

Abstract
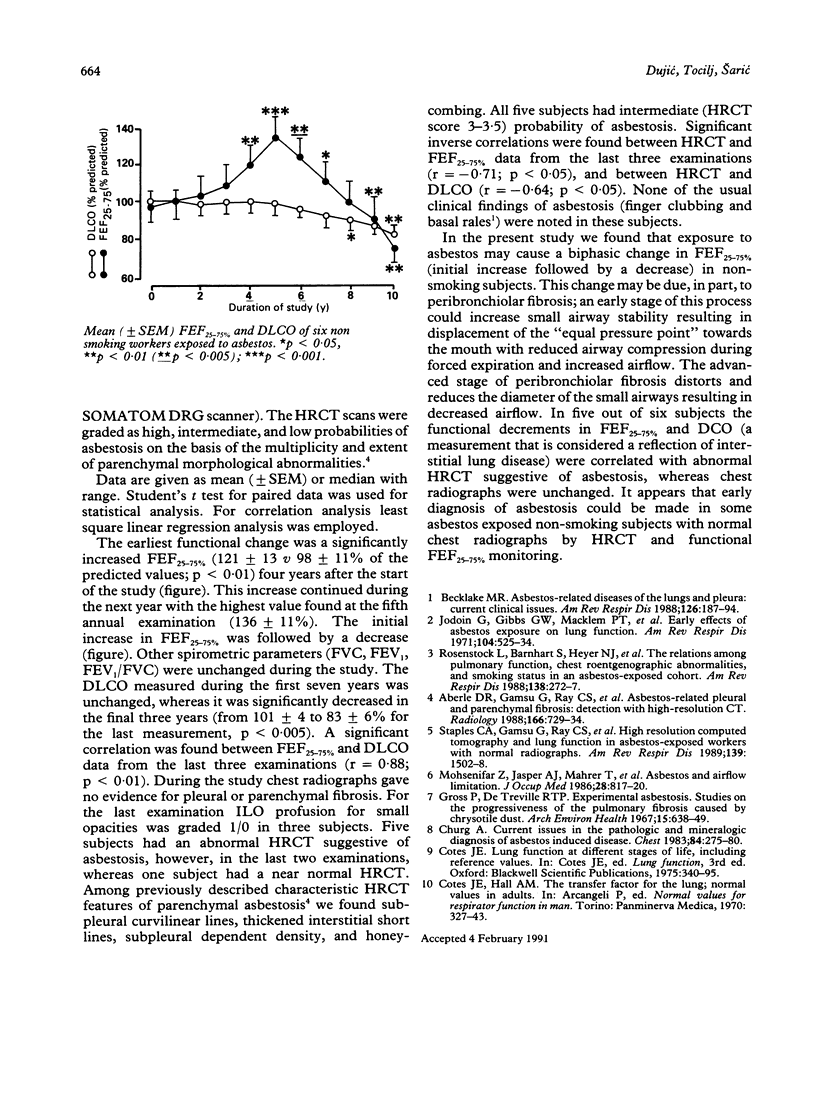
Ten years of lung function and radiological findings in six non-smoking asbestos exposed subjects who had increased mid-expiratory flow rate (FEF 25-75%) as the only functional abnormality were prospectively analysed. A biphasic change in FEF25-75% was noted. It initially increased up to the fifth year, and then a decrease was seen. In the final three years of the study, FEF25-75% reduction correlated well with a decrease in pulmonary capacity for CO (DLCO). During that time high resolution computed tomography (HRCT) probability scores correlated inversely with FEF25-75% and with DLCO, whereas chest radiography was unchanged (International Labour Organisation (ILO) profusion below 1/1). For five of the six subjects HRCT probability of asbestosis was intermediate. An increase in FEF25-75% in some asbestos exposed non-smoking workers may be one of the earliest functional signs indicative of future development of parenchymal asbestosis. Early asbestos related parenchymal abnormalities are seen more frequently on HRCT than on chest radiography.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Aberle D. R., Gamsu G., Ray C. S., Feuerstein I. M. Asbestos-related pleural and parenchymal fibrosis: detection with high-resolution CT. Radiology. 1988 Mar;166(3):729–734. doi: 10.1148/radiology.166.3.3340770. [DOI] [PubMed] [Google Scholar]
- Becklake M. R. Asbestos-related diseases of the lungs and pleura: current clinical issues. Am Rev Respir Dis. 1982 Aug;126(2):187–194. doi: 10.1164/arrd.1982.126.2.187. [DOI] [PubMed] [Google Scholar]
- Churg A. Current issues in the pathologic and mineralogic diagnosis of asbestos-induced disease. Chest. 1983 Sep;84(3):275–280. doi: 10.1378/chest.84.3.275. [DOI] [PubMed] [Google Scholar]
- Gross P., De Treville R. T. Experimental asbestosis. Studies on the progressiveness of the pulmonary fibrosis caused by chrysotile dust. Arch Environ Health. 1967 Nov;15(5):638–649. doi: 10.1080/00039896.1967.10664980. [DOI] [PubMed] [Google Scholar]
- Jodoin G., Gibbs G. W., Macklem P. T., McDonald J. C., Becklake M. R. Early effects of asbestos exposure on lung function. Am Rev Respir Dis. 1971 Oct;104(4):525–535. doi: 10.1164/arrd.1971.104.4.525. [DOI] [PubMed] [Google Scholar]
- Mohsenifar Z., Jasper A. J., Mahrer T., Koerner S. K. Asbestos and airflow limitation. J Occup Med. 1986 Sep;28(9):817–820. doi: 10.1097/00043764-198609000-00012. [DOI] [PubMed] [Google Scholar]
- Rosenstock L., Barnhart S., Heyer N. J., Pierson D. J., Hudson L. D. The relation among pulmonary function, chest roentgenographic abnormalities, and smoking status in an asbestos-exposed cohort. Am Rev Respir Dis. 1988 Aug;138(2):272–277. doi: 10.1164/ajrccm/138.2.272. [DOI] [PubMed] [Google Scholar]
- Staples C. A., Gamsu G., Ray C. S., Webb W. R. High resolution computed tomography and lung function in asbestos-exposed workers with normal chest radiographs. Am Rev Respir Dis. 1989 Jun;139(6):1502–1508. doi: 10.1164/ajrccm/139.6.1502. [DOI] [PubMed] [Google Scholar]