

Abstract
A 41-year-old man with no relevant cardiac history presented for evaluation of episodic syncope. Electrocardiography showed sinus rhythm with right bundle-branch block and Q waves in leads II, III, and aVF. Subsequent exercise treadmill testing and technetium 99m sestamibi study revealed a reversible posterior defect. Coronary angiography later showed a right coronary artery that arose from the left coronary sinus—an anomaly that has been associated with angina, myocardial infarction, and sudden cardiac death.
After being informed of the potential risks and options associated with this anomaly, the patient chose long-term β-blocker medical therapy. At follow-up, this treatment appeared to have resolved his episodic syncope. (Tex Heart Inst J 2002;29:37–9)
Key words: Coronary vessel anomalies/diagnosis/complications/pathology/therapy, heart catheterization, risk assessment
The incidence of coronary anomalies in patients undergoing coronary angiography varies from 0.64% to 1.3%. Many of these anomalies are clinically benign; however, others are associated with serious morbidity. We describe the case of a patient in whom evaluation of episodic syncope revealed an anomalous right coronary artery arising from the left coronary sinus. We discuss the clinical importance of this anomaly and review the literature concerning current views and therapy.
Case Report
In October 2000, a 41-year-old white man with no relevant medical history went to his internist with lightheadedness and syncope on exertion. The patient was an active individual and had not previously had problems with chest pain or shortness of breath on exertion. The presenting symptoms had begun approximately 5 weeks before, when the patient experienced the sudden onset of lightheadedness while running to an airline gate. The episode lasted a few seconds but resolved spontaneously. One week later, while pounding in a tent stake, the patient lost consciousness, and the episode resolved spontaneously after about 30 seconds. According to the patient, during neither episode was there any occurrence of postictal confusion, tongue biting, incontinence, or notable neurological symptoms. The patient also stated that the episodes were not associated with any palpitations, urination, defecation, or unusual neck positions.
Exercise treadmill testing (ETT) and a technetium 99m sestamibi study revealed a reversible posterior defect. Echocardiography showed lateral hypokinesis and a slightly low ejection fraction. An electrocardiogram showed sinus rhythm with right bundle-branch block and Q waves in leads II, III, and aVF. The patient's initial physical examination and laboratory results showed no other abnormalities. He was referred to our institution for cardiac catheterization.
Selective catheterization of the left coronary artery revealed nonocclusive coronary artery disease. Attempted cannulation of the right coronary artery was difficult and at times resulted in episodes of complete heart block, especially during inadvertent entry into the left ventricle with the catheter. Prophylactic pacing wires were placed, and nonselective catheterization revealed an anomalous origin of the right coronary artery from the left coronary sinus (Fig. 1).
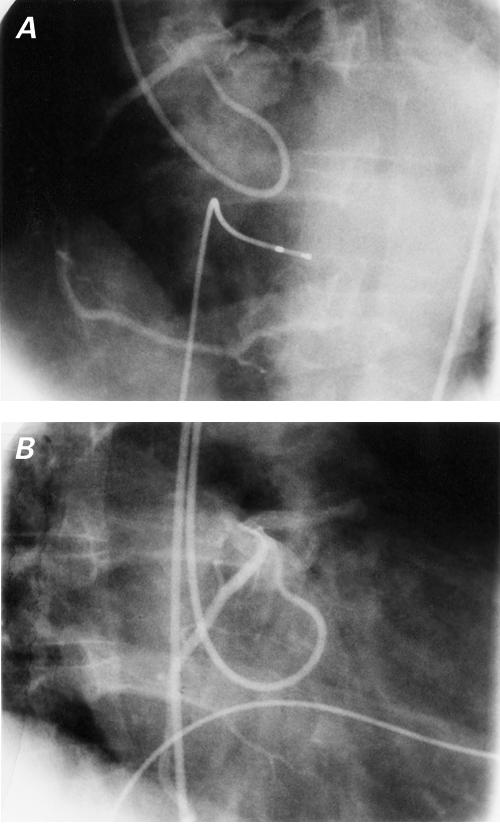
Fig. 1 Nonselective angiography in the left anterior oblique projection (A) and the right anterior oblique projection (B) revealing an anomalous origin of the right coronary artery from the left coronary sinus.
Because of the known association between this coronary anomaly and adverse cardiac events (see Discussion), the patient was started on β-blockers. A subsequent Holter study revealed no arrhythmias, and the patient has since experienced no episodes of lightheadedness or syncope.
Discussion
Anomalous origin of the right coronary artery is a rare congenital anomaly that was 1st described in 1948 by White and Edwards. 1 The prevalence of this anomaly in the white population, as determined from autopsy studies, is 0.026%. 2 The prevalence of this anomaly in other populations, however, is significantly higher. Kaku and colleagues 3 examined 17,731 patients undergoing coronary angiography in Japanese centers between 1968 and 1994 and noted a prevalence of 0.25%. Topaz and coworkers 4 reported similar numbers in their study and noted that anomalous origin of the right coronary artery was the most common coronary anomaly in people of Hispanic origin.
It is well established that an anomalous origin of the right coronary artery can lead to angina pectoris, myocardial infarction, or sudden death, in the absence of atherosclerosis. 5 The pathophysiologic basis for this association, however, is unclear. Mechanical compression of the right coronary artery by the great vessels is the usual explanation, because the anomalous right coronary artery generally courses between the aorta and the pulmonary artery to its normal position. Others have suggested that the oblique angle at the juncture of the anomalous right coronary artery and the left coronary sinus produces a slit-like orifice in the aortic wall that can collapse during exercise. 5 Recently, Kaku's group 6 suggested that the proximal portion of the right coronary artery, situated between the aorta and the pulmonary artery, might be more prone to spasm than it would be otherwise.
Regardless of the causes of the adverse associations, there is a need to study prospectively those patients at highest risk. In 1992, Taylor and co-authors, 5 in their study of 52 patients with anomalous origin of the right coronary artery, noted that 25% had died suddenly and in most cases asymptomatically. Moreover, the anomalous right coronary artery was 2nd only to the anomalous left main coronary artery as the cardiac anomaly most frequently associated with sudden cardiac death.
In an effort to stratify such cases by risk, Taylor and associates later (in 1997) 7 performed a blinded pathologic analysis of 21 cases of anomalous origin of the right coronary artery. Despite reviewing a variety of anatomic variables (including ostial size, length of intramural course, angle of takeoff, and the presence of symptoms), this group found that only an age of 30 years or older was associated with a lower incidence of sudden cardiac death.
Understandably, the choice of treatment for this coronary anomaly is controversial, with some advocating revascularization in all cases. Proposed options include translocation of the right coronary artery to the aorta, 8 ostioplasty (excision of the common wall between the right coronary artery and the aorta), 9 and bypass grafting of the right coronary artery (with optional ligation of the native artery proximal to the graft anastomosis to prevent competitive flow). 10 However, the long-term benefits of such therapies have not yet been demonstrated.
In Japan, treatment for this condition is more conservative. Kaku and associates 3 studied 56 patients with an anomalous origin of a coronary artery and treated them medically with β-blockers. Approximately 9% of these patients experienced episodes of hypotension and arrhythmias on exertion, and no death was found to be directly related to the congenital anomaly during 5 years of follow-up.
In the present case, the patient was informed of the various options to manage his condition. He chose medical therapy, which was effective in resolving the syncope.
Footnotes
Address for reprints: John S. Ho, MD, Texas Heart Institute, P.O. Box 20269, Houston, TX 77225-0269
References
- 1.White NK, Edwards JE. Anomalies of the coronary arteries. Report of four cases. Arch Pathol 1948;45:766–71. [PubMed]
- 2.Alexander RW, Griffiths GC. Anomalies of the coronary arteries and their clinical significance. Circulation 1956;14: 800–5. [DOI] [PubMed]
- 3.Kaku B, Shimizu M, Yoshio H, Ino H, Mizuno S, Kanaya H, et al. Clinical features of prognosis of Japanese patients with anomalous origin of the coronary artery. Jpn Circ J 1996;60:731–41. [DOI] [PubMed]
- 4.Topaz O, DeMarchena EJ, Perin E, Sommer LS, Mallon SM, Chahine RA. Anomalous coronary arteries: angiographic findings in 80 patients. Int J Cardiol 1992;34:129–38. [DOI] [PubMed]
- 5.Taylor AJ, Rogan KM, Virmani R. Sudden cardiac death associated with isolated congenital coronary artery anomalies. J Am Coll Cardiol 1992;20:640–7. [DOI] [PubMed]
- 6.Kaku B, Kanaya H, Ikeda M, Uno Y, Fujita S, Kato F, Oka T. Acute inferior myocardial infarction and coronary spasm in a patient with an anomalous origin of the right coronary artery from the left sinus of Valsalva. Jpn Circ J 2000;64: 641–3. [DOI] [PubMed]
- 7.Taylor AJ, Byers JP, Cheitlin MD, Virmani R. Anomalous right or left coronary artery from the contralateral coronary sinus: “high-risk” abnormalities in the initial coronary artery course and heterogeneous clinical outcomes. Am Heart J 1997;133:428–35. [DOI] [PubMed]
- 8.Di Lello F, Mnuk JF, Flemma RJ, Mullen DC. Successful coronary reimplantation for anomalous origin of the right coronary artery from the left sinus of Valsalva. J Thorac Cardiovasc Surg 1991;102:455–6. [PubMed]
- 9.Rinaldi RG, Carballido J, Giles R, Del Toro E, Porro R. Right coronary artery with anomalous origin and slit ostium. Ann Thorac Surg 1994;58:829–32. [DOI] [PubMed]
- 10.Shah AS, Milano CA, Lucke JP. Anomalous origin of the right coronary artery from the left coronary sinus: case report and review of surgical treatments. Cardiovasc Surg 2000;8:284–6. [DOI] [PubMed]