

Abstract
Available assessments of patient nutrition knowledge and carbohydrate counting ability are lengthy. This article reports on a study to implement and validate a series of brief nutrition quizzes of varying difficulty for use in pediatric type 1 diabetes. Among 129 youth with type 1 diabetes, participants completed an average of 2.4 ± 1 of the six quizzes, with a median score of 4.7 of 5. Higher quiz scores were associated with lower A1C (P <0.001), higher parental education (P = 0.02), and higher income (P = 0.01). Such quizzes can help to identify knowledge gaps and provide opportunities for education, which may improve glycemic outcomes in youth with type 1 diabetes.
One of the key elements of type 1 diabetes management is carbohydrate counting to determine prandial insulin doses (1,2). This practice is based on the premise that, of all macronutrients, carbohydrates have the most significant impact on postprandial glucose levels (3). Postprandial glycemia is a major determinant of A1C, a measure of glycemic control that is linked to development of diabetes complications when elevated (4). Thus, carbohydrate counting is taught as a management intervention at the time of diabetes diagnosis. The benefits of carbohydrate counting include improved glycemic control (with lower A1C) (5), diabetes-specific quality of life, and coping ability in daily life (6,7).
Nutrition education and ongoing re-education that is age appropriate and engages the individual with diabetes in active learning is recommended (7,8). Furthermore, as youth with diabetes reach their adolescent years, it is important for them to independently master carbohydrate counting for their future independent diabetes management (1). Although many individuals self-report knowledge of and comfort with carbohydrate counting, there is no standardized method for determining the accuracy of these self-reports. While there have been several assessments developed to measure carbohydrate counting and general nutrition knowledge (9–12), adoption of these tools in clinical practice has been limited because they include a minimum of 19 items and can be time-consuming to administer in busy multidisciplinary diabetes clinics. The 78-item PedCarbQuiz (PCQ) is one such survey developed to assess knowledge of carbohydrate counting in youth with type 1 diabetes (9). Other, shorter quizzes such as the 23-item Nutrition Knowledge Survey (NKS) (10), the 19-item electronic NutraCarbQuiz (eNCQ) (11), and the 19-item Mercy What I Know About Diabetes (M-WIKAD) (12) have been implemented in research and clinical practice. Greater nutrition knowledge has been associated with better glycemic control in studies using these assessments, but longitudinal improvements in individual patients’ glycemic control have yet to be shown.
We developed, implemented, and validated six brief, five-question nutrition assessments with photos of commonly consumed foods to assess fundamental knowledge of carbohydrate counting and ability to calculate prandial insulin doses and to engage youth in nutrition education. These assessments covered three strata of content, ranging from fundamental to intermediate to advanced knowledge, and were administered by a dietitian in a diabetes clinic at multiple time points. The objective of this study was to measure improvements in nutrition knowledge and carbohydrate counting and determine their association with glycemic control in youth with type 1 diabetes.
Research Design and Methods
Study Participants
Pediatric participants who were 8–18 years of age, had type 1 diabetes, and were independent in their diabetes management as assessed by the diabetes team dietitian at an academic, multidisciplinary diabetes center were included in this study. From December 2018 through March 2020, nutrition quizzes were implemented in the diabetes clinic as part of a clinical practice improvement project and were administered by a dietitian at quarterly diabetes clinic visits (1). Youth were excluded if they did not have type 1 diabetes, did not use carbohydrate counting as part of their diabetes treatment regimen, or did not have an English-speaking family member in attendance with them at their clinic appointment. This study was approved by the institutional review board at Johns Hopkins Hospital according to the Declaration of Helsinki and included a waiver of consent.
Development of the Nutritional Quizzes
Six carbohydrate-counting quizzes were created and designed to cover three different levels of difficulty: fundamental, intermediate, and advanced. Each of the six quizzes contained a five-item pictorial carbohydrate counting assessment of common food products that youth in our practice reported eating (Supplementary Materials). The purpose of the quizzes was to assess degree of knowledge of carbohydrate counting and ability to calculate prandial insulin doses. The nutrition quiz design was based on guidelines for diabetes education in children and adolescents from the International Society for Pediatric and Adolescent Diabetes (13) and diabetes education best practices.
Fundamental, or beginner level, quizzes evaluated the ability to 1) recognize a serving size, 2) read and understand information from a nutrition label, 3) independently count carbohydrates in individual food items, 4) use an insulin-to-carbohydrate ratio for insulin dosing, and 5) count carbohydrates in various serving sizes. Intermediate-level quizzes also assessed the ability to 6) identify carbohydrates without a label, 7) calculate insulin based on grams of carbohydrates and blood glucose level, 8) estimate carbohydrate amounts with only pictorial images of whole meals, and 9) recognize different sources of carbohydrates. Advanced quizzes included criteria for evaluating proficiency in 10) insulin correction dose based on blood glucose level and 11) understanding how different sources of carbohydrates affect blood glucose.
Face validity was established by a multidisciplinary team consisting of pediatric endocrinologists and dietitians/certified diabetes care and education specialists. Internal consistency was measured using Cronbach α. The coefficient was calculated for each of the six quizzes based on initial responses. The results reflected overall good internal reliability, with standardized Cronbach α scores of 0.65–0.88: quiz 1 α = 0.75 (n = 23), quiz 2 α = 0.76 (n = 25), quiz 3 α = 0.88 (n = 21), quiz 4 α = 0.85 (n = 25), quiz 5 α = 0.65 (n = 26), and quiz 6 α = 0.67 (n = 14). To assess criterion validity, quiz scores were analyzed for associations with A1C and parental education level.
Quiz Administration and Scoring
At quarterly clinic visits, during which patients saw the dietitian, quizzes were administered on paper by the diabetes team dietitian. The number of quizzes given during the visit ranged from one to two and varied depending on the family’s time allowance, team’s request, and need for time to discuss other topics with the dietitian. The initial quiz level at the start of the study was determined at the recommendation of the physician, nurse, or dietitian based on the patient’s age and clinical history. Each correctly answered item contributed one point to the total raw score, for a maximum score of 5 for each quiz. No half points were awarded for partially correct answers. Participants were required to work independently, without assistance from the dietitian or a caregiver. However, the patient could ask the dietitian for clarification if they did not understand the questions posed in particular items. Carbohydrate calculating resources, including phone apps and websites, were allowed. In addition, patients using insulin pumps were allowed to use their pump to calculate insulin doses. Based on the dietitian’s recommendation, raw scores ≥4 were considered to be passing. Patients who passed a nutrition assessment could progress to the next level of quiz difficulty. Quiz responses were reviewed by patients and the dietitian together to identify knowledge gaps and provide education in those areas. The estimated time of quiz administration and completion by patient ranged from 10 to 15 minutes.
Demographic and Clinical Data
Demographic and clinical data were extracted from the electronic medical record system and included date of birth, sex, race, ethnicity, primary language, insurance status, diabetes type, date of diabetes diagnosis, age at diabetes diagnosis, duration of diabetes, type of insulin delivery, use of continuous glucose monitoring (CGM), clinic visit date, and A1C at clinic visits. Parental education and income level were self-reported from another overlapping study. Point-of-care A1C testing was performed at each clinic visit as part of routine care using the Afinion As100 Analyzer.
Statistical Analysis
Descriptive and summary statistics were used to describe the patient cohort, quiz scores, and clinical characteristics. Univariate regression analysis was used to assess the relationship between outcomes (quiz score and A1C) and participant characteristics. Comparison of groups was performed using t tests for continuous variables and χ2 tests for categorical variables. For patients who completed different quizzes at subsequent visits and for whom longitudinal data were captured, paired t tests were used to evaluate A1C before and after quiz implementation. Statistical analysis was performed using Stata, v. 15.1, statistical software. Statistical significance was assessed at the P <0.05 level.
Results
Clinical Characteristics of Participants
A total of 129 participants were included in this study, of whom 64 completed two or more successive quizzes. As shown in Table 1, the mean age of the cohort was 13.8 ± 2.7 years, 47% were female, 67% were non- Hispanic White, 21% were Black, and 4% were Hispanic. All patients had type 1 diabetes, with mean duration of diabetes of 5.3 ± 4.1 years and a mean A1C of 8.8 ± 2.0%. Of the participants, 20% had a diabetes duration <1 year, 72% were using CGM, and 67% used an insulin pump.
TABLE 1.
Participant Characteristics (N = 129)
| Characteristic | Value |
|---|---|
| Age, years | 13.8 ± 2.7 |
| Male sex | 69 (53) |
| Race/ethnicity White Black Hispanic Other |
86 (67) 27 (21) 5 (4) 11 (8) |
| Age at diabetes diagnosis, years | 8.9 ± 3.9 |
| Duration of diabetes, years | 5.3 ± 4.1 |
| Diabetes duration <1 year | 26 (20) |
| A1C, % | 8.8 ± 2.0 |
| Parental education (n = 106) High school/general education diploma Associate’s degree Undergraduate degree Postgraduate degree |
23 (21) 13 (12) 30 (28) 40 (38) |
| Income, $ (n = 95) <25,000 25,000–49,999 50,000–74,999 75,000–99,999 ≥100,000 DK/NA* |
6 (5) 15 (12) 14 (11) 9 (7) 51 (39) 34 (26) |
| Insulin delivery Multiple daily injections Insulin pump |
43 (33) 86 (67) |
| CGM use | 93 (72) |
| Mean number of quizzes completed | 2.4 ± 1.0 |
| Quiz score, median (interquartile range) | 4.67 (4–5) |
Data are n (%) or mean ± SD unless otherwise noted.
DK/NA stands for do not know or no answer, as some participants chose not to report this information.
Nutrition Assessment and Scoring
Participants completed an average of 2.4 ± 1 quizzes (range 1–5), with a median quiz score of 4.7 (interquartile range [IQR] 4–5). The mean time between quizzes for participants who completed more than one quiz at subsequent visits was ∼5 months, or 157.8 ± 74.2 days. Nutrition assessments were scored from 0 to 5, with a passing score of ≥4.
Nutrition Assessment and Relationship to Outcomes
The relationship between baseline quiz score and patient characteristics was analyzed for all 129 participants who completed at least one quiz, as shown in Table 2. Higher parental education levels and income ≥$50,000 were associated with a higher baseline quiz score (P = 0.02 and P = 0.014, respectively). Black race was associated with a lower quiz score (P <0.001). Age at diagnosis, duration of diabetes, mode of insulin delivery, and CGM use were not associated with quiz score. A lower A1C was associated with a higher first quiz score (P <0.001) and higher mean quiz scores (P = 0.001) (Figure 1).
TABLE 2.
Relationship of Participant Demographics and Clinical Characteristics With Baseline Nutrition Assessment Score (N = 129)
| Characteristic | β | P |
|---|---|---|
| First A1C | −0.152 | 0.000 |
| Age | 0.010 | 0.758 |
| Male sex | 0.141 | 0.416 |
| Race/ethnicity White Black Hispanic Other |
Reference −0.994 −0.298 −0.425 |
0.000 0.473 0.143 |
| Age at diagnosis | −0.005 | 0.829 |
| Diabetes duration | 0.002 | 0.932 |
| Parental education (n = 106) High school/general education diploma Higher education |
Reference 0.967 |
0.000 |
| Income* (n = 95) <$50,000 ≥$50,000 |
Reference 1.051 |
0.000 |
| Insulin delivery Multiple daily injections Insulin pump |
Reference 0.209 |
0.252 |
| CGM use | 0.151 | 0.434 |
Bold type indicates statistical significance.
Some participants chose not to report this information. β, regression coefficient.
FIGURE 1.
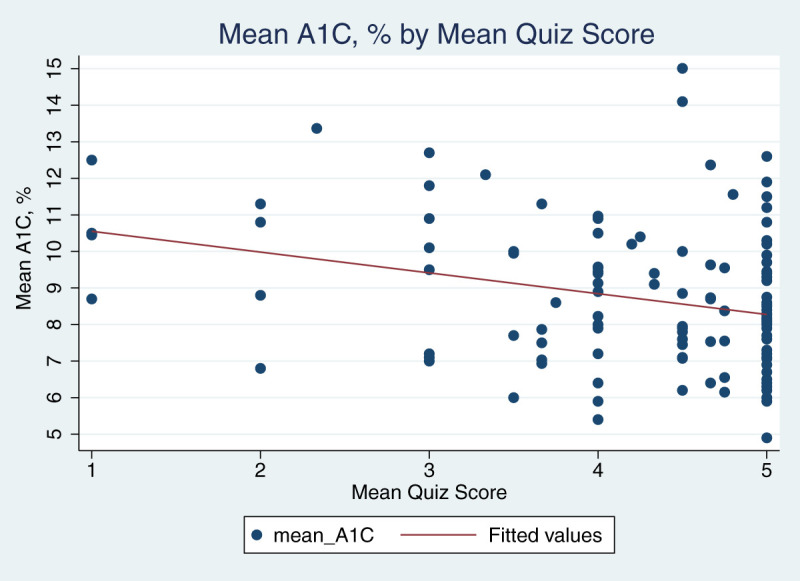
Relationship of mean A1C and mean quiz score (n = 129, P = 0.001). Circles = mean A1C, %; line = fitted values.
Participants with lower A1C values at the initial quiz administration had higher parental education and income (P <0.001 and P = 0.002, respectively), and Black race was associated with higher A1C (P <0.001). Insulin pump use was associated with lower A1C (P = 0.001). There was no association between the number of quizzes taken and A1C (P = 0.382) (Supplementary Table S1).
A total of 64 participants had longitudinal assessments, with different nutrition quizzes completed at consecutive clinic visits. This subset was similar in age, sex, race/ethnicity, diabetes duration, parental education, and income to the overall cohort. Using paired t tests, this group demonstrated a significant reduction in A1C from the initial quiz to the last quiz completed (9.2 vs. 8.7%, P <0.001), with a lower mean assessment score on the final quiz completed (4.5 [SD 1] vs. 3.9 [SD 1.2], P = 0.0017).
Discussion
Multidisciplinary diabetes care with continued nutrition education is recommended, and these brief, reliable, and interactive five-item nutrition assessments were feasible to implement in a time-efficient manner (10–12). Most patients scored well and, similar to prior studies, this study showed that higher quiz scores were associated with lower A1C levels (10–12). Participants who completed multiple assessments longitudinally at consecutive visits had a mean reduction in A1C.
Nutrition assessments for youth with type 1 diabetes range in length and number of questions and include the 78-item PCQ (9), 19-item eNCQ (11), 23-item NKS (10), and 19-item M-WIKAD (12). In contrast to these instruments, our nutrition quizzes were brief, with five questions each, making them quick and feasible to implement in a busy, multidisciplinary diabetes clinic setting. Reports using these other measures have shown that higher quiz scores are correlated with lower A1C levels and thus greater glycemic control (9–11). We showed similar results.
Furthermore, in patients who completed more than one nutrition assessment, we also observed a longitudinal reduction in A1C, suggesting that administration of nutrition quizzes as part of ongoing diabetes education may help to improve glycemic control. Although patients who took multiple quizzes may not have performed better on subsequent quizzes, these findings may have been the result of the increasing difficulty of intermediate- and advanced-level nutrition quizzes. Prior studies have posited that the positive effects of nutrition education may not last beyond 3 months (14). Therefore, the longitudinal aspect of re-education is crucial for continued optimization of diabetes management and glycemic control.
A notable characteristic in this study is its inclusion of a larger subset of minority patients compared with other studies that was reflective of our local population and the growing trend of minority youth with type 1 diabetes (15). We found that Black youth scored lower on the nutrition assessments and had higher A1C levels. Unfortunately, this finding is consistent with prior reports, demonstrating disparities in glycemic control, diabetes-related outcomes, and diabetes technology use (16–18).
Similar to other studies, we also found that youth with type 1 diabetes who had parents with a greater than high school education had lower A1C and more nutrition knowledge (9–11). Interestingly, some participants had suboptimal A1C levels despite having higher quiz scores, indicating that poor glycemic control was likely not the result of poor carbohydrate-counting skills or a lack of nutrition knowledge, but rather a lack of adherence to other diabetes recommendations and/or insulin administration.
There are varying practices regarding nutrition education for type 1 diabetes worldwide (6). A prior study demonstrated that, in the first year after diagnosis of type 1 diabetes, patients and their caregivers receive a total of 210 minutes of nutrition education, whereas in subsequent years, only 60% of patients receive nutrition education at least annually (6). In our practice, the dietitian sees each patient at least once per year, but, prior to implementation of the nutrition assessments, some reasons why patients may not have seen the dietitian included lack of time, no specific questions for the dietitian, self-reported comfort with carbohydrate counting, or concern about the cost of nutrition consultation.
Implementation of the brief nutrition assessments provided a new opportunity for the dietitian to assess each patient’s nutrition knowledge in an engaging manner. Often, when children are diagnosed with diabetes at a young age, their parents do most of the nutrition and diabetes management. These brief quizzes facilitate engagement with adolescents in the transition years and assess their independent knowledge of carbohydrate counting. The nutrition quizzes also provide insight for caregivers on their child’s carbohydrate-counting abilities and nutrition knowledge, allowing them to adjust their support to their child’s current needs. For the dietitians in diabetes clinic, it provided an opportunity to discuss advanced nutrition topics beyond carbohydrate counting, including the effects of different food components (e.g., fiber and protein) on blood glucose levels, glycemic index, new online carbohydrate calculation tools, nutrition apps, and advanced insulin pump functions that could help to optimize glycemic control.
A limitation of this study was that the choice of which quizzes to administer was subjective and based on providers’ and dietitian’s discretion and recommendation. Additionally, the nutrition assessments were developed based on typical patient-reported food selections in this community and may not be generalizable to other practice populations. Advanced-level quizzes (quizzes 5 and 6) also had lower Cronbach α scores, likely reflecting their increased difficulty; with more challenging questions, there was more variability in consistency of the responses. Finally, this study was implemented as a quality improvement project to assess nutrition and carbohydrate-counting knowledge and its relationship to glycemic control and thus could not directly determine the impact of the quizzes on A1C levels without a randomized controlled trial design.
Conclusion
Our findings suggest that implementing nutrition assessments as part of routine diabetes care may improve glycemic outcomes in youth with type 1 diabetes. Additionally, taking quizzes can be an engaging opportunity for patients to practice and improve their nutrition knowledge, while providing clinicians a means of identifying knowledge gaps and offering opportunities for point-of-care education. The brevity and range of difficulty of these nutrition assessments make them feasible for implementation in busy diabetes clinics, while also effectively providing continuing education opportunities for young people with type 1 diabetes.
Article Information
Duality of Interest
No potential conflicts of interest relevant to this article were reported.
Author Contributions
M.W. performed the research, collected and analyzed data, and contributed to writing the manuscript. T.L. performed the research, collected data, and contributed to writing the manuscript. M.T. designed the study, performed the research, collected data, and contributed to writing the manuscript. M.S. designed the study, performed the research, and collected data. L.P. and E.A.B. analyzed the data. R.M.W. designed the study, performed the research, collected and analyzed data, and contributed to writing the manuscript. All authors read and approved the final manuscript. R.M.W. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Prior Presentation
This research was presented in abstract form at the American Diabetes Association’s virtual 80th Scientific Sessions, 12–16 June 2020.
Footnotes
M.W. and T.L. are co-first authors.
This article contains supplementary material online at https://doi.org/10.2337/figshare.19757014.
References
- 1. American Diabetes Association . 13. Children and adolescents: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020;43(Suppl. 1):S163–S182 [DOI] [PubMed] [Google Scholar]
- 2. Kawamura T. The importance of carbohydrate counting in the treatment of children with diabetes. Pediatr Diabetes 2007;8(Suppl. 6):57–62 [DOI] [PubMed] [Google Scholar]
- 3. Wolever TM, Bolognesi C. Source and amount of carbohydrate affect postprandial glucose and insulin in normal subjects. J Nutr 1996;126:2798–2806 [DOI] [PubMed] [Google Scholar]
- 4. Diabetes Control and Complications Trial Research Group; Nathan DM, Genuth S, Lachin J, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;329:977–986 [DOI] [PubMed] [Google Scholar]
- 5. Deeb A, Al Hajeri A, Alhmoudi I, Nagelkerke N. Accurate carbohydrate counting is an important determinant of postprandial glycemia in children and adolescents with type 1 diabetes on insulin pump therapy. J Diabetes Sci Technol 2017;11:753–758 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Alonso GT, Fink K, Maffeis C, et al. Variation in nutrition education practices in SWEET pediatric diabetes centers: an international comparison. Pediatr Diabetes 2021;22:215–220 [DOI] [PubMed] [Google Scholar]
- 7. Smart CE, Annan F, Higgins LA, Jelleryd E, Lopez M, Acerini CL. ISPAD Clinical Practice Consensus Guidelines 2018: Nutritional management in children and adolescents with diabetes. Pediatr Diabetes 2018;19(Suppl. 27):136–154 [DOI] [PubMed] [Google Scholar]
- 8. Knowles J, Waller H, Eiser C, et al. The development of an innovative education curriculum for 11-16 yr old children with type 1 diabetes mellitus (T1DM). Pediatr Diabetes 2006;7:322–328 [DOI] [PubMed] [Google Scholar]
- 9. Koontz MB, Cuttler L, Palmert MR, et al. Development and validation of a questionnaire to assess carbohydrate and insulin-dosing knowledge in youth with type 1 diabetes. Diabetes Care 2010;33:457–462 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Rovner AJ, Nansel TR, Mehta SN, Higgins LA, Haynie DL, Laffel LM. Development and validation of the type 1 diabetes nutrition knowledge survey. Diabetes Care 2012;35:1643–1647 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Marker AM, Noser AE, Knecht N, Clements MA, Patton SR. A time-friendly, feasible measure of nutrition knowledge in type 1 diabetes: The Electronic Nutrition and Carbohydrate Counting Quiz (eNCQ). J Diabetes Sci Technol 2019;13:68–74 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Tsai S, Patton S, DeLurgio S, et al. A new paediatric diabetes knowledge test: M-WIKAD development and factor analysis. Eur Endocrinol 2019;15:1–5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Phelan H, Lange K, Cengiz E, et al. ISPAD Clinical Practice Consensus Guidelines 2018: Diabetes education in children and adolescents. Pediatr Diabetes 2018;19(Suppl. 27):75–83 [DOI] [PubMed] [Google Scholar]
- 14. Dłużniak-Gołaska K, Panczyk M, Szypowska A, Sińska B, Szostak-Węgierek D. Interactive nutrition education is more effective in terms of improved levels of glycated hemoglobin in adolescent patients with poorly controlled type 1 diabetes: a randomized study. Diabetes Metab Syndr Obes 2019;12:2619–2631 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Dabelea D, Mayer-Davis EJ, Saydah S, et al.; SEARCH for Diabetes in Youth Study . Prevalence of type 1 and type 2 diabetes among children and adolescents from 2001 to 2009. JAMA 2014;311:1778–1786 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Kahkoska AR, Shay CM, Crandell J, et al. Association of race and ethnicity with glycemic control and hemoglobin A1c levels in youth with type 1 diabetes. JAMA Netw Open 2018;1:e181851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Valenzuela JM, Seid M, Waitzfelder B, et al.; SEARCH for Diabetes in Youth Study Group . Prevalence of and disparities in barriers to care experienced by youth with type 1 diabetes. J Pediatr 2014;164:1369–75.e1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Willi SM, Miller KM, DiMeglio LA, et al.; T1D Exchange Clinic Network . Racial-ethnic disparities in management and outcomes among children with type 1 diabetes. Pediatrics 2015;135:424–434 [DOI] [PMC free article] [PubMed] [Google Scholar]