

Abstract
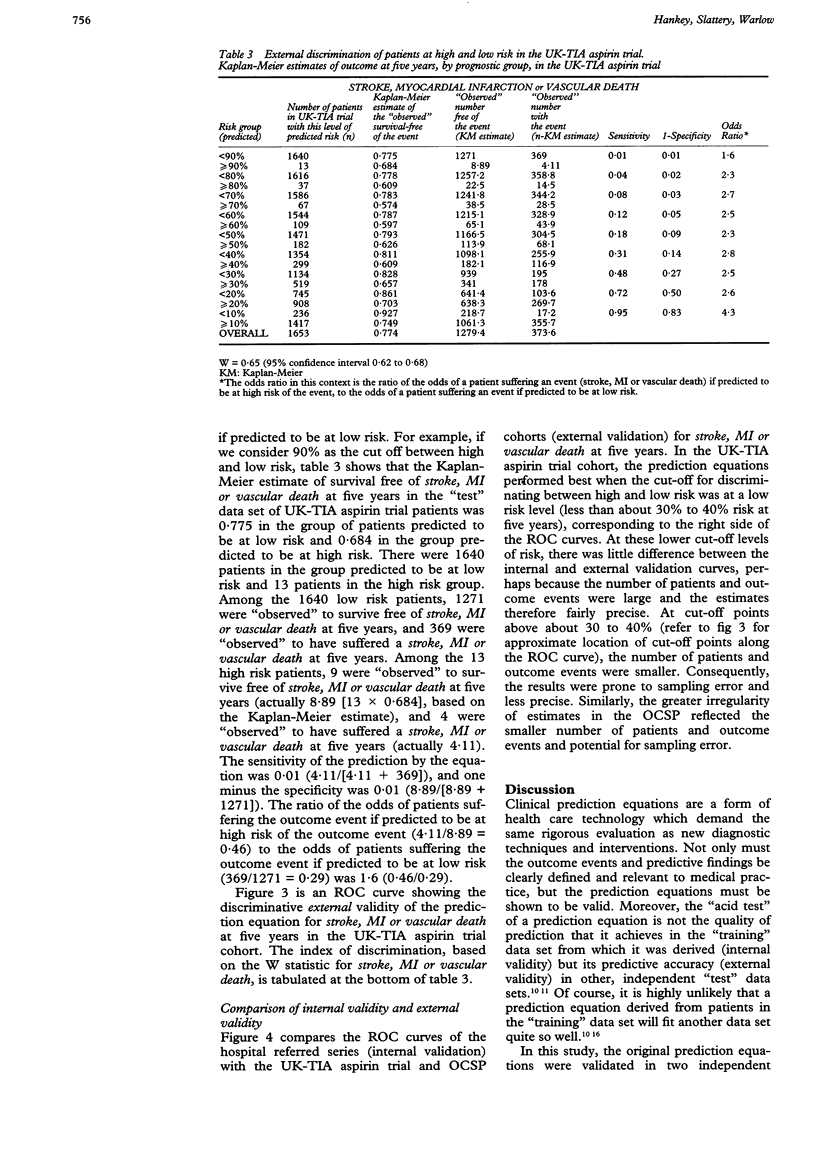
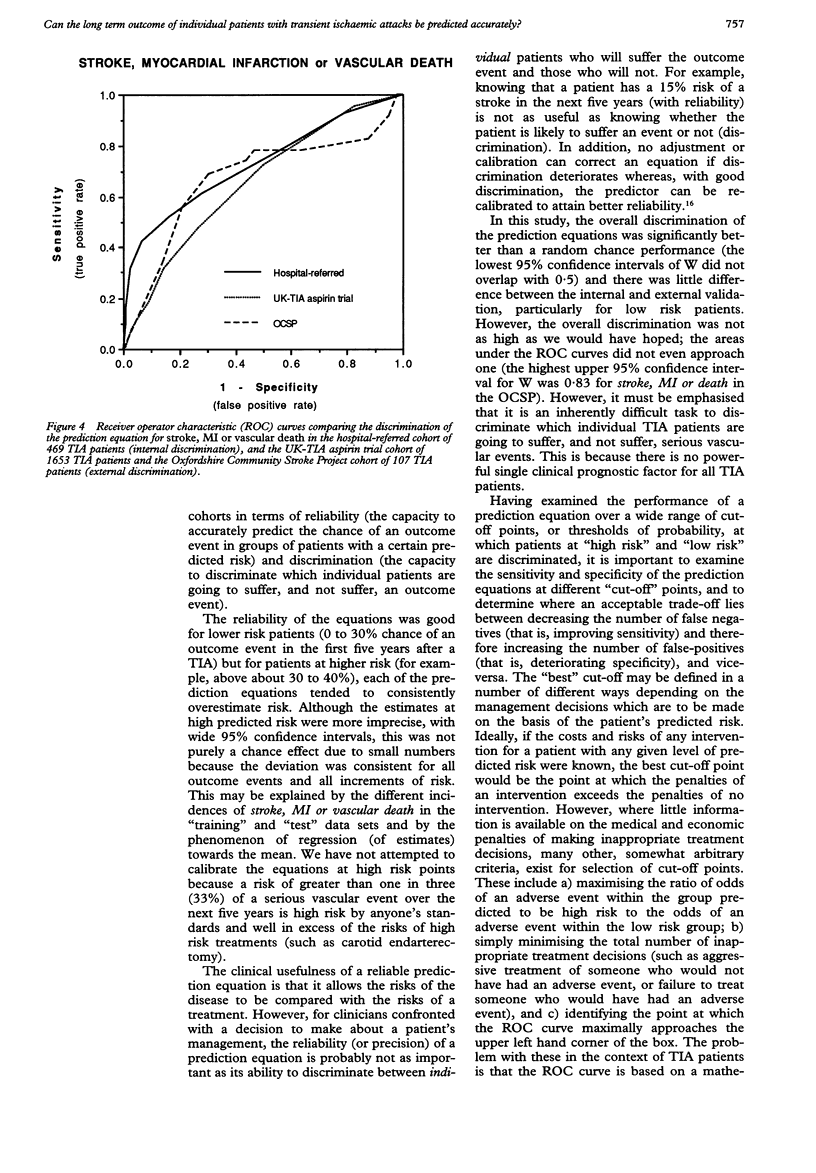
The prognosis of individual patients with transient ischaemic attacks (TIAs) is extremely variable; some patients are at high risk and others at low risk of a serious vascular event. Prediction equations of outcome were developed, based on eight clinical prognostic factors, from a cohort of 469 hospital-referred TIA patients ("training" data set), that enable high (and low) risk patients to be identified and for whom costly and risky treatments may (or may not) be targeted. The study aimed to determine whether these equations are externally valid and can predict outcome, with reliability and discrimination, in two independent cohorts of TIA patients ("test" data sets): 1653 TIA patients in the UK-TIA aspirin trial and 107 TIA patients in the Oxfordshire Community Stroke Project. Predicted outcomes agreed closely with the observed outcomes in the "test" data sets (reliability) for all outcome events at low five year risk (< 30%) but the estimates of risk were less precise in groups predicted to have a high five year risk (> 40%). The prediction equations were fairly accurate in discriminating between patients who subsequently suffered the outcome event of interest and those who survived free of the event at five years after the TIA, particularly at lower cut-off levels distinguishing high and low risk (for example, < 30% vs > 30% at five years). It is very difficult to achieve perfect discrimination because there is no single important prognostic factor for TIA patients that indicates whether a patient is going to suffer an event or not. These equations can be used to provide a reliable estimate of the absolute five year risk of a serious vascular event in hospital-referred TIA patients but they cannot, as yet, be used with confidence to distinguish patients at high risk from patients at low risk.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Collins R., Peto R., MacMahon S., Hebert P., Fiebach N. H., Eberlein K. A., Godwin J., Qizilbash N., Taylor J. O., Hennekens C. H. Blood pressure, stroke, and coronary heart disease. Part 2, Short-term reductions in blood pressure: overview of randomised drug trials in their epidemiological context. Lancet. 1990 Apr 7;335(8693):827–838. doi: 10.1016/0140-6736(90)90944-z. [DOI] [PubMed] [Google Scholar]
- Dennis M. S., Bamford J. M., Sandercock P. A., Warlow C. P. A comparison of risk factors and prognosis for transient ischemic attacks and minor ischemic strokes. The Oxfordshire Community Stroke Project. Stroke. 1989 Nov;20(11):1494–1499. doi: 10.1161/01.str.20.11.1494. [DOI] [PubMed] [Google Scholar]
- Dennis M. S., Bamford J. M., Sandercock P. A., Warlow C. P. Incidence of transient ischemic attacks in Oxfordshire, England. Stroke. 1989 Mar;20(3):333–339. doi: 10.1161/01.str.20.3.333. [DOI] [PubMed] [Google Scholar]
- Dennis M., Bamford J., Sandercock P., Warlow C. Prognosis of transient ischemic attacks in the Oxfordshire Community Stroke Project. Stroke. 1990 Jun;21(6):848–853. doi: 10.1161/01.str.21.6.848. [DOI] [PubMed] [Google Scholar]
- Hankey G. J., Slattery J. M., Warlow C. P. The prognosis of hospital-referred transient ischaemic attacks. J Neurol Neurosurg Psychiatry. 1991 Sep;54(9):793–802. doi: 10.1136/jnnp.54.9.793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hankey G. J., Slattery J. M., Warlow C. P. Transient ischaemic attacks: which patients are at high (and low) risk of serious vascular events? J Neurol Neurosurg Psychiatry. 1992 Aug;55(8):640–652. doi: 10.1136/jnnp.55.8.640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hanley J. A., McNeil B. J. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982 Apr;143(1):29–36. doi: 10.1148/radiology.143.1.7063747. [DOI] [PubMed] [Google Scholar]
- Harrell F. E., Jr, Califf R. M., Pryor D. B., Lee K. L., Rosati R. A. Evaluating the yield of medical tests. JAMA. 1982 May 14;247(18):2543–2546. [PubMed] [Google Scholar]
- Harrell F. E., Jr, Lee K. L., Califf R. M., Pryor D. B., Rosati R. A. Regression modelling strategies for improved prognostic prediction. Stat Med. 1984 Apr-Jun;3(2):143–152. doi: 10.1002/sim.4780030207. [DOI] [PubMed] [Google Scholar]
- Kernan W. N., Horwitz R. I., Brass L. M., Viscoli C. M., Taylor K. J. A prognostic system for transient ischemia or minor stroke. Ann Intern Med. 1991 Apr 1;114(7):552–557. doi: 10.7326/0003-4819-114-7-552. [DOI] [PubMed] [Google Scholar]
- Rose G., Day S. The population mean predicts the number of deviant individuals. BMJ. 1990 Nov 3;301(6759):1031–1034. doi: 10.1136/bmj.301.6759.1031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rose G. Strategy of prevention: lessons from cardiovascular disease. Br Med J (Clin Res Ed) 1981 Jun 6;282(6279):1847–1851. doi: 10.1136/bmj.282.6279.1847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Warlow C. Ticlopidine, a new antithrombotic drug: but is it better than aspirin for longterm use? J Neurol Neurosurg Psychiatry. 1990 Mar;53(3):185–187. doi: 10.1136/jnnp.53.3.185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wasson J. H., Sox H. C., Neff R. K., Goldman L. Clinical prediction rules. Applications and methodological standards. N Engl J Med. 1985 Sep 26;313(13):793–799. doi: 10.1056/NEJM198509263131306. [DOI] [PubMed] [Google Scholar]
- de Dombal F. T. Analysis of symptoms in the acute abdomen. Clin Gastroenterol. 1985 Jul;14(3):531–543. [PubMed] [Google Scholar]