

Abstract
Aneurysm of the left sinus of Valsalva is extremely rare. Compression of the left coronary artery by such an aneurysm is an unusual complication of this condition and can cause coronary insufficiency.
We describe the case of a 75-year-old woman who had an isolated unruptured aneurysm of the left coronary sinus with intraluminal thrombus, which caused coronary artery compression. We performed successful surgical correction by closing the mouth of the aneurysm without aortic valve replacement or coronary artery bypass grafting. A review of the world medical literature revealed 19 cases of sinus of Valsalva aneurysms that hindered the coronary arterial flow. The previously published reports of this rare condition and its treatment are discussed herein. (Tex Heart Inst J 2002;29:40–4)
Key words: Angina pectoris/etiology; aortic aneurysm/complications/diagnosis/surgery; coronary arteries; heart defects, congenital; myocardial ischemia/etiology; sinus of Valsalva
Sinus of Valsalva aneurysms (SVAs) are rare anomalies, most often caused by the congenital absence of muscular and elastic tissue in the aortic wall behind the sinus of Valsalva. 1 Acquired, or noncongenital, SVAs are caused by conditions affecting the aortic wall, such as infections (bacterial endocarditis, syphilis, or tuberculosis); trauma; or degenerative disease (atherosclerosis, connective tissue disorders, or cystic medial necrosis). The origin of SVAs is the right coronary sinus in 94%, the noncoronary sinus in 5%, and the left coronary sinus in 1%. 2 These aneurysms are often complicated by rupture; those that remain unruptured are typically asymptomatic. However, compression of the left coronary arteries by SVAs can cause myocardial ischemia.
We report herein the successful treatment of a 75-year-old woman who had a large, unruptured, isolated aneurysm of the left sinus of Valsalva. The SVA, which contained thrombus, had caused direct compression of the left anterior descending coronary artery and the resultant symptoms. Nineteen previously reported cases of isolated aneurysm of the left aortic sinus causing coronary insufficiency are reviewed.
Case Report
In May 2000, a 75-year-old woman was admitted to the cardiology department of our institution with a 1-month history of chest pain, which suggested angina pectoris. One week before admission, the chest pain had begun to increase in frequency, duration, and intensity. The patient was a smoker and had a 10-year history of hypertension.
On admission, physical examination and laboratory data, including cardiac enzyme levels, revealed no abnormalities. The chest radiograph delineated a normal cardiothoracic ratio and no focal lung lesion. The electrocardiogram showed sinus rhythm and T wave inversion in leads I and aVL. An exercise test indicated the presence of myocardial ischemia (downsloping S-T segment and typical chest pain) during the 2nd stage. Left ventricular angiography and aortography revealed an isolated aneurysm of the left sinus of Valsalva with intraluminal thrombus (Fig. 1). There was no evidence of aortic stenosis or regurgitation. Left and right ventricular hemodynamic variables and function were within normal limits. Selective coronary angiography showed a normal right coronary artery. However, the left main coronary artery and proximal segments of the left anterior descending and circumflex arteries were displaced superiorly. The 1st and 2nd diagonal branches of the left anterior descending coronary artery were stretched and elongated by the SVA, causing severe fusiform stenosis (Fig. 2). Upon transesophageal echocardiography, a large isolated aneurysm was visible, arising from the left coronary sinus and extending into the left ventricular wall behind the pulmonary artery up to the left atrium.
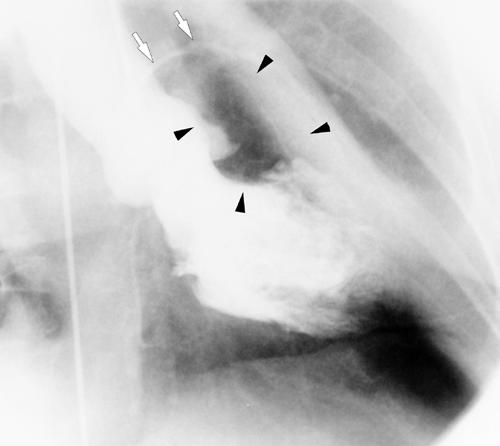
Fig. 1 Opacification of the aorta during left ventriculography shows a left sinus of Valsalva aneurysm (black arrows). The left main stem and the left anterior descending coronary artery are stretched and displaced upward (white arrows).
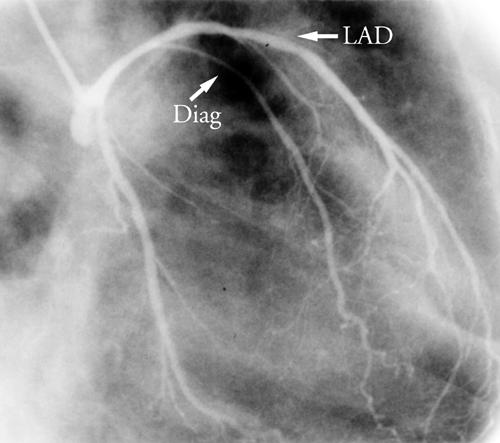
Fig. 2 Selective angiogram of the left coronary artery shows the main trunk and the left anterior descending coronary artery (LAD) displaced upward. The proximal portion of the diagonal branch (Diag) is markedly compressed by the aneurysm.
The patient was then referred for operation. At surgery, normothermic cardiopulmonary bypass was instituted, the aorta was clamped, and warm-blood cardioplegia was infused directly into the coronary ostia. The ascending aorta appeared normal. The aortic valve was trileaflet and competent; there was no evidence of inflammation or degeneration. The aneurysm, filled with organized thrombus, extended toward the left side of the aorta and through the left lateral ventricular wall. The saccular, finger-like aneurysm (2 cm in diameter and about 7 cm in length) arose from the central part of the left coronary sinus of Valsalva just inferior to the left coronary ostium. The aneurysmal sac ended below the left atrium. The 2- × 3-cm oval orifice of the aneurysm was situated between the left coronary ostium and the annulus of the aortic valve (Fig. 3). The left coronary artery ostium was superiorly displaced by the neck of the aneurysm. The right coronary artery originated from the normal position. The organized thrombus was removed, and the opening of the aneurysm was closed with horizontal mattress sutures and reinforced with Teflon buttresses (Fig. 4), although the tissue of the adjacent aortic wall was solid. When placing the sutures, we were careful to avoid inadvertent injury to or distortion of the left coronary ostium and the aortic valve cusps. After the repair, the aortic sinus was normal in appearance. The reinforced suture, parallel to the aortic annulus, did not interfere with valvular function or with the left coronary ostium.
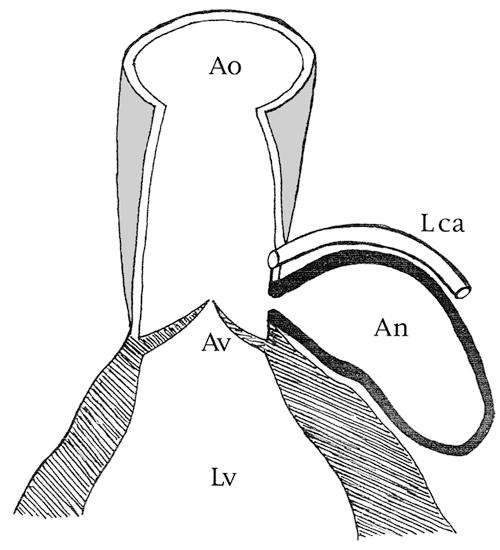
Fig. 3 Drawing shows the aneurysm of the sinus of Valsalva and the left coronary artery compression. An = aneurysm; Ao = aorta; Av = aortic valve; Lca = left coronary artery; Lv = left ventricle
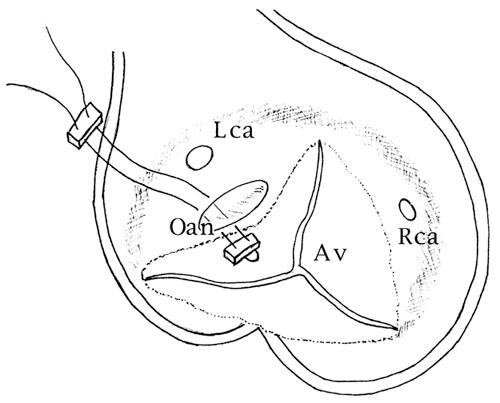
Fig. 4 Drawing shows the surgical treatment: the oval opening of the aneurysm is closed by horizontal sutures enforced with Teflon buttresses. Av = aortic valve; Lca = left coronary artery; Oan = opening of the aneurysm; Rca = right coronary artery
The patient was discharged from the hospital in good condition, without complications. We recommended 4 months of anticoagulation therapy to prevent sequelae that could be caused by the intra-aortic reinforced sutures. Six months postoperatively, the patient was asymptomatic. Echocardiography showed a normal aortic root with no aortic regurgitation and with normal left ventricular function. Thallium scintigraphy performed in conjunction with an exercise stress test showed no residual ischemia. Postoperative coronary angiography was proposed to the patient but was refused.
Discussion
Sinus of Valsalva aneurysms can be congenital or noncongenital. Congenital SVAs are generally isolated and consist of a localized burrowing of part of the aortic sinus into the myocardium, the neighboring cardiac chamber, or the free pericardium. Noncongenital SVAs are most often caused by bacterial endocarditis, syphilis, or atherosclerosis.
Aneurysms of the right and the noncoronary sinuses occur much more frequently than do those of the left, 2 and they commonly protrude and rupture into the right ventricle and the right atrium, respectively. Aneurysms of the left coronary sinus, which are extremely rare, typically protrude and rupture into the pulmonary artery, the left ventricle, the myocardium, or even the epicardium. 3 Unruptured SVAs are typically symptom free. In many cases, however, SVAs cause intracardiac rupture that results in aortocardiac fistulas. These aneurysms occasionally occur in conjunction with ventricular or atrial septal defects and with aortic or pulmonary valve abnormalities. 4
We found 19 previously reported cases 5-23 in which isolated, unruptured aneurysms of the left aortic sinus of Valsalva had hindered the coronary arterial flow. These reports are summarized in Table I. The 1st case, reported by Chipps in 1941, 5 described a 39-year-old man in whom myocardial infarction resulted from compression of the left main coronary artery by a syphilitic isolated aneurysm of the left sinus of Valsalva. The patient died 25 hours after hospital admission. In 1976, Garcia-Rinaldi 8 described the 1st case of congenital aneurysm of the left aortic sinus to be successfully treated by surgery. In all 19 previously reported cases, the clinical manifestation was angina or myocardial infarction, and the electrocardiographic results were compatible with coronary insufficiency. The aneurysms were isolated and unruptured, and the affected sinus was always the left one. The aneurysm was congenital in 10 patients and acquired in 9. The diagnosis was made by use of angiography in 14 patients, autopsy in 4, and echocardiography in 1. In 1 case, 19 the outcome was not available. Only 9 of these 19 patients underwent surgery; of these, successful surgical repair was achieved in 6, and 3 died postoperatively. 14,16,22 In 8 of the surgically treated patients, the chosen technique was closure of the aneurysmal opening (in the 9th patient, 23 the technique was not reported). Associated aortic valve replacement was necessary in 6 patients, and aortocoronary saphenous vein bypass grafting (CABG) was performed in 5. Only 1 patient 17 before ours was treated successfully with isolated closure of the opening of the aneurysm. That case was reported in 1988.
TABLE I. Nineteen Previous Reports, Along with the Current Case, of Patients with Isolated, Unruptured, Left Sinus of Valsalva Aneurysms, Who Presented with Angina or Myocardial Infarction*

Obstruction of coronary flow secondary to SVA is an uncommon manifestation of this rare malformation. Noninvasive diagnosis is accomplished with echocardiography or with computed tomography and magnetic resonance imaging; cardiac catheterization, aortography, and selective coronary arteriography are necessary to demonstrate coronary artery compression. An aggressive surgical approach is recommended in order to prevent acute coronary artery obstruction and ischemia that can lead to myocardial infarction or severe left ventricular failure. Without surgery, other risks include aneurysmal enlargement, rupture with sudden death, aortic incompetence, infection, and malignant arrhythmias.
Because of a lack of controlled trials, the surgical method for treating an unruptured SVA is chosen on the basis of anecdoctal experience and generally consists of closure of the opening of the aneurysm, replacement of the aortic valve, saphenous vein bypass, or a combination of these. To our knowledge, we present only the 2nd case of a left SVA to be successfully repaired by closure of the opening of the aneurysm without aortic valve replacement or coronary artery bypass grafting. Despite the lack of follow-up angiography to provide visual proof of the successful repair in our patient, we suggest that the lack of postoperative symptoms, the lack of residual ischemia upon stress thallium study, and the normal postoperative echocardiographic results provide conclusive evidence that this method of repair is effective and should be considered in order to avoid the late complications associated with aortic valve prostheses and aortocoronary bypass grafting.
Footnotes
Address for reprints: Antonio Lijoi, MD, Divisione di Cardiochirurgia, Università di Genova, Ospedale San Martino, Monoblocco V. Piano, Largo Rosanna Benzi 10, 16132 Genoa, Italy
References
- 1.Edwards JE, Burchell HB. The pathological anatomy of deficiencies between the aortic root and the heart, including aortic sinus aneurysms. Thorax 1957;12:125–39. [DOI] [PMC free article] [PubMed]
- 2.Guo DW, Cheng TO, Lin ML, Gu ZQ. Aneurysm of the sinus of Valsalva: a roentgenologic study of 105 Chinese patients. Am Heart J 1987;114:1169–77. [DOI] [PubMed]
- 3.Chu SH, Hung CR, How SS, Chang H, Wang SS, Tsai CH, et al. Ruptured aneurysms of the sinus of Valsalva in Oriental patients. J Thorac Cardiovasc Surg 1990;99:288–98. [PubMed]
- 4.Chakfe N, Kretz JG, Nicolini P, Gasser B, Zupan M, Brechenmacher C, Wolff F. Triple aneurysm of the Valsalva sinus complicated by right coronary occlusion: apropos of a case and review of the literature [in French]. Ann Chir 1994;48: 825–31. [PubMed]
- 5.Chipps HD. Aneurysm of the sinus of Valsalva causing coronary occlusion. Arch Pathol 1941;31:627–30.
- 6.Eliot RS, Wolbrink A, Edwards JE. Congenital aneurysm of the left aortic sinus. A rare lesion and a rare cause of coronary insufficiency. Circulation 1963;28:951–6. [DOI] [PubMed]
- 7.Olsen J. Aneurysm of the aortic sinus of Valsalva. A case of rupture and myocardial infarction. Acta Pathol Microbiol Scand 1969;76:12–8. [DOI] [PubMed]
- 8.Garcia-Rinaldi R, Von Koch L, Howell JF. Aneurysm of the sinus of Valsalva producing obstruction of the left main coronary artery. J Thorac Cardiovasc Surg 1976;72:123–6. [PubMed]
- 9.Feldman RL, Buchoff HF, Pepine CJ, Conti CR. Aneurysm of sinus of Valsalva: cause of dynamic coronary constriction after aortic valvular replacement and bacterial endocarditis. Chest 1978;74:312–4. [DOI] [PubMed]
- 10.Cupo LN, Pyeritz RE, Olson JL, McPhee SJ, Hutchins GM, McKusick VA. Ehlers-Danlos syndrome with abnormal collagen fibrils, sinus of Valsalva aneurysms, myocardial infarction, panacinar emphysema and cerebral heterotopias. Am J Med 1981;71:1051–8. [DOI] [PubMed]
- 11.Williams TG, Williams BT. Isolated unruptured aneurysm of the left coronary sinus of Valsalva. Ann Thorac Surg 1983;35:556–9. [DOI] [PubMed]
- 12.Hiyamuta K, Ohtsuki T, Shimamatsu M, Ohkita Y, Terasawa M, Bekki H, et al. Aneurysm of the left aortic sinus causing acute myocardial infarction. Circulation 1983;67: 1151–4. [DOI] [PubMed]
- 13.Brandt J, Jogi P, Luhrs C. Sinus of Valsalva aneurysm obstructing coronary arterial flow: case report and collective review of the literature. Eur Heart J 1985;6:1069–73. [DOI] [PubMed]
- 14.Faillace RT, Greenland P, Nanda NC. Rapid expansion of a saccular aneurysm on the left coronary sinus of Valsalva: a role for early surgical repair? Br Heart J 1985;54:442–4. [DOI] [PMC free article] [PubMed]
- 15.Nakano T, Okano H, Konishi T, Takezawa H. Aneurysm of the left aortic sinus caused by Takayasu's arteritis: compression of the left coronary artery producing coronary insufficiency. J Am Coll Cardiol 1986;7:696–700. [DOI] [PubMed]
- 16.Le Helloco A, Danchin N, Amrein D, Nizak J, Pernot C. Aneurysm of the sinistro-anterior sinus of Valsalva causing coronary insufficiency [in French]. Arch Mal Coeur Vaiss 1986;79:1515–20. [PubMed]
- 17.Gallet B, Combe E, Saudemont JP, Tetard C, Barret F, Gandjbakhch I, Hiltgen M. Aneurysm of the left aortic sinus causing coronary compression and unstable angina: successful repair by isolated closure of the aneurysm. Am Heart J 1988;115:1308–10. [DOI] [PubMed]
- 18.Henry RE, Daisley H, Barton EN. Sudden cardiac death caused by coronary ostial compression by an aneurysm of the sinus of Valsalva. West Indian Med J 1989;38:250–2. [PubMed]
- 19.Morgan JM, Coupe MO, Honey M, Miller GA. Aneurysms of the sinuses of Valsalva in Noonan's syndrome. Eur Heart J 1989;10:190–3. [DOI] [PubMed]
- 20.Koike S, Takayama S, Furihata A, Furihata Y, Sasaki Y, Furuta S, Morimoto M. Infective endocarditis causing acute myocardial infarction by compression of the proximal left coronary artery due to a mycotic aneurysm of the sinus of Valsalva. Jpn Circ J 1991;55:1228–32. [DOI] [PubMed]
- 21.Tahir MZ, Rustom M, Al Ebrahim K. Left coronary sinus of Valsalva aneurysm: an extremely rare malformation. A case report. Angiology 1995;46:753–8. [DOI] [PubMed]
- 22.Bashour TT, Chen F, Yap A, Mason DT, Baladi N. Fatal myocardial ischemia caused by compression of the left coronary system by a large left sinus of Valsalva aneurysm. Am Heart J 1996;132:1050–2. [DOI] [PubMed]
- 23.Ferreira AC, de Marchena E, Mayor M, Bolooki H. Sinus of Valsalva aneurysm presenting as myocardial infarction during dobutamine stress test. Cathet Cardiovasc Diagn 1996;39:400–2. [DOI] [PubMed]