

Abstract
Background
The number of wearable technological devices or sensors that are commercially available for gait training is increasing. These devices can fill a gap by extending therapy outside the clinical setting. This was shown to be important during the COVID-19 pandemic when people could not access one-on-one treatment. These devices vary widely in terms of mechanisms of therapeutic effect, as well as targeted gait parameters, availability, and strength of the evidence supporting the claims.
Objective
This study aimed to create an inventory of devices targeting improvement in gait pattern and walking behavior and identify the strength of the evidence underlying the claims of effectiveness for devices that are commercially available to the public.
Methods
As there is no systematic or reproducible way to identify gait training technologies available to the public, we used a pragmatic, iterative approach using both the gray and published literature. Four approaches were used: simple words, including some suggested by laypersons; devices endorsed by condition-specific organizations or charities; impairment-specific search terms; and systematic reviews. A findable list of technological devices targeting walking was extracted separately by 3 authors. For each device identified, the evidence for efficacy was extracted from material displayed on the websites, and full-text articles were obtained from the scientific databases PubMed, Ovid MEDLINE, Scopus, or Google Scholar. Additional information on the target population, mechanism of feedback, evidence for efficacy or effectiveness, and commercial availability was obtained from the published material or websites. A level of evidence was assigned to each study involving the device using the Oxford Centre for Evidence-Based Medicine classification. We also proposed reporting guidelines for the clinical appraisal of devices targeting movement and mobility.
Results
The search strategy for this consumer-centered review yielded 17 biofeedback devices that claim to target gait quality improvement through various sensory feedback mechanisms. Of these 17 devices, 11 (65%) are commercially available, and 6 (35%) are at various stages of research and development. Of the 11 commercially available devices, 4 (36%) had findable evidence for efficacy potential supporting the claims. Most of these devices were targeted to people living with Parkinson disease. The reporting of key information about the devices was inconsistent; in addition, there was no summary of research findings in layperson’s language.
Conclusions
The amount of information that is currently available to the general public to help them make an informed choice is insufficient, and, at times, the information presented is misleading. The evidence supporting the effectiveness does not cover all aspects of technology uptake. Commercially available technologies help to provide continuity of therapy outside the clinical setting, but there is a need to demonstrate effectiveness to support claims made by the technologies.
Keywords: wearables, technologies, walking training, rehabilitation, biofeedback, mobile phone
Introduction
Background
Gait is one of the most frequently assessed attributes in clinical settings because gait impairment is the hallmark of several different health conditions [1,2]. Prevalence of poor gait and gait-associated impairments is on the rise because people are living longer, with multimorbidity of chronic conditions such as obesity, diabetes, and arthritis, and because of a global increase in the proportion of neurological conditions [3-5]. Gait impairments and walking limitations from aging, disease, or injury increase the risk of falls, joint damage, and a sedentary lifestyle, leading to a vicious cycle toward further deterioration [6,7]. To illustrate, gait and balance impairments have been shown to increase with age—from 10% among individuals aged between 60 and 69 years to >60% in individuals aged >80 years [8]. Gait and mobility challenges are among the main concerns for older adults and people with neurological conditions and are a major reason for seeking rehabilitation services. There is considerable evidence to support the effectiveness of gait training in older adults and people with neurological conditions [9-15]. Although traditional therapist-led gait training strategies are well-accepted and effective in improving gait patterns, the effects abate with cessation of training [16,17]. Hence, traditional therapist-led gait training alone will not translate into sustained neuromuscular change nor lead to the behavioral change needed for physical activity guidelines to be met.
Effective and accessible treatments for gait impairments will increasingly be needed with the aging of the population and as people with health conditions live longer. Skilled therapy professionals are a limited resource, and therapy is rationed; furthermore, rehabilitation is a global target of the World Health Organization’s 2030 strategy, with key areas for action to increase affordable services and use technology to address this need to assess and reassess how individuals mobilize and move and implement long-term training programs [18]. Increasingly, people with gait vulnerabilities and their family members will turn to technological solutions to supplement and extend rehabilitation services [19,20]. Technological innovations are poised to close the gap between demand and supply [21]. There is no doubt that older adults and people living with health conditions would benefit from focused gait training beyond what is offered during a clinical visit [22,23]. Technology can provide people with opportunities to practice gait-related skills outside the clinical environment and gain ownership over their therapy [24]. There is evidence to support that technology alone can influence positive behavior and that smartphone apps have been shown to reduce sedentary time by 41 minutes per day [25,26]. These effects are thought to be a result of the user’s ability to self-monitor and self-correct, thus providing them with more control and responsibility for their own therapy [26]. Given the unmet need for access to rehabilitation services and the need to continue therapy outside clinical settings, the commercialization of technology is timely and necessary.
Available devices range in sophistication from nonelectronic shoe insoles and walking aids to inertial or pressure sensors. Most of the technologies used have gait assessment functionality, but there is now increasing interest in harnessing the capacity of wearable sensors for providing biofeedback. The literature is rich in supporting the effectiveness of biofeedback in improving gait patterns in healthy and clinical populations [27-30].
There is an increasing number of devices that claim to improve gait impairments through biofeedback. However, it is still rare for these devices to be available to the consumer; most are still tied to a laboratory setting. There is an urgent need to move technological innovations from research laboratories to the people who would benefit the most—those with gait impairments. The COVID-19 pandemic has alerted us to the vulnerability of seniors and people living with chronic health conditions when they were no longer able to access clinical and community resources [31-37]. In addition, the growing size of the older population means that one-on-one treatment will no longer be feasible, and a self-management strategy facilitated by technologies will be needed [31-33,38].
The market of people needing gait training technologies is huge. As a result of direct access of the general public to several technologies, the impact of evidence presented on the websites could affect purchasing behavior. A study on the purchasing intention of consumers who shop on the web found that “high involvement” consumers, defined as people living with health conditions who need to improve their gait to meet functional demands or mobility needs and are intently looking to purchase something specific, were more likely to purchase a product if the number of quality reviews was high [39]. Individuals with gait impairments may be considered “high involvement” consumers and, therefore, may purchase related products based solely on available reviews that may or may not have evidenced research quality.
Gait training technologies must be appealing with features such as product attractiveness, functionality, and price, as well as be supported by robust research demonstrating usability, reliability, efficacy, and effectiveness. All these features are equally important; an attractive product that does not work or a product that does work but is expensive would not be appealing. Although the attractiveness of technologies is often featured on websites, the evidence for efficacy could be hard to locate. Furthermore, the public is not likely to have access, time, or training to find the scientific literature and critically appraise the content to guide the decision to purchase such products.
Objectives
The objectives of this customer-centered review were to create an inventory of devices targeting improvement in gait pattern and walking behavior and identify the strength of the evidence underlying the claims of effectiveness for devices that are commercially available to the general public [40].
Methods
Pragmatic, Iterative Approach
As there is no systematic or reproducible way to identify technologies available to the public to help improve gait, we used a pragmatic and iterative approach. Our search strategy involved a search of gray literature as well as published literature. Figure 1 shows the 4 approaches used to identify a list of commercially available biofeedback devices. We used simple words, including those suggested by laypersons. Our focus was on devices that provided feedback, but this would not be thought of by the consumer. Therefore, we supplemented this strategy by searching for condition-specific organizations or charities because they might endorse such devices. This search yielded 2 feedback devices. We also performed a search using clinical impairment–specific search terms, and this yielded another 15 feedback devices. Finally, we searched for systematic reviews covering gait but found no new devices [41-45]. The search was first conducted in October 2021 and repeated in December 2022. Once we had a list of devices, we searched for evidence of efficacy published on the device web page as well as on PubMed and Google Scholar using the device name to search.
Figure 1.
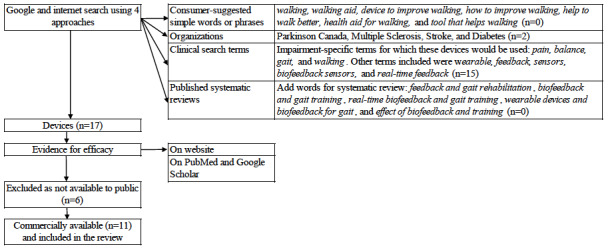
The steps taken to identify commercially available biofeedback devices to improve gait pattern and walking behavior.
A findable list of technological devices targeted to health conditions was extracted separately by 3 authors and compared for completeness. For each device identified, the evidence for efficacy or effectiveness was extracted from material displayed on the websites, and full-text articles were obtained from the scientific databases PubMed, Ovid MEDLINE, Scopus, or Google Scholar. This step was carried out by MM, AA, MW, OS, SG, DG, and HD; any conflicts were resolved in consultation with KM and AA-S. Finally, KM and NEM organized the results into tables and reverified all data and assigned levels of evidence. A level of evidence was assigned to each study involving the device using the Oxford Centre for Evidence-Based Medicine scale [46,47].
Levels of Evidence
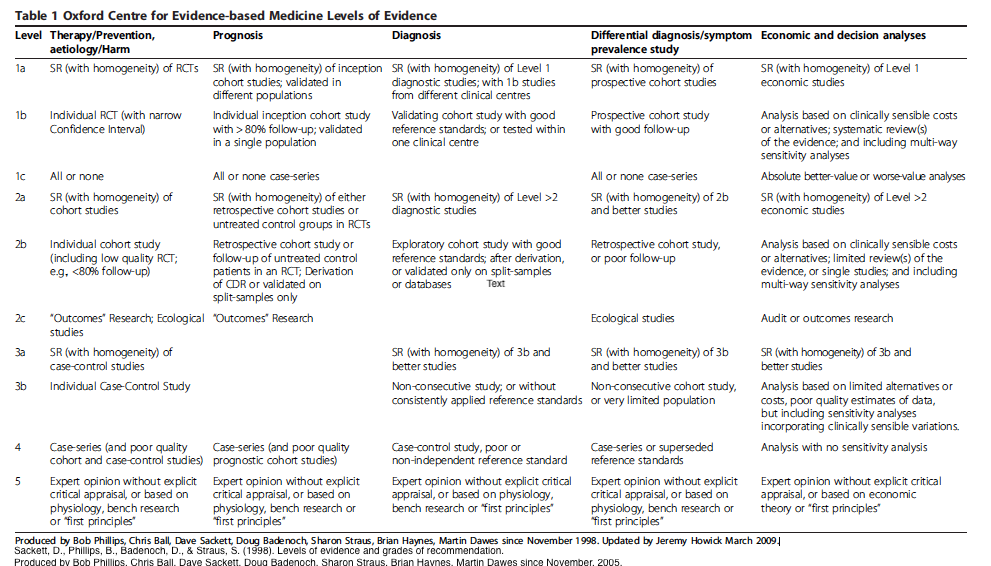
The levels of evidence rating system is a method of quantifying the best clinical evidence that is available about the efficacy and safety of treatment approaches that are destined to be implemented in clinical care [46,47]. The Oxford Centre for Evidence-Based Medicine scale was used because it provides the best granularity of evidence arising from the majority of trials of new technologies that usually are not included in meta-analyses and do not have randomized clinical trials with large sample sizes producing narrow CIs. Multimedia Appendix 1 shows the Oxford Center for Evidence-Based Medicine levels of evidence.
Information on the target population, mechanism of feedback, evidence for efficacy or effectiveness, and commercial availability was obtained from the published material or websites. Only devices that claimed gait rehabilitation or gait quality improvement through any sensory feedback mode—visual, auditory, haptic (tactile or kinesthetic), or vibration—were included. The devices were excluded if the technology was not targeted to any health condition or if it targeted high-functioning populations such as athletes or healthy individuals. The term feedback is defined as a physiological or performance signal arising as a result of human movement that, in turn, generates an output (error or correct performance) that is relayed back to the user and that has the potential to modulate (enhance or diminish) subsequent movement.
Results
Overview
The search yielded 17 wearable devices that claimed to target improvement in gait quality through various types of feedback: 11 (65%) were commercially available, and 6 (35%) were at various stages of research and development. Of the 11 commercially available devices, 2 (18%) were sold under the trademark WalkWithPath: Path Finder Laser Shoes and Pathfeel. The inclusion of the devices was appraised by KM and NEM. Table 1 presents a brief description of the devices (grouped into insoles, wearable sensors, and vests or walking aids), feedback type, target condition, and components. The devices are organized according to availability: directly available to clients or only for research purposes and thus not commercially available. Among the 11 commercially available devices, there were 6 (55%) insoles, 4 (36%) wearable sensors, 1 (9%) vest, and 1 (9%) walking aid; for example, BalancePro insoles, which provide only passive sensory feedback, and FeetMe insoles, which have embedded sensors to provide different types of feedback, including electrical stimulation or an auditory signal. All technologies used a variety of biofeedback (positive, negative, and continuous) and offered options for choosing or providing a single preset sensory stimulus—auditory, haptic, visual, or vibration—enabling users to set individual preferences. A few of the devices offered practitioners and consumers a choice to select the feedback frequency and type of stimuli. Regarding choosing the type of sensory stimulus, there is no information available on the efficacy of one sensory stimulus compared with that of another. Most devices target gait improvement for people with neurological conditions, specifically people with Parkinson disease.
Table 1.
Description of gait training devices (1) available to consumers and (2) for research only.
| Gait rehabilitation devices | Feedback type | Condition | Interface | ||||
| Targeted: directly available to clients | |||||||
|
|
BalancePro: insoles with raised edges that provide passive sensory feedback on soles to enhance proprioception [48,49] | Haptic (continuous feedback) | Older adults, impaired circulation, and neuropathy | None | |||
|
|
FeetMe Stimulate or Insole or Rehab: insoles with embedded sensors that collect gait and balance data and provide electrical stimulation at the foot or ankle to correct the gait pattern [50,51] | Auditory +a, haptic +, and visual + | Neurological conditions, obesity, chronic obstructive pulmonary disease, and older adults | Pressure and IMUb sensors in insoles, electrodes, and Android app | |||
|
|
WalkWithPath (Pathfeel): insoles with embedded pressure sensors that provide vibration corresponding to the pressure detected to enhance sensory information coming from the foot [52,53] | Haptic vibration (continuous feedback) | Parkinson disease and peripheral neuropathy | Pressure sensors and Bluetooth connection to smartphone app | |||
|
|
Vibrating Insoles (Wyss Institute): insoles that provide subthreshold vibration continuously to enhance natural sensory information coming from the foot to improve balance and step consistency [54,55] | Vibration (continuous feedback) | Recreational athletes, older adults, and neurological conditions | None | |||
|
|
Voxx Human Performance Technology socks and insoles: socks or insoles with embedded tactile pattern under the ball of the foot that stimulates the neural system to encourage the brain into a state of homeostasis [56,57] | Tactile (continuous feedback) | Poor balance and fall risk | None | |||
|
|
Walkasins: insoles attached to ankle unit that detect pressure under the foot and provide vibration just above the ankles to improve balance and gait [49] | Haptic vibration + | Asymmetric gait (stroke) and neuropathy | None | |||
|
|
Heel2Toe: sensor worn over the shoe that provides real-time auditory feedback on making “good steps” in which the heel strikes first [58] | Auditory + | Parkinson disease and older adults | IMU sensor and Android app | |||
|
|
MEDRhythms: 2 wearable sensors attached to each shoe that provide rhythmic auditory feedback based on gait parameters to improve gait [59,60] | Auditory + | Neurological conditions | Headphones, IMU sensor, and smartphone app | |||
|
|
CuPiD/Gait Tutor: 3 wireless sensors that evaluate real-time quality of gait and provide vocal message to walk safely, effectively, and smoothly [61] | Auditory and visual –c | Parkinson disease | Smartphone, IMU sensor, and docking station | |||
|
|
WalkWithPath (Path Finder Laser Shoes): lasers attached to shoes bilaterally activated by body weight on the stance foot emit a horizontal light line on the floor on the opposite side for user to step on or over [52,53] | Visual (continuous feedback) | Parkinson disease | None | |||
|
|
ReMoD V5.0 Type 1: vest with attached sensors that detect postural deviations and provide electrical stimulation at the anterior shoulders to correct trunk position when the user deviates past the set threshold [62,63] | Electrical – | Stroke, scoliosis, poor posture, and sensory or vestibular dysfunction | None | |||
|
|
Isowalk: self-propulsive cane that guides user’s step forward [64] | Haptic (continuous feedback) | Fall risk | None | |||
| Research only, not commercially available | |||||||
|
|
Artistic 2.0: insoles that detect asymmetries and use a smartphone app display, high or low tone beeps, or long or short vibrations at the ankle to encourage symmetry | Auditory, visual, and vibration – | Neurological conditions and amputations | Silicon insoles with force sensors, a microcontroller, Bluetooth, and Android app | |||
|
|
Walk-Even: insoles detect uneven weight distribution and use a speaker on the waistband to signal to the user to change weight distribution (auditory cue), or nociceptive electric stimulation is given on the thigh of the unaffected leg to encourage faster movement of the paretic limb | Auditory – and nociceptive – | Asymmetric gait (stroke) | Hard wired | |||
|
|
AmbuloSono: wearable sensor worn on the leg provides auditory feedback (music) once a preset threshold is reached; if steps are too small, the music will stop | Auditory + | Parkinson disease | IMU sensor, audio speaker, iPod Touch, and Bluetooth | |||
|
|
CueStim: electrical stimulation unit with electrodes on the quadriceps or hamstrings that continuously ramp up and down to overcome shuffling and freezing of gait | Electrical (continuous feedback) | Parkinson disease | Electrostimulation device, Bluetooth, smartphone app, and electrodes | |||
|
|
VibeForward: 2 vibratory tactors placed inside the user’s shoes, a small electronics box containing a battery and an IMU sensor strapped around the ankle, and Bluetooth connection to a smartphone app; when activated by a switch on the device or a remote, the tactors provide vibration cycling from the hind foot to the forefoot in synchrony with the user’s step; the smartphone app acts as a remote control for the vibration | Vibration – | Parkinson disease | Tactors, IMU sensor, Bluetooth, and smartphone app | |||
|
|
Walk-Mate: wearable sensor that provides auditory feedback on foot-ground contact; used as a gait compensation device to promote consistent cadence and gait symmetry | Auditory – | Neurological conditions | IMU, computer, headphones, and hard wired | |||
a+: positive feedback.
bIMU: inertial measurement unit.
c–: negative feedback.
Effectiveness of Gait Training Devices
Textbox 1 presents information on population, intervention, control, outcomes, time, training, results, usability, and level of evidence with study design. Of the 11 commercially available devices, 4 (36%) have published evidence of efficacy reported in 10 studies with sample sizes ranging from 6 to 40: CuPiD/Gait Tutor, BalancePRO, Heel2Toe, and WalkWithPath [58,65-67]; for example, the BalancePro insoles are plastic insoles with a raised ridge around the perimeter that provide continuous haptic feedback and are targeted to people with Parkinson disease and older adults. The insoles are available for direct purchase on the company website, and the design patent application is under review. The evidence supporting the BalancePro technology comes from 2 crossover study designs and 1 randomized controlled trial, all at level 2b of evidence using the Oxford Center for Evidence-Based Medicine scale.
Evidence supporting the effectiveness of gait training devices.
BalancePro (studies: 3; level of evidence: 2b)
-
Authors, year: Jenkins et al [66], 2009
Population: individuals with Parkinson disease, n=40: 16 women and 24 men; age-matched controls, n=40: 25 women and 15 men
Intervention: facilitatory shoe insole
Control: conventional flat insole
Outcome: spatiotemporal gait parameters measured using GAITRite mat and muscle activity measured using electromyography (in 20 people with Parkinson disease and 20 controls)
Time: concurrent trials
Training: 10 walking trials: 5 with facilitatory insoles and 5 with conventional insoles
Results: group effect on velocity, step length, and step length variability
Usability: not reported
Level of evidence, study design: 2b, crossover (website and PubMed)
-
Authors, year: Maki et al [68], 1999
Population: older adults, n=14: 6 women and 8 men; 7 healthy controls
Intervention: modified insoles
Control: none
Outcome: center of mass displacement and stepping reactions using force plates
Time: concurrent trials
Experimental condition: multiple transient perturbations and continuous perturbations: 40 and 16, respectively, for older adults and 56 and 24, respectively, for controls
Results: facilitation reduced the number of forward step reactions to perturbations
Usability: not reported
Level of evidence, study design: 2b, crossover (website and PubMed)
-
Authors, year: Perry et al [67], 2008
Population: older adults, n=40: 19 women and 21 men aged 65 to 75 years
Intervention: facilitatory insole
Control: conventional insole
Outcome: lateral displacement of center of mass in relation to base of support during single-support phase
Time: 12 weeks
Training: 12 trials on 4 uneven surfaces wearing each sole
Experimental: 12 weeks of wearing randomly assigned sole
Results: outcome effect for 2 of the 4 uneven surface conditions
Usability: lower fall rate in intervention (25% vs 45%); mild discomfort occurrences reported for 17 out of 240 wear-weeks; 17 out of 20 participants would continue wearing
Level of evidence, study design: 2b, randomized trial (website and PubMed)
Walk With Path (studies: 3; level of evidence: 2b)
-
Authors, year: McCandless et al [69], 2016
Population: individuals with Parkinson disease, n=20: 14 men and 6 women; mean age 68 years; independently ambulatory indoors, with freezing of gait
Intervention: laser cane, sound metronome, vibrating metronome, and vibrating walking stick
Control: no cueing
Outcome: frequency of freezing of gait episodes over 3-meter walk, first step length, second step length, forward center of mass velocity, sideways center of mass velocity, number of forward and backward sways and number of sideways sways, and forward center of pressure velocity (meters per second) and side-to-side center of pressure velocity
Time: concurrent trials, 3 per device and 3 control (total: 15 trials per participant)
Training: none
Results: 12 out of 20 participants contributed 100 freezing and 91 nonfreezing trials; laser cane was most effective for freezing of gait and for movement strategies to reinitiate movement, whereas vibrating walking stick was second most effective; vibration metronome disrupt movement compared with the sound metronome at the same beat frequency
Usability: not reported
Level of evidence, study design: 2b, crossover (website and PubMed)
-
Authors, year: Barthel et al [70], 2018
Population: individuals with Parkinson disease with freezing of gait, n=21: 5 women and 15 men
Intervention: visual cueing using laser shoes
Control: no cueing
Outcome: duration and number of freezing of gait episodes
Time: concurrent trials, 5 trials each during on medication and off medication periods
Training: (1) walking back and forth over 10 meters; (2) task 1 plus counting down from 100 in steps of 7 or 3; (3) turning on command while walking, including 180° and 360° right and left turns; (4) walking to pick up a cone at 7 meters and then back carrying the cone; and (5) walking around obstacles placed on the walkway
Results: cueing reduced the number of freezing of gait episodes, both off (45.9%) and on (37.7%) medication, reduced the percentage of time frozen during the off period by 56.5% (95% CI 32.5-85.8), and reduced the percentage of time frozen during the on by 51.4% (95% CI –41.8 to 91.5)
Usability: not reported
Level of evidence, study design: 2b, crossover (website and PubMed)
-
Authors, year: Velik et al [71], 2012
Population: individuals with Parkinson disease with freezing of gait, n=7: 1 woman and 6 men
Intervention: 3 cueing conditions: no cue, visual cue on for 10 seconds whenever freezing occurred, and continuous visual cue
Control: no cues
Outcome: average duration and number of freezing episodes under 3 conditions
Time: concurrent trials
Training: 6 tasks to be performed: (1) standing up from a chair and getting a glass of water from the kitchen, (2) going with the glass of water to the bathroom and leaving it on the washbasin, (3) walking to the bedroom and picking up a clothes hanger from the cupboard, (4) carrying a clothes hanger to the washing room and leaving it there, (5) going back to the chair, and (6) performing tasks 1 to 5 in reverse order, starting with task 5
Results: continuous cueing: mean duration of freezing reduced by 51%, with 43% fewer freezing of gait episodes; on-demand cueing: mean duration of freezing reduced by 69%, with 9% fewer freezing of gait episodes
Usability: not reported
Level of evidence, study design: 2b, crossover (website and PubMed)
Heel2Toe (studies: 2; level of evidence: 2b)
-
Authors, year: Mate et al [58], 2020
Population: older frail and prefrail persons, n=6: 4 women and 2 men
Intervention: supervised training with the Heel2Toe sensor, 5 sessions over 2 weeks
Control: none
Outcome: spatiotemporal gait parameters and system usability
Time: immediate and posttest feedback; end of training without and with feedback
Training: supervised gait training and walking practice with the Heel2Toe sensor providing feedback for good steps; prescription of 5 exercises, 1 per walking component
Results: immediate and posttraining response: 5 of the 6 participants displayed meaningful changes in terms of good steps, angular velocity, and coefficient of variation, whereas 1 high-functioning person showed no change
Usability: 38-item responses: 25/38 (66%) were at optimal levels, and 9/38 (24%) were at the poorest levels
Level of evidence, study design: 2b, sequential pretest-posttest design (website and PubMed)
-
Authors, year: Carvalho et al [72], 2020
Population: individuals with Parkinson disease, n=6: 4 women and 2 men
Intervention: supervised training with the Heel2Toe sensor, 5 sessions over 2 to 3 weeks
Control: none
Outcome: spatiotemporal gait parameters and system usability
Time: immediate pretest and posttest feedback; end of training without and with feedback
Training: supervised gait training and walking practice with the Heel2Toe sensor providing feedback for good steps; prescription of 8 mobility exercises
Results: immediate and posttraining response: of the 6 participants, 3 displayed meaningful changes in terms of good steps, 4 improved on angular velocity, and 1 reduced coefficient of variation
Usability: 24-item responses: 17/24 (71%) were at optimal levels, and 9/24 (37%) were at the poorest levels
Level of evidence, study design: 2b, randomized clinical trial (website and PubMed)
CuPiD/Gait Tutor (studies: 2; level of evidence: 2b)
-
Authors, year: Ginis et al [65], 2016
Population: individuals with Parkinson disease, n=40: 8 women and 30 men independently ambulatory for at least 10 minutes, with freezing of gait
Intervention: supervised weekly visits for 6 weeks plus recommendation to walk at least 3 times per week for 30 minutes with feedback and cues provided separately
Control: walking training with no feedback
Outcome: gait speed, stride length, and double support time for comfortable gait and dual-task gait conditions; balance evaluated using Mini Balance Evaluation Systems Test; Four Square Step Test; Falls Efficacy Scale-International; 2-minute walk test; freezing of gait; Unified Parkinson’s Disease Rating Scale, part III; cognition; and quality of life
Time: pretest-posttest training (6 weeks) and retention (4 weeks)
Training: weekly home visits for 6 weeks
Results: single-task and dual-task gait speeds improved within group at posttest and follow-up assessments; intervention group improved on balance at posttraining assessment
Usability: not reported
Level of evidence, study design: 2b, randomized clinical trial (website and PubMed)
-
Authors, year: Ginis et al [52], 2017
Population: individuals with Parkinson disease, n=28: 5 women and 23 men; 14 age matched
Intervention: 4 walks (continuous and intelligent cues, intelligent feedback, no information) over 6 weeks with at least 1 week between walks
Control: no information
Outcome: cadence, stride length, and fatigue
Time: concurrent trials
Training: comfortable 1-minute reference walk before testing
Results: decrease in cadence in participants with Parkinson disease without cues or feedback; participants with Parkinson disease reported more fatigue with continuous cueing and intelligent feedback; increase in coefficient of variation in cadence in participants with Parkinson disease; and less variation in cadence with continuous and intelligent cueing in participants with Parkinson disease
Usability: reported
Level of evidence, study design: 2b, crossover (website and PubMed)
Textbox 2 outlines some important areas that would help judge the usefulness of technologies targeting gait from the perspective of consumers. These areas emerged from this review because the needed information was either absent from the papers or inconsistently presented. The list of technology-relevant items presented in Textbox 2 would be applicable for inventors publishing in the scientific literature.
Suggested content for reporting guidelines for the clinical appraisal of devices targeting movement and mobility.
Problem to be addressed: gap that the technology is filling
Functionality: assessment, treatment, or both
Technology type: implant, robot, exoskeleton, biosensors, virtual or augmented reality, assisted living technologies, wearables, smart devices, trackers, remote monitoring, and chatbots
Technology: describe in a way that it can be pictured without an image
Level of technology: technology readiness level (levels 1 to 9) [48]
Population: (1) health condition and special selection criteria and (2) level of technology readiness
Technology: country-specific regulatory authority classification of the medical device; mechanism of action: actual or hypothesized; reliability of algorithm used in the technology; and comparability with existing methods: (1) comparing assessments: competing technologies and (2) comparing treatments: sham, nothing, usual care, alternative form of technology, alternative intervention, and attention control
Experimental protocol: as per Consolidated Standards of Reporting Trials (CONSORT) or other reporting guidelines [50] or as per the Template for Intervention Description and Replication (TIDieR) and other reporting guidelines [56]
-
Outcomes: biofunctional model linking the technology to proximal and distal outcomes:
Proximal (explanatory) outcomes: technological metrics and impairment level from the patient’s perspective
Primary (confirmatory) outcomes: clinically assessed activity outcomes (capacity)
Distal (exploratory) outcomes: real-world assessed activity outcomes (performance) and health-related quality of life
Source of information: patient-reported outcomes, self-reported outcomes, performance outcomes, and technologically assessed outcomes [64]
Results: as per CONSORT or other reporting guidelines; distributional parameters presented for every outcome, every time point, and every transition
Safety: symptoms (new or aggravated), allergies, injuries, abrasions, and falls
-
User experience: qualitative and quantitative information on positive and negative experiences with the technology; actions taken to remedy negative experiences
Usability: quantitative measure of perceived usability
Adoption: data on short-term update and data on long-term use
Level of evidence: level of evidence classification system specified
Discussion
Principal Findings
This review identified a total of 17 wearable biofeedback devices targeting gait patterns and walking behavior. Of these 17 devices, 11 (65%) are commercially available to the public and have a dedicated website for direct purchase. Of these 11 devices, 4 (36%) had published evidence on effectiveness at level 2b according to the Oxford Centre for Evidence-Based Medicine scale (Textbox 1). There was no searchable evidence available for the efficacy or effectiveness of the feedback from the remaining gait training technologies (7/11, 64%). Evidence is primarily generated for 1 health condition, but the claims are generalized to other health conditions with similar gait impairments. There was limited to no data available on accuracy, reliability, usability, and safety. Almost all websites presented user reviews or testimonials, which are likely to be selective in favor of supporting the technology. It is important for clinicians to be aware that some scientific evidence supporting the technology may exist, but a consumer is most likely unable to access the published material. A consumer may be driven to purchase a device or not merely by reading reviews or testimonials.
This review provides a summary of commercial wearable gait training technologies that are currently available in the market or the development phase. A unique feature of this review is that it was conducted from a consumer’s perspective and then augmented by summarizing the evidence from scientific publications. Although the strength of the evidence supporting the effectiveness of these technologies is low or moderate at best, the claims on the website often outweigh the evidence. The results of our review can also be used by professionals involved in gait rehabilitation to direct their clients to promising technologies based on available evidence. These technologies can also be incorporated into treatment plans.
Comparison With Prior Work
Several of the papers (9/10, 90%) that contributed evidence toward the efficacy and effectiveness of the wearable sensors failed to capture or report patient-centered outcomes or declared level of evidence. In summary, the quality of evidence was low. Only 36% (4/11) of the devices had searchable evidence for efficacy potential, with all studies being small-sample sized (Textbox 1). This calls into question the strength of the evidence and the generalizability of the findings outside the study population. Although the mechanism of action and information on spatiotemporal gait parameters have been reported for all devices, it is important to provide information on walking speed, distance, physical function, and walking behaviors such as step count or walking bouts. Overall, the approach to statistical analysis is rudimentary, and inference is mainly based on within-group P values rather than CIs. Lack of raw data in the published manuscripts, such as mean, median, SD, and range, prevented a calculation of between-group effects, effect sizes, and reliable change among other metrics that can potentially provide more interpretable information. Sample sizes are typically small, leading to a high degree of uncertainty in the results. Very few papers (4/10, 40%) reported information on missing data or steps taken to account for missing data and the potential impact on the conclusions.
Strengths and Limitations
There is a challenge in searching for information on technology. A 2022 review evaluated the type and quality of information available on the web for aquatic physiotherapy targeted to people with Parkinson diseases [59]. The authors used a commercial social listening service Awario that searches social media platforms (eg, Twitter and Instagram) and the web for investigator-selected keywords [59]. The strategy used here was a form of snowball sampling where systematic reviews served as the source, and the web was searched for any devices named in these reviews.
Many commercial technology companies reported ≥1 clinical trials that are underway; yet, there is a lack of trial-specific information. A potential consumer is unlikely to track these details. It is important to consider the transparency and accessibility of scientific evidence when making evidence-based recommendations to consumers. There is limited research in this area, specifically from a consumer’s perspective. Although there is a need to provide therapy outside clinical settings, it is critical that companies marketing technologies do not scam people into buying products that are possibly noneffective or even harmful and that clear reporting standards for consumers are made mandatory for these technologies, similar to those now standard for food.
The approach taken here may not have yielded complete results, and, because new technologies are continually developed and added to or removed from the market, the results can quickly become out of date. Many technologies are developed in research settings and are not given a proprietary name until there is evidence to support commercialization. Hence, searching for earlier information is impossible. In addition, the inventors, the authors of the papers, and the entrepreneurs commercializing the technology may not be the same people; hence, an author search will also be fruitless. CuPiD/Gait Tutor is an example of a name change [61,65]. Finally, there is no gold standard for rigorous, systematic gray literature search methods, and there are few resources on how to conduct this type of search; for example, the Cochrane Handbook, often cited as the gold standard for conducting systematic reviews, provides limited guidance and specificity for gray literature search methods [62]. In addition, the reporting of gray literature search methods in systematic reviews is often not held to the same high standards in transparency and reproducibility as the academic database search methods.
Therefore, the findings of this review are only valid based on the search conducted at the time. Given the difficulty in searching for gait training technologies, the search method reported here may be difficult to reproduce. Nevertheless, the information presented on the technologies discovered in this search uncovers existing gaps in the evidence and the reporting.
Future Directions
As newer technologies for gait training are continually developed, it is important that the evidence supporting their efficacy and effectiveness is quickly made available to people to make an informed choice. Often, the published literature is unavailable to the general population because of journal paywalls. There was also a lack of consistency in reporting information related to usability, safety, or user feedback. Standards for reporting on research involving technological devices, in the form of reporting guidelines, seem to be a critical need to ensure that the data needed by the potential consumer are communicated.
There are several reviews on the efficacy and effectiveness of gait training technologies. One objective of the research is to build capacity and empower patients who wish to take charge of their health. By equipping people living with gait impairments with the opportunity to improve walking outside clinical settings through biofeedback is a step in the right direction, given the limited access to rehabilitation services. A few technological innovations were initiated along the commercialization path but were abandoned at different stages. Despite the many benefits of at-home therapy, some challenges exist, including device maintenance, battery life, and technological literacy. One study suggests that the most effective devices are those that have a “user-centered design,” meaning patients or practitioners are involved in the design process [30]. Many of the devices included in this review use this approach by consulting patients for feedback on comfort, ease of use, and preferred feedback modes, when applicable, during pilot studies.
Although there is strong interest from academic institutions and government agencies to transfer technologies from laboratories to clients, there is a need for due diligence on the part of both the institutions and industry to accurately report all the findings that not only support the science but will also influence a client’s or an organization’s decision to purchase the technology.
Research in the field of technology development seems to lack the rigorous research method standards required for drug testing, allowing some devices to enter the market based mainly on safety rather than efficacy. Almost all commercial devices overclaim the efficacy of the technology to other populations not supported by their research; for instance, a website will claim effectiveness for people with gait impairments when the device was tested only in people with Parkinson disease. Finally, it would truly benefit the general public to have a summary of the research in layperson’s terms similar to food standards.
The field of technology evaluation would benefit from reporting guidelines to extend the guidelines for reporting on randomized clinical trials (eg, Consolidated Standards of Reporting Trials [CONSORT]), such as are available for many different types of experimental studies, including pilot and feasibility studies and crossover designs, all of which can be found on the Enhancing the Quality and Transparency of Health Research (EQUATOR) website [54]. There are also guidelines for reporting on the features of the intervention (Template for Intervention Description and Replication [TIDieR]), which would be helpful to fully understand the intervention protocol and encourage replication [56]. For technology, it would be useful to provide additional information on user experience using both closed- and open-ended formats to identify challenges that users encounter with the technology.
Conclusions
This review is the first of its kind from a consumer’s perspective that critically appraises wearable biofeedback gait devices found on the internet, the literature available on the respective websites, and the strength of evidence supporting the claims. The review highlights the need for providing standardized reporting of device capabilities as information accessible to the public when marketing commercialized devices. This review provides the public and health care practitioners with a summary of information that can be used to choose wearable biofeedback gait technologies or decide not to adopt them. The review covers 17 wearable devices that provide 1 form of feedback to improve gait and outlines the mechanisms claimed to underlie gait improvement. There was no predominance for biofeedback type (positive, negative, or continuous). A variety of biofeedback modes have been used (auditory, visual, or haptic), with auditory and vibratory haptic being the most common. The strength of the evidence supporting these devices from scientific sources was at 2a (lower randomized controlled trial) or 2b (prospective controlled trial—not randomized) level. Gaps in reporting all needed information for the consumer were uncovered. The propensity of small trials and heterogeneity of studies and conditions highlight the requirement for standardizing reporting of feedback intervention measures and doses to enable meta-analyses to move gait technological rehabilitation forward. Of note, there is a lack of evidence for motor learning interventions even in the field of sport, with a need for current evidence to be extended by theory-driven, high-quality studies to allow for more consolidated and evidence-based recommendations. Technology has the potential to advance the rehabilitation space and enable a better understanding of optimal interventions for learning and maintaining skills. Taken together, our findings target the need for clear reporting standards for gait interventions.
Abbreviations
- CONSORT
Consolidated Standards of Reporting Trials
- EQUATOR
Enhancing the Quality and Transparency of Health Research
- TIDieR
Template for Intervention Description and Replication
Oxford Centre for Evidence-Based Medicine levels of evidence. https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009.
{kind=link}
Footnotes
Conflicts of Interest: KKVM, AA-S, HD, and NEM are cofounders of the start-up PhysioBiometrics Inc, with the Heel2Toe sensor as a flagship product.
References
- 1.Morris ME, Iansek R, Matyas TA, Summers JJ. The pathogenesis of gait hypokinesia in Parkinson's disease. Brain. 1994 Oct;117 ( Pt 5):1169–81. doi: 10.1093/brain/117.5.1169. [DOI] [PubMed] [Google Scholar]
- 2.von Schroeder HP, Coutts RD, Lyden PD, Billings Jr E, Nickel VL. Gait parameters following stroke: a practical assessment. J Rehabil Res Dev. 1995 Feb;32(1):25–31. [PubMed] [Google Scholar]
- 3.Carroll WM. The global burden of neurological disorders. Lancet Neurol. 2019 May;18(5):418–9. doi: 10.1016/s1474-4422(19)30029-8. [DOI] [PubMed] [Google Scholar]
- 4.Chooi YC, Ding C, Magkos F. The epidemiology of obesity. Metabolism. 2019 Mar;92:6–10. doi: 10.1016/j.metabol.2018.09.005.S0026-0495(18)30194-X [DOI] [PubMed] [Google Scholar]
- 5.Tinajero MG, Malik VS. An update on the epidemiology of type 2 diabetes: a global perspective. Endocrinol Metab Clin North Am. 2021 Sep;50(3):337–55. doi: 10.1016/j.ecl.2021.05.013.S0889-8529(21)00049-9 [DOI] [PubMed] [Google Scholar]
- 6.Jankovic J, Nutt JG, Sudarsky L. Classification, diagnosis, and etiology of gait disorders. Adv Neurol. 2001;87:119–33. [PubMed] [Google Scholar]
- 7.Pirker W, Katzenschlager R. Gait disorders in adults and the elderly: a clinical guide. Wien Klin Wochenschr. 2017 Feb;129(3-4):81–95. doi: 10.1007/s00508-016-1096-4. https://europepmc.org/abstract/MED/27770207 .10.1007/s00508-016-1096-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mahlknecht P, Kiechl S, Bloem BR, Willeit J, Scherfler C, Gasperi A, Rungger G, Poewe W, Seppi K. Prevalence and burden of gait disorders in elderly men and women aged 60-97 years: a population-based study. PLoS One. 2013 Jul 24;8(7):e69627. doi: 10.1371/journal.pone.0069627. https://dx.plos.org/10.1371/journal.pone.0069627 .PONE-D-13-11728 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Arias P, Cudeiro J. Effects of rhythmic sensory stimulation (auditory, visual) on gait in Parkinson's disease patients. Exp Brain Res. 2008 Apr;186(4):589–601. doi: 10.1007/s00221-007-1263-y. https://core.ac.uk/reader/61914795?utm_source=linkout . [DOI] [PubMed] [Google Scholar]
- 10.Cho KH, Lee WH. Virtual walking training program using a real-world video recording for patients with chronic stroke: a pilot study. Am J Phys Med Rehabil. 2013 May;92(5):371–84. doi: 10.1097/PHM.0b013e31828cd5d3.00002060-201305000-00001 [DOI] [PubMed] [Google Scholar]
- 11.Delval A, Krystkowiak P, Delliaux M, Blatt JL, Derambure P, Destée A, Defebvre L. Effect of external cueing on gait in Huntington's disease. Mov Disord. 2008 Jul 30;23(10):1446–52. doi: 10.1002/mds.22125. [DOI] [PubMed] [Google Scholar]
- 12.Dobkin BH. Strategies for stroke rehabilitation. Lancet Neurol. 2004 Sep;3(9):528–36. doi: 10.1016/S1474-4422(04)00851-8. https://europepmc.org/abstract/MED/15324721 .S1474442204008518 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Heeren A, van Ooijen M, Geurts AC, Day BL, Janssen TW, Beek PJ, Roerdink M, Weerdesteyn V. Step by step: a proof of concept study of C-Mill gait adaptability training in the chronic phase after stroke. J Rehabil Med. 2013 Jul;45(7):616–22. doi: 10.2340/16501977-1180. https://www.medicaljournals.se/jrm/content/abstract/10.2340/16501977-1180 . [DOI] [PubMed] [Google Scholar]
- 14.LaGasse AB, Knight A. Rhythm and music in rehabilitation: a critical review of current research. Crit Rev Phys Rehabil Med. 2011;23(1-4):49–67. doi: 10.1615/critrevphysrehabilmed.v23.i1-4.40. [DOI] [Google Scholar]
- 15.Roerdink M, Lamoth CJ, Kwakkel G, van Wieringen PC, Beek PJ. Gait coordination after stroke: benefits of acoustically paced treadmill walking. Phys Ther. 2007 Aug;87(8):1009–22. doi: 10.2522/ptj.20050394. https://core.ac.uk/reader/16139495?utm_source=linkout .ptj.20050394 [DOI] [PubMed] [Google Scholar]
- 16.Peurala SH, Karttunen AH, Sjögren T, Paltamaa J, Heinonen A. Evidence for the effectiveness of walking training on walking and self-care after stroke: a systematic review and meta-analysis of randomized controlled trials. J Rehabil Med. 2014 May;46(5):387–99. doi: 10.2340/16501977-1805. https://www.medicaljournals.se/jrm/content/abstract/10.2340/16501977-1805 . [DOI] [PubMed] [Google Scholar]
- 17.Eng JJ, Tang PF. Gait training strategies to optimize walking ability in people with stroke: a synthesis of the evidence. Expert Rev Neurother. 2007 Oct;7(10):1417–36. doi: 10.1586/14737175.7.10.1417. https://europepmc.org/abstract/MED/17939776 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Gimigliano F, Negrini S. The World Health Organization "rehabilitation 2030: a call for action". Eur J Phys Rehabil Med. 2017 Apr;53(2):155–68. doi: 10.23736/S1973-9087.17.04746-3. [DOI] [PubMed] [Google Scholar]
- 19.Tavares E, Coelho J, Rogado P, Correia R, Castro C, Fernandes JB. Barriers to gait training among stroke survivors: an integrative review. J Funct Morphol Kinesiol. 2022 Oct 13;7(4):85. doi: 10.3390/jfmk7040085. https://www.mdpi.com/resolver?pii=jfmk7040085 .jfmk7040085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wu M, Luo J. Wearable technology applications in healthcare: a literature review. Online J Nurs Inform. 2019;23(3) https://www.himss.org/resources/wearable-technology-applications-healthcare-literature-review . [Google Scholar]
- 21.Jensen W, Andersen OK, Akay M. Replace, Repair, Restore, Relieve – Bridging Clinical and Engineering Solutions in Neurorehabilitation: Proceedings of the 2nd International Conference on NeuroRehabilitation (ICNR2014), Aalborg, 24-26 June, 2014. ICNR '14; Aalborg, Denmark; June 24-26, 2014. 2014. [DOI] [Google Scholar]
- 22.Eskofier BM, Lee SI, Baron M, Simon A, Martindale CF, Gaßner H, Klucken J. An overview of smart shoes in the internet of health things: gait and mobility assessment in health promotion and disease monitoring. Appl Sci. 2017 Sep 25;7(10):986. doi: 10.3390/app7100986. https://www.mdpi.com/2076-3417/7/10/986 . [DOI] [Google Scholar]
- 23.Mikolajczyk T, Ciobanu I, Badea DI, Iliescu A, Pizzamiglio S, Schauer T, Seel T, Seiciu PL, Turner DL, Berteanu M. Advanced technology for gait rehabilitation: an overview. Adv Mech Eng. 2018 Jul 29;10(7):168781401878362. doi: 10.1177/1687814018783627. https://journals.sagepub.com/doi/pdf/10.1177/1687814018783627 . [DOI] [Google Scholar]
- 24.Chen DK, Haller M, Besier TF. Wearable lower limb haptic feedback device for retraining foot progression angle and step width. Gait Posture. 2017 Jun;55:177–83. doi: 10.1016/j.gaitpost.2017.04.028.S0966-6362(17)30159-5 [DOI] [PubMed] [Google Scholar]
- 25.Stephenson A, McDonough SM, Murphy MH, Nugent CD, Mair JL. Using computer, mobile and wearable technology enhanced interventions to reduce sedentary behaviour: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. 2017 Aug 11;14(1):105. doi: 10.1186/s12966-017-0561-4. https://ijbnpa.biomedcentral.com/articles/10.1186/s12966-017-0561-4 .10.1186/s12966-017-0561-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sullivan AN, Lachman ME. Behavior change with fitness technology in sedentary adults: a review of the evidence for increasing physical activity. Front Public Health. 2017 Jan 11;4:289. doi: 10.3389/fpubh.2016.00289. https://europepmc.org/abstract/MED/28123997 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Tate JJ, Milner CE. Real-time kinematic, temporospatial, and kinetic biofeedback during gait retraining in patients: a systematic review. Phys Ther. 2010 Aug;90(8):1123–34. doi: 10.2522/ptj.20080281.ptj.20080281 [DOI] [PubMed] [Google Scholar]
- 28.van Gelder LM, Barnes A, Wheat JS, Heller BW. The use of biofeedback for gait retraining: a mapping review. Clin Biomech (Bristol, Avon) 2018 Nov;59:159–66. doi: 10.1016/j.clinbiomech.2018.09.020. https://eprints.whiterose.ac.uk/181606/ S0268-0033(18)30237-7 [DOI] [PubMed] [Google Scholar]
- 29.Spencer J, Wolf SL, Kesar TM. Biofeedback for post-stroke gait retraining: a review of current evidence and future research directions in the context of emerging technologies. Front Neurol. 2021 Mar 30;12:637199. doi: 10.3389/fneur.2021.637199. https://europepmc.org/abstract/MED/33859607 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Bowman T, Gervasoni E, Arienti C, Lazzarini SG, Negrini S, Crea S, Cattaneo D, Carrozza MC. Wearable devices for biofeedback rehabilitation: a systematic review and meta-analysis to design application rules and estimate the effectiveness on balance and gait outcomes in neurological diseases. Sensors (Basel) 2021 May 15;21(10):3444. doi: 10.3390/s21103444. https://air.unimi.it/handle/2434/869269 .s21103444 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Chambonniere C, Lambert C, Tardieu M, Fillon A, Genin P, Larras B, Melsens P, Baker JS, Pereira B, Tremblay A, Thivel D, Duclos M. Physical activity and sedentary behavior of elderly populations during confinement: results from the FRENCH COVID-19 ONAPS survey. Exp Aging Res. 2021;47(5):401–13. doi: 10.1080/0361073X.2021.1908750. [DOI] [PubMed] [Google Scholar]
- 32.Goethals L, Barth N, Guyot J, Hupin D, Celarier T, Bongue B. Impact of home quarantine on physical activity among older adults living at home during the COVID-19 pandemic: qualitative interview study. JMIR Aging. 2020 May 07;3(1):e19007. doi: 10.2196/19007. https://aging.jmir.org/2020/1/e19007/ v3i1e19007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Sepúlveda-Loyola W, Rodríguez-Sánchez I, Pérez-Rodríguez P, Ganz F, Torralba R, Oliveira DV, Rodríguez-Mañas L. Impact of social isolation due to COVID-19 on health in older people: mental and physical effects and recommendations. J Nutr Health Aging. 2020;24(9):938–47. doi: 10.1007/s12603-020-1469-2. https://europepmc.org/abstract/MED/33155618 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kokorelias KM, Ripat J, Jones CA, Mayo NE, Salbach NM, Barclay R. Moving through COVID-19: perspectives of older adults in the getting older adults outdoors study. J Aging Phys Act. 2022 Aug 01;30(4):705–15. doi: 10.1123/japa.2021-0098. [DOI] [PubMed] [Google Scholar]
- 35.Oliveira MR, Sudati IP, Konzen VD, de Campos AC, Wibelinger LM, Correa C, Miguel FM, Silva RN, Borghi-Silva A. COVID-19 and the impact on the physical activity level of elderly people: a systematic review. Exp Gerontol. 2022 Mar;159:111675. doi: 10.1016/j.exger.2021.111675. https://europepmc.org/abstract/MED/34954282 .S0531-5565(21)00457-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Suárez-González A, Rajagopalan J, Livingston G, Alladi S. The effect of COVID-19 isolation measures on the cognition and mental health of people living with dementia: a rapid systematic review of one year of quantitative evidence. EClinicalMedicine. 2021 Jul 31;39:101047. doi: 10.1016/j.eclinm.2021.101047. https://linkinghub.elsevier.com/retrieve/pii/S2589-5370(21)00327-8 .S2589-5370(21)00327-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ho KH, Mak AK, Chung RW, Leung DY, Chiang VC, Cheung DS. Implications of COVID-19 on the loneliness of older adults in residential care homes. Qual Health Res. 2022 Jan;32(2):279–90. doi: 10.1177/10497323211050910. [DOI] [PubMed] [Google Scholar]
- 38.Pillai D. Impact of COVID-19 pandemic on physiotherapy services in India: a survey. Manipal Academy of Higher Education. 2021. Jan 05, [2023-03-20]. https://impressions.manipal.edu/cgi/viewcontent.cgi?article=1085&context=mcph .
- 39.Park DH, Lee J, Han I. The effect of on-line consumer reviews on consumer purchasing intention: the moderating role of involvement. Int J Electron Commer. 2007;11(4):125–48. doi: 10.2753/jec1086-4415110405. https://dl.acm.org/doi/10.5555/1481722.1481728 . [DOI] [Google Scholar]
- 40.Mayo NE, Ow N, Asano M, Askari S, Barclay R, Figueiredo S, Hawkins M, Hum S, Inceer M, Kaur N, Kuspinar A, Mate KK, Moga AM, Mozafarinia M. Reducing research wastage by starting off on the right foot: optimally framing the research question. Qual Life Res. 2022 Oct;31(10):2889–99. doi: 10.1007/s11136-022-03117-y.10.1007/s11136-022-03117-y [DOI] [PubMed] [Google Scholar]
- 41.Chaparro-Cárdenas SL, Lozano-Guzmán AA, Ramirez-Bautista JA, Hernández-Zavala A. A review in gait rehabilitation devices and applied control techniques. Disabil Rehabil Assist Technol. 2018 Nov;13(8):819–34. doi: 10.1080/17483107.2018.1447611. [DOI] [PubMed] [Google Scholar]
- 42.Ekker MS, Janssen S, Nonnekes J, Bloem BR, de Vries NM. Neurorehabilitation for Parkinson's disease: future perspectives for behavioural adaptation. Parkinsonism Relat Disord. 2016 Jan;22:S73–7. doi: 10.1016/j.parkreldis.2015.08.031.S1353-8020(15)00370-3 [DOI] [PubMed] [Google Scholar]
- 43.Ma CZ, Wong DW, Lam WK, Wan AH, Lee WC. Balance improvement effects of biofeedback systems with state-of-the-art wearable sensors: a systematic review. Sensors (Basel) 2016 Mar 25;16(4):434. doi: 10.3390/s16040434. https://www.mdpi.com/resolver?pii=s16040434 .s16040434 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Nagano H, Begg RK. Shoe-insole technology for injury prevention in walking. Sensors (Basel) 2018 May 08;18(5):1468. doi: 10.3390/s18051468. https://www.mdpi.com/resolver?pii=s18051468 .s18051468 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Shull PB, Jirattigalachote W, Hunt MA, Cutkosky MR, Delp SL. Quantified self and human movement: a review on the clinical impact of wearable sensing and feedback for gait analysis and intervention. Gait Posture. 2014;40(1):11–9. doi: 10.1016/j.gaitpost.2014.03.189.S0966-6362(14)00287-2 [DOI] [PubMed] [Google Scholar]
- 46.Phillips B, Ball C, Sackett D, Badenoch D, Straus S, Haynes B, Dawes M. Oxford centre for evidence-based medicine: levels of evidence (March 2009) Nuffield Department of Primary Care Health Sciences. 2009. [2023-03-20]. https://www.cebm.ox.ac.uk/resources/levels-of-evidence/oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009 .
- 47.Sackett DL. Evidence-based medicine. Semin Perinatol. 1997 Feb;21(1):3–5. doi: 10.1016/s0146-0005(97)80013-4. https://www.ncbi.nlm.nih.gov/nlmcatalog/?term=Seminars+in+Perinatology%5BJournal%5D . [DOI] [PubMed] [Google Scholar]
- 48.Mankins JC. Technology readiness assessments: a retrospective. Acta Astronaut. 2009;65(9-10):1216–23. doi: 10.1016/j.actaastro.2009.03.058. https://www.sciencedirect.com/science/article/abs/pii/S0094576509002008 .63/6/595 [DOI] [Google Scholar]
- 49.Balance Pro. [2023-03-23]. https://balancepro.ca/
- 50.Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. J Pharmacol Pharmacother. 2010 Jul;1(2):100–7. doi: 10.4103/0976-500X.72352. https://europepmc.org/abstract/MED/21350618 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.FeetMe. [2023-03-23]. https://feetmehealth.com/
- 52.Ginis P, Heremans E, Ferrari A, Dockx K, Canning CG, Nieuwboer A. Prolonged walking with a wearable system providing intelligent auditory input in people with Parkinson's disease. Front Neurol. 2017 Apr 6;8:128. doi: 10.3389/fneur.2017.00128. https://europepmc.org/abstract/MED/28428770 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Walk With Path. [2023-03-23]. https://www.walkwithpath.com/
- 54.Richards D. The EQUATOR network and website. Evid Based Dent. 2007;8(4):117. doi: 10.1038/sj.ebd.6400533.6400533 [DOI] [PubMed] [Google Scholar]
- 55.Vibrating insoles for better balance. Wyss Institute. [2023-03-23]. https://wyss.harvard.edu/technology/vibrating-insoles-for-better -balance/
- 56.Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, Altman DG, Barbour V, Macdonald H, Johnston M, Lamb SE, Dixon-Woods M, McCulloch P, Wyatt JC, Chan AW, Michie S. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014 Mar 07;348:g1687. doi: 10.1136/bmj.g1687. https://core.ac.uk/reader/19913708?utm_source=linkout .bmj.g1687 [DOI] [PubMed] [Google Scholar]
- 57.VoxxLife. [2023-03-23]. https://voxxlife.com .
- 58.Mate KK, Abou-Sharkh A, Morais JA, Mayo NE. Real-time auditory feedback-induced adaptation to walking among seniors using the heel2toe sensor: proof-of-concept study. JMIR Rehabil Assist Technol. 2019 Dec 11;6(2):e13889. doi: 10.2196/13889. https://rehab.jmir.org/2019/2/e13889/ v6i2e13889 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Terrens AF, Soh SE, Morgan P. What web-based information is available for people with Parkinson's disease interested in aquatic physiotherapy? A social listening study. BMC Neurol. 2022 May 05;22(1):170. doi: 10.1186/s12883-022-02669-3. https://bmcneurol.biomedcentral.com/articles/10.1186/s12883-022-02669-3 .10.1186/s12883-022-02669-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.MEDRhythms. [2023-03-23]. https://medrhythms.com .
- 61.mHealth Technologies. [2023-03-23]. https://mhealthtechnologies.it .
- 62.Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Cochrane Handbook for Systematic Reviews of Interventions. 2nd edition. Hoboken, NJ, USA: John Wiley & Sons; 2019. Oct, [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.ReMoD. [2023-03-23]. https://www.hemiparese-therapie.de/gehhilfe-remod/
- 64.Mayo NE, Figueiredo S, Ahmed S, Bartlett SJ. Montreal accord on Patient-Reported Outcomes (PROs) use series - paper 2: terminology proposed to measure what matters in health. J Clin Epidemiol. 2017 Sep;89:119–24. doi: 10.1016/j.jclinepi.2017.04.013.S0895-4356(17)30409-2 [DOI] [PubMed] [Google Scholar]
- 65.Ginis P, Nieuwboer A, Dorfman M, Ferrari A, Gazit E, Canning CG, Rocchi L, Chiari L, Hausdorff JM, Mirelman A. Feasibility and effects of home-based smartphone-delivered automated feedback training for gait in people with Parkinson's disease: a pilot randomized controlled trial. Parkinsonism Relat Disord. 2016 Jan;22:28–34. doi: 10.1016/j.parkreldis.2015.11.004. https://core.ac.uk/reader/34645871?utm_source=linkout .S1353-8020(15)30027-4 [DOI] [PubMed] [Google Scholar]
- 66.Jenkins M, Almeida QJ, Spaulding SJ, van Oostveen RB, Holmes JD, Johnson AM, Perry SD. Plantar cutaneous sensory stimulation improves single-limb support time, and EMG activation patterns among individuals with Parkinson's disease. Parkinsonism Relat Disord. 2009 Nov;15(9):697–702. doi: 10.1016/j.parkreldis.2009.04.004.S1353-8020(09)00091-1 [DOI] [PubMed] [Google Scholar]
- 67.Perry SD, Radtke A, McIlroy WE, Fernie GR, Maki BE. Efficacy and effectiveness of a balance-enhancing insole. J Gerontol A Biol Sci Med Sci. 2008 Jun;63(6):595–602. doi: 10.1093/gerona/63.6.595.63/6/595 [DOI] [PubMed] [Google Scholar]
- 68.Maki BE, Perry SD, Norrie RG, McIlroy WE. Effect of facilitation of sensation from plantar foot-surface boundaries on postural stabilization in young and older adults. J Gerontol A Biol Sci Med Sci. 1999 Jun;54(6):M281–7. doi: 10.1093/gerona/54.6.m281. [DOI] [PubMed] [Google Scholar]
- 69.McCandless PJ, Evans BJ, Janssen J, Selfe J, Churchill A, Richards J. Effect of three cueing devices for people with Parkinson's disease with gait initiation difficulties. Gait Posture. 2016 Feb;44:7–11. doi: 10.1016/j.gaitpost.2015.11.006. https://europepmc.org/abstract/MED/27004625 .S0966-6362(15)00942-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Barthel C, van Helvert M, Haan R, Janssen AM, Delval A, de Vries NM, Weerdesteyn V, Debû B, van Wezel R, Bloem BR, Ferraye MU. Visual cueing using laser shoes reduces freezing of gait in Parkinson's patients at home. Mov Disord. 2018 Oct;33(10):1664–5. doi: 10.1002/mds.27455. [DOI] [PubMed] [Google Scholar]
- 71.Velik R, Hoffmann U, Zabaleta H, Marti Masso JF, Keller T. The effect of visual cues on the number and duration of freezing episodes in Parkinson's patients. Annu Int Conf IEEE Eng Med Biol Soc. 2012;2012:4656–9. doi: 10.1109/EMBC.2012.6347005. [DOI] [PubMed] [Google Scholar]
- 72.Carvalho LP, Mate KK, Cinar E, Abou-Sharkh A, Lafontaine AL, Mayo NE. A new approach toward gait training in patients with Parkinson's Disease. Gait Posture. 2020 Sep;81:14–20. doi: 10.1016/j.gaitpost.2020.06.031.S0966-6362(20)30232-0 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Oxford Centre for Evidence-Based Medicine levels of evidence. https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009.