

Abstract
Subendocardial ischemia as indicated by electrocardiography during exercise, in association with severe systolic anterior motion of the anterior mitral valve leaflet without left ventricular hypertrophy, has not been well described. We report the case of a 42-year-old man who presented with symptoms of exertional angina and 2-mm ST depression on treadmill electrocardiography but had a normal perfusion scan and coronary angiogram. Initially, the negative angiographic results caused us to regard the treadmill results as false-positive. Subsequently, low-dose dobutamine echocardiography showed severe systolic anterior motion of the anterior mitral valve leaflet with a >144-mmHg left ventricular outflow tract gradient; we then recognized the original treadmill results to be pseudo-false-positive. Electrocardiographic changes in association with the above-described motion of the anterior mitral valve leaflet and increased left ventricular outflow tract gradient were verified by use of treadmill and supine bicycle stress echocardiography. (Tex Heart Inst J 2001;28:308–11)
Key words: Angina pectoris; coronary disease/ultrasonography; dobutamine/diagnostic use; echocardiography, Doppler; exercise test; myocardial ischemia; ventricular outflow obstruction/ultrasonography; ventricular function, left/physiology
Exercise echocardiography is gaining popularity as a tool for evaluating atherosclerotic coronary artery disease. However, its utility in evaluating myocardial ischemia due to other causes has not been well documented. The application of exercise echocardiography in cases of left ventricular outflow tract (LVOT) obstruction and systolic anterior motion (SAM) of the anterior mitral valve leaflet may also be important, because coronary angiography and nuclear perfusion scanning do not depict such functional abnormalities. In the case presented here, a serendipitously ordered dobutamine echocardiogram resulted in the diagnosis of severe SAM of the mitral valve. Follow-up treadmill and bicycle tests confirmed the severe dynamic LVOT obstruction-associated ischemic changes seen on the initial treadmill electrocardiogram (ECG).
Case Report
In August 1999, a 42-year-old physician with no known risk factors for coronary artery disease presented with a 1-year history of exertional chest pressure. The previous year, because of a positive treadmill exercise test, he had undergone coronary angiography that showed no overt atherosclerotic disease. Due to the persistent symptoms, another treadmill test with technetium 99m sestamibi imaging was performed at the current visit. He again developed anginal symptoms during stage III of the Bruce protocol, and the ECG showed a 2-mm horizontal ST depression that persisted into the first 9-minute recovery period. The perfusion scan, however, showed physiologic radiotracer distribution with normal wall motion.
Perplexed by his symptoms and uncertain about the risks of aerobic training, the patient requested dobutamine echocardiography at his primary physician's office. With the patient at rest, the echocardiogram showed a ventricular septal thickness of 1.2 cm, with normal wall motion and mitral valve dynamics (Fig. 1). At 10-μg/kg per min of dobutamine infusion, he developed severe SAM of the anterior mitral valve leaflet with a LVOT gradient greater than 144 mmHg and recurrent symptoms of angina. The patient had hyperdynamic left ventricular wall motion during stress, and his mitral valve apparatus appeared normal in structure with no evidence of redundant chordae (Fig. 2). The patient subsequently underwent supine bicycle-exercise and treadmill echocardiography. After 12 minutes of exercise on the supine bicycle (maximum resistance, 150 W), the patient's peak heart rate was 172 beats/min, his blood pressure was 195/109 mmHg, and he developed chest pressure. The ECG showed ST depression, and echocardiography revealed the same LVOT gradient (>144 mmHg) due to SAM of the mitral valve. Treadmill echocardiography showed similar evidence of LVOT obstruction at stage III of the Bruce protocol.
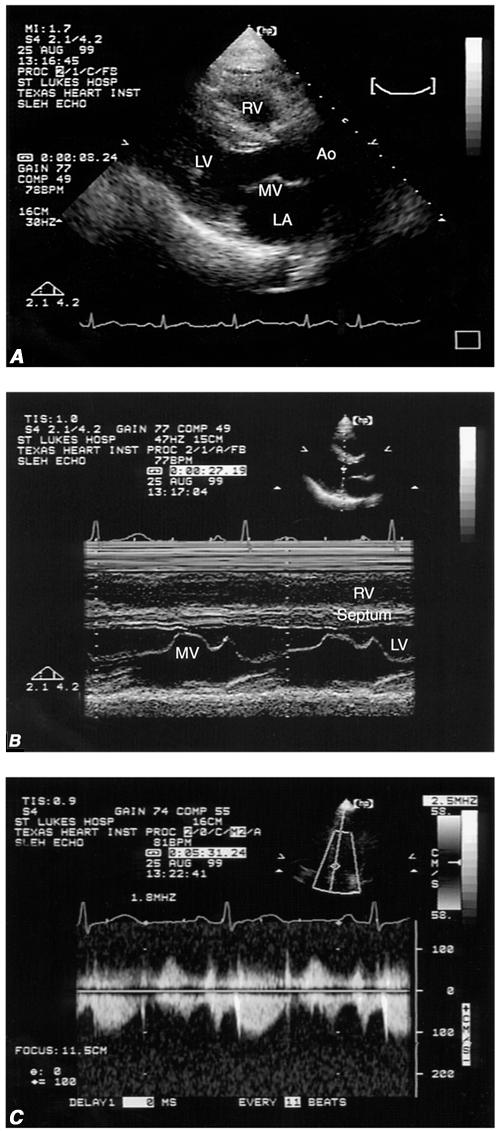
Fig. 1 Resting echocardiographic images: A) parasternal long-axis view at end-systole; B) M-mode of the parasternal long axis; and C) continuous-wave Doppler across the left ventricular outflow tract with an outflow velocity of 1.2 m/sec.
Ao = aorta; LA = left atrium; LV = left ventricle; MV = mitral valve; RV = right ventricle
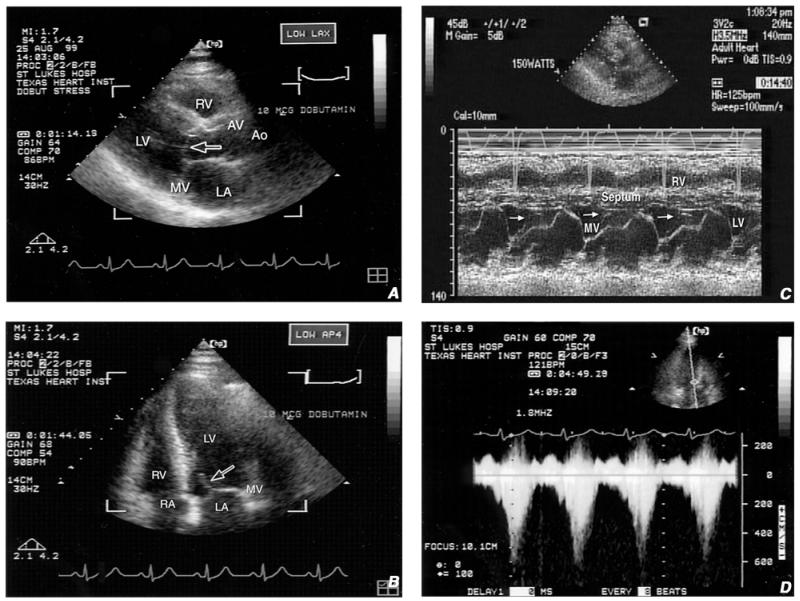
Fig. 2 Stress echocardiographic images: A) parasternal long-axis view shows the systolic anterior motion (SAM) of the anterior mitral leaflet (arrow); B) 4-chamber long-axis view shows SAM (arrow); C) M-mode of the parasternal long axis shows the anterior mitral leaflet in close proximity to the septum at end-systole (arrow); and D) continuous-wave Doppler shows a left ventricular outflow velocity approaching 6 m/sec and a left ventricular outflow tract gradient >144 mmHg.
Ao = aorta; AV = aortic valve; LA = left atrium; LV = left ventricle; MV = mitral valve; RA = right atrium; RV = right ventricle
A diagnosis of myocardial ischemia due to SAM of the anterior mitral valve leaflet was supported by the normal coronary angiogram, the patient's ischemic symptoms of exertional angina, and the marked ECG changes during exercise and recovery. We prescribed bisoprolol (5 mg once daily) and advised the patient to keep his heart rate below 150 beats/min during exercise. Outpatient follow-up at 1 and 2 years showed him to be symptom free.
Discussion
Although exercise or dobutamine echocardiography has been used to evaluate myocardial ischemia and viability in patients with ischemic heart disease, it is often overlooked as a means of assessing the hemodynamic aspects of valvular and myocardial diseases during stress. Our patient had classic ischemic symptoms of exertional angina and associated ECG changes in the absence of flow-limiting coronary artery disease (as shown by cardiac catheterization). The positive stress test in the presence of a normal coronary angiogram caused us to regard the treadmill results as false-positive. Nevertheless, the patient's seemingly contradictory signs and symptoms led us to explore other causes for the angina, such as the presence of left ventricular hypertrophy, aortic stenosis, or, as was the case, LVOT obstruction due to SAM of the mitral valve. Stress echocardiography showed that the patient's ischemic symptoms resulted not from coronary artery disease but rather from LVOT obstruction caused by SAM of the mitral valve, which most likely compromised subendocardial blood flow. Thus, what we had thought to be a false-positive treadmill test was shown to be a pseudo-false-positive result.
A LVOT gradient secondary to SAM of the mitral valve during exercise and dobutamine stress testing has been described in the medical literature. 1–4 The contribution of this condition to myocardial ischemia and associated angina, however, has not been well documented. Dynamic intraventricular obstruction during dobutamine infusion has been reported in a large number of patients with or without myocardial hypertrophy. 1–5 The incidence of SAM of the mitral valve, which ranges from 2% to 16%, is more common after mitral valve repair in patients who have myxomatous mitral valve disease. 6–9 Its incidence during stress echocardiography (produced either by exercise or by dobutamine infusion) varies, depending on the study population. The incidence of LVOT obstruction induced by dobutamine stress ranges from 8% to 21%, and 13% to 25% of those cases are the result of SAM of the mitral valve. 1,3,10,11
Barletta and coworkers, 12 studying 16 patients who had exercise-induced ECG changes and intraventricular obstruction during dobutamine stress echocardiography, found that 9 of the patients experienced SAM of the mitral valve during the dobutamine infusion. As in our patient, there were no notable lesions evident on the coronary angiogram, and results of radionuclide myocardial perfusion studies were normal. All 16 of their patients were treated with β-blockers and remained symptom free at 12-months' follow-up. Those authors proposed that the ischemia-like response could be secondary to the high myocardial oxygen demand that the obstruction imposes on the mid-to-apical left ventricular walls, with a subsequent decrease in subendocardial perfusion from the lower aortic pressure. The presence of microvascular disease was proposed as another possible explanation. 12
We recommend the use of stress echocardiography for patients in whom myocardial ischemia is suspected. In addition to the patients' symptoms and ECG changes on the treadmill, the results from stress echocardiography can be used to determine whether the symptoms of ischemia and associated ECG findings are due to an atherosclerotic coronary obstruction or to a myocardial intracavitary obstruction—the latter may account for ischemic symptoms in some patients. Future studies are needed to examine the implications of a stress-induced LVOT gradient, with or without SAM of the mitral valve, on long-term morbidity and mortality. Whether inotropic and chronotropic agents such as β-blockers and calcium channel blockers are beneficial in reversing such an obstruction has yet to be determined.
Footnotes
Address for reprints: Theodore K. Lau, MD, Texas Heart Institute, MC 1–133, 6720 Bertner Avenue, Room P332, Houston, TX 77030
References
- 1.Pellikka PA, Oh JK, Bailey KR, Nichols BA, Monahan KH, Tajik AJ. Dynamic intraventricular obstruction during dobutamine stress echocardiography. A new observation. Circulation 1992;86:1429–32. [DOI] [PubMed]
- 2.Henein MY, O'Sullivan C, Sutton GC, Gibson DG, Coats AJ. Stress-induced left ventricular outflow tract obstruction: a potential cause of dyspnea in the elderly. J Am Coll Cardiol 1997;30:1301–7. [DOI] [PubMed]
- 3.Luria D, Klutstein MW, Rosenmann D, Shaheen J, Sergey S, Tzivoni D. Prevalence and significance of left ventricular outflow gradient during dobutamine echocardiography. Eur Heart J 1999;20:386–92. [DOI] [PubMed]
- 4.Peteiro J, Montserrat L, Castro-Beiras A. Labil subaortic obstruction during exercise stress echocardiography. Am J Cardiol 1999;84:1119–23,A10–1. [DOI] [PubMed]
- 5.Hashimoto Y, Reid CL, Gardin JM. Left ventricular cavitary geometry and dynamic intracavitary left ventricular obstruction during dobutamine stress echocardiography. Am J Card Imaging 1996;10:163–9. [PubMed]
- 6.Jebara VA, Mihaileanu S, Acar C, Brizard C, Grare P, Latremouille C, et al. Left ventricular outflow tract obstruction after mitral valve repair. Results of the sliding leaflet technique. Circulation 1993;88(5 Pt 2):II30–4. [PubMed]
- 7.Lee KS, Stewart WJ, Lever HM, Underwood PL, Cosgrove DM. Mechanism of outflow tract obstruction causing failed mitral valve repair. Anterior displacement of leaflet coaptation. Circulation 1993;88(5 Pt 2):II4–29. [PubMed]
- 8.Rey MJ, Mercier LA, Castonguay Y. Echocardiographic diagnosis of left ventricular outflow tract obstruction after mitral valvuloplasty with a flexible Duran ring. J Am Soc Echocardiogr 1992;5:89–92. [DOI] [PubMed]
- 9.Maslow AD, Regan MM, Haering JM, Johnson RG, Levine RA. Echocardiographic predictors of left ventricular outflow tract obstruction and systolic anterior motion of the mitral valve after mitral valve reconstruction for myxomatous valve disease. J Am Coll Cardiol 1999;34:2096–104. [DOI] [PubMed]
- 10.Murakami H, Nishimura M, Urabe K. Relation between dynamic midventricular obstruction and unexplained chest pain in patients with normal echocardiograms at rest. Am J Cardiol 1996;78:1063–5. [DOI] [PubMed]
- 11.Scandura S, Arcidiacono S, Felis S, Barbagallo G, Deste W, Drago A, et al. Dynamic obstruction to left ventricular outflow during dobutamine stress echocardiography: the probable mechanisms and clinical implications [in Italian]. Cardiologia 1998;43:1201–8. [PubMed]
- 12.Barletta G, Del Bene MR, Gallini C, Salvi S, Costanzo E, Masini M, et al. The clinical impact of dynamic intraventricular obstruction during dobutamine stress echocardiography. Int J Cardiol 1999;70:179–89. [DOI] [PubMed]