Tikuisis P, Keefe AA. Effects of cold strain on simulated sentry duty and marksmanship. Aviat space environ med. 2007;78(4):399–407. [PubMed] [Google Scholar]
- [4].Heil K, Thomas R, Robertson G, et al. Freezing and non-freezing cold weather injuries: a systematic review. Br Med Bull. 2016;117(1):79–93. [DOI] [PubMed] [Google Scholar]
- [5].Heil K, Oakley E, Wood A. British Military freezing cold injuries: a 13-year review. J R Army Med Corps. 2016;162(6):413–418. [DOI] [PubMed] [Google Scholar]
- [6].Parsons K. Human thermal environments: the effects of hot, moderate, and cold environments on human health, comfort and performance. Florida, US: CRC Press; 2007. [Google Scholar]
- [7].Ungley C, Channell G, Richards R. The immersion foot syndrome. Br J Surg. 1945;33(129):17–31. [DOI] [PubMed] [Google Scholar]
- [8].Daanen H, Van Der Struijs N. Resistance index of frostbite as a predictor of cold injury in arctic operations. Aviat space environ med. 2005;76(12):1119–1122. [PubMed] [Google Scholar]
- [9].Rav-Acha M, Heled Y, Moran D. Cold injuries among Israeli soldiers operating and training in a semiarid zone: a 10-year review. Mil Med. 2004;169(9):702–706. [DOI] [PubMed] [Google Scholar]
- [10].Falla M, Micarelli A, Hufner K, et al. The Effect of Cold Exposure on Cognitive Performance in Healthy Adults: A Systematic Review. International Journal of Environmental Research and Public Health. 2021;18(18):9725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Harris D, Vine S, Wilson S M, et al. HS1.002 Application of novel techniques to enhance cognitive performance; 2020. (Hum Social Sci Research Capability; no. O-HSSRC-1.002-008). [Google Scholar]
- [12].Yang L, Wu J, Hu Z, et al. Effects of workload on human cognitive performance of exposure to extremely cold environment. Physiology & Behaviour. 2021;230:113296. DOI: 10.1016/2021 [DOI] [PubMed] [Google Scholar]
- [13].BS EN ISO 9886 . Ergonomics — Evaluation of thermal strain by physiological measurements. 2004;3. [Google Scholar]
- [14].Organization WM. The Beaufort scale of wind force: (Technical and Operational Aspects). Geneva: WMO, Commission for Maritime Meteorology; 1970. [Google Scholar]
- [15].Cheung S, Montie D, W M, et al. Changes in manual dexterity following short-term hand and forearm immersion in 10 degrees C water. Aviat space environ med. 2003;74(9):990–993. [PubMed] [Google Scholar]
- [16].Imray C, Grieve A, Dhillon S. Cold damage to the extremities: frostbite and non-freezing cold injuries. Postgrad Med J. 2009;85(1007):481–488. [DOI] [PubMed] [Google Scholar]
- [17].Perkins K, Epstein L, Stiller R, et al. Acute effects of nicotine on resting metabolic rate in cigarette smokers. Am J Clin Nutr. 1989;50(3):545–550. [DOI] [PubMed] [Google Scholar]