

Our group has reported that cardiac echinococcosis can mimic many other diseases in its clinical presentation (for example, atrial myxoma, ruptured sinus of Valsalva aneurysm, left ventricular aneurysm, pericardial tamponade, and subdiaphragmatic abscess). 1 In this paper, we present a very rare manifestation of echinococcosis that mimics a left ventricular tumor; we think that this new example may be helpful in the differential diagnosis of cardiac tumors and cysts.
A 9-year-old boy was admitted to another hospital with symptoms of dyspnea (most especially orthopnea), fever, and syncope. Physical examination revealed tachycardia, distended jugular veins, and 5-cm hepatomegaly. In the echocardiographic examination, pericardial tamponade and a myocardial tumoral mass were visualized. While at that hospital, the patient underwent pericardiocentesis. He was then referred to our center.
At our center, 2-dimensional transthoracic echocardiography revealed a 13-mm effusion at the lateral margin of the intrapericardial cavity, a 9-mm effusion near the inferior surface of the heart, a 5-mm effusion near the posterior surface, and minimal effusion near the anterior surface. A 30- × 30-mm tumoral mass at the posterior wall of the left ventricle bulged towards the pericardial cavity (Fig. 1). The tissue of this mass appeared to be healthy myocardium. Computerized tomography revealed the same mass at the posterior of the left ventricle. We performed cardiac magnetic resonance imaging, which revealed a left ventricular tumor at the posterior wall. Dimensions of the mass were 3 × 4 × 3 cm (Fig. 2).
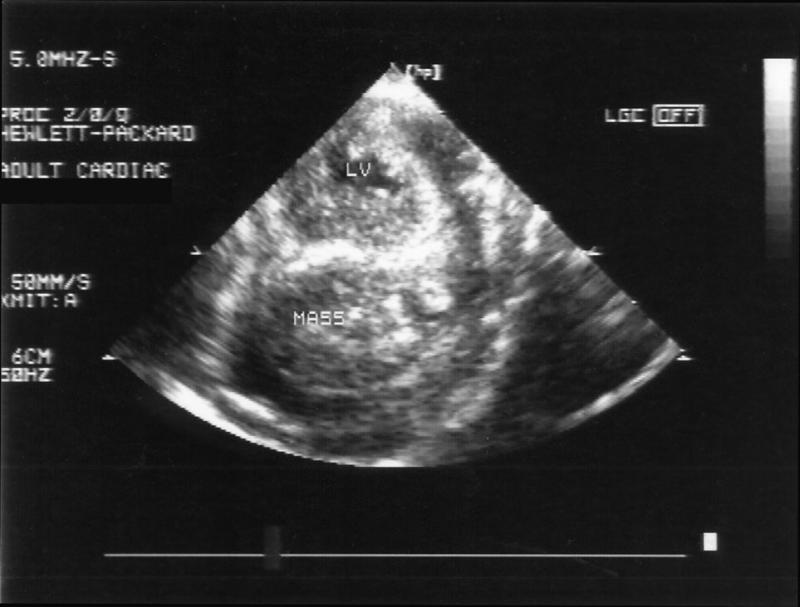
Fig. 1 Short-axis transthoracic echocardiographic view showing the tumoral mass (MASS) at the posterolateral wall of the left ventricle.
LV = left ventricular cavity
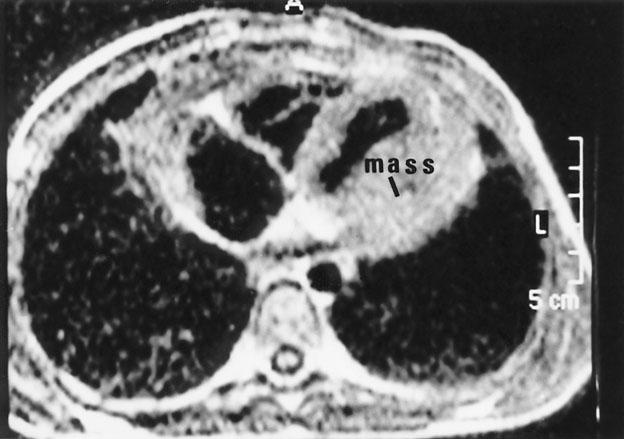
Fig. 2 Magnetic resonance imaging shows a tumor at the posterior wall of the left ventricle.
Due to a positive hydatid hemagglutination test and eosinophilia, we suspected cardiac echinococcosis and decided to operate. We approached via a median sternotomy; after dissecting pericardial adhesions, we found, at the posterolateral surface of the heart, a 3- × 4-cm yellowish-white mass surrounded by muscle tissue. Intraoperative transesophageal and intraoperative surface (epicardial) echocardiography were negative for cystic formation, but our past experience indicated the probability of hydatid cyst. This suspicion was confirmed when fine-needle aspiration revealed grayish-white viscous material. We opened the cavity and removed the cyst.
The patient was discharged on the standard regimen of oral albendazole therapy and was doing well at routine 2- and 6-month follow-up visits.
The kinetic pressure of the heart increases the tension around the cyst, restricting its enlargement. A cyst that contains relatively little liquid and relatively more scoleces gives the appearance of a solid mass upon imaging. Moreover, other factors can lead to a false-positive diagnosis of neoplastic mass upon imaging: in time, cysts under high kinetic pressure lose their viability and the liquid becomes more viscous; and the margins of the cyst can appear blurred because the surrounding muscle tissue has become more vascular in response to increased pressure. Klodas and colleagues 2 have also reported an extraordinary case involving a cardiac echinococcal lesion that was neither echolucent nor multiseptated upon echo-cardiography. A few cases of cardiac echinococcosis mimicking an intra-atrial tumoral mass (atrial myxoma) have been reported. 1,3,4
In our patient, computed tomography, magnetic resonance imaging, transthoracic echocardiography, and intraoperative transesophageal echocardiography were all misleading. Needle aspiration was necessary to determine the cystic nature of the mass.
In conclusion, cardiac echinococcosis is an uncommon but serious condition that should be remembered in the differential diagnosis of cardiac tumors.
Footnotes
Address for reprints: Dr. Cemal Levent Birincioglu, Cardiovascular Surgery Clinic, Türkiye Yüksek Ihtisas Hospital, 06100 Sihhiye, Ankara, Turkey
References
- 1.Birincioglu CL, Bardakci H, Kucuker SA, Ulus AT, Arda K, Yamak B, Tasdemir O. A clinical dilemma: cardiac and pericardiac echinococcosis. Ann Thorac Surg 1999;68:1290–4. [DOI] [PubMed]
- 2.Klodas E, Roger VL, Miller FA Jr, Utz JP, Danielson GK, Edwards WD. Cardiac echinococcosis: case report of unusual echocardiographic appearance. Mayo Clin Proc 1995; 70:657-61. [DOI] [PubMed]
- 3.Dutka DP, Morris GK. Intracardiac thrombus formation in association with hydatid disease. Eur Heart J 1990;11: 1120-3. [DOI] [PubMed]
- 4.Jeridi G, Boughzala E, Hajri S, Hediji A, Ammar H. Complicated hydatid cyst of the right atrium simulating myxoma of the tricuspid valve [in French]. Ann Cardiol Angeiol (Paris) 1997;46:159-62. [PubMed]