

Abstract
Prior research has linked deficits in executive control (EC) to marijuana use in adolescents but has relied either primarily on adolescent self-report of EC or tasked-based EC, and focused on limited aspects of EC, usually inhibitory control. We examined unique associations of three established aspects of EC (inhibitory control, working memory, and flexible shifting) assessed with both performance on laboratory tasks and self-report in relation to marijuana initiation. Participants were 260 youth (ages 14-18 years) from a small Midwestern city in the United States enrolled in the adolescent phase (beginning in 2017) of an ongoing study of EC development recruited originally between 2006 and 2012 (46% male, 72% European American). The three aspects of executive control were measured in a laboratory setting with well-established performance-based measures and with a psychometrically-sound self-report survey instrument. Youth also provided self-report of marijuana initiation in a phone survey administered during their laboratory visit. Multiple logistic regression analysis indicated that flexible shifting as measured by a performance-based task was negatively and uniquely associated with marijuana initiation (AOR = 0.68, 95% CI = 0.48 – 0.91), and self-reported deficits in inhibitory control were positively associated with marijuana initiation (AOR = 1.92, 95% CI = 1.15 – 3.21). Although larger-scale longitudinal research is needed, findings of this study suggest that screening efforts to identify youth at risk of marijuana initiation might rely on more cost- effective self-report assessment of inhibitory control, but further valuable information can come from more resource-intensive but sensitive performance-based assessment of flexible shifting.
Keywords: executive control, adolescence, marijuana, initiation
Marijuana is a commonly used substance among adolescents in the United States. The overall prevalence of lifetime and annual marijuana use has remained relatively stable; for example, there was no change in the lifetime prevalence of marijuana use among 12th grade students from 2019 to 2020 (43.7% in both years; Miech et al., 2021). By contrast, the prevalence of daily or near-daily marijuana use in the past 30 days has increased recently (e.g., from 6.4% in 2019 to 6.9% in 2020 among 12th grade students; Miech et al., 2021), corresponding to the declines in perceived harm of marijuana use among adolescents (Johnston et al., 2021). Early initiation of marijuana may adversely affect youth’s mental health (e.g., affective disorder; Levine et al., 2017), and increase their chances of developing marijuana dependence in adulthood (Paige & Colder, 2020).
Executive Control in Adolescence
Research to elucidate modifiable factors associated with adolescent marijuana use can help guide the design of interventions for preventing such use and its potential adverse consequences (Mason et al., 2016). One important factor is executive control (EC; also termed executive function), which refers to high-level cognitive processes involved in the regulation of behavior (Diamond, 2013). EC becomes organized and can be measured as a unitary construct in early childhood (Espy, 2016). With increasing brain maturation throughout childhood and into adolescence, differentiation of EC occurs (Lee et al., 2013; Nelson et al., 2022). Although additional research on the structure of EC among adolescents is needed, current models suggest that EC differentiation into early adulthood increasingly can be partitioned into three aspects, including inhibitory control (the ability to inhibit prepotent responses), working memory (the ability to hold information temporarily and work with it), and flexible shifting (the ability to shift between changing task demands) (Friedman & Miyake, 2017; Lee et al. 2013; Miyake et al., 2000; Nelson et al., 2019).
Research on Composite EC and Adolescent Substance Use
EC has been studied as a composite measure in relation to adolescent substance use, which has most often referred to alcohol and tobacco use or general substance use in a combined measure (sometimes including marijuana). Shoal and Giancola (2001) examined the relationship between composite EC and substance use frequency and problems in a sample of adolescent males. Substances included alcohol, marijuana, and other drugs measured as a combined variable. They used a battery of neuropsychological tests (e.g., the Porteus Maze Test, the Stroop Test) and combined them to form a latent EC factor. Results showed that a high-risk group of individuals with a family history of substance use disorder had significantly lower EC than a low-risk group of individuals without a family history of substance use disorder. Better EC predicted less substance use frequency and less substance use problems in the high-risk group, but not in the low-risk group. Composite EC also has been shown to be significantly related to adolescent cigarette and alcohol use (Pentz & Riggs, 2013; Pentz et al., 2015). For example, Pentz and Riggs (2013) examined the relationship between executive control and substance use in a sample of fourth grade children. This study used the self-report Behavioral Rating Inventory of Executive Function (BRIEF) to measure executive control and combined lifetime cigarette and alcohol use into an overall measure of substance use. Strong EC was significantly related to less substance use 6 months later, controlling for gender, ethnicity, out-of-school physical activity, exercising with parent, baseline substance use, and socioeconomic status. Pentz and colleagues (2015) found that executive function problems, also measured via the BRIEF, were significantly positively related to e-cigarette, cigarette, and alcohol use. Adolescents with executive function problems were more than two times as likely to use cigarettes and alcohol and around five times as likely to use e-cigarettes, as adolescents without such problems.
Research on Specific EC Dimensions and Adolescent Substance Use
Important as these studies have been, they leave significant gaps in knowledge because each of the three aspects of EC may have independent associations with adolescent substance use. For example, inhibitory control can be a factor in inhibiting substance use when it is available, such as in response to offers from peers. Working memory is crucial in holding and manipulating substance use-related information that might help prevent substance use in the moment. Flexible shifting is critical in choosing healthy, safe behaviors and in diverting attention away from substance-related cues (Fleming et al., 2020; Nelson et al., 2019). However, research on specific EC aspects has tended to focus on measures of inhibitory control to the exclusion of other aspects (see Nelson et al., 2019), and studies typically have not examined marijuana use, specifically, or have incorporated such use into combined measures of general substance use. For instance, studies have consistently shown that inhibition predicts substance initiation and use among adolescents (Mahmood et al., 2013; Squeglia et al., 2014; Tarter et al., 2003, 2004; Wills et al, 2006). Tarter and colleagues (2003) used three constructs to measure neurobehavioral disinhibition, including affective disinhibition (measured by the Revised Dimensions of Temperament Survey), behavioral disinhibition (measured by the number of conduct disorder, ODD, and ADHD symptoms reported on K-SADS- E and the total score on the Disruptive Disorders Rating Scale), and cognitive disinhibition (measured by the Stroop, Porteus Maze, Vigilance, Motor restraint, Forbidden toys, and Block Design tests). The frequency of general substance use (alcohol, tobacco, marijuana, and other drugs combined) was measured at age 16 with reference to the prior 30 days, and substance use disorder diagnosis and severity were measured at age 19. This study found that neurobehavioral disinhibition at age 16 significantly discriminated boys at low and high risk for substance use disorder at age 19. Mahmood and colleagues (2013) used the Go/No- Go task during an fMRI session to measure response inhibition and conducted a detailed interview to measure substance use and dependence in a sample of 80 adolescents aged 16-19 years (39 with a history of high frequency substance use and 41 with low frequency use). Substance use was measured by questions about lifetime and past 3-month use of alcohol, marijuana, nicotine, and eight other illicit drugs at baseline, and by past 18-month use of those substances at follow-up. Of note, alcohol was measured alone, and marijuana was incorporated into a combined measure with other substances. They found that atypical activation patterns in the prefrontal cortex during the Go/No-Go task (particularly during No-Go trails) were associated with greater alcohol and other substance use 18 months later.
Studies examining other EC aspects in relation to adolescent substance use are few in number. For example, working memory has been shown to predict alcohol and tobacco use (Khurana et al., 2013; Romer et al., 2011). Khurana and colleagues (2013) indicated that pre- existing deficits in working memory predicted both concurrent alcohol use and increased frequency of drinking over four-year follow-ups among early adolescents, though this effect was mediated fully by impulsivity. This study used the Digit Span, Visual Spatial Working Memory, Corsi Block Tapping, and Letter Two-Back tasks to measure working memory. Romer and colleagues (2011) found that working memory was inversely related to subsequent alcohol and tobacco use; however, substance use was measured together with fighting and gambling as one construct. Working memory was measured by the Corsi Block Tapping, Letter two-back, Digit span, and Spatial Working Memory tasks. Working memory has also been shown to be unrelated to alcohol, tobacco, and other substance use (Nigg et al., 2006; Romer et al., 2009).
Research on Composite EC and Specific EC Dimensions and Adolescent Marijuana Use
Taken together, the literature reviewed above indicates that additional studies addressing all three EC aspects simultaneously are needed. Moreover, many prior studies have excluded marijuana or only incorporated it into measures of general substance use. Still, similar to studies of EC in relation to other substances, studies that have examined marijuana use as a separate outcome have restricted their attention to composite EC or to particular EC aspects. For example, deficits in composite EC in childhood, at ages 10-12-years of age, have been shown to predict early adolescent marijuana, tobacco, and alcohol use measured separately at 2-year follow- up (Aytaclar et al., 1999). Findings from extant research indicate that inhibitory control problems are associated with the early initiation and use of marijuana (e.g., Tarter et al., 2003; Squeglia et al., 2014; Wills et al., 2006). Wills and colleagues (2006) found that poor behavior control and poor emotion control were positively associated with marijuana, alcohol, and tobacco use among adolescents aged 12-16-years. Squeglia and colleagues (2014) reported that inhibitory functioning, measured via neuropsychological tests, in early adolescence was related to subsequent marijuana use frequency and intensity by late adolescence; however, early adolescent cognitive functioning including short- term memory was not related to alcohol and marijuana use in late adolescence. Moreover, attention dysfunction, a measure of flexible shifting deficiency, has been shown to predict substance use (e.g., alcohol, marijuana, and stimulants; Tapert et al., 2002). Tapert and colleagues (2002) reported that poorer attention, measured via performance-based tasks (i.e., Digits Forward, Digits Backward, Arithmetic and Coding, and Trails tasks) was associated with greater substance use frequency, and particularly with more marijuana use, in a community sample of adolescents, above and beyond preexisting substance use levels.
Summary of Research Gaps
In summary, there are at least three significant gaps in prior research on EC and adolescent substance use. First, relevant studies often have represented EC as either a general construct (e.g., Aytaclar et al., 1999) or as only one aspect, usually inhibition (e.g., Squeglia et al., 2014). Second, studies in this area of research have either relied on questionnaire-based assessments of EC (e.g., Pentz & Riggs, 2013; Wills et al., 2006) or performance-based tasks (e.g., Tapert et al., 2002; Mahmood et al., 2013) only, but typically have not used multiple assessment methods and compared them in adjusted analyses. In one known exception, Hagen and colleagues (2016) compared performance- based executive function tasks and a self-report questionnaire assessment of executive function problems, finding that executive function tasks displayed modest, and self-report assessment displayed robust, ability to distinguish adults with and without substance use disorder. Toplak and colleagues (2013) concluded that the relationships between BRIEF self-report and performance-based measures of EC were fairly weak in both clinical and non-clinical samples of children, adolescents, and young adults, suggesting that self-reported and performance- based measures of EC assess different underlying constructs to some degree. Self-report measures (e.g., BRIEF) tap into the difficulties experienced in everyday activities, whereas performance- based measures refer to individual’s decision- making abilities under standardized conditions and consider individual’s response time and accuracy (Toplak at el., 2013). To extend Hagen et al. (2016), similar studies comparing self-report questionnaire and performance-based EC assessments during adolescence, a period of ongoing brain maturation and associated EC development (Bava & Tapert, 2010), are needed. Third, many studies in this area of research have focused on alcohol and tobacco use or general substance use. Prior research that has examined marijuana-related outcomes, specifically, has been informative (e.g., Tapert et al., 2002), but has been limited by narrow, mono-method EC assessment. Thus, little is known about the degree to which the three aspects of EC might have independent associations with adolescent marijuana use, and whether associations are evident when using both performance-based tasks and a questionnaire-based assessment completed in a laboratory setting.
The Current Study
This study addresses key gaps in the literature by examining the independent associations of performance-based abilities as well as self-reported deficits in inhibitory control, working memory, and flexible shifting in relation to marijuana initiation in adolescents (ages 14-18 years) from the general population. It was expected that EC aspects as reflected by both performance-based and self-reported tasks would be associated with marijuana use initiation. Given prior research, we expected associations to be strongest for measures of inhibitory control.
METHODS
Participants
Participants were 260 adolescents (45.7% male), aged 14-18 years (M = 16.22, SD = 1.32), who are part of an ongoing study of the development and consequences of EC (Espy, 2016). Families with preschool age children (M = 4.12, SD = 0.97) from a small Midwestern city enrolled in the study between 2006 and 2012 and have been followed over time. Here, we used data from enrolled youth who participated in the adolescent phase of the study. The analysis sample is 72% European American, 4% African American, < 1% Asian, and 23% multiracial; 13% are Latino/Hispanic ethnicity. A third of their families (33%) were headed by one parent upon enrollment into the larger study and the median household income was $42,000 per year. Slightly less than half (44%) of mothers had a college or post-graduate degree. More information on recruitment and assessment procedures is provided in James et al. (2016).
Procedures
Families enrolled in the original study have been asked to participate in the adolescent phase of the ongoing study. Specifically, beginning in 2017, participating youth have been assessed annually around the time of their birthdays from ages 14-18 years. These assessments involve both an in-person laboratory visit and a phone survey. Due to the larger study’s original cohort- sequential design, participants ranged in age from 10 to 16 years at the beginning of the adolescent data collection. Thus, some participants were not yet age 14, the age at which participants became eligible for the adolescent phase of the study, when the new phase began. In the current analyses, we use data collected through May 2021, by which time the youngest cohort had aged into the adolescent phase of the study at age 14. Adolescents who completed at least one phone survey (n = 260) and, therefore, gave information on adolescent marijuana initiation make up the analysis sample for the current study. Parents/legal guardians gave informed consent for both adolescent participation and their own participation. Adolescent participants gave informed assent. The Institutional Review Board of the University of Nebraska-Lincoln approved all procedures.
Measures
Task-based measures of EC abilities. Measures of adolescent EC included well- established neuropsychological tasks capturing abilities in inhibitory control, working memory, and flexible shifting. Tasks were administered to individual participants by trained research assistants during laboratory visits. For all three tasks, higher scores indicate better EC abilities. Each task is described briefly below, and further details are available elsewhere (Nelson et al., 2020). Inhibitory control was assessed with the computerized version of the Go/No-Go task (adapted from Bezdjian et al., 2009). During this task, the participant is asked to press a button when any letter except X, Y, or Z appears on the computer screen. A buzzer sound is provided if the participant presses the button incorrectly, when any of the excluded letters are present on the screen. There are 300 trials including 225 “go” trials and 75 “no-go” trials. The standardized difference between hit rate and incorrect hit rate is used as the outcome variable (d-prime).
Working memory was assessed using the Nebraska Barnyard task, which was adapted for the current study from the Noisy Book task (Hughes et al., 1998). In this performance-based task, the participant is asked to remember animal names in a sequence and press matching boxes on screen in the correct order. In the initial training stage, the participant is provided with a set of nine barnyard animals in a 3 × 3 grid of colored boxes on the screen. The corresponding sound of an animal is produced when the participant presses each animal. The participant is asked to complete nine trials during which animals are removed. The examiner names the animal individually, and the participant is asked to press the colored box that matches the animal. Then, the examiner administers the sequences of animals, which begins with only two animals and increases progressively to a maximum of nine animals until the participant demonstrations deterioration of performance. The participant is scored 0.33 for correctly pressing the box for one animal and is scored 1 for correctly pressing the boxes for a sequence of several animals. The outcome variable is the final summed score throughout all nine trials.
Flexible shifting was assessed with the computerized version of the Shape School- Switching condition task (Espy, 1997; Espy et al., 2006). During this task, the participant is presented with the stimuli of cartoon figures that come in two colors and two shapes, and either wearing a hat or not. The task requires the participant to switch between naming the color of stimuli without a hat and naming the shape of the stimuli with hat. About one-third of the trials are shifted trails, which means the subsequent stimulus is different from the preceding stimulus; two-third of the trials are not shifted trials, which means the subsequent stimulus is the same as the preceding stimulus. The outcome variable is percent correct across the shift trials, which combines accuracy and response time into a single score.
Questionnaire-Based Measures of EC Deficits. Adolescents also completed the Behavior Rating Inventory of Executive Function, Second Edition (BRIEF-2; Gioia et al., 2015) in the laboratory to provide a measure of daily symptoms of problems with EC. The BRIEF-2 has been norm-referenced for youth ages 11-18 years and is widely used. Among the instrument’s available scales, we used the three subscales that correspond to the three main aspects of EC: Inhibit (8 items; e.g., problems with impulsivity); Working Memory (8 items; e.g., problems remembering things); and Shift (8 items; e.g., problems adjusting to changes in routine). Each item was rated on a 3-point Likert-type scale with response options of “Never,” “Sometimes,” or “Often.” In the current analyses, we used adjusted scores, which are raw scores corrected for missingness. The BRIEF-2 has demonstrated acceptable reliability (Inhibit: α = 0.87; Working Memory: α = 0.86; Shift: α = 0.82; Gioia et al., 2015) and construct validity (Jacobson et al., 2020). For all three BRIEF-2 subscales, higher scores indicate greater EC problems.
Marijuana use initiation. In each adolescent phone survey, participants were asked about substances used, including marijuana. Marijuana use initiation was a dichotomous measure (0 = never, 1 = at least once) based on whether a participant reported lifetime use of marijuana by the last age 14-18 survey completed, which was age 14 for 31 participants, age 15 for 56 participants, age 16 for 53 participants, age 17 for 65 participants, and age 18 for 55 participants. For example, initiation was based only on the age 14 survey for those who only completed the age 14 survey, but was based on initiation by age 18 for those who completed an age 18 survey. If a participant reported initiation at a given age, they were not asked the initiation question at subsequent ages. There were 80 marijuana initiators (30.8% of the full sample). Of these, the last survey was at age 14 for 2 (2.5%), age 15 for 16 (20%), age 16 for 13 (16.3%), age 17 for 22 (27.5%), and age 18 for 27 (33.8%). Those who reported ever using marijuana were asked, “At what age did you first use marijuana?” Of the 79 initiators who answered this question, age of first use was 11 for 2 (2.5%), 12 for 10 (12.7%), 13 for 17 (21.5%), 14 for 13 (16.5%), 15 for 15 (19.0%), 16 for 14 (17%), 17 for 7 (8.9%), and 18 for 1 (1.3%).
Covariates. Youth age, sex, maternal education, family socioeconomic status (SES), and family history of alcohol problems were included in the analyses as covariates. The age of participants was determined at the last phone survey completed, ranging from ages 14 to 18 years. Sex of participating youth was female (coded 0) or male (coded 1). Mother’s highest level of education was measured in the background survey at enrollment into the larger study. Family SES was a summary measure based on caregiver reports of family income, student free/reduced lunch status, and family public health insurance status (e.g., Medicaid, CHIP, Champus). Families reporting low income-to-needs ratio (below the poverty line), qualifying for free/reduced lunch status, and/or using public health insurance were classified as “at risk” (coded 1) versus “low-risk” (coded 0 for all other families). A single item completed by caregivers as part of the background survey at enrollment measured if any of the child’s biological parents or grandparents had ever been “diagnosed or treated” for an alcohol problem (coded 1 for family history of alcohol problems and 0 for no family history of alcohol problems). We did not have a measure of other substance use disorders (SUDs) in the family; therefore, this variable was used as a proxy for family history of cannabis use disorder (CUD). Since AUDs are often comorbid with other SUDs, including CUD (Duncan et al., 2015), having a family history of alcohol problems might increase risk for adolescent marijuana initiation.
Previous Publications
This is an ongoing and long-term longitudinal study that began when target children were in preschool. In addition to published reports from earlier phases of the project, we have begun to publish results from analyses in the adolescent phase that examine long-term prediction of childhood EC on co-occurring adolescent psychopathology and substance involvement (Fleming et al., 2020), including tobacco use (Mason et al., 2021). No prior project publications have used adolescent EC data to examine links with marijuana use, a prevalent substance in this sample.
Analysis Plan
A logistic regression model assessing unique associations between different EC measures and marijuana initiation was estimated with Mplus version 8 (Muthén & Muthén, 2017). All six measures of EC were Z-scored (standardized) by adopting the “STANDARDIZE” option in Mplus, as was the measure of mother’s education, while other covariates were dichotomous. The standardization procedure was intended to put all scores on a common metric (mean = 0, standard deviation = 1) by subtracting the mean and dividing by the standard deviation. Therefore, the interpretation of model coefficients was in terms of one standard deviation unit change. Maximum Likelihood Robust estimation was used. Overall, 27 individuals in the analysis model did not complete a laboratory visit and another 11 were missing data on the Go/No-go task, which was not included in an abbreviated laboratory visit administered during the coronavirus pandemic. Multiple imputation conducted in Mplus was used in order to include cases with partially missing data. The imputation model included all study variables, and dichotomous variables were treated as categorical. Forty datasets were imputed, and the logistic regression analyses were conducted on each dataset and then the results were averaged using Rubin’s rules. This approach makes the assumption that data are missing at random conditional on non-missing data on other study variables. A statistical significance criterion of p < .05 was used.
RESULTS
Table 1 shows bivariate correlations among, and descriptive information for, all study variables. All three BRIEF measures were positively associated with marijuana use initiation (r = 0.22 – 0.27) and were strongly correlated (r = 0.60 – 0.73) with one another. The three laboratory measures were moderately positively correlated with one another (r = 0.26 – 0.54), modestly to moderately negatively correlated with the BRIEF measures (r = -0.27 – - 0.08), and had small associations (r = -0.12 – 0.02; d = -0.03 – 0.28) with marijuana use initiation. Although not shown in the table, the Spearman’s correlation between the oldest age and marijuana initiation was (r = 0.32, p < .001). Table 2 reports t-tests comparing marijuana initiators versus non-initiators. The standard deviation unit difference between initiators and non-initiators ranged from d = -0.58 – -0.49.
Table 1.
Correlations and Descriptive Statistics
| MI | Male | FHAP | MEA | LI | LAA | ICT | WMT | FST | PIC | PWM | PS | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) MI | 1.00 | |||||||||||
| (2) Male | -0.06 | 1.00 | ||||||||||
| (3) FHAP | 0.13 | 0.01 | 1.00 | |||||||||
| (4) MEA | -0.07 | 0.00 | -0.16 | 1.00 | ||||||||
| (5) LI | 0.00 | -0.06 | 0.20 | -0.44 | 1.00 | |||||||
| (6) LAA | 0.24 | 0.01 | -0.08 | 0.30 | -0.43 | 1.00 | ||||||
| (7) ICT | -0.06 | -0.02 | -0.02 | 0.30 | -0.18 | 0.24 | 1.00 | |||||
| (8) WMT | 0.02 | 0.02 | -0.01 | 0.28 | -0.22 | 0.32 | 0.41 | 1.00 | ||||
| (9) FST | -0.12 | 0.01 | -0.06 | 0.12 | -0.12 | 0.17 | 0.54 | 0.26 | 1.00 | |||
| (10) PIC | 0.27 | 0.06 | 0.10 | -0.12 | 0.10 | -0.08 | -0.27 | -0.08 | -0.16 | 1.00 | ||
| (11) PWM | 0.22 | -0.04 | 0.14 | -0.08 | 0.12 | -0.05 | -0.19 | -0.08 | -0.15 | 0.73 | 1.00 | |
| (12) PS | 0.24 | -0.13 | 0.12 | -0.07 | 0.11 | -0.07 | -0.12 | -0.12 | -0.08 | 0.60 | 0.70 | 1.00 |
| M | 0.31 | 0.46 | 0.31 | 14.83 | 0.53 | 16.22 | 3.31 | 15.55 | 308.31 | 13.27 | 13.71 | 13.38 |
| SD | 0.46 | 0.50 | 0.46 | 2.12 | 0.50 | 1.32 | 0.68 | 2.28 | 67.18 | 2.90 | 3.18 | 2.90 |
Note. Numbers that are significant at p < .05 are in boldface. MI=marijuana initiation; FHAP=family history of alcohol problems; MEA=mother’s educational attainment; LI=low income; LAA=last age assessed; ICT=inhibitory control task; WMT=working memory task; FST= flexible shifting task; PIC=BRIEF-2 poor inhibitory control; PWM=BRIEF-2 poor working memory; PS=BRIEF-2 poor shifting.
Table 2.
T-tests Comparing Initiators with Non-initiators on Task and BRIEF Scores (Means/Standard Deviations)
| Not initiated | Initiated | t | df | p | |||
|---|---|---|---|---|---|---|---|
| Inhibitory control | 3.35 | 0.69 | 3.24 | 0.66 | 1.12 | 219 | 0.264 |
| Working memory | 15.53 | 2.28 | 15.61 | 2.29 | -0.24 | 231 | 0.808 |
| Flexible shifting | 314.09 | 66.37 | 295.39 | 67.65 | 1.98 | 231 | 0.049 |
| BRIEF-2 poor inhibitory control | 12.75 | 2.84 | 14.43 | 2.70 | -4.24 | 230 | 0.000 |
| BRIEF-2 poor working memory | 13.22 | 2.97 | 14.78 | 3.39 | -3.53 | 230 | 0.000 |
| BRIEF-2 poor shifting | 12.90 | 2.75 | 14.44 | 2.96 | -3.83 | 230 | 0.000 |
Table 3 shows the estimates for the multiple logistic regression model. Among the EC performance-based tasks, the measure of flexible shifting was statistically significantly associated with marijuana initiation; among the BRIEF-2 self-report subscales the measure of inhibitory control was statistically significantly associated with the outcome. A one standard deviation unit increase in the flexible shifting task score was associated with 32% lower odds of marijuana use initiation (AOR = 0.68, 95% CI = 0.48 – 0.97). A one standard deviation unit increase in the BRIEF-2 measure of poor inhibitory control was associated with 92% greater odds of marijuana use initiation (AOR = 1.92, 95% CI = 1.15 – 3.21). The last age assessed was also statistically significant (AORs = 2.05, 95% CI = 1.54 – 2.75). With one standard deviation unit increase of age, the odds of marijuana initiation increased by 105%, indicating that as children get older, they are more likely to initiate marijuana. Figures 1 and 2 show model-predicted probabilities for marijuana initiation up to age 17 (which is slightly above the mean oldest age at which initiation was assessed) by flexible shifting task score and BRIEF-2 measure of poor inhibitory control, respectively, with other model covariates at their sample means. None of the other tasks or BRIEF-2 subscales were reliably associated with marijuana initiation.
Table 3.
Estimates for Logistic Regression Model Predicting Marijuana Use Initiation
| Predictor | AOR | 95% CI | |
|---|---|---|---|
| Low | High | ||
| Male | 0.69 | 0.37 | 1.28 |
| Family history of alcohol problems (0/1) | 1.76 | 0.90 | 3.42 |
| Mother’s educational attainment (zscore) | 0.75 | 0.53 | 1.06 |
| Low income (0/1) | 1.32 | 0.62 | 2.78 |
| Last age assessed (in years) | 2.05 | 1.54 | 2.75 |
| Inhibitory control task (zscore) | 1.12 | 0.73 | 1.72 |
| Working memory task (zscore) | 1.02 | 0.70 | 1.48 |
| Flexible shifting (zscore) | 0.68 | 0.48 | 0.97 |
| BRIEF-2 poor inhibitory control (zscore) | 1.92 | 1.15 | 3.21 |
| BRIEF-2 poor working memory (zscore) | 0.76 | 0.43 | 1.32 |
| BRIEF-2 poor shifting (zscore) | 1.50 | 0.96 | 2.35 |
Note. AOR = adjusted odds ratio; CI = confidence interval.
Figure 1.
Probability of Marijuana Initiation by Flexible Shifting Task
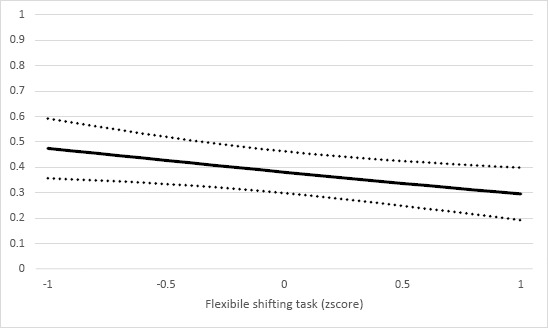
Note. Model-predicted probability of marijuana initiation by age 17 by flexible shifting task score with 95% confidence band.
Figure 2.
Probability of Marijuana Initiation by BRIEF Inhibitory Control
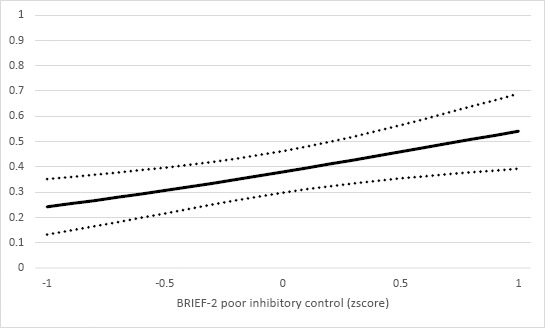
Note. Model-predicted probability of marijuana initiation by age 17 by score on BRIEF Inhibitory Control subscale with 95% confidence band.
DISCUSSION
The current study extends prior research by examining three aspects of EC (inhibitory control, working memory, and flexible shifting) assessed across two methods (performance-based tasks and questionnaire) in relation to adolescent marijuana initiation. Findings support prior research indicating the important role of disinhibition in marijuana use among youth (Squeglia et al., 2014; Tarter et al., 2003), and the increasing risk of initiating marijuana with age (Chen et al., 2017; Kosterman et al., 2000). In a previous study, inhibitory control measured by neuropsychological tests in early adolescence predicted marijuana use by late adolescence (Squeglia et al., 2014). In the current study, we found that self-reported inhibitory control problems in daily life, but not performance on the Go/No-Go task, was associated with marijuana initiation in a model that adjusted for all aspects of EC across both questionnaire and task-based methods. This extends prior research indicating that self-report assessment of EC is robustly associated with adolescent cigarette and alcohol use (Pentz & Riggs, 2013; Pentz et al., 2015) by showing a similar association with marijuana use. The stronger association observed for the self-report measure of inhibitory control may be due to the more contextualized nature of the BRIEF compared to the task-based assessment. Individuals with poor inhibitory control may be less likely to refuse marijuana use offers from peers and, thus, more likely to initiate use. On the contrary, individuals with strong inhibitory control may be able to ignore the cues related to marijuana use from the environment and/or to refuse offers by peers.
Results also indicated that flexible shifting, represented as ability according to performance on a switching task, was negatively associated with marijuana initiation. Similarly, Tapert and colleagues (2002) found that low scores on a performance-based test of attention were related to greater marijuana use among adolescents. Since self-reported and performance-based measures of EC assess different underlying constructs to some degree (Toplak et al., 2013), it is possible that the ability of flexible shifting is better captured as a performance-based ability in a neutral context than as the self-perceived difficulties of flexible shifting in a daily life context (self-report measure of BRIEF). Prior research on adolescent substance use has paid less attention to this aspect of EC, but youth with good flexible shifting ability assessed by performance tasks may be better able to evaluate alternative courses of action and consider the negative consequences of using marijuana (e.g., being found out by parents), and then redirect their attention away from substance-using cues to prosocial activities.
Only working memory was unrelated to marijuana onset regardless of assessment methods in this study. The non-significant relation between working memory and marijuana use is consistent with one prior study (Squeglia et al., 2014), suggesting that the ability to hold and use information in service of cognitive tasks does not appear to be related to adolescents’ marijuana initiation. This may be because working memory is not instrumental in helping adolescents weigh the long-term benefits of prosocial behaviors (e.g., getting good grades in school) against the short- term benefits of using marijuana in the moment. There have been mixed results in prior studies of working memory in relation to other substances and general substance use. Poor performance- based working memory (Digit Span, Visual Spatial Working Memory, Corsi Block Tapping, Letter Two-Back) has been shown to predict adolescent alcohol use and increased frequency of alcohol use (Khurana et al., 2013), as well as onset of first drink and first binge drinking episode above and beyond response inhibition (Self Ordered Pointing Task; Peeters et al., 2015). However, other studies have shown that working memory did not predict substance use in high-risk adolescents (Nigg et al., 2006; Romer et al., 2009).
Limitations
There are a few limitations to this study. All aspects of EC and marijuana initiation were assessed in adolescence (indeed, the youngest cohort had only completed a single laboratory visit at age 14); therefore, temporal ordering could not be established with these cross sectional analyses. Also, only the lifetime initiation of marijuana use was examined as one dimension of marijuana involvement, due to the relatively young age of the youngest cohorts in the sample at this point in time. Given the timing of assessments, initiation might have occurred prior to when EC was assessed for some participants. Longitudinal studies of EC in relation to prolonged and heavier marijuana use later in adolescence and into young adulthood are needed. Family history of alcohol use problems was the only measure available to adjust for substance-related risks in the family. Having a family history of alcohol problems might increase risk for adolescent marijuana initiation because of the comorbidity of alcohol use and marijuana use disorders (Duncan et al., 2015). It was important, therefore, to include this variable as covariate in the current study, but future studies should assess family history of cannabis use disorder to better account for different levels of risks related to adolescent marijuana use. Finally, the sample was drawn from one region of the United States and results might not generalize broadly.
Notwithstanding its limitations, this study extends prior studies of EC and adolescent marijuana use that have only examined global EC or a single aspect, usually inhibitory control, and that have used only a single method for EC assessment. Findings hold promise for identifying effective screening methods to identify youth with patterns of EC that might increase or decrease risk for marijuana initiation. Whereas inhibitory control problems might be readily identifiable through cost-effective self-report methods, flexible shifting might represent a more subtle cognitive function that is best assessed via more resource- intensive but sensitive task-based procedures when it comes to understanding marijuana initiation. Moreover, because EC has been shown to be modifiable (Diamond, 2013; Diamond & Lee, 2011), results might help guide the targeting of specific EC abilities in skills development interventions to potentially prevent marijuana initiation and its adverse consequences in adolescents.
Funding and Acknowledgements:
We have no conflicts of interests to disclose. Funding was provided by the National Institute of Mental Health (MH065668), the National Institute of General Medical Sciences (P20GM130461), and the National Institute on Drug Abuse (DA041738) of the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the funding agencies.
REFERENCES
- Aytaclar, S., Tarter, R. E., Kirisci, L., & Lu, S. (1999). Association between hyperactivity and executive cognitive functioning in childhood and substance use in early adolescence. Journal of the American Academy of Child and Adolescent Psychiatry, 38(2), 172–178. [DOI] [PubMed] [Google Scholar]
- Bava, S., & Tapert, S. F. (2010). Adolescent brain development and the risk for alcohol and other drug problems. Neuropsychology Review, 20(4), 398–413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bezdjian, S., Baker, L. A., Lozano, D. I., & Raine, A. (2009). Assessing inattention and impulsivity in children during the Go/NoGo task. The British Journal of Developmental Psychology, 27(2), 365–383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen, X., Yu, B., Lasopa, S. O., & Cottler, L. B. (2017). Current patterns of marijuana use initiation by age among US adolescents and emerging adults: implications for intervention. The American Journal of Drug and Alcohol Abuse, 43(3), 261–270. [DOI] [PubMed] [Google Scholar]
- Diamond, A. (2013). Executive functions. Annual Review of Psychology, 64(1), 135–168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diamond, A., & Lee, K. (2011). Interventions shown to aid executive function development in children 4 to 12 years old. Science, 333(6045), 959–964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duncan, S. C., Gau, J. M., Farmer, R. F., Seeley, J. R., Kosty, D. B., & Lewinsohn, P. M. (2015). Comorbidity and temporal relations of alcohol and cannabis use disorders from youth through adulthood. Drug and Alcohol Dependence, 149, 80–86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Espy, K. A. (1997). The shape school: Assessing executive function in preschool children. Developmental Neuropsychology, 13(4), 495–499. [Google Scholar]
- Espy, K. A. (2016). The changing nature of executive control in preschool. Monographs of the Society for Research in Child Development, 81(4), 1–179. [DOI] [PubMed] [Google Scholar]
- Espy, K. A., Bull, R., Martin, J., & Stroup, W. (2006). Measuring the development of executive control with the shape school. Psychological Assessment, 18(4), 373–381. [DOI] [PubMed] [Google Scholar]
- Fleming, C. B., Stevens, A. L., Vivero, M., Patwardhan, I., Nelson, T. D., Nelson, J. M., James, T. D., Espy, K. A., & Mason, W. A. (2020). Executive control in early childhood as an antecedent of adolescent problem behaviors: A longitudinal study with performance-based measures of early childhood cognitive processes. Journal of Youth and Adolescence, 49(12), 2429–2440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedman, N. P., & Miyake, A. (2017). Unity and diversity of executive functions: Individual differences as a window on cognitive structure. Cortex, 86, 186–204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gioia, G. A., Isquith, P. K., Guy, S. C., & Kenworthy, L. (2015). BRIEF2: Behavior Rating Inventory of Executive Function, Second Edition. Lutz, FL: Psychological Assessment Resources. [Google Scholar]
- Hagen, E., Erga, A. H., Hagen, K. P., Nesvåg, S. M., McKay, J. R., Lundervold, A. J., & Walderhaug, E. (2016). Assessment of executive function in patients with substance use disorder: A comparison of inventory- and performance-based assessment. Journal of Substance Abuse Treatment, 66, 1–8. [DOI] [PubMed] [Google Scholar]
- Hughes, C., Dunn, J., & White, A. (1998). Trick or treat?: Uneven understanding of mind and emotion and executive dysfunction in “hard-to-manage” preschoolers. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 39(7), 981–994. [PubMed] [Google Scholar]
- Jacobson, L. A., Pritchard, A. E., Koriakin, T. A., Jones, K. E., & Mahone, E. M. (2020). Initial examination of the BRIEF2 in clinically referred children with and without ADHD symptoms. Journal of Attention Disorders, 24(12), 1775–1784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- James, T. D., Choi, H.-J., Wiebe, S. A., & Espy, K. A. (2016). II. The preschool problem solving study: Sample, data, and statistical methods. Monographs of the Society for Research in Child Development, 81(4), 30–46. [DOI] [PubMed] [Google Scholar]
- Johnston, L. D., Miech, R. A., O’Malley, P. M., Bachman, J. G., Schulenberg, J. E., & Patrick, M. E. (2021). 2020 overview key findings on adolescent drug use. Monitoring the Future: National Survey Results on Drug Use, 1–136. [Google Scholar]
- Khurana, A., Romer, D., Betancourt, L. M., Brodsky, N. L., Giannetta, J. M., & Hurt, H. (2013). Working memory ability predicts trajectories of early alcohol use in adolescents: The mediational role of impulsivity. Addiction, 108(3), 506–515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kosterman, R., Hawkins, J. D., Guo, J., Catalano, R. F., & Abbott, R. D. (2000). The dynamics of alcohol and marijuana initiation: patterns and predictors of first use in adolescence. American Journal of Public Health, 90(3), 360–366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, K., Bull, R., & Ho, R. M. (2013). Developmental changes in executive functioning. Child Development, 84(6), 1933–1953. 10.1111/cdev.12096. [DOI] [PubMed] [Google Scholar]
- Levine, A., Clemenza, K., Rynn, M., & Lieberman, J. (2017). Evidence for the risks and consequences of adolescent cannabis exposure. Journal of the American Academy of Child and Adolescent Psychiatry, 56(3), 214–225. [DOI] [PubMed] [Google Scholar]
- Mahmood, O. M., Goldenberg, D., Thayer, R., Migliorini, R., Simmons, A. N., & Tapert, S. F. (2013). Adolescents’ fMRI activation to a response inhibition task predicts future substance use. Addictive Behaviors, 38(1), 1435–1441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mason, W. A., Fleming, C. B., & Haggerty, K. P. (2016). Prevention of marijuana misuse: School-, family-, and community-based approaches. In M. T. Compton (Ed.), Marijuana and mental health (pp. 199–225). Arlington: American Psychiatric Association Publishing. [Google Scholar]
- Mason, W. A., Patwardhan, I., Fleming, C. B., Stevens, A. L., James, T. D., Nelson, J. M., . . . Nelson, T. D. (2021). Associations of childhood executive control with adolescent cigarette and E-cigarette use: Tests of moderation by poverty level. Addictive Behaviors, 119, 106923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miech, R. A., Johnston, L. D., O’Malley, P. M., Bachman, J. G., Schulenberg, J. E., & Patrick, M. E. (2021). Monitoring the Future national survey results on drug use, 1975–2020: Volume I, Secondary school students. Ann Arbor: Institute for Social Research, The University of Michigan. [Google Scholar]
- Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A., & Wager, T. D. (2000). The Unity and diversity of executive functions and their contributions to complex “Frontal Lobe” tasks: A latent variable analysis. Cognitive Psychology, 41(1), 49–100. [DOI] [PubMed] [Google Scholar]
- Muthén, L. K., & Muthén, B. O. (2017). Mplus user’s guide (8th ed.). Los Angeles, CA: Muthen and Muthen. [Google Scholar]
- Nelson, T. D., James, T. D., Nelson, J. M., Johnson, A. B., Mason, W. A., Yaroch, A. L., & Espy, K. A. (2020). Associations between specific components of executive control and eating behaviors in adolescence: A study using objective and subjective measures. Appetite, 154, 104784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nelson, T. D., Nelson, J. M., Mason, W. A., Tomaso, C. C., Kozikowski, C. B., & Espy, K. A. (2019). Executive Control and Adolescent Health: Toward A Conceptual Framework. Adolescent Research Review, 4(1), 31–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nelson, T. D., James, T. D., Nelson, J. M., Tomaso, C. C., & Espy, K. A. (2022). Executive control in elementary school: Factor structure and associations with early childhood executive control. Developmental Psychology. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nigg, J. T., Wong, M. M., Martel, M. M., Jester, J. M., Puttler, L. I., Glass, J. M., Adams, K. M., Fitzgerald, H. E., & Zucker, R. A. (2006). Poor response inhibition as a predictor of problem drinking and illicit drug use in adolescents at risk for alcoholism and other substance use disorders. Journal of the American Academy of Child and Adolescent Psychiatry, 45(4), 468–475. [DOI] [PubMed] [Google Scholar]
- Paige, K. J., & Colder, C. R. (2020). Long-term effects of early adolescent marijuana use on attentional and inhibitory control. Journal of Studies on Alcohol and Drugs, 81(2), 164–172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peeters, M., Janssen, T., Monshouwer, K., Boendermaker, W., Pronk, T., Wiers, R., & Vollebergh, W. (2015). Weaknesses in executive functioning predict the initiating of adolescents’ alcohol use. Developmental Cognitive Neuroscience, 16, 139–146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pentz, M. A., & Riggs, N. R. (2013). Longitudinal relationships of executive cognitive function and parent influence to child substance use and physical activity. Prevention Science, 14(3), 229–237. [DOI] [PubMed] [Google Scholar]
- Pentz, M. A., Shin, H., Riggs, N., Unger, J. B., Collison, K. L., & Chou, C. (2015). Parent, peer, and executive function relationships to early adolescent e-cigarette use: A substance use pathway? Addictive Behaviors, 42, 73–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Romer, D., Betancourt, L. M., Brodsky, N. L., Giannetta, J. M., Yang, W., & Hurt, H. (2011). Does adolescent risk taking imply weak executive function? A prospective study of relations between working memory performance, impulsivity, and risk taking in early adolescence. Developmental Science, 14(5), 1119–1133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Romer, D., Betancourt, L., Giannetta, J. M., Brodsky, N. L., Farah, M., & Hurt, H. (2009). Executive cognitive functions and impulsivity as correlates of risk taking and problem behavior in preadolescents. Neuropsychologia, 47(13), 2916–2926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Excutive Cognitive Functioning, Negative Affectivity, and Drug Use in Adolescent Boys With and Without a Family History of a Substance Use Disorder. Journal of Child & Adolescent Substance Abuse, 10(4), 111–121. [Google Scholar]
- Squeglia, L. M., Jacobus, J., Nguyen-Louie, T. T., & Tapert, S. F. (2014). Inhibition during early adolescence predicts alcohol and marijuana use by late adolescence. Neuropsychology, 28(5), 782–790. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tapert, S. F., Baratta, M. V., Abrantes, A. M., & Brown, S. A. (2002). Attention Dysfunction Predicts Substance Involvement in Community Youths. Journal of the American Academy of Child & Adolescent Psychiatry, 41(6), 680–686. [DOI] [PubMed] [Google Scholar]
- Tarter, R. E., Kirisci, L., Habeych, M., Reynolds, M., & Vanyukov, M. (2004). Neurobehavior disinhibition in childhood predisposes boys to substance use disorder by young adulthood: Direct and mediated etiologic pathways. Drug and Alcohol Dependence, 73(2), 121–132. [DOI] [PubMed] [Google Scholar]
- Tarter, R. E., Kirisci, L., Mezzich, A., Cornelius, J. R., Pajer, K., Vanyukov, M., Gardner, W., Blackson, T., & Claxrk, D. (2003). Neurobehavioral disinhibition in childhood predicts early age at onset of substance use disorder. American Journal of Psychiatry, 160(6), 1078–1085. [DOI] [PubMed] [Google Scholar]
- Toplak, M. E., West, R. F., & Stanovich, K. E. (2013). Practitioner Review: Do performance- based measures and ratings of executive function assess the same construct? Journal of Child Psychology and Psychiatry and Allied Disciplines, 54(2), 131–143. [DOI] [PubMed] [Google Scholar]
- Wills, T. A., Walker, C., Mendoza, D., & Ainette, M. G. (2006). Behavioral and emotional self- control: Relations to substance use in samples of middle and high school students. Psychology of Addictive Behaviors, 20(3), 265–278. [DOI] [PubMed] [Google Scholar]