

Key Points
Question
What is the efficacy and safety of low-dose combination triple and quadruple antihypertensives for the management of hypertension?
Findings
This systematic review and meta-analysis of 7 trials enrolling 1918 patients found that low-dose combination antihypertensives were more efficacious than monotherapy, usual care, or placebo in terms of mean blood pressure reduction and achieving blood pressure target. Low-dose combinations were also well tolerated but were associated with higher rates of dizziness than monotherapy or usual care.
Meaning
The findings suggest that low-dose combinations with 3 or 4 antihypertensives were effective and well tolerated in the lowering of blood pressure and may be an effective strategy for the early management of hypertension.
This systematic review and meta-analysis evaluates the safety and efficacy of low-dose combination therapy vs monotherapy, usual care, and placebo for early treatment of hypertension.
Abstract
Importance
Low-dose combination (LDC) antihypertensives consisting of 3 or 4 blood pressure (BP)–lowering drugs have emerged as a potentially important therapy for the initial management of hypertension.
Objective
To assess the efficacy and safety of LDC therapies for the management of hypertension.
Data Sources
PubMed and Medline were searched from date of inception until September 2022.
Study Selection
Randomized clinical trials comparing LDC consisting of 3 or 4 BP-lowering drugs compared to either monotherapy, usual care, or placebo.
Data Extraction and Synthesis
Data were extracted by 2 independent authors and synthesized using both random and fixed-effects models using risk ratios (RR) for binary outcomes and mean differences for continuous outcomes.
Main Outcomes and Measures
The primary outcome was mean reduction in systolic BP (SBP) between LDC and monotherapy, usual care, or placebo. Other outcomes of interest included the proportion of patients achieving BP less than 140/90 mm Hg, rates of adverse effects, and treatment withdrawal.
Results
Seven trials with a total of 1918 patients (mean [mean range] age, 59 [50-70] years; 739 [38%] female) were included. Four trials involved triple-component LDC and 3 involved quadruple-component LDC. At 4 to 12 weeks follow-up, LDC was associated with a greater mean reduction in SBP than initial monotherapy or usual care (mean reduction, 7.4 mm Hg; 95% CI, 4.3-10.5) and placebo (mean reduction, 18.0 mm Hg; 95% CI, 15.1-20.8). LDC was associated with a higher proportion of participants achieving BP less than 140/90 mm Hg at 4 to 12 weeks compared to both monotherapy or usual care (66% vs 46%; RR, 1.40; 95% CI, 1.27-1.52) and placebo (54% vs 18%; RR, 3.03; 95% CI, 1.93-4.77). There was no significant heterogeneity between trials enrolling patients with and without baseline BP-lowering therapy. Results from 2 trials indicated LDC remained superior to monotherapy or usual care at 6 to 12 months. LDC was associated with more dizziness (14% vs 11%; RR 1.28, 95% CI 1.00-1.63) but no other adverse effects nor treatment withdrawal.
Conclusions and Relevance
The findings in the study showed that LDCs with 3 or 4 antihypertensives were an effective and well-tolerated BP-lowering treatment option for the initial or early management of hypertension.
Introduction
Globally, blood pressure (BP) control is inadequate, with fewer than 1 in 3 people with hypertension achieving BP targets in high-income countries and fewer than 1 in 10 in middle- and low-income countries.1,2 Hypertension treatment guidelines traditionally recommended initiation of treatment with a single BP-lowering agent and more recently have recommended starting with dual combinations for an increasing proportion of people.3,4 These guidelines only recommend triple combination therapy in those whose BP remains uncontrolled with dual therapy.3,4 However, trial data have recently emerged relating to a new paradigm of hypertension treatment, indicating that low-dose combinations (LDCs) of 3 or more BP-lowering agents (also referred to as hypertension polypills), are a potentially useful initial or early treatment strategy. The pharmacological rationale, outlined almost 20 years ago, was that most BP-lowering effects can be maintained and most adverse effects avoided at low dosages5 and that there are additive effects when combining agents from different classes.5,6
To our knowledge, there has been no review comparing the evidence generated for these hypertension polypills. It is unclear whether an initial LDC strategy is associated with more adverse effects than usual care and whether usual care eventually catches up to an initial LDC strategy in terms of hypertension control. Therefore, the aim of the current study was to assess the efficacy and safety of LDC BP-lowering drugs that contain 3 or 4 drug classes as the initial strategy for the management of hypertension in randomized clinical trials.
Methods
We performed a systematic literature search in PubMed and Medline from date of inception to September 2022 to identify randomized clinical trials of low-dose triple or quadruple combinations. Two reviewers (N.W. and P.R.) independently reviewed the articles against predefined inclusion criteria: randomized clinical trials (parallel or crossover) of triple or quadruple low-dose combinations of BP-lowering drugs. Low dose was defined as the use of BP-lowering drugs at half or less than half the standard dose, using methods from Bennett et al.7 Studies were only considered if at least 1 arm was allocated to triple or quadruple LDC therapy and at least 1 arm to placebo, monotherapy, or usual care. Studies were included only if BP-lowering efficacy was reported (the presence of adverse effects data was not a requirement for inclusion).
Study Outcomes
The primary outcome of interest was the mean reduction in systolic BP (SBP) between LDC and active comparator and/or placebo. Other outcomes of interest included the proportion of patients achieving a BP less than 140/90 mm Hg, proportion experiencing adverse effects, and treatment withdrawal. We assessed these outcomes at both short-term follow-up (4 to 12 weeks) and longer-term follow-up (6 to 12 months), as reported by the included trials.
Statistical Analysis
We performed a random-effects meta-analysis with inverse variance weighting. For those models with low heterogeneity (I2 < 50%), we used a fixed effects model to obtain more precise estimates. Binary outcomes were summarized using risk ratios (RRs) and continuous outcomes using mean difference with 95% CIs. We compared LDC (either triple or quadruple combination therapy) to either placebo or an active comparator (initial monotherapy or usual care). Subgroup analyses were conducted to test for heterogeneity between trials that included patients with prior baseline antihypertensive use and those that excluded patients using antihypertensives at baseline. Data were analyzed using Comprehensive Meta-Analysis version 3 (Biostat). Two-tailed P values <.05 were considered significant.
Results
The initial search identified 498 articles, with 13 proceeding to full-text evaluation and 7 included in the final analysis, totaling 1918 patients (mean [mean range] age, 59 [50-7] years; 739 [38%] female) (eAppendix in Supplement 1). Five of the trials were short term (4 to 12 weeks follow-up),8,9,10,11,12 and 2 reported outcomes at 6 to 12 months follow-up.13,14 Five of the 7 trials included active comparators (either monotherapy or usual care), and 4 of the 7 included a placebo comparator. Four trials involved triple component (3 drug classes) LDC,8,11,12,14 and 3 used quadruple component (4 drug classes) LDC9,10,13 (Table).
Table. Characteristics of Included Trials.
| Source | Study design | No. of patients | Treatment with antihypertensive at baseline, No. (%) | Fixed dose of LDC regimen | LDC pill | Comparator(s) | Baseline BP, mm Hg | Follow-up duration |
|---|---|---|---|---|---|---|---|---|
| TRIUMPH,14 2018 | Open label RCT | 700 | 287 (41) | No | Telmisartan, 20 mg; amlodipine, 2.5 mg; chlorthalidone 12.5 mg | Usual care | 154/90 | 6 mo |
| QUARTET,13 2021 | Double-blinded RCT | 591 | 273 (46) | No | Irbesartan, 37.5 mg; amlodipine, 1.25 mg; indapamide, 0.625 mg; bisoprolol, 2.5 mg | Irbesartan, 150 mg | 152/88 | 12 mo |
| Mahmud and Feely,9 2007 | Open label RCT | 108 | 0 | Yes | Amlodipine, 1.25 mg; atenolol, 12.5 mg; bendroflumethiazide, 0.625 mg; captopril, 12.5 mg | Amlodipine, 5 mg, or atenolol, 50 mg, or bendroflumethiazide, 2.5 mg, or captopril, 100 mg | 160/96 | 4 wk |
| Hong et al,8 2020 | Double-blinded RCT | 238 | 0 | Yes | Losartanm, 25 mg; amlodipine, 2.5 mg; chlorthiadone, 6.25 mg | Amlodipine, 5 and 10 mg; losartan, 100 mg; placebo | 154/91 | 8 wk |
| Chow et al,10 2017 | Double-blinded RCT, crossover | 21 | 0 | Yes | Irbesartan, 37.5 mg; amlodipine, 1.25 mg; hydrochlorothiazide, 6.25 mg; atenolol, 12.5 mg | Placebo | 154/90 | 4 wk |
| Sung et al,11 2022 | Double-blinded RCT | 176 | 158 (90) | Yes | Telmisartan, 20 mg; amlodipine, 2.5 mg; chlorthiadone, 6.25 mg | Amlodipine, 5 and 10 mg; losartan, 100 mg; placebo | 151/92 | 4 wk |
| Wald et al,12 2012 | Double-blinded RCT, crossover | 86 | 86 (100) | Yes | Amlodipine, 2.5 mg; losartan, 25 mg; hydrochlorothiazide, 12.5 mg; simvastatin, 40 mg | Placebo | 143/86 | 12 wk |
Abbreviations: BP, blood pressure; LDC, low-dose combination; RCT, randomized clinical trial.
BP-Lowering Efficacy of LDC Therapies
In all 7 trials, LDC therapy was associated with significant reductions in SBP, with SBP falling between 16 to 28 mm Hg at early follow-up (4 to 12 weeks) in the LDC group and 12 to 18 mm Hg in the initial monotherapy or usual care group (Figure 1). These reductions in SBP with LDC were sustained at 6 and 12 months (Figure 1). LDC was associated with a greater mean reduction in SBP compared to initial monotherapy or usual care at early follow-up (mean difference, 7.4 mm Hg; 95% CI, 4.3-10.5) (Figure 2). There was no significant heterogeneity in treatment effect between trials that included participants who were not taking baseline BP-lowering therapy vs those that included some patients taking prior baseline therapy, nor was there significant heterogeneity between trials that were double-blinded vs open label. LDC was associated with greater mean reduction in SBP compared to placebo at early follow-up (mean difference, 18.0 mm Hg; 95% CI, 15.1-20.8), with no significant heterogeneity between trials that included patients with and without baseline BP-lowering therapy. Compared to initial monotherapy or usual care, LDC was associated with greater reduction in mean SBP at 6 to 12 months follow-up (mean difference, 6.4 mm Hg; 95% CI, 1.8-11.0) (Figure 2).
Figure 1. Mean Systolic Blood Pressure (SBP) During Baseline and Follow-up in Trials of Low-Dose Combination (LDC) Blood Pressure–Lowering Drugs Containing 3 or 4 Agents.
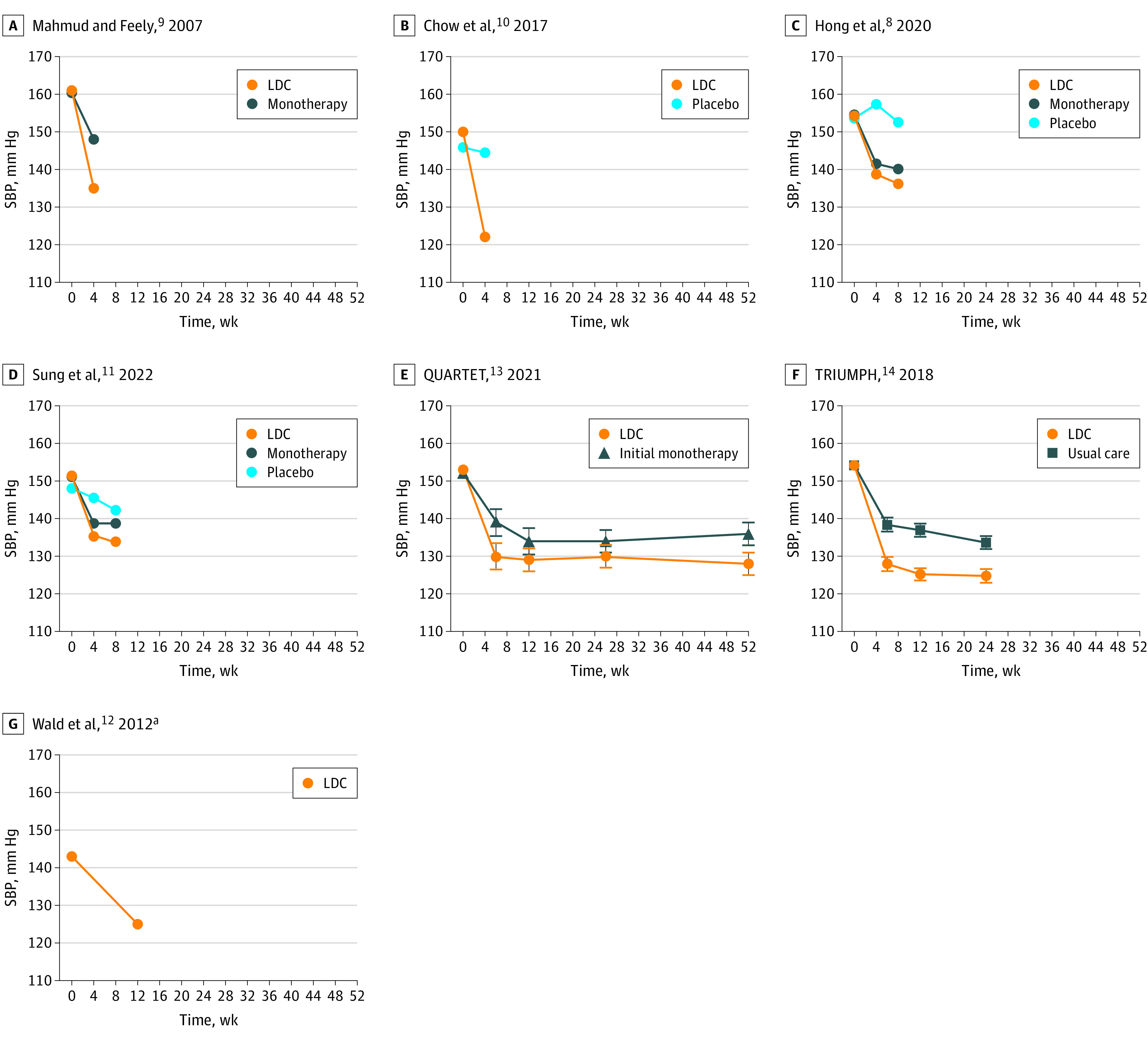
Error bars represent 95% CIs. QUARTET indicates the Quadruple Ultra-Low-Dose Treatment for Hypertension trial; TRIUMPH, the Treatment for Immune Mediated Pathophysiology trial.
aWald et al12 did not report blood pressure levels in the placebo arm.
Figure 2. Low-Dose Combination (LDC) Therapy vs Active Comparator for Reducing Systolic Blood Pressure (SBP).
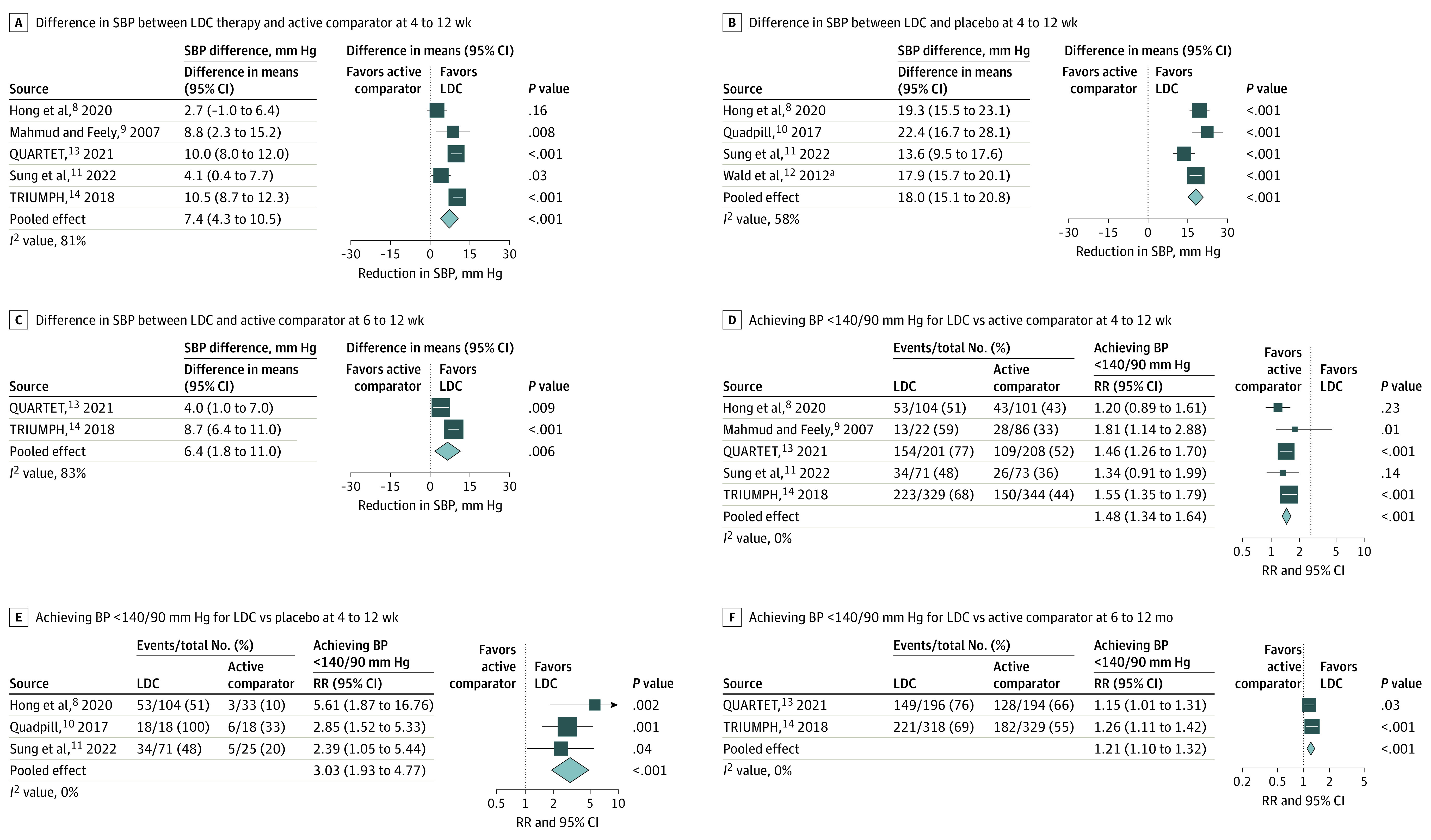
Squares represent individual studies, with the size proportional to the weight in the meta-analysis. Horizontal lines and width of diamonds show 95% CIs. RR indicates risk ratio.
aWald et al12 was a crossover randomized trial design and did not report BP levels in the placebo arm.
Compared to initial monotherapy or usual care, LDC was associated with a significantly greater proportion of patients achieving BP less than 140/90 mm Hg at 4 to 12 weeks (66% vs 46%; RR, 1.40; 95% CI, 1.27-1.52), with no significant heterogeneity between trials of patients with and without baseline BP-lowering therapy, and no significant heterogeneity between double-blinded vs open-label trials (Figure 2). Similarly, at 6 to 12 months follow-up, compared to initial monotherapy or usual care, LDC was associated with significantly greater proportions achieving BP less than 140/90 mm Hg (72% vs 59%; RR, 1.21; 95% CI, 1.10-1.32) (Figure 2). Compared to placebo, LDC was also associated with significantly greater proportions achieving BP less than 140/90 mm Hg at 4 to 12 weeks follow-up (54% vs 18%; RR, 3.03; 95% CI, 1.93-4.77) (Figure 2).
Adverse Effects and Tolerability
Overall, there was a low absolute risk of adverse events with LDC, active comparator, and placebo. Compared to active comparator, LDC therapy was associated with greater proportions experiencing dizziness (14% vs 11%; RR, 1.28; 95% CI, 1.00-1.63) but not with other adverse effects, including peripheral edema, headache, musculoskeletal pain, or serious adverse effects (eAppendix in Supplement 1). The number of treatment withdrawals due to adverse effects was not significantly different between LDC therapy and active comparator but confidence intervals were wide (5% vs 4%; RR, 1.14; 95% CI, 0.71-1.82). Compared to placebo, LDC had similar proportions experiencing adverse effects and treatment withdrawal (eAppendix in Supplement 1). Self-reported treatment adherence was similar in the LDC arm compared to active comparator (eAppendix in Supplement 1).
Discussion
This systematic review and meta-analysis found that LDC BP-lowering therapies with 3 or 4 agents were safe and effective as an initial BP-lowering treatment strategy for hypertension in the 7 included studies. The BP-lowering effects observed after a few weeks with LDC therapy were sustained at 6 to 12 months. LDC therapy was associated with more dizziness but not with other adverse effects, and treatment withdrawal due to adverse effects was similar between LDC therapy, monotherapy or usual care, and placebo. The use of LDC as initial therapy achieved BP control in 66% of patients, although that would mean around 34% might be expected to require treatment intensification to achieve better control rates. Despite the efficacy observed in these trials, additional novel BP-lowering therapies (both pharmacological and novel interventions) may be required in those with resistant hypertension.
Usual care did not eventually catch up to an initial LDC strategy in terms of hypertension control. At 6 months in the Quadruple Ultra-Low-Dose Treatment for Hypertension (QUARTET)13 and Treatment for Immune Mediated Pathophysiology (TRIUMPH)14 trials, LDC was associated with a 21% greater rate of achieving BP less than 140/90 mm Hg compared to the initial monotherapy strategy. Importantly, LDC therapies were well tolerated and were not associated with greater rates of treatment withdrawal than initial monotherapy strategies.
Limitations
The study has several limitations to address. First, the included trials differed in the choice of antihypertensives used in each LDC. Several trials included patients who were taking BP-lowering drugs at baseline. However, our analyses showed that the results were consistent among those trials that did and did not include patients who were taking BP-lowering therapy at baseline. Although 2 of the included trials were open label, we did not find any significant heterogeneity between those trials and double-blinded trials for the primary outcome. There were relatively few included studies, particularly with analyses at 6 to 12 months follow-up. Some analyses may be underpowered to detect a difference in adverse effects. Trials of other antihypertensive combinations and use in other patient populations are needed. This study was not powered to investigate for clinical event reduction, although we would expect better BP control to translate to proportionally lower adverse cardiovascular events.15
Conclusions
In this study, LDC with 3 or 4 antihypertensives provided an effective and well-tolerated BP-lowering treatment option for the initial management of hypertension. LDC antihypertensives provide a single-step solution that has been shown to achieve 70% sustained BP control rates—an important therapeutic advance. However, to achieve long-term control rates even higher than this, further research on the best strategy to tolerably intensify therapy for people taking LDCs is required.
eAppendix
Data sharing statement
References
- 1.Chow CK, Teo KK, Rangarajan S, et al. ; PURE (Prospective Urban Rural Epidemiology) Study investigators . Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. JAMA. 2013;310(9):959-968. doi: 10.1001/jama.2013.184182 [DOI] [PubMed] [Google Scholar]
- 2.Webster RJ, Heeley EL, Peiris DP, Bayram C, Cass A, Patel AA. Gaps in cardiovascular disease risk management in Australian general practice. Med J Aust. 2009;191(6):324-329. doi: 10.5694/j.1326-5377.2009.tb02816.x [DOI] [PubMed] [Google Scholar]
- 3.Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71(19):e127-e248. doi: 10.1016/j.jacc.2017.11.006 [DOI] [PubMed] [Google Scholar]
- 4.Williams B, Mancia G, Spiering W, et al. ; ESC Scientific Document Group . 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J. 2018;39(33):3021-3104. doi: 10.1093/eurheartj/ehy339 [DOI] [PubMed] [Google Scholar]
- 5.Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose combination treatment with blood pressure lowering drugs: analysis of 354 randomised trials. BMJ. 2003;326(7404):1427. doi: 10.1136/bmj.326.7404.1427 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Salam A, Atkins ER, Hsu B, Webster R, Patel A, Rodgers A. Efficacy and safety of triple versus dual combination blood pressure-lowering drug therapy: a systematic review and meta-analysis of randomized controlled trials. J Hypertens. 2019;37(8):1567-1573. doi: 10.1097/HJH.0000000000002089 [DOI] [PubMed] [Google Scholar]
- 7.Bennett A, Chow CK, Chou M, et al. Efficacy and safety of quarter-dose blood pressure–lowering agents: a systematic review and meta-analysis of randomized controlled trials. Hypertension. 2017;70(1):85-93. doi: 10.1161/HYPERTENSIONAHA.117.09202 [DOI] [PubMed] [Google Scholar]
- 8.Hong SJ, Sung K-C, Lim S-W, et al. ; HM_APOLLO Investigators . Low-dose triple antihypertensive combination therapy in patients with hypertension: a randomized, double-blind, phase II study. Drug Des Dev Ther. 2020;14:5735-5746. doi: 10.2147/DDDT.S286586 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mahmud A, Feely J. Low-dose quadruple antihypertensive combination: more efficacious than individual agents–a preliminary report. Hypertension. 2007;49(2):272-275. doi: 10.1161/01.HYP.0000254479.66645.a3 [DOI] [PubMed] [Google Scholar]
- 10.Chow CK, Thakkar J, Bennett A, et al. Quarter-dose quadruple combination therapy for initial treatment of hypertension: placebo-controlled, crossover, randomised trial and systematic review. Lancet. 2017;389(10073):1035-1042. doi: 10.1016/S0140-6736(17)30260-X [DOI] [PubMed] [Google Scholar]
- 11.Sung KC, Sung JH, Cho EJ, et al. Efficacy and safety of low-dose antihypertensive combination of amlodipine, telmisartan, and chlorthalidone: a randomized, double-blind, parallel, phase II trial. J Clin Hypertens (Greenwich). 2022;24(10):1298-1309. doi: 10.1111/jch.14570 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wald DS, Morris JK, Wald NJ. Randomized polypill crossover trial in people aged 50 and over. PLoS One. 2012;7(7):e41297. doi: 10.1371/journal.pone.0041297 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chow CK, Atkins ER, Hillis GS, et al. ; QUARTET Investigators . Initial treatment with a single pill containing quadruple combination of quarter doses of blood pressure medicines versus standard dose monotherapy in patients with hypertension (QUARTET): a phase 3, randomised, double-blind, active-controlled trial. Lancet. 2021;398(10305):1043-1052. doi: 10.1016/S0140-6736(21)01922-X [DOI] [PubMed] [Google Scholar]
- 14.Webster R, Salam A, de Silva HA, et al. ; TRIUMPH Study Group . Fixed low-dose triple combination antihypertensive medication vs usual care for blood pressure control in patients with mild to moderate hypertension in Sri Lanka: a randomized clinical trial. JAMA. 2018;320(6):566-579. doi: 10.1001/jama.2018.10359 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ettehad D, Emdin CA, Kiran A, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387(10022):957-967. doi: 10.1016/S0140-6736(15)01225-8 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eAppendix
Data sharing statement