

Abstract
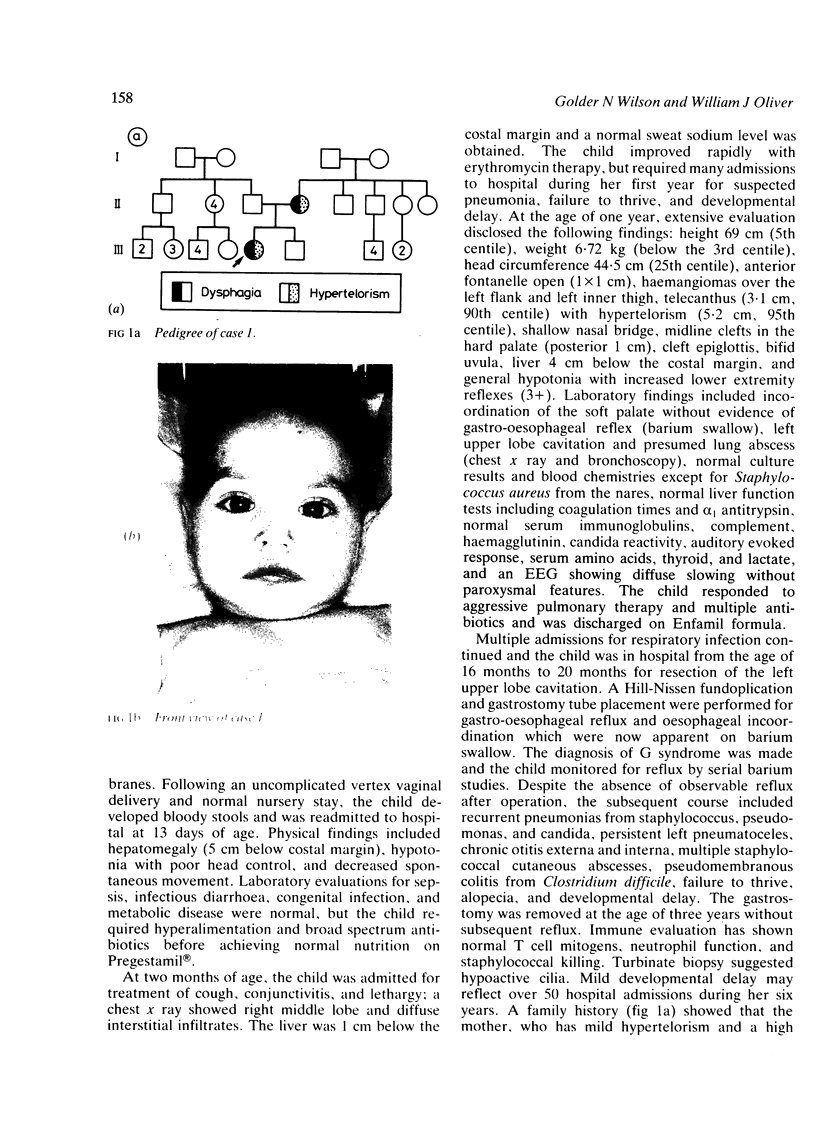
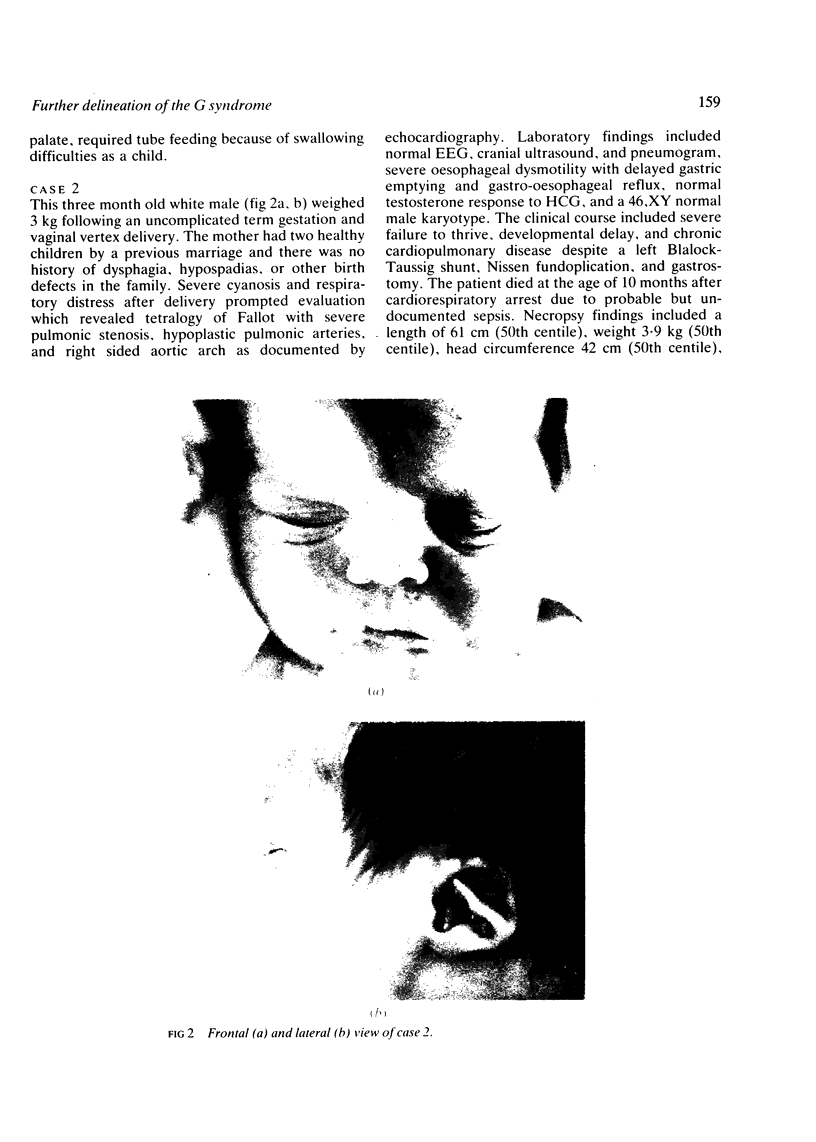
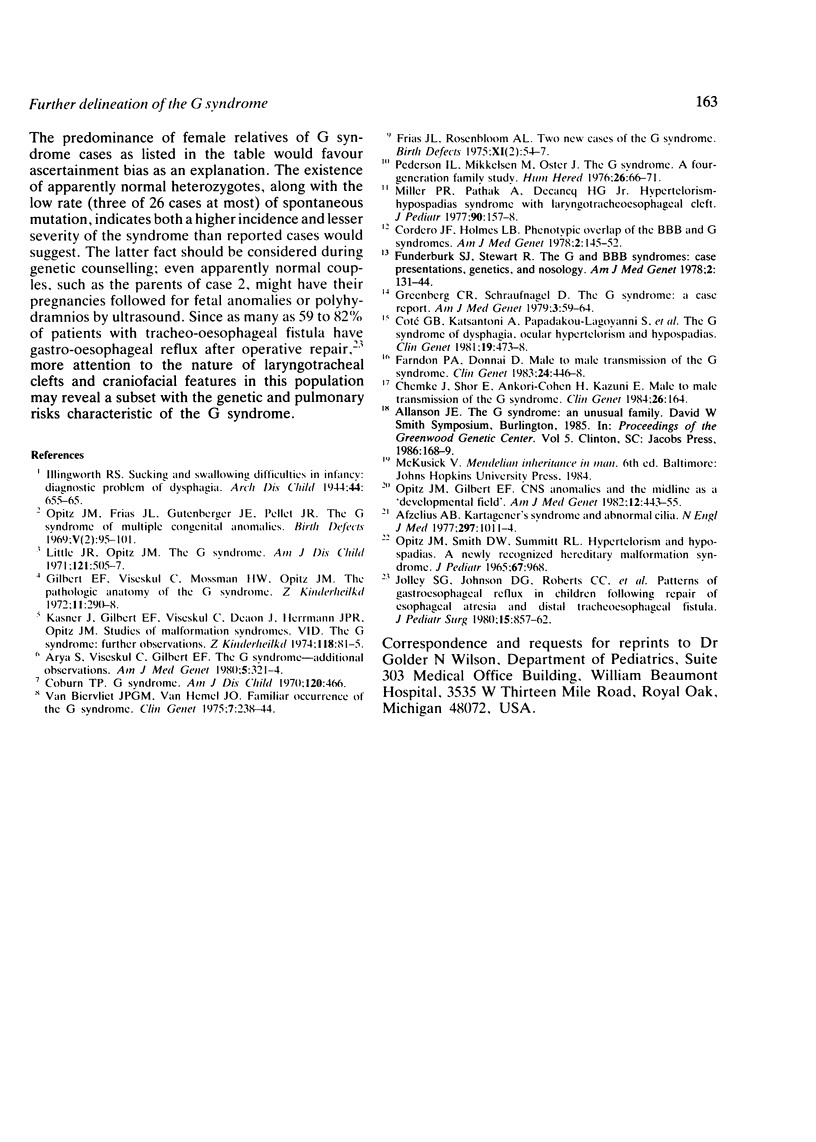
Three families including five subjects with the G or Opitz-Frias syndrome are added to 23 published cases who had dysphagia; characteristics of the two affected relatives were added to 19 well documented published reports. The data from index cases support the concept of the G syndrome as a constellation of midline defects, which include hypertelorism or telecanthus (89%), oesophageal dysmotility (69%), laryngotracheal clefts (44%), cleft palate or bifid uvula (34%), heart defects (29%), hypospadias (100% of males), renal or ureteral anomalies (42%), and mental retardation (38%). Affected relatives, often identified by hypertelorism, dysphagia, or hypospadias, had a much lower incidence of associated defects and mental retardation. They provide a more rounded but still biased view of a syndrome compatible with normal intelligence and life span. The data do not support a highly characteristic face in the G syndrome, which discriminates it from the phenotypically similar BBB syndrome. The variable expressivity and five cases of male to male transmission observed in 18 families are consistent with autosomal dominant inheritance. Vigilance for the morphological characteristics of G syndrome in patients with dysphagia is underscored by the potential for normal development with appropriate intervention.
Full text
PDF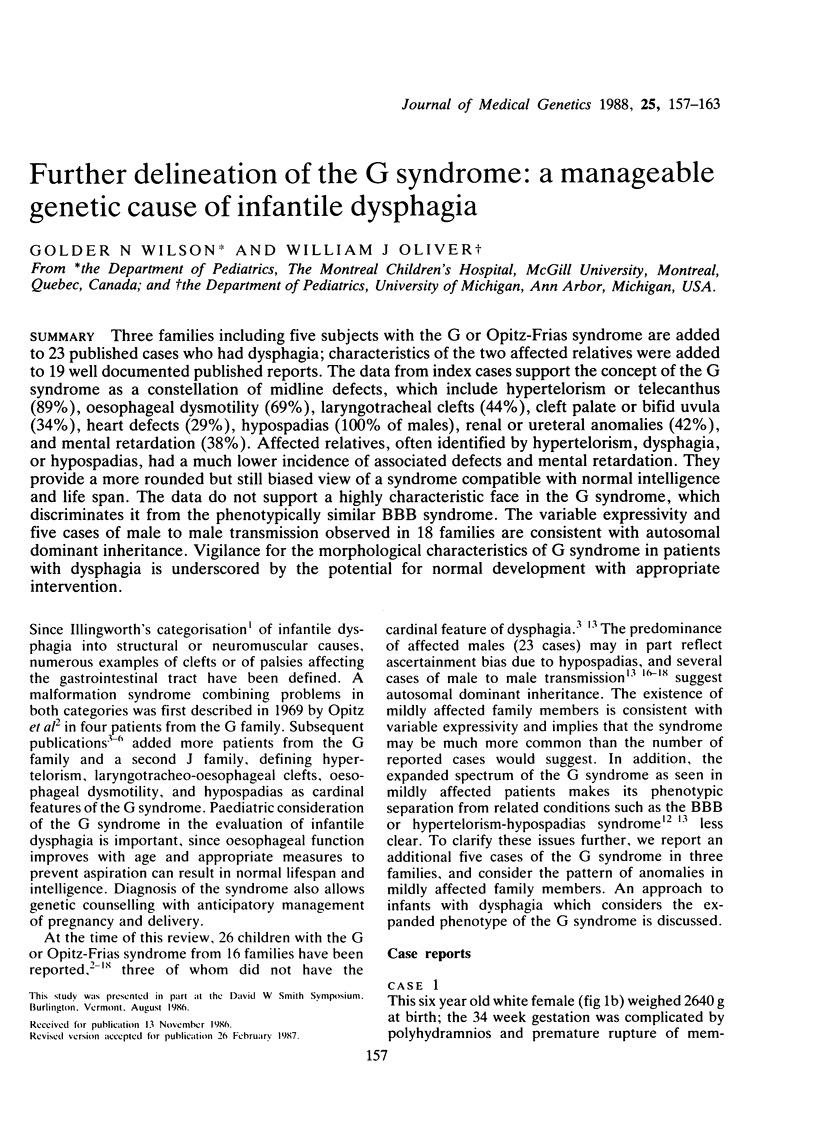



Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Arya S., Viseskul C., Gilbert E. F. The G syndrome--additional observations. Am J Med Genet. 1980;5(3):321–324. doi: 10.1002/ajmg.1320050316. [DOI] [PubMed] [Google Scholar]
- Chemke J., Shor E., Ankori-Cohen H., Kazuni E. Male to male transmission of the G syndrome. Clin Genet. 1984 Aug;26(2):164–164. doi: 10.1111/j.1399-0004.1984.tb00808.x. [DOI] [PubMed] [Google Scholar]
- Coburn T. P. G syndrome. Am J Dis Child. 1970 Nov;120(5):466–466. doi: 10.1001/archpedi.1970.02100100130018. [DOI] [PubMed] [Google Scholar]
- Funderburk S. J., Stewart R. The G and BBB syndromes: case presentations, genetics, and nosology. Am J Med Genet. 1978;2(2):131–144. doi: 10.1002/ajmg.1320020204. [DOI] [PubMed] [Google Scholar]
- Greenberg C. R., Schraufnagel D. The G syndrome: a case report. Am J Med Genet. 1979;3(1):59–64. doi: 10.1002/ajmg.1320030111. [DOI] [PubMed] [Google Scholar]
- Opitz J. M., Gilbert E. F. CNS anomalies and the midline as a "developmental field". Am J Med Genet. 1982 Aug;12(4):443–455. doi: 10.1002/ajmg.1320120408. [DOI] [PubMed] [Google Scholar]
- Pedersen I. L., Mikkelsen M., Oster J. The G syndrome. A four-generation family study. Hum Hered. 1976;26(1):66–71. doi: 10.1159/000152784. [DOI] [PubMed] [Google Scholar]