

Abstract
Introduction Otosclerosis is a common cause of conductive hearing loss in the adult population that is caused by fixation of the stapes footplate. Cochlear otosclerosis may also present with sensorineural or mixed hearing loss. Surgery is the definitive treatment of choice and, during the procedure, sealing of the oval window with autologous tissue graft around the stapes prosthesis has been routinely done to improve hearing outcome and to mitigate postoperative complications.
Objective To evaluate the efficacy of two different types of autologous tissue (vein or fat) grafts as oval window sealing materials in stapedotomy in improving short-term hearing outcomes.
Methods In our study, 70 patients with otosclerosis who underwent primary stapedotomy were included. They were divided into group 1 (vein graft) and group 2 (fat graft) based on the type of sealing material used. All patients were followed-up at the end of 3 months, undergoing an audiometric examination to assess the hearing outcome.
Results A total of 80% ( n = 28) of the patients in group1 had an air-bone gap (ABG) closure < 10dB, and, in group 2, 85.7% had an ABG closure < 10 dB; this difference was found to be statistically insignificant. A total of 42.9% ( n = 15) of the patients in group 1 and of 31.4% ( n = 11) in group 2 had a significant improvement in bone conduction, while 14.3% ( n = 5) of the patients in group 1 and 17.1% ( n = 6) in group 2 had worsening of average bone conduction postoperatively, which was found to be statistically insignificant.
Conclusion Both vein and fat grafts had comparable effects on hearing outcomes when used as sealing materials in stapedotomy.
Keywords: otosclerosis, otospongiosis, stapes surgery, hearing loss, stapedectomy
Introduction
Otosclerosis is a common cause of acquired hearing loss, with a prevalence of between 0.3 and 0.4% in caucasians. 1 It is a disease of the bony labyrinth of the inner ear caused by abnormal bone remodeling in the otic capsule and in the fissula antefenestrum, leading to the fixation of the stapediovestibular joint, consequently impeding sound transmission in the middle ear, resulting in conductive hearing loss. 2 Otosclerosis was classified into clinical and histological types by Schuknecht et al. Clinical otosclerosis is defined as a lesion that fixes the stapes footplate, while histological otosclerosis refers to cases without footplate fixation. 3 Cochlear otosclerosis refers to cases of histological otosclerosis that involve the endosteum of the cochlea without stapes fixation. 4 Although most cases present with conductive hearing loss, ∼ 10% of cases present with sensorineural hearing loss (SNHL), since the cochlea is involved.
The etiology of the disease has been attributed to multiple factors, including genetic, environmental, and hormonal factors. The most important aspect in the diagnosis of the disease includes a positive family history, complete physical examination, head and neck examination, and quantitative testing. A family history of otosclerosis provides a clue to the diagnosis. Otoscopic examination reveals an intact drum with Schwartz sign in the active stage of the disease. Clinically, negative Rinne at 512 Hz is considered a prerequisite before surgery by several otologists. 5 A complete and precise audiological work-out including pure-tone audiometry (PTA) and immittance measurements is mandatory for the diagnosis. Pure tone audiometry shows an air-bone gap (ABG) > 25dB in speech frequencies, indicating conductive hearing loss according to the American Academy of Otolaryngology – Head and Neck Surgery (AAO-HNS) guidelines. Patients with cochlear otosclerosis may present with SNHL. However, fixity of stapes confirmed perioperatively confirms the diagnosis. Radiological imaging such as high-resolution computed tomography (HRCT) of the temporal bone is increasingly used nowadays in the diagnosis, staging, prognosis, planning of the surgery, and in predicting the outcome of the surgery.
Although medical treatment with sodium fluoride is possible, there is no evidence of definitive hearing improvement in such cases. Surgery is the definitive treatment of choice. Both stapedectomy and stapedotomy are commonly performed for otosclerosis, but stapedotomy is the most accepted and well-established procedure for good hearing outcomes in patients with otosclerosis. Initially, surgery for otosclerosis was considered dangerous because of the risk of labyrinthine fistula and of SNHL. Shea perfected stapedectomy in 1956 and used vein graft as sealing material to prevent complications. 7 Stapedotomy involves the use of prosthesis to bridge the incus to the vestibule after fenestration of the oval window.
Sealing the opening of the oval window during stapes surgery is essential to prevent postoperative complications such as perilymph fistula and SNHL. 6 Autologous tissue is routinely used to seal the fenestra around the prosthesis, but the choice of tissue varies between surgeons. Several studies have compared the results of surgeries in terms of hearing outcome, using several prostheses and techniques, but there are less studies comparing hearing outcomes using various types of tissue seals in stapedotomy. Autologous tissues, such as vein, adipose tissue, fascia, perichondrium, and blood, are used as tissue seals in stapedotomy. Synthetic materials, such as absorbable gelatin sponge, have been used as sealing materials by some surgeons; however subsequently, these materials were proven to cause a higher incidence of perilymph fistula, so their use is highly discouraged. 6 The purpose of sealing the fenestration around the prosthesis in stapedotomy is to prevent labyrinthine fistula and to preserve the stability of the prosthesis, thus improving hearing outcomes following surgery. The present study compares hearing outcomes in primary stapedotomy patients using either vein or fat as oval window sealing materials.
Aim
To evaluate the efficacy of two different types of autologous tissue (vein or fat) grafts as oval window sealing materials in stapedotomy in improving short-term hearing outcomes.
Objectives
– To compare ABG closure achieved in each of the two groups, using either vein or fat as sealing material in stapedotomy.
– To assess the difference in bone conduction between both groups.
Material and Methods
This was a prospective comparative study conducted among patients between 20 and 70 years old undergoing primary stapedotomy in our hospital between April 2017 and January 2018. After taking relevant clinical history and performing otologic examination, those with a clinical diagnosis of otosclerosis were subjected to PTA and tympanometry. Patients with a minimum ABG of 25 dB and absent acoustic reflexes were included in the present study. Revision cases, only hearing ear, other associated ear diseases like Meniere, otitis media, and tympanosclerosis were excluded from the present study. The sample size was calculated using the formula for comparison between 2 means with α = 0.05 and power (1- β err) = 0.8 i.e with a power of 80%
Based on the results obtained from previous studies that used ABG to compare the hearing outcomes of different sealing materials and substituting the mean difference in ABG with 4.2 and the standard deviation (SD) with 0.06, the minimum sample size should be 32. Hence, 70 patients were included in the study, with 35 in each group. Patients with a clinical diagnosis of otosclerosis were then taken up for exploratory tympanotomy and the diagnosis of otosclerosis was confirmed on table.
All patients included in the study underwent primary stapedotomy procedures performed by a single experienced surgeon to eliminate experience bias. The procedure involved a small fenestration technique in the posterior half of the stapes footplate with a 0.8mm skeeter drill. All patients had Nitinol piston of 0.4 mm diameter and of varying lengths, between 4.25 and 5 mm, based on individual measurements for the unbiased results. The only difference in the procedure between the two groups was the choice of the oval window sealing material that holds the 0.4 mm piston into 0.8 mm fenestration in the footplate. Based on the type of autologous tissue used as sealing material, patients were allotted into two groups by simple random sampling.
Group 1: Subjects who underwent stapedotomy with vein as sealing material.
Group 2: Subjects who underwent stapedotomy with adipose tissue (fat) as sealing material.
In group 1 (vein graft), a dried sheet of vein graft harvested from the dorsum of the hand of the patient was placed over the fenestra with a crater created in the middle of the graft, into which the piston snuggly fits into the footplate ( Fig. 1 ). In group 2 (fat graft), fat harvested from the ear lobule of the patient was placed anterosuperiorly around the piston in the footplate, which yielded better stability to the piston ( Fig. 2 ).
Fig. 1.
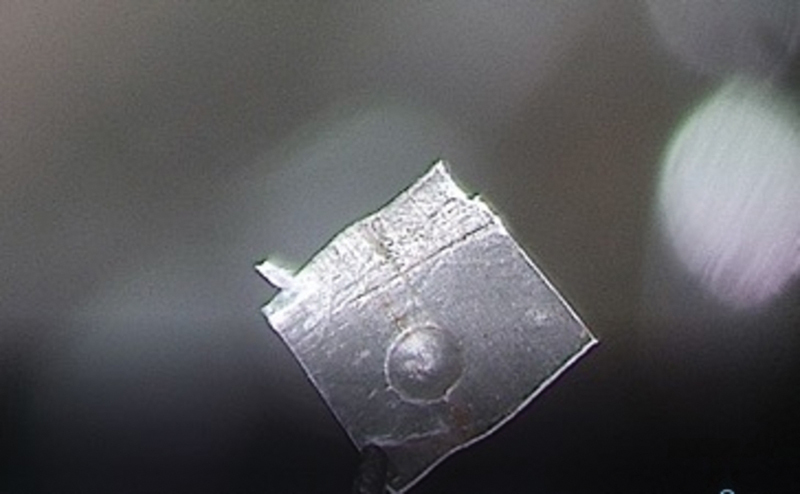
Prepared vein graft.
Fig. 2.

Fat graft placed anterosuperiorly around the piston.
The patients were followed-up for a period of 1 year with a minimum follow-up period of 3 months. A postoperative audiogram was performed at the end of 3 months postsurgery, and the short-term hearing outcomes from both groups were compared. Pure-tone audiometry was performed with an AD629 audiometer (Interacoustics, Middelfart, Denmark) and DECOS (Noordwijk, Netherlands) version 2.5.2. Both air conduction and bone conduction (BC) thresholds were measured at the following frequencies: 125, 250, 500, 1,000, 2,000, 4,000, and 8,000 Hz. In our study, ABG closures at 500, 1,000, 2,000, and 4,000 Hz were considered to calculate the mean ABG closure achieved postoperatively in accordance with the AAO-HNS guidelines from 1995. The measurement of the difference between the pre- and poststapedotomy high-frequency sensorineural hearing levels was calculated by the average BC at 3 frequencies: 1,000, 2,000, and 4,000 Hz. According to the AAO- HNS guidelines, a postoperative ABG closure < 10 dB is considered statistically significant. The difference between the pre- and postoperative average high-frequency BC was calculated to assess the incidence of SNHL following surgery. The changes in the average postoperative BC from preoperative values were stratified into 3 groups: first, those that showed > 10dB improvement in the BC thresholds; second, those that showed < 10dB improvement in the BC thresholds; and, finally, those that had a deterioration in BC, indicating postoperative worsening of SNHL.
The results of continuous measurements were presented as mean ± standard deviation (SD), and the results of categorical measurements were presented as numbers (%). The pre- and postoperative means and SDs of hearing loss in dB in each group were analyzed by the paired t -test, and the difference in the hearing outcomes achieved between both groups (intergroup) were assessed by the Pearson chi-squared test. All statistical analyses were performed at 5% level of significance and a p- value < 0.05 was considered significant.
Results
The mean age of the study population was 40.53 ± 10.860 years old. Amongst these, 47.1% ( n = 33) were males and 52.9% ( n = 37) were females. A total of 90% ( n = 63) of the patients had bilateral otosclerosis at the time of diagnosis, while only 10% ( n = 7) had unilateral disease.
Group 1 (vein graft) had 35 patients with an average preoperative PTA ranging from 30 to 101.25 dB, and the mean preoperative average PTA obtained was 60.64 ± 14.87 dB. In this group, the postoperative hearing ranged from 12.5 to 65 dB, and the mean postoperative PTA was 28.99 ± 8.94 dB. The difference between the PTAs was 31.59 ± 12.74 dB, which indicates improvement in hearing thresholds postoperatively. In the same group, the mean preoperative ABG was 30.54 ± 10.96 dB and the mean postoperative ABG was 7.44 ± 8.42 dB. This difference of 23.10 ± 8.76 dB in the paired t -test was found to be statistically significant, with p < 0.000. All patients in the study population had an improvement in AC thresholds at all frequencies, that is, at 500, 1,000, 2,000, and 4,000 Hz, and 80% ( n = 28) of these patients achieved an ABG closure < 10 dB postoperatively, which is considered highly significant according to the AAO-HNS guidelines, and 20% ( n = 7) achieved a closure between 10 and 20 dB. Comparing the BC thresholds, 43% ( n = 15) of the patients showed significant improvement in BC thresholds (> 10 dB), and 43% ( n = 15) showed improvement in postoperative BC average to within 10dB. However, 14% ( n = 5) of the patients showed a worsening of the BC threshold. The mean preoperative BC average was 28.46 ± 9.26 dB, and the mean postoperative BC average was 22.12 ± 9.89 dB. This difference of 6.34 ± 8.08 dB between the pre- and postoperative BC averages was found to be statistically significant in the paired t -test.
Group 2 (fat graft) had 35 patients with an average preoperative PTA ranging from 31.2 to 81.25 dB, with a mean of 62.03 ± 11.64 dB. The minimum and maximum average postoperative PTAs were 18.75 and 65 dB, respectively, with a mean PTA average of 32.45 ± 9.14 dB. The mean difference between the pre- and postoperative PTAs was 29.58 ± 11.73 dB, which indicates improvement in hearing thresholds postoperatively. In this group, 34 patients showed improvement in the PTA at all frequencies, that is, at 500, 1,000, 2,000, and 4,000 Hz, and the remaining 1 patient had mild (1.25 dB) worsening of PTA. These patients had a mean preoperative ABG of 33.00 ± 8.01 dB, and the mean postoperative ABG was 7.2857 ± 4.56 dB. The mean difference between the pre- and the postoperative ABG was 25.71 ± 1.37 dB, which was statistically significant in the paired t -test. Out of the 35 patients in the study population, 30 (86%) had an ABG closure to within 10dB, which is highly significant according to the AAO-HNS guidelines. The remaining 5 (14%) patients had an ABG closure between 11 and 20dB. Regarding BC, the mean preoperative BC average was 26.83 ± 9.07 dB and the mean postoperative BC average was 21.95 ± 8.24dB. The mean difference between the pre- and postoperative BC averages was of 4.88 ± 10 dB, which was found to be statistically significant in the paired t -test. A total of 31% ( n = 11) of the patients showed an improvement >10 dB in the BC threshold values, which is a significant improvement, and 52% ( n = 18) showed an improvement in the BC threshold values to within 10 dB. The remaining 17% ( n = 6) showed a worsening of the BC average.
Amongst the study population, in group 1 (vein graft), 100% ( n = 35) had an improvement in the postoperative PTA; in group 2 (fat graft), 97.1% ( n = 34) had an improvement in the postoperative PTA. This difference was analyzed by the Pearson chi-squared test and was found to be statistically insignificant ( Table 1 ). In group 1, 80% ( n = 28) of the patients had an ABG closure < 10 dB; in group 2, 85.7% ( n = 30) had an ABG closure < 10 dB. This difference between the two groups was analyzed by the Pearson chi-squared test and was found to be statistically insignificant ( Table 2 ) ( Fig. 3 ). Fifteen patients (42.9%) in group 1 and 11 (31.4%) in group 2 had a significant improvement in the BC average at 1, 2, and 4 kHz, which met the AAO-HNS guidelines, while 5 patients (14.3%) in group 1 and 6 (17.1%) in group 2 had a worsening of the BC average postoperatively. This difference was analyzed by the Pearson chi-squared test and was found to be statistically insignificant ( Table 3 ) ( Fig. 4 ).
Table 1. Comparison of average postoperative pure-tone audiometry at 3 months in both groups.
| Type of graft | Total | ||||
|---|---|---|---|---|---|
| Vein | Fat | ||||
| PTA | Improved | Count | 35 | 34 | 69 |
| % within PTA | 50.7% | 49.3% | 100.0% | ||
| % within type of graft | 100.0% | 97.1% | 98.6% | ||
| Worsened | Count | 0 | 1 | 1 | |
| % within PTA | 0% | 100.0% | 100.0% | ||
| % within type of graft | 0% | 2.9% | 1.4% | ||
| Total | Count | 35 | 35 | 70 | |
| % within PTA | 50.0% | 50.0% | 100.0% | ||
| % within type of graft | 100.0% | 100.0% | 100.0% | ||
Abbreviation: PTA, pure-tone audiometry.
Pearson chi-squared test: 1.014
Degree of freedom = 1
p= 0 .314.
Table 2. Comparison of postoperative air bone gap closure achieved in both groups.
| Type of graft | Total | ||||
|---|---|---|---|---|---|
| Vein | Fat | ||||
| ABG closure |
≤ 10 dB | Count | 28 | 30 | 58 |
| % within ABG closure | 48.3% | 51.7% | 100.0% | ||
| % within type of graft | 80.0% | 85.7% | 82.9% | ||
| 11–20 dB | Count | 7 | 5 | 12 | |
| % within ABG closure | 58.3% | 41.7% | 100.0% | ||
| % within type of graft | 20.0% | 14.3% | 17.1% | ||
| Total | Count | 35 | 35 | 70 | |
| % within ABG closure | 50.0% | 50.0% | 100.0% | ||
| % within type of graft | 100.0% | 100.0% | 100.0% | ||
Abbreviation: ABG, air bone gap.
Pearson chi-squared test: 0.402
Degree of freedom =1
p = 0.526.
Fig. 3.
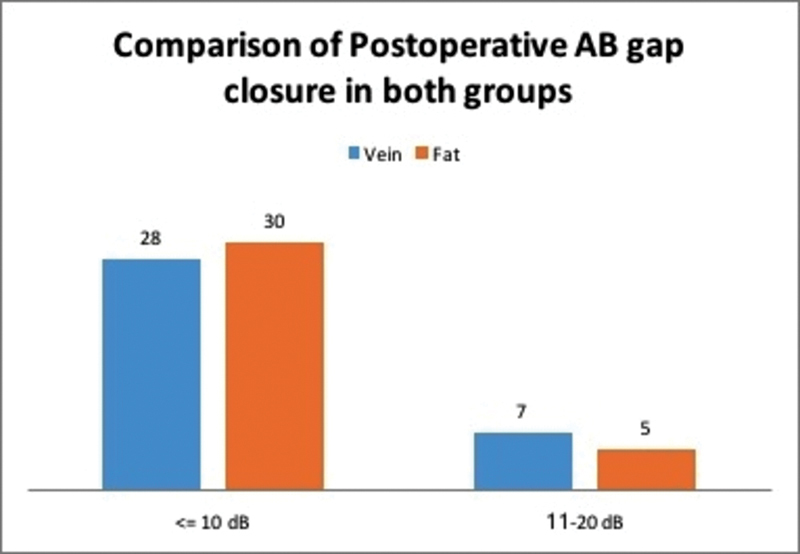
Comparison of postoperative air bone gap closure between groups 1 and 2.
Table 3. Comparison of postoperative bone conduction average in both groups.
| Type of graft | Total | ||||
|---|---|---|---|---|---|
| Vein | Fat | ||||
| Improvement of BC | > 10 dB | Count | 15 | 11 | 26 |
| % within improvement of BC | 57.7% | 42.3% | 100.0% | ||
| % within type of graft | 42.9% | 31.4% | 37.1% | ||
| < 10 dB | Count | 15 | 18 | 33 | |
| % within improvement of BC | 45.5% | 54.5% | 100.0% | ||
| % within type of graft | 42.9% | 51.4% | 47.1% | ||
| Worsened | Count | 5 | 6 | 11 | |
| % within improvement of BC | 45.5% | 54.5% | 100.0% | ||
| % within type of graft | 14.3% | 17.1% | 15.7% | ||
| Total | Count | 35 | 35 | 70 | |
| % within improvement of BC | 50.0% | 50.0% | 100.0% | ||
| % within type of graft | 100.0% | 100.0% | 100.0% | ||
Abbreviation: BC, bone conduction.
Pearson chi-squared test: 0.979
Degree of freedom = 2
p = 0.613.
Fig. 4.

Comparison of postoperative bone conduction between groups 1 and 2 .
Discussion
Surgery is the definitive treatment of choice for otosclerosis. The evolution of stapes surgery has a long history. In 1956, John Shea, in his thirties, described the stapedectomy procedure. He performed surgery in a female patient by removing the stapes and covering the oval window with subcutaneous tissue. Shea perfected stapedectomy with ossicular chain reconstruction (Teflon) and vein graft to reduce the incidence of postoperative complications and to improve hearing. 7 The procedure underwent so many modifications that eventually led to a small fenestration being created in the footplate. 7 Stapedectomy and stapedotomy represent the standard surgical procedures in otosclerosis. Stapedectomy involves either complete or partial removal of the stapes footplate followed by insertion of the prosthesis between the long process of the incus and the tissue graft over the oval window. In stapedotomy, the prosthesis is inserted through a small opening in the stapes footplate to recreate the mobile ossicular chain movement into the labyrinth. Stapedotomy provides better high-frequency hearing improvement and stable hearing when compared with stapedectomy. 8 However, both stapedectomy and stapedotomy have proven to provide long-term stability in conductive hearing improvements. Stapedotomy also has lower complication rates when compared with stapedectomy, since it involves a small fenestration technique.
Autologous tissue is routinely used to seal the fenestra around the prosthesis to improve hearing by stabilizing the prosthesis and to prevent labyrinthine fistula. 9 10 It is said that the thickness of the oval window sealing material plays an important role to prevent perilymphatic fistula formation, since some atrophic changes might occur over time. Most otologists agree that, during stapedotomy, the oval window should be sealed with grafting (sealing) material. 11 Several autologous and heterologous materials are used to seal the oval window. The different autologous materials that are routinely used are vein, fascia, perichondrium, adipose tissue (fat of the ear lobule or of the postauricular region), and blood. The heterologous materials include gelatin sponge (Gelfoam, Pfizer, New York, United States) and, more recently, esterified hyaluronic acid (Merogel, Medtronic, Minneapolis, United States).
Lopez et al. have shown that the vein graft occupies a space of 0.2 mm 2 between the edge of the stapedotomy hole and the piston and simulates the same compliance and resistance as the annular ligament of the stapes footplate, thus preventing excessive movement of the labyrinthine fluids. 12 The vein graft becomes integrated with the middle-ear mucosa and develops a rich and active blood supply, also retaining its elastic fibers. Kamal, in his study on vein graft as sealing material, has mentioned that sealing the opening of the oval window during stapes surgery is essential and helps preventing major postoperative complications, such as perilymph fistula and SNHL. 6 Hearing improvement after surgery was acceptable, and none of his patients had total hearing loss or perilymphatic fistula. Causse et al., in their several studies, have shown that vein grafting of the oval window helps to create an effective continuation of the sound conduction system, including a reduced risk of fistulas and of intracochlear damage. 13 14 15 It was also observed that the application of a vein graft in otosclerosis surgery is an ideal method to perform a stapedotomy, which leads to better postoperative hearing outcomes in terms of the postoperative ABG. 16 Bittermann et al. studied the hearing outcome of patients who underwent primary stapedotomy surgery without a vein graft ( n = 939) with that of those who underwent primary stapedotomy surgery with a vein graft ( n = 3691). 17 An analysis of variance was performed to evaluate differences in postoperative ABG and air conduction gains between surgeries with and without a vein graft, and it was found that the postoperative ABG was ≤ 10 dB in 72.1% of the patients without a vein graft and in 93.2% of the patients with a vein graft. Perkins et al. compared vein graft with blood patch in a series of laser stapedotomy surgeries, of which 86% of the patients with a vein graft closed the ABG to within 10 dB, compared with only 59% of the patients with a blood patch, and found that vein graft is superior to blood patch. 18 Similarly, Schmerber et al. did a retrospective analysis of audiometric data of 452 stapes procedures and published their experience with vein grafts and tragal perichondrium in stapedotomy. 19 They demonstrated better hearing outcomes with vein grafts, with 91% of the cases closing the ABG to within 10 dB, compared with 76% in the perichondrium group. In our study, we found excellent hearing outcomes in the subjects of group 1 (vein graft), with a mean postoperative ABG of 7.44 dB (8.42) from a mean preoperative ABG of 30.54 dB (10.96), which was statistically significant. Although vein graft has the distinct advantage of reduced risk of perilymph fistula over other sealing materials, it has also been reported to have the disadvantage of producing fibrous reactions that sometimes result in lifting of the prosthesis and reossification of the footplate below the graft. 10 Hence, thin vein grafts should be used as much as possible.
Adipose tissue, mostly harvested from the medial aspect of the earlobe, is known to be resistant to infections and to remain stable over many years. Moreover, adipose tissue conforms to the shape of the niche of the oval window. However, sometimes, a few patients were found to have postoperative vertigo due to the effect of high concentrations of local anesthetics used to harvest the adipose tissue. According to our study, in the subjects of group 2 (fat graft), there were excellent hearing outcomes, with a mean postoperative ABG of 7.28 dB (4.56) from a preoperative ABG of 33 dB (8.01), which was statistically significant. Lin et al. 9 compared 179 primary stapedotomy procedures with adipose tissue seal with 123 cases of alternative stapes surgery techniques and found excellent hearing outcomes with adipose tissue seal, with an average postoperative ABG of 7.57 dB from a preoperative average of 28.87 dB. The authors concluded that adipose tissue is an effective and cost-efficient tissue seal during stapedotomy, with excellent hearing outcomes and a low incidence of SNHL.
On comparing the mean postoperative ABG from both groups, the differences were minimal, with mean postoperative ABGs of 7.44 and 7.28 dB in the vein and fat graft groups, respectively, which was found not to be statistically significant. In group 1, 80% ( n = 28) of the patients achieved a postoperative ABG closure < 10 dB, and the remaining 20% ( n = 7) had an ABG closure between 11 and 20 dB. In group 2 ( fat graft), 85.7% ( n = 30) of the patients achieved a significant ABG closure < 10dB, and the remaining 14.3% ( n = 5) had an ABG closure between 11 and 20 dB. Similarly, Wiet et al., 11 in their study in 2012 that included 365 stapes procedures, compared 3 oval window sealing materials, namely, fat, fascia, and vein grafts. Most patients in all 3 groups had an ABG <10 dB at the long-term follow-up (fat, 79.5%; fascia, 78.8%; and vein, 75.6%), with 90.3% of all patients at < 20 dB. The authors found that there were no significant differences in hearing results among the 3 types of tissue seals of the oval window in stapes surgery both in the short-term (3 months) and in the long-term (at or > 1 year) follow-up. In contrast, Lin et al., 9 in a series of 179 patients subjected to primary stapedotomy, compared adipose tissue seal with alternative techniques (vein, fascia, or perichondrium) and found excellent hearing outcomes for adipose tissue seal, with the postoperative ABG closing to within 10 and 15 dB in 79.89% and 93.30% of cases, respectively.
Additionally, our study compared the change in bone conduction thresholds between the two groups to assess SNHL. In patients with vein graft, 42.9% ( n = 15) had an improvement > 10 dB in the BC average, and 42.9% ( n = 15) had an improvement < 10dB in the BC average, while 14.3% ( n = 5) had a worsening of SNHL by deterioration of the BC average. In patients with fat graft, 31.4% ( n = 11) had an improvement > 10 dB in the BC average, and 51.4% ( n = 18) had an improvement < 10 dB in the BC average, while 17.1% ( n = 6) had a worsening of SNHL. However, the differences between the two groups were statistically insignificant. Similarly, Wiet et al. 11 found that there was no difference in SNHL after stapedectomy between adipose, fascia, and vein seals. In contrast, Schmerber et al. 19 compared the mean preoperative and postoperative bone conduction thresholds and showed that a SNHL > 10 dB occurred in 1.4 and 4.4% of the patients in the vein and perichondrium groups, respectively, and concluded that vein graft is superior to perichondrium in their study.
A comparative analysis of the various interventions in the literature for the benefits of oval window sealing materials in stapes procedures is difficult because of the wide array of outcome measures used. The results of short-term hearing outcomes in both study groups were compared and no statistically significant differences were noted. Patients in both study groups, either with vein or fat as oval window sealing material, achieved a significant ABG closure. And the incidence of postoperative deterioration of sensorineural hearing level was very minimal and insignificant in both groups. None of the patients in either group had total SNHL postoperatively. None of the patients in the study population suffered from perilymph fistula, which is a common complication of stapes surgery, either with Gelfoam graft or without any oval window sealing material. And none of the patients in either group had postoperative complication of granuloma formation, as found by earlier studies on fat graft. Both groups had a stable and significant short-term hearing improvement. However, long-term follow-up of patients is required to know the stability of the hearing outcomes in the long run. Although vein grafts and adipose tissue may be comparable regarding hearing outcomes, the procedure of harvesting fat graft is much simpler than that of harvesting vein graft.
Conclusion
Both vein graft and adipose tissue had a comparable effect on hearing outcomes when used as sealing materials in stapedotomy. None of the patients in the study population had neither perilymph fistula nor total SNHL. However, long-term follow-up is required for a period of at least 1 year to assess the stability of long-term hearing outcomes following stapedotomy.
Conflict of Interests The authors have no conflict of interests to declare.
Ethical Approval
All procedures involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its amendments or comparable ethical standards. Ethical clearance was obtained from the institute ethics committee (EC/NEW/INST/2017/1262). Informed consent was obtained from all individual participants in the study
References
- 1.Ealy M, Smith R JH. Otosclerosis. Adv Otorhinolaryngol. 2011;70:122–129. doi: 10.1159/000322488. [DOI] [PubMed] [Google Scholar]
- 2.Ealy M, Smith R JH.The genetics of otosclerosis Hear Res 2010266(1-2):70–74. [DOI] [PubMed] [Google Scholar]
- 3.Schuknecht H F, Barber W. Histologic variants in otosclerosis. Laryngoscope. 1985;95(11):1307–1317. doi: 10.1288/00005537-198511000-00003. [DOI] [PubMed] [Google Scholar]
- 4.Schuknecht H F, Kirchner J C. Cochlear otosclerosis: fact or fantasy. Laryngoscope. 1974;84(05):766–782. doi: 10.1288/00005537-197405000-00008. [DOI] [PubMed] [Google Scholar]
- 5.Shambaugh G E. Philadelphia, PA: Saunders & Co; 1959. Surgery of the Ear; pp. 529–543. [Google Scholar]
- 6.Kamal S A. Vein graft in stapes surgery. Am J Otol. 1996;17(02):230–235. [PubMed] [Google Scholar]
- 7.Shea J J., Jr Fenestration of the oval window. Ann Otol Rhinol Laryngol. 1958;67(04):932–951. doi: 10.1177/000348945806700403. [DOI] [PubMed] [Google Scholar]
- 8.Fisch U. Stapedotomy versus stapedectomy. Am J Otol. 1982;4(02):112–117. [PubMed] [Google Scholar]
- 9.Lin K F, Selesnick S. Stapedotomy With Adipose Tissue Seal: Hearing Outcomes, Incidence of Sensorineural Hearing Loss, and Comparison to Alternative Techniques. Otol Neurotol. 2016;37(07):851–858. doi: 10.1097/MAO.0000000000001117. [DOI] [PubMed] [Google Scholar]
- 10.Incesulu A, Häusler R. Advantages and risks of various sealing procedures of the oval window: vein graft, adipose tissue, gelfoam, merogel. Adv Otorhinolaryngol. 2007;65:206–209. doi: 10.1159/000098809. [DOI] [PubMed] [Google Scholar]
- 11.Wiet R J, Battista R A, Wiet R M, Sabin A T. Hearing outcomes in stapes surgery: a comparison of fat, fascia, and vein tissue seals. Otolaryngol Head Neck Surg. 2013;148(01):115–120. doi: 10.1177/0194599812463184. [DOI] [PubMed] [Google Scholar]
- 12.Lopez A, Juberthie L, Olivier J C, Causse J B, Robinson J. Survival and evolution of vein grafts in otosclerosis surgery: structural and ultrastructural evidence. Am J Otol. 1992;13(02):173–184. [PubMed] [Google Scholar]
- 13.Causse J B, Causse J R. Technique for otosclerosis. Am J Otol. 1984;5(05):392–396. [PubMed] [Google Scholar]
- 14.Causse J B, Causse J R, Parahy C. Stapedotomy technique and results. Am J Otol. 1985;6(01):68–71. [PubMed] [Google Scholar]
- 15.Causse J B. The twenty fine points of otosclerosis surgery. Am J Otol. 1989;10(01):75–77. [PubMed] [Google Scholar]
- 16.Vincent R, Sperling N M, Oates J, Jindal M.Surgical findings and long-term hearing results in 3,050 stapedotomies for primary otosclerosis: a prospective study with the otology-neurotology database Otol Neurotol 200627(8, Suppl 2)S25–S47. [DOI] [PubMed] [Google Scholar]
- 17.Bittermann A JN, Vincent R, Rovers M M. A nonrandomized comparison of stapes surgery with and without a vein graft in patients with otosclerosis. Otol Neurotol. 2013;34(05):827–831. doi: 10.1097/MAO.0b013e31828bb523. [DOI] [PubMed] [Google Scholar]
- 18.Perkins R, Curto F S., JrLaser stapedotomy: a comparative study of prostheses and seals Laryngoscope 1992102(12 Pt 1):1321–1327. [DOI] [PubMed] [Google Scholar]
- 19.Schmerber S, Cuisnier O, Charachon R, Lavieille J P. Vein versus tragal perichondrium in stapedotomy. Otol Neurotol. 2004;25(05):694–698. doi: 10.1097/00129492-200409000-00008. [DOI] [PubMed] [Google Scholar]