

Abstract
Introduction and importance
The common mesentery is an abnormal rotation of the primitive intestinal loop or omphalomesenteric loop. It is not necessarily symptomatic, but a clinical presentation of acute bowel obstruction on the band or volvulus can reveal it. We report a case of small bowel obstruction due to Ladd's band and Meckel's diverticulum on the incomplete common mesentery.
Presentation of case
We report a case of a 54-year-old man with no previous abdominal surgery who experienced periumbilical abdominal pain and vomiting. Physical examination revealed a diffusely tender and distended abdomen. Laboratory data showed a biological inflammatory syndrome. An abdominal CT scan revealed a small bowel mechanical obstruction with a double transitional level under the umbilical without a loop enhancement. An emergent laparotomy was performed. We found an incomplete common mesentery. The small bowel obstruction was due to a Ladd's band attrapping the Meckel's diverticulum. This association was responsible for dilating ileal loops at the superior part of the mechanical obstruction with necrosis of 30 cm of the small bowel. We have sectioned the congenital band and resected the necrotic segment, followed by an intestinal anastomosis. The postoperative follow-up was uneventful.
Clinical discussion
Incomplete common mesentery with Ladd's band and Meckel's diverticulum is an extremely rare association. Causing a small bowel obstruction remains an uncommon complication and circumstance of discovery. This complication presents a life-threatening condition. An abdominal CT scan could help for the diagnosis in some cases. Surgery is the standard treatment in most cases.
Conclusion
The association of incomplete common mesentery with Ladd's band and Meckel's diverticulum is uncommon and should be known to avoid intraoperative misdiagnose.
Keywords: Ladd's band, Meckel's diverticulum, Obstruction, Case report
Highlights
-
•
The common mesentery is not necessarily symptomatic, but a clinical presentation of acute bowel obstruction on the band or volvulus can reveal it.
-
•
The association with a complicated Meckel’s diverticulum is uncommon.
-
•
Small bowel obstruction due to Ladd's band and Meckel's diverticulum on the incomplete common mesentery is an extremely rare association and clinical presentation.
1. Introduction
The common mesentery is an abnormal rotation of the primitive intestinal loop or omphalomesenteric loop during embryonic development, occurring very rarely in adults [1]. This defect is always congenital [2]. It is not necessarily symptomatic, but a clinical presentation of acute bowel obstruction on the band or volvulus can reveal it. We report a case, using SCARE guideline [3], of small bowel obstruction due to Ladd's band and Meckel's diverticulum on the incomplete common mesentery.
2. Presentation of case
We report a case of a 54-year-old man with no previous abdominal surgery who experienced periumbilical abdominal pain and vomiting and had not passed flatus or faeces one day earlier. Physical examination revealed a diffusely tender and distended abdomen without peritoneal signs. Laboratory data showed a biological inflammatory syndrome. An abdominal CT scan revealed a small bowel mechanical obstruction with a double transitional level under the umbilical without a loop enhancement (Fig. 1). An emergent laparotomy was performed under general anaesthesia. We found an incomplete common mesentery. The small bowel obstruction was due to a Ladd's band attrapping the Meckel's diverticulum (Fig. 2, Fig. 3). This association was responsible for dilating ileal loops at the superior part of the mechanical obstruction with necrosis of 30 cm of the small bowel (Fig. 3). We have sectioned the congenital band and resected the necrotic segment, followed by an intestinal anastomosis. We have not performed the appendectomy. The postoperative follow-up was uneventful. The patient recovered without complications and was discharged after seven days of hospitalization. He was examined after two weeks in the outpoint clinic.
Fig. 1.
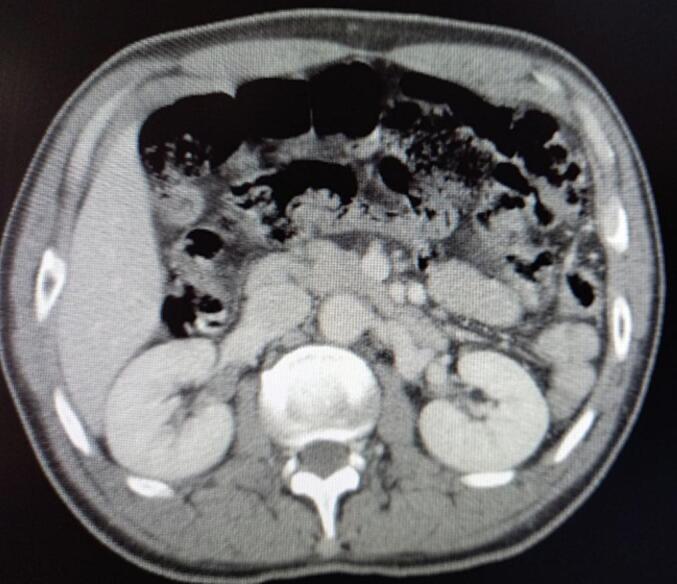
Abdominal CT scan shows dilated loops of the small bowel, indicating small bowel obstruction. The dilated loops of the small bowel are located on the right side of the abdomen, while the collapsed large bowel is on the left side.
Fig. 2.

Intraoperative views showing the incomplete common mesentery with Ladd's band.
Fig. 3.
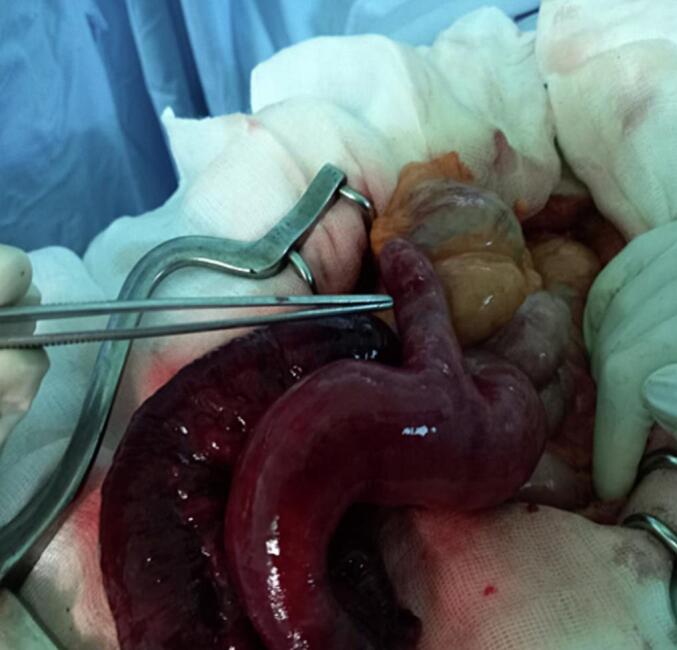
Intraoperative view showing the Meckel's diverticulum responsible for the small bowel's volvulus through the Ladd's band.
3. Discussion
Intestinal malrotation or incomplete common mesentery is caused by the partial or complete failure of 270 degrees' counterclockwise rotation of the midgut around superior mesenteric vessels in fetal life [4]. Embryologically, it is malrotation and joining of the primitive intestine that is causing the incomplete common mesentery [1], so the root of the mesentery is very short, and the whole small intestine is located on the superior mesenteric artery axis [2], the peritoneal fibrous band – also known as Ladd's band –can compress duodenum causing a duodenal obstruction [4]. Intestinal malrotation is a disease of the newborn as it frequently manifests in the first month of life; adult manifestation is very rare [4]. Acute intestinal obstruction and enteromesenteric infarction are the main life-threatening complications of incomplete common mesentery [5], [6]. Small bowel obstruction is frequently secondary to Ladd bands or volvulus [7]. In this report, we had these two mechanisms. Clinical presentation in adults is more variable and non-specific and can be asymptomatic. Bilious vomiting, bowel obstruction, and abdominal pain are classified as presenting complaints of intestinal malrotation [4]. Adult patients rarely present with acute midgut volvulus or internal hernias caused by Ladd's bands. Often a diagnosis of intestinal malrotation is made incidentally on routine imaging [4], hence the importance of knowing the radiological features, particularly scenographic features of this rare entity, thus enabling early therapeutic management [5]. On cross-sectional imaging, one should see the affected segment of the bowel twisted about the mesentery. This imaging feature is known as the whirlpool sign. In our case, the patient had a Meckel diverticulum, which was incarcerated with the bowel loop into the band, causing the volvulus. Meckel's diverticulum originates from the failure of the vitelline duct to obliterate, which is usually located on the antimesenteric border of the ileum [8]. It is the most common congenital variation of the small intestine, with a prevalence of approximately 1–3 %. Most cases with Meckel's diverticulum are asymptomatic, and the diagnosis is difficult to confirm preoperatively. Intestinal obstruction is Meckel's diverticulum's second most common complication after haemorrhage [9]. There are many mechanisms for bowel obstruction arising from a Meckel's diverticulum; in our case, obstruction was caused by the Ladd band's trapping of a bowel loop [7]. Ladd first described the Ladd procedure in 1932 to treat malrotation and volvulus, and since then, it has been the definitive treatment for intestinal malrotation. Ladd's procedure consists of the initial untwisting of the volvulus. Secondly, Ladd's thick peritoneal bands are divided from the caecum to the right upper quadrant and the duodenum. The ligament of Treitz is taken down, and the duodenum is mobilized to the right and straightened. The entire bowel is returned to the abdomen in a non-rotated position [3]. This procedure may performed safely, with a high degree of patient satisfaction, by a laparoscopic approach in adults [10].
4. Conclusion
Incomplete common mesentery with Ladd's band and Meckel's diverticulum causing a small bowel obstruction remains an extremely rare association. This complication presents a life-threatening condition. An abdominal CT scan help for the diagnosis in some cases. Surgery is the standard treatment in most cases. The surgery should be performed emergently to reduce the mortality and morbidity of this affection.
Patient consent
Written informed consent was obtained from the patient to publish this case report and accompanying images. On request, a copy of the written consent is available for review by the Editor-in-Chief of this journal.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Ethical approval
Ethical approval is exempt/waived at our institution.
Funding
None.
Author contribution
Ethical approval is exempt/waived at our institution.
Guarantor
Mohamed Ali Chaouch, MD
Research registration number
Not applicable.
Conflict of interest statement
None.
Acknowledgements
There were no acknowledgements to mention.
References
- 1.Ongoïba N., Ba B., Coulibaly B., Togola B., Traoré D., Siby O., et al. Common mesentery: discovered two cases of intestinal obstruction. Mali Med. 2013;28(3):49–52. [PubMed] [Google Scholar]
- 2.Oudou A.Z., Soumana I.D., Souiki T., Majdoub K., Toughrai I., Laalim S.A., et al. Total small bowel volvulus complicating common incomplete mesentery, an exceptional complication in adults: about a case. Pan Afr. Med. J. 2019;33 doi: 10.11604/pamj.2019.33.220.18159. 220-220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Agha R.A., Fowler A.J., Saeta A., Barai I., Rajmohan S., Orgill D.P., et al. The SCARE statement: consensus-based surgical case report guidelines. Int. J. Surg. 2016;34:180–186. doi: 10.1016/j.ijsu.2016.08.014. [DOI] [PubMed] [Google Scholar]
- 4.Grassi C., Conti L., Palmieri G., Banchini F., Dacco M.D., Cattaneo G.M., et al. Ladd’s band in the adult, an unusual case of occlusion: case report and review of the literature. Int. J. Surg. Case Rep. 2020;71:45–49. doi: 10.1016/j.ijscr.2020.04.046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Alaoui A., Alami B., Lamrani Y.A., Boubou M., Maaroufi M. Small bowel volvulus complicating common incomplete mesentery in an adult: a case report. Pan Afr. Med. J. 2020;37 doi: 10.11604/pamj.2020.37.287.17538. 287-287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Toumi O., Chaouch M.A., Ghedira A., Korbi I., Nasr M., Noomene F., et al. adult’s congenital bile duct cysts les dilatations kystiques congénitales des voies biliaires diagnostiquées chez l’adulte. Tunis Med. 2017;95(06) [PubMed] [Google Scholar]
- 7.Raphaeli T., Parimi C., Mattix K., Javid P.J. Acute colonic obstruction from Ladd bands: a unique complication from intestinal malrotation. J. Pediatr. Surg. 2010;45(3):630–631. doi: 10.1016/j.jpedsurg.2009.12.026. [DOI] [PubMed] [Google Scholar]
- 8.Sumer A., Kemik O., Olmez A., Dulger A.C., Hasirci I., Iliklerden U., et al. Small bowel obstruction due to mesodiverticular band of Meckel’s diverticulum: a case report. Case Rep. Med. 2010;2010 doi: 10.1155/2010/901456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Low S.F., Ngiu C.S., Sridharan R., Lee Y.L. Midgut malrotation with congenital peritoneal band: a rare cause of small bowel obstruction in adulthood. Case Rep. 2014;2014 doi: 10.1136/bcr-2013-202690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mizuta N., Kikuchi T., Fukuda Y. Adult intestinal malrotation treated with laparoscopic Ladd procedure. Case Rep. Surg. 2022;2022 doi: 10.1155/2022/6874885. [DOI] [PMC free article] [PubMed] [Google Scholar]