

Abstract
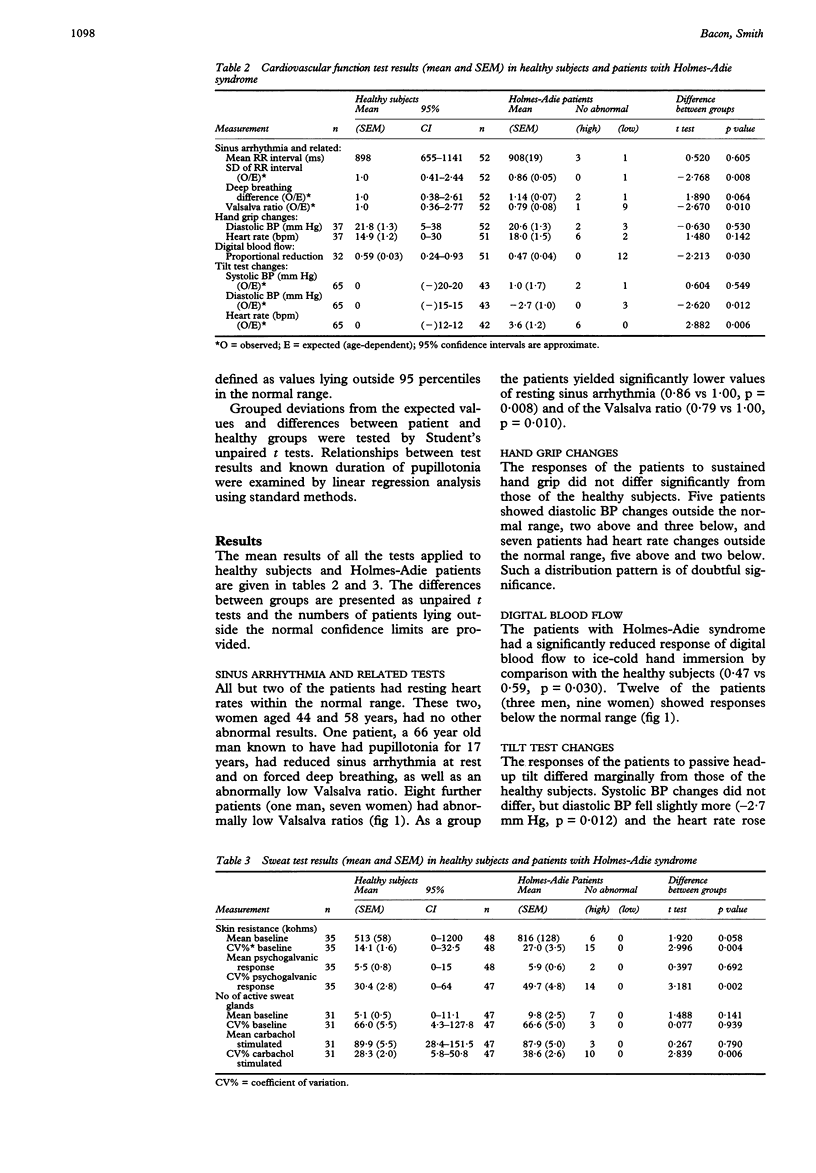
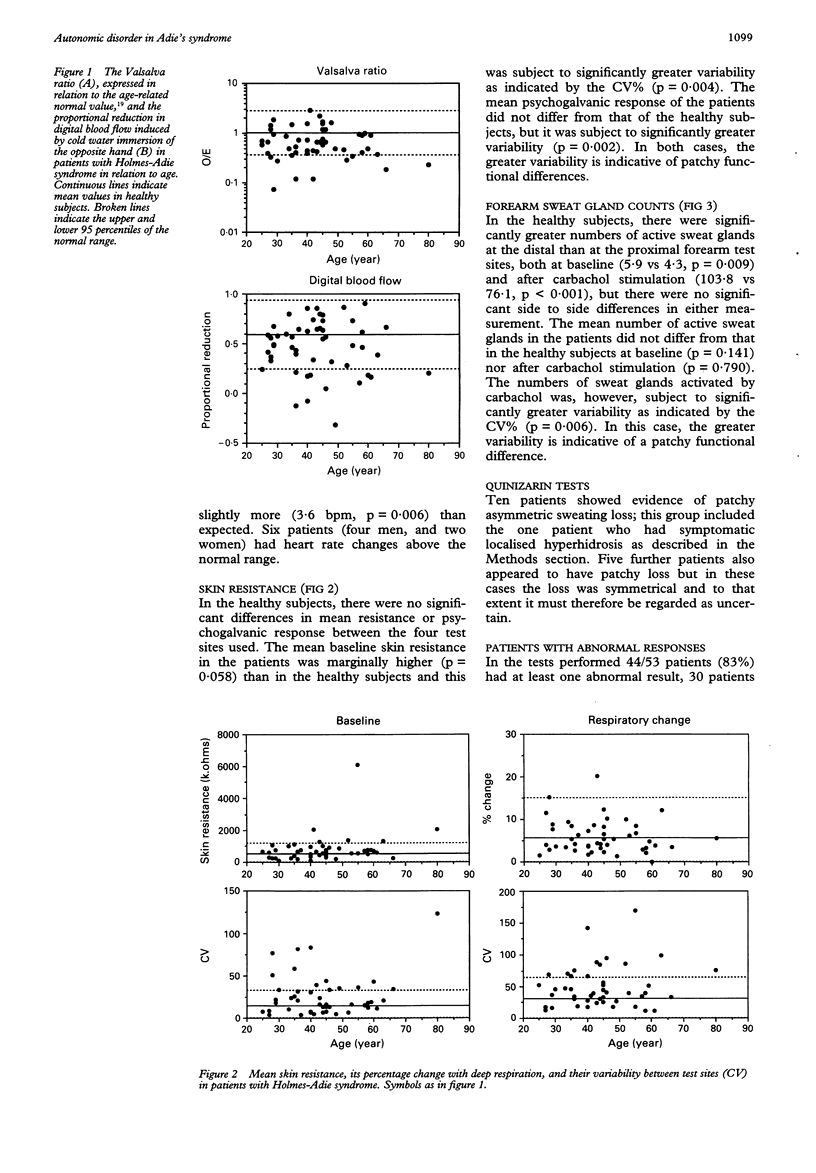
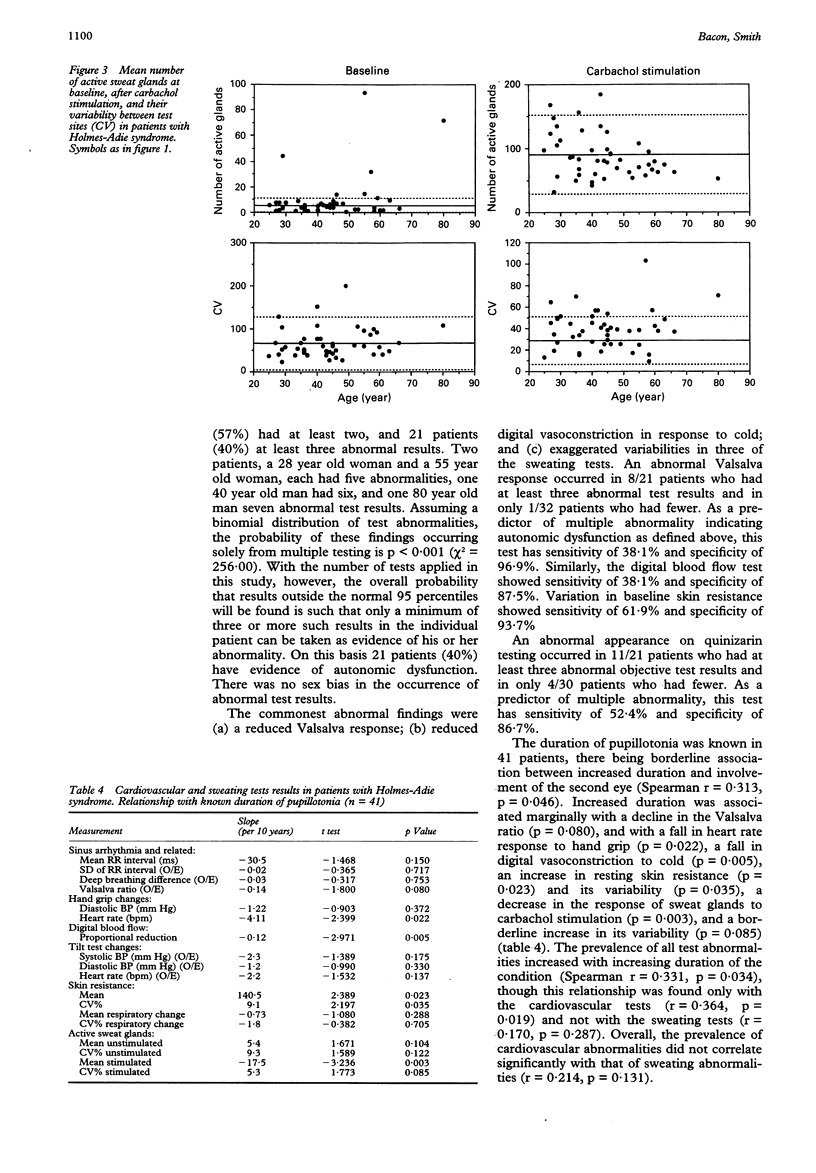
A cross-sectional study is reported in which 53 patients with Holmes-Adie syndrome have been subjected to a battery of tests of autonomic nervous function referable to the cardiovascular system, to two objective tests of sweating function, and to subjective assessment of sweating by application of quinizarin powder followed by body heating. The majority of patients were consecutive referrals; none was selected because of clinical indications of autonomic dysfunction. Eighty three per cent of these patients had at least one, 57% at least two, and 40% at least three objective test abnormalities, as defined by values lying outside 95 percentiles of healthy subjects who were matched for age and subjected to the same tests. In the context of multiple testing, the probability of finding outside values was such that a minimum of 3 was required to define abnormality. On this basis 40% of patients were found to have significant evidence of autonomic dysfunction. The most frequent abnormalities were impaired digital vasoconstriction to cold (23%), a reduced heart rate response to the Valsalva manoeuvre (17%), and excessive variability in sweating between test sites (in one of the tests, 43%) which is consistent with patchy loss. Abnormal quinizarin test appearances were seen in 10 patients and in a further five patients the appearances were thought to be suggestive of abnormality. Though assessment of the results of this test are subjective, the observations are consistent with the findings obtained from the objective tests which were applied. Cardiovascular and sweating abnormality did not concur significantly and only the former was found to increase progressively with known duration of the pupillotonia. It is concluded that Holmes-Adie syndrome is commonly accompanied by progressive mild but widespread autonomic involvement but rarely is this symptomatic. If symptoms suggestive of autonomic neuropathy are found in a patient with tonic pupils, a careful search for some other generalised disorder is recommended.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BONNIN M., SKINNER S. L., WHELAN R. F. Holmes-Adie syndrome with progressive autonomic degeneration. Australas Ann Med. 1961 Nov;10:304–307. doi: 10.1111/imj.1961.10.4.304. [DOI] [PubMed] [Google Scholar]
- Clubley M., Bye C. E., Henson T., Peck A. W., Riddington C. A technique for studying the effects of drugs on human sweat gland activity. Eur J Clin Pharmacol. 1978 Nov 27;14(3):221–226. doi: 10.1007/BF02089963. [DOI] [PubMed] [Google Scholar]
- Esterly N. B., Cantolino S. J., Alte B. P., Brusilow S. W. Pupillotonia, hyporeflexia, and segmental hypohidrosis: autonomic dysfunction in a child. J Pediatr. 1968 Dec;73(6):852–859. doi: 10.1016/s0022-3476(68)80238-0. [DOI] [PubMed] [Google Scholar]
- Ewing D. J., Irving J. B., Kerr F., Wildsmith J. A., Clarke B. F. Cardiovascular responses to sustained handgrip in normal subjects and in patients with diabetes mellitus: a test of autonomic function. Clin Sci Mol Med. 1974 Mar;46(3):295–306. doi: 10.1042/cs0460295. [DOI] [PubMed] [Google Scholar]
- HARDIN W. B., Jr, GAY A. J. THE PHENOMENON OF BENIGN AREFLEXIA. REVIEW OF THE HOLMES-ADIE SYNDROME WITH CASE REPORTS AND A STUDY OF THE ACHILLES REFLEX. Neurology. 1965 Jul;15:613–621. doi: 10.1212/wnl.15.7.613. [DOI] [PubMed] [Google Scholar]
- Hart G., Oldershaw P. J., Cull R. E., Humphrey P., Ward D. Syncope caused by cough-induced complete atrioventricular block. Pacing Clin Electrophysiol. 1982 Jul;5(4):564–566. doi: 10.1111/j.1540-8159.1982.tb02279.x. [DOI] [PubMed] [Google Scholar]
- Heath P. D., Moss C., Cartlidge N. E. Ross syndrome and skin changes. Neurology. 1982 Sep;32(9):1041–1042. doi: 10.1212/wnl.32.9.1041. [DOI] [PubMed] [Google Scholar]
- Hedges T. R., Gerner E. W. Ross' syndrome (tonic pupil plus). Br J Ophthalmol. 1975 Jul;59(7):387–391. doi: 10.1136/bjo.59.7.387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hope-Ross M., Buchanan T. A., Archer D. B., Allen J. A. Autonomic function in Holmes Adie syndrome. Eye (Lond) 1990;4(Pt 4):607–612. doi: 10.1038/eye.1990.85. [DOI] [PubMed] [Google Scholar]
- Lucy D. D., Jr, Van Allen M. W., Thompson H. S. Holmes-Adie syndrome with segmental hypohidrosis. Neurology. 1967 Aug;17(8 Pt 1):763-9, 778. doi: 10.1212/wnl.17.8.763. [DOI] [PubMed] [Google Scholar]
- PETAJAN J. H., DANFORTH R. C., D ALLESIO D., LUCAS G. J. PROGRESSIVE SUDOMOTOR DENERVATION AND ADIE'S SYNDROME. Neurology. 1965 Feb;15:172–176. doi: 10.1212/wnl.15.2.172. [DOI] [PubMed] [Google Scholar]
- ROSS A. T. Progressive selective sudomotor denervation; a case with coexisting Adie's syndrome. Neurology. 1958 Nov;8(11):809–817. doi: 10.1212/wnl.8.11.809. [DOI] [PubMed] [Google Scholar]
- Rubenstein A. E., Yahr M. D., Mytilineou C., Sivak M., Mindel J., Frontera A. T. Orthostatic hypotension in the Holmes-Adie syndrome. Mt Sinai J Med. 1980 Jan-Feb;47(1):57–61. [PubMed] [Google Scholar]
- Smith S. E., Smith S. A. Heart rate variability in healthy subjects measured with a bedside computer-based technique. Clin Sci (Lond) 1981 Oct;61(4):379–383. doi: 10.1042/cs0610379. [DOI] [PubMed] [Google Scholar]
- Spector R. H., Bachman D. L. Bilateral Adie's tonic pupil with anhidrosis and hyperthermia. Arch Neurol. 1984 Mar;41(3):342–343. doi: 10.1001/archneur.1984.04050150124034. [DOI] [PubMed] [Google Scholar]
- Vanasse M., Molina-Negro P., Saint-Hilaire J. M. Syndrome d'Adie associé à une hypophidrose segmentaire. Etude clinique et neurophysiologique. Rev Neurol (Paris) 1974 May-Jun;130(5-6):237–244. [PubMed] [Google Scholar]