

Abstract
Yoga interventions can reduce stress, but the mechanisms remain largely unidentified. Understanding how yoga works is essential to optimizing interventions. The present study tested five potential psychosocial mechanisms (increased mindfulness, interoceptive awareness, spiritual well-being, self-compassion, and self-control) that have been proposed to explain yoga’s impact on stress.
Method:
Forty-two participants (62% female; 64% White) in a yoga program for stress reduction completed surveys at baseline (T1), mid-intervention (T2), and post-intervention (12 weeks; T3). We measured both perceived global stress and stress reactivity. Changes were assessed with paired t-tests; associations between changes in mechanisms were tested in residual change models.
Results:
Only stress reactivity decreased, on average, from T1 to T3. Except for self-compassion, all psychosocial mechanisms increased from T1 to T3, with minimal changes from T2 to T3. Except for self-control, increases in each mechanism were strongly associated with decreases in both measures of stress between T1 and T2 and decreases in perceived global stress from T1 to T3 (all p’s<.05)
Conclusions:
Increased psychosocial resources are associated with stress reduction. Yoga interventions targeting these resources may show stronger stress reduction effects. Future research should test these linkages more rigorously using active comparison groups and larger samples.
Keywords: Yoga, stress-reduction, mind-body, self-regulation
Stress is a commonly-experienced aversive state purported to impact the course of disease and illness at a systemic level (Cohen, Edmondson, & Kronish, 2015; Muscatell & Eisenberger, 2012). Indeed, many health conditions have been shown to directly relate to or be exacerbated by stress (e.g., migraine, gastrointestinal problems, hypertension), and even health conditions that are not overtly related to stress often have close linkages (Muscatell & Eisenberger, 2012). For example, acute pain severity is highly influenced by perceived stress (Wieland et al., 2017; Woda, Picard, & Dutheil, 2016). In addition, stress itself is widely considered to constitute a problematic health condition (Goyal et al., 2014).
Stress is one of the most commonly studied outcomes of yoga practice (Domingues, 2018) and yoga interventions targeting stress reduction have generally demonstrated favorable findings (Chong, Tsunaka, Tsang, Chan, & Cheung, 2011; Pascoe & Bauer, 2015; Pascoe, Thompson, & Ski, 2017). Indeed, randomized controlled trials (RCTs) of yoga conducted across varied samples, including healthy stressed individuals, employees, students, pregnant women, people in treatment for cancer, and people with hypertension, arthritis, headaches, and asthma, have demonstrated significant reductions in self-reported stress (see Pascoe & Bauer, 2015, for a review).
Importantly, self-reported stress can reflect either global perceptions of psychological pressure in one’s life (e.g., feeling overwhelmed, unable to keep up) or physiological arousal that leaves one overly-reactive to provocations (e.g., feeling agitated, intolerant, touchy). While related, these aspects of stress are distinct in terms of individuals’ experience (Oken, Chamine, & Wakeland, 2015; Flett, Nepon, Hewitt, & Fitzgerald, 2016). consequences (Adam & Epel, 2007; Crawford & Henry, 2003), and treatment approaches (Chiesa & Seretti, 2009; Iglesias et al., 2012; Lindsay, Young, Smyth, Brown, & Creswell, 2018). Yoga research has generally focused on the former (e.g., Chong et al., 2011), but people tend to find both aspects of stress aversive and troubling (Aldwin, 2007; Cohen, Kamarck, & Mermelstein 1983; Lovibond & Lovibond, 1994). Thus, assessing the impact of yoga on both aspects of stress may be useful, given that yoga’s effects on each aspect is distinct and might act through different mechanisms of change. For example, stress reactivity may be impacted more strongly by physical posture and breathwork than would psychological perceived stress. In turn, elements of yoga that target cognitive-affective aspects of stress appraisals, such as mindfulness, self-compassion, and meditation, may exert stronger direct effects on psychological stress than on stress reactivity. However, these differences remain purely speculative in the absence of empirical research and merit formal tests.
Indeed, despite the considerable amount of research on yoga and stress, we know little about how yoga reduces stress. Until recently, researchers focused primarily on testing yoga’s efficacy for improving health status across a variety of health problems and conditions, with little emphasis on cognitive-behavioral mechanisms of change. As efficacy is increasingly demonstrated in clinical trials research, understanding how yoga produces salutary effects is emerging as an important next step toward optimizing interventions offered to the public. To date, surprisingly few studies have focused on identifying the mechanisms through which yoga reduces stress (Riley & Park, 2015), and of those, most lacked adequate sample sizes, time frames, and theoretical bases. However, multiple theoretical perspectives have been advanced regarding the psychological mechanisms that might underlie yoga’s effects on stress (Gard, Noggle, Park, Vago, & Wilson, 2014; Kinser et al., 2012; Streeter et al., 2012). Among the most promising are increased mindfulness, interoceptive awareness, self-compassion, self-control, and spiritual well-being.
First, myriad studies have shown that yoga practice is positively related to mindfulness. Several studies have tested whether mindfulness mediates yoga’s effects on outcomes such as post-traumatic stress (PTS) symptoms, with mixed effects (e.g., Mehling et al., 2018; Dick et al., 2014), but we were not able to locate studies that specifically examined mindfulness as a mechanism of yoga’s effects on stress per se. Interoceptive awareness, the representation of the body’s internal states, has been suggested as a related potential mechanism of action for body-based mindfulness interventions, particularly those with a strong physical basis such as yoga (Mehling et al., 2011). Improving awareness of one’s internal states may provide opportunities to engage in mind-body skills that allow yoga practitioners to consciously intervene in their own stress reduction. One clinical trial of war veterans with PTSD found that interoceptive awareness, along with mindfulness, corresponded with reductions in symptoms in an integrated exercise program that included some elements of yoga (Neukirch, Reid, & Shires, 2018). Again, we were unable to find any formal tests of interoceptive awareness as a mechanism of change that may predict stress reduction in a yoga intervention.
Improvement in self-compassion, or mindful self-kindness, has also been suggested to be a mechanism by which yoga reduces stress (Braun et al., 2016; Neff & Germer, 2012). Self-compassion involves being caring and compassionate towards oneself in the face of hardship or perceived inadequacy (Neff, 2003). Acting with kindness towards oneself is associated with less stress reactivity and better coping skills (Allen & Leary, 2010). We located one study that tested self-compassion as a mediator of yoga’s effects on stress, a longitudinal study of 33 young adults in a four-month residential yoga intervention program; increases in self-compassion were associated with reductions in perceived stress (Gard et al., 2012).
Self-control and spiritual well-being have also been theoretically and empirically linked to yoga practice (Gard et al., 2014; Gerbarg & Brown, 2015), but we were unable to find any studies directly testing mechanistic linkages to stress. Self-control, the capacity to consciously alter or override one’s incipient responses, especially to bring them into line with one’s goals or standards, is related to lower stress levels (Tangney et al., 2004; Park et al., 2016) and several studies have suggested that yoga can increase self-control (e.g., Park et al., 2017; Ramadoss & Bose, 2010). Copious empirical evidence links higher spiritual well-being with lower levels of stress (e.g., Park & Slattery, 2013), and several studies have demonstrated that yoga is associated with positive aspects of spirituality (Büssing, Hedtstück, Khalsa, Ostermann, & Heusser, 2012; Gaiswinkler & Unterrainer, 2016). Thus, while not directly tested to date, these pathways—self-control and spiritual well-being—may indeed explain yoga’s effects on stress.
The present study set out to examine these five potential mechanisms of change (mindfulness, interoceptive awareness, spiritual well-being, self-compassion, and self-control) that may be associated with the effects of a 12-week yoga intervention and subsequent stress reduction. We elected to use an intervention based on Kripalu yoga, a practice that is relatively high in body awareness, acceptance/self-compassion, breathwork, mental and emotional awareness, and active postures compared to other yoga types (Park et al., 2018). Based on previous literature, we hypothesized that: 1) all five psychosocial mechanisms, as well as indicators of two different aspects of stress, would significantly improve over the course of the intervention; 2) changes in psychosocial mechanisms from pre- to mid-treatment would be associated with changes in both indicators of stress from pre- to mid-and pre- to post-treatment.
Method
Participants and procedures
The current study comprises a secondary analysis of a parent study assessing the effects of yoga on dietary change, which will be reported elsewhere (Masked for review, under review). Recruitment from two sites in the Northeastern US – an urban medical school in MA and a rural public university in CT – began in April 2015 and final assessments were completed in October 2016. Recruitment ads for a stress reduction program were posted via public transit and direct mail and online advertisements. Study candidates completed a web survey and phone screen, and for those remaining eligible, an in-person screening appointment where they provided written informed consent. Final eligibility was then confirmed following completion of the Mini International Neuropsychiatric Interview (MINI; Sheehan et al., 1998), the Eating Disorders module from the DSM-IV Structured Clinical Interview (SCID; First, Spitzer, Gibbon, & Williams, 1995), and a BMI assessment. Participants were required to be between 23–67 years of age and to be seeking stress reduction.
Exclusion criteria, based on the parent study, encompassed an exercise regimen of more than 180 minutes per week (based on Haskell et al., 2007), consumption of 5 or more servings of fruits and vegetables, current diagnosis of psychiatric illness or prior eating disorder diagnosis as determined by the MINI or SCID eating disorders module, significant prior meditation or yoga experience (defined as ≥12 classes in last 3 years or more than 20 classes in lifetime), medications that altered appetite, and medical conditions that would limit the ability to exercise or do yoga. Following screening, 117 volunteers provided informed consent, of whom 84 were randomized. Participant flow is shown in Figure 1.
Figure 1.
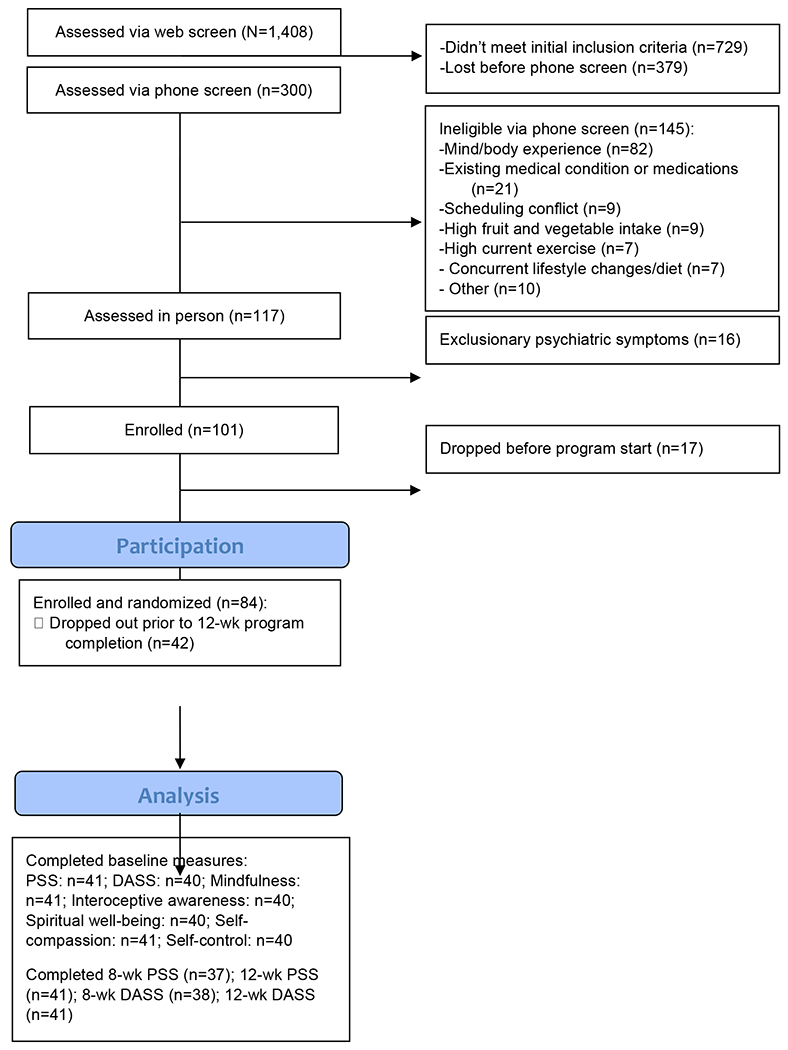
Participant Flow (CONSORT diagram)
Participants were randomized with equal allocation ratio into one of three home practice groups for the program duration: “low practice” (10 min./day six days per week), “medium practice” (40 min./day three days per week, and 10 min./day three days a week), and “high practice” (40 min./day six days per week). The parent study was conservatively powered on an N of 135 participants to detect significant differences in change between home practice groups. In light of the present study’s focus on covariance between stress and potential mechanisms over the course of the yoga program, the analyses reported here were collapsed across randomization groups to preserve statistical power.
Following initial baseline assessment (T1), this study included two additional assessment points: at 8 weeks (T2; mid-treatment), and at 12 weeks (T3; post-treatment). Participants were remunerated up to $100 for completing study assessments and received the yoga program for free. The study protocol was approved by both sites’ Institutional Review Boards (IRBs) and monitored by Westat. The protocol is registered in Clinicaltrials.gov (NCT02098018).
Yoga intervention
The Kripalu yoga intervention integrated yoga practice with yoga philosophy pertinent to self- and affect-regulation to decrease physiological arousal and enhance well-being. Participants learned how to monitor and modulate mental, emotional, and physiological responses moment-to-moment through in-class experiential exercises and prescribed home yoga practice. The intervention was 12 weeks in length and consisted of two consecutive segments. The first segment was a manualized eight-week intervention designed to serve as an introduction to mindful yoga that was initially created and piloted by the Kripalu Center for Yoga. The intervention was slightly modified for use with a high-stress population. Each of the eight once-weekly, two-hour sessions included 100–115 minutes of yoga practice (meditation, breathing exercises, postures, relaxation) and 25–30 min. of theory/philosophy. The second segment began at the ninth week, comprised four weeks of 90-minute, once-weekly sessions of yoga practice (no didactic content), and concluded at 12 weeks. Participants who completed nine or more sessions from the first and/or second segment of the yoga intervention were considered to have received the full “dose” of the intervention and were categorized as compliant to the study protocol. Treatment compliance had no bearing on the analyses reported here; all participants who completed post-treatment assessments were retained for analyses (see Data Analysis section).
Measures
Psychological Stress and Stress Reactivity were assessed, respectively, with a measure tapping into global psychological appraisals of one’s life as overwhelmingly stressful (the Perceived Stress Scale; PSS; Cohen & Williamson, 1988) and a measure tapping descriptions of oneself as stress-reactive (stress subscale of the Depression Anxiety Stress Scale; DASS-21; Lovibond & Lovibond, 1995). The PSS contains 10 items, rated from 0 (Never) to 3 (Very Often); higher sum scores indicate higher levels of overall perceived stress. The PSS has good reliability and validity (Cohen & Williamson, 1988). The PSS is designed to measure subjective perceptions of stress depending on changes in environmental stressors and coping resources (Cohen & Williamson, 1988); thus, no standardized clinical cut-offs exist for this measure. Within the present study, alphas for the PSS were .90, .93, and .91, at T1, T2, and T3, respectively. The DASS-21 stress subscale consists of 7 of the 21 items of the DASS-21 scale and assesses stress in terms of stress reactivity and arousal (e.g., “touchy”, “agitated”, “difficult to relax”). Items are rated from 0 (did not apply to me at all) to 3 (applied to me very much, or most of the time); higher sum scores indicate higher levels of stress. Clinical cut-offs for stress scores on the DASS were developed by authors, including: normal (0–14) mild (15–18), moderate (19–25), severe (26–33), and extremely severe (34+) (Lovibond & Lovibond, 1995). The DASS subscales have good reliability and validity (Lovibond & Lovibond, 1995). Within the present study, alphas for the DASS stress subscale were .83, .85, and .88, at T1, T2, and T3, respectively.
Mindfulness was assessed with the 24-item Five-Facet Mindfulness Questionnaire, short form (FFMQ-SF; Bohlmeijer, ten Klooster, Fledderus, Veehof, & Baer, 2011), a revision of the original 39-item FFMQ (Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006). The FFMQ taps into five domains of mindfulness (acting with awareness, describing, observing, non-reacting, non-judging) and produces a global score. Item responses range from 1 (Never or Very Rarely True) to 5 (Very Often or Always True); higher average scores indicate greater mindfulness. The FFMQ global score has demonstrated good validity and reliability (Bohlmeijer et al., 2011). In the present study, alphas were .88, .89, and .90, at T1, T2, and T3, respectively.
Interoceptive awareness was assessed with the 32-item Multi-dimensional Assessment of Interoceptive Awareness Scale (MAIA; Mehling et al., 2012). Item responses range from 1 (Never) to 5 (Always). Higher scores indicate more interoceptive awareness. The MAIA’s global domain, used in the present study, sums eight subscales (noticing, not distracting, not worrying, attention regulation, emotional awareness, self-regulation, body listening, and trusting). The MAIA global scale demonstrates good internal consistency (Mehling et al., 2012). In the present study, alpha was .93, .94, and .93 at T1, T2, and T3, respectively.
Spiritual well-being was assessed with the 12-item Functional Assessment of Chronic Illness Therapy - Spiritual Well-Being (FACIT-Sp; Peterman, Fitchett, Brady, Hernandez, & Cella, 2002). Item responses range from 0 (Not at all) to 4 (Very much), with higher sum scores indicating greater spiritual well-being. The FACIT-Sp generates subscales for meaning, peace, and faith and an overall score, the latter of which was used in the present study. The validation study indicated good internal consistency for the overall scale (Peterman et al., 2002). Within the present study, alphas were .83, .86, and .88, at T1, T2, and T3, respectively.
Self-compassion was assessed with the 12-item Self-Compassion Scale, Short Form (SCS-SF; Raes, Pommier, Neff, & Van Gucht, 2011), a revision of the original 26-item SCS (Neff, 2003). Item responses range from 1 (Almost Never) to 5 (Almost Always), with higher scores indicating greater self-compassion. The SCS generates six subscales (self-kindness, self-judgment, common humanity, isolation, mindfulness, over-identification) and a global score, the latter used in the present study. The SCS-SF demonstrated good internal consistency for the global scale in the validation study (Raes et al., 2011). Within the present study, alphas were .89, .87, and .82, at T1, T2, and T3, respectively.
Self-control was assessed with the 10-item Brief Self-Control Scale (BSCS; Tangey et al., 2004). Items are rated from 1 (Not at all like me) to 5 (Very much like me) and summed; higher scores indicate higher self-control. The BSCS produces two subscales and an overall score, the latter reported here. The BSCS has demonstrated adequate reliability and validity (Tangey et al., 2004). Within the present study, alphas were .78, .86, and .88, at T1, T2, and T3, respectively.
Recruitment and retention
At study start, a total of 84 participants attended at least one intervention session and elected to proceed with study participation. Those who did not complete T3 assessments (n=42) evidenced no significant variance on baseline demographics or study variables relative to intervention completers (n=42; p’s>.11). Information on attendance and study attrition and completion rates are detailed in Figure 1.
Data Analysis
Descriptive statistics were conducted to describe demographics and study variables at all timepoints; when available, clinical cut-offs were used to interpret magnitude of study variables. Paired t-tests were conducted to determine if study variables differed between T1 and T2, T2 and T3, and T1 and T3; effect sizes were calculated using Cohen’s d to describe standardized magnitudes of change between time-points. Study variables were inter-correlated using Pearson’s r to determine if any meaningful relationships existed at T1. Research site (i.e., rural vs. urban) and cohort (i.e., time of year that the intervention was completed) were also examined as potential covariates to study variable at T1 by conducting a series of ANOVAs. Correlational analyses were carried out to test primary mechanism of change hypotheses. For each mechanism and stress measure, standardized residuals were obtained by regressing observed endpoints on baseline scores (e.g., T2 PSS scores were regressed on T1 PSS scores). Standardized residuals of mechanisms and stress measures were correlated using Pearson’s r; correlations were compared between stress measures using Z-tests. Standardized residuals of mechanisms were also inter-correlated using Pearson’s r to determine if any meaningful relationships existed between mechanisms of change. Missing data within those who completed T3 assessments was negligible (1 to 2 missing values, <=5 for few variables), and thus list-wise deletion was utilized. Alpha for two-sided tests was set to .05. All analyses were conducted in IBM SPSS Statistics for Windows, Version 26.0.
Results
Descriptive Information
Descriptive statistics and change in all study variables is outlined in Table 1.
Table 1.
Participant Characteristics and Estimated Differences between Timepoints.
| T1 (n=42) | T2 | T3 | T1 to T2 | T2 to T3 | T1 to T3 | ||||
|---|---|---|---|---|---|---|---|---|---|
|
|
|||||||||
| %/ M (SD) | M (SD) | M (SD) | d | t (p) | d | t (p) | d | t (p) | |
| Gender (% Female) | 61.9% | ||||||||
| Race (% White) | 64.3% | ||||||||
| Ethnicity (% Hispanic/Latino) | 9.5% | ||||||||
| Age | 41.0 (14.2) | ||||||||
| Body Mass Index (kg/m2) | 25.2 (4.9) | ||||||||
| Psychological Stress (PSS) | 18.5 (6.8) | 18.3 (8.1) | 17.1 (7.1) | 0.06 | −0.43 (.67) | 0.17 | −1.37 (.18) | 0.20 | −1.52 (.14) |
| Stress Reactivity (DASS) | 15.2 (9.3) | 13.5 (8.9) | 12.0 (9.2) | 0.20 | −1.35 (.19) | 0.14 | 0.80 (.43) | 0.37 | −2.16 (.04) |
| Mindfulness (FFMQ-SF) | 3.4 (0.5) | 3.5 (0.5) | 3.6 (0.5) | 0.11 | 0.87 (.39) | 0.21 | 2.05 (.05) | 0.29 | 2.36 (.02) |
| Interoceptive Awareness (MAIA) | 2.3 (0.7) | 3.0 (0.7) | 3.0 (0.7) | 1.01 | 6.28 (<.001) | <0.01 | .02 (.98) | 0.98 | 4.98 (<.001) |
| Spiritual Well-being (FACIT-Sp) | 26.6 (7.8) | 29.1 (8.9) | 29.7 (8.6) | 0.30 | 2.08 (.05) | 0.04 | 2.43 (.75) | 0.41 | 3.22 (.003) |
| Self-Compassion (SCS-SF) | 3.2 (0.8) | 3.3 (0.7) | 3.4 (0.6) | 0.12 | 0.91 (.37) | 0.16 | 1.24 (.22) | 0.28 | 1.92 (.06) |
| Self-Control (BSCS) | 43.6 (8.1) | 45.5 (9.0) | 46.1 (8.6) | 0.24 | 1.91 (.07) | 0.02 | 0.27 (.79) | 0.29 | 2.12 (.04) |
Note. Bolded values indicate p<.05
Demographics.
Participants who completed the intervention were predominantly female (61.9%; n=26), were an average age of 41.0 years old (SD=14.2), and had an average baseline BMI of 25.2 (overweight; SD=4.9). A majority of participants were White (64.3%; n=27), with fewer being Asian (11.9%; n=5), biracial (11.9%; n=5), or reporting another (4.8%; n=2) or no race (7.1%; n=3). Few participants were Hispanic/Latino (9.5%; n=4). Over half of participants had a graduate degree (50.0%; n=21) or a 4-year undergraduate degree (33.3%; n=14), and fewer had a 2-year undergraduate degree (11.9%; n=5), some college completion (2.4%; n=1), or a high school diploma (2.4%; n=1). Most participants were either currently married (47.6%; n=20) or never married (40.5%; n=17); few participants were divorced (7.1%; n=3) or separated (2.4%; n=1).
Stress.
As measured by the DASS, stress reactivity was mild to moderate at T1, and remained similar between T1 and T2, and T2 and T3. However, decreases in stress reactivity were moderate from T1 to T3. Psychological stress as measured by the PSS declined over timepoints, but these small effect sizes were not statistically significant.
Mechanisms.
Mindfulness was similar at T1 and T2, increased slightly between T2 and T3, and between T1 and T3. Interoceptive awareness greatly increased from T1 to T2 and remained similar between T2 and T3; increases between T1 and T3 were large, and similar to the observed increases between T1 and T2. Spiritual well-being increased with only small effect sizes from T1 to T2 and remained similar between T2 and T3; increases between T1 and T3 were moderate. Self-compassion remained statistically unchanged at T1, T2, and T3. Self-control also remained similar at T1, T2, and T3, with a small statistically significant increase from T1 to T3.
Differences in study variables by research site and cohort.
Regarding differences in study variables between research site and cohort, only baseline self-control differed by research site, in that the rural site (M=46.5, SD=8.5) reported significantly greater self-control than the urban site (M=39.6, SD=5.7), F(1,39)=8.5, p=.006. No study variables differed by cohort.
Cross-Sectional Correlations among Mechanisms and Stress at Baseline
Inter-correlation of mechanisms with stress.
Stress reactivity and psychological stress (as measured by DASS-21 and PSS, respectively) were strongly correlated at T1 (r=0.72, p<.001). Higher psychological stress was related to lower levels of most psychosocial mechanisms: mindfulness (r=−0.59, p<.001), spiritual well-being (r=−0.47, p=.002), self-compassion (r=−0.63, p<.001), and self-control (r=−0.45, p=.004), but was not significantly related to interoceptive awareness (p=.24). Associations with stress reactivity were similar for mindfulness (r=−0.42, p=.007), self-compassion (r=−0.47, p=.002), and self-control (r=−0.33, p=.04), but stress reactivity was not significantly related to interoceptive awareness or spiritual well-being at T1 (p’s>.10).
Intercorrelation of mechanisms
Mindfulness was positively associated with spiritual well-being (r=0.58, p<.001), self-compassion (r=0.77, p<.001), and self-control at T1 (r=0.50, p=.001). Spiritual well-being was also positively associated with self-compassion (r=0.54, p<.001) and self-control (r=0.38, p=.02). Self-compassion was positively correlated with self-control (r=0.43, p=.005). Interoceptive awareness was only marginally positively related to self-compassion (r=0.31, p=.052). No other relationships were statistically significant (p’s>.14).
Intercorrelation of Residual Change in Mechanisms and Stress
Intercorrelation of changes in mechanisms.
As shown in Table 2, many inter-correlations between residual changes in mechanisms from T1 to T2 were noted: increases in self-compassion were associated with increases in mindfulness, interoceptive awareness, and spiritual well-being. Increases in spiritual well-being also correlated with increases in self-control. Increases in mindfulness and interoceptive awareness were marginally associated (p=.053).
Table 2.
Inter-correlations between Residual Changes in Psychosocial Mechanisms from T1 to T2
| T1 to T2 | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1. Mindfulness (FFMQ-SF) | 1.00 | |||
| 2. Interoceptive Awareness (MAIA) | 0.33 | 1.00 | ||
| 3. Spiritual Well-being (FACIT-Sp) | 0.17 | 0.26 | 1.00 | |
| 4. Self-Compassion (SCS-SF) | 0.55 ** | 0.45 ** | 0.34 * | 1.00 |
| 5. Self-Control (BSCS) | 0.30 | 0.12 | 0.33 * | 0.09 |
Note.
p<.05.
p<.01.
p<.001.
Bolded values indicate p<.05.
Intercorrelation of changes in stress
As shown in Table 3, decreases in psychological stress were strongly associated with decreases in stress reactivity from T1 to T2, T2 to T3, and T1 to T3. Decreases in psychological stress from T1 to T3 were also strongly associated with decreases in stress reactivity from T2 to T3, and vice versa, decreases in stress reactivity from T1 to T3 were strongly associated with decreases in psychological stress from T2 to T3. Residual changes in neither stress measures from T1 to T2 associated with changes in the other from T2 to T3 or T1 to T3.
Table 3.
Inter-correlations between Residual Changes in Stress
| Stress Reactivity (DASS) |
|||
|---|---|---|---|
| Psychological Stress (PSS) | T1-T2 | T2-T3 | T1-T3 |
| T1-T2 | 0.60 *** | 0.11 | 0.30 |
| T2-T3 | −0.09 | 0.52 ** | 0.48 ** |
| T1-T3 | 0.30 | 0.49 ** | 0.60 *** |
Note.
p<.05
p<.01.
p<.001.
Bolded values indicate p<.05
Intercorrelation of changes in mechanisms with changes in stress.
As shown in Table 4, residual increases from T1 to T2 in all psychosocial mechanisms except self-control were significantly associated with residual decreases in both stress reactivity and global psychological stress from T1 to T2. The correlation between T1-T2 residual change in spiritual well-being and T1-T2 change in stress was greater for psychological stress than stress reactivity. Residual changes in mechanisms from T1 to T2 were not associated with residual changes in stress reactivity or psychological stress from T2 to T3. For psychological stress, associations between T1 to T2 changes in mechanisms and T1 to T3 changes in stress followed the same pattern of statistical significance as did correlations with T1 to T2 changes in psychological stress (i.e., all residual change scores were significantly associated, excepting self-control). In contrast, only T1 to T2 change in self-compassion was significantly associated with T1 to T3 change in stress reactivity. The correlation between T1-T2 residual change in mindfulness and T1-T3 change in stress was greater for psychological stress than stress reactivity.
Table 4.
Associations between Post-Intervention Changes in Psychological Stress (PSS) and Stress Reactivity (DASS) and Changes in Proposed Mechanisms
| T1 to T2 | T2 to T3 | T1 to T3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
|
|
|||||||||
| T1 to T2 | PSS | DASS | Z (p) | PSS | DASS | Z (p) | PSS | DASS | Z (p) |
| Mindfulness (FFMQ-SF) | −0.45 ** | −0.40 * | −0.4 (.70) | −0.17 | −0.03 | −0.9 (.37) | −0.42 * | −0.13 | −2.1 (.04) * |
| Interoceptive Awareness (MAIA) | −0.41 * | −0.42 ** | 0.1 (.92) | −0.14 | −0.16 | 0.2 (.87) | −0.38 * | −0.32 | −0.4 (.66) |
| Spiritual Well-being (FACIT-Sp) | −0.63 *** | −0.38 * | −2.1 (.03) * | 0.02 | −0.02 | 0.3 (.77) | −0.38 * | −0.12 | −1.9 (.06) |
| Self-Compassion (SCS-SF) | −0.64 *** | −0.73 *** | 0.9 (.35) | −0.07 | −0.18 | 0.7 (.47) | −0.50 ** | −0.40 * | −0.8 (.45) |
| Self-Control (BSCS) | −0.25 | −0.16 | −0.6 (.53) | −0.06 | 0.05 | −0.7 (.49) | −0.13 | 0.08 | −1.5 (.14) |
Note.
p<.05.
p<.01
p<.001.
Bolded values indicate p<.05.
Discussion
These results advance yoga intervention research by providing essential information on psychological mechanisms through which yoga practice may reduce perceived stress. Most importantly, we demonstrate the usefulness of examining psychosocial mechanisms of change in a clinical trial and provide potentially fruitful direction for future research to build on the current evidence base regarding yoga and stress.
First, while stress reactivity and psychological stress are fairly strongly related, we found different patterns of yoga’s effects on these two outcomes. Although both aspects of stress declined across the intervention timepoints, only the reduction in stress reactivity was statistically significant across the entire sample. Yet, generally, we found stronger associations of within-person changes in psychosocial resources with perceived psychological stress than with stress reactivity, suggesting that cognitive/emotional aspects of stress may be most directly linked to the proposed “active ingredients” of yoga intervention.
Such differential findings may also be related to the type of yoga that we tested. Kripalu yoga emphasizes a self-compassionate stance toward stressful experience, such that participants are encouraged to non-judgmentally attend to and accept stressful experience while using breathwork and posture to regulate the effects of stress on well-being (Faulds, 2005). Future research might compare different yoga interventions that are optimized more for reactivity or psychological stress to determine differential effects. For example, an intervention encouraging participants to direct attention away from stressful experience or reappraise perceptions of events as stressful might have stronger effects on perceptions of psychological than physiological stress. These findings also suggest that researchers should be more explicit about the type of stress that they are intent on studying and may have implications for future review articles, which might find differential effects for yoga on different dimensions of stress.
Second, all of the psychological resources included here increased over the course of the intervention, as we would expect based on previous research (e.g., Gard et al., 2012; DiGreeson et al, 2011; Dick et al., 2014; Mehling et al., 2018; Park et al., 2018; Bussing et al., 2012). The exception to this general trend was self-compassion, which did not significantly increase over the course of the intervention, in contrast to prior yoga studies (e.g., Gard et al., 2012). All of these increases became larger—and several only then large enough to be statistically significant at T3, suggesting that length of practice has a meaningful influence on steady change in psychological resources. In the present study, interoceptive awareness demonstrated by far the largest effect size from pre- to post-intervention (d = 0.98); in contrast, mindfulness, self-compassion, and self-control all demonstrated only small effect sizes (ds = 0.28, 0.28, 0.29). Future studies will benefit from examining change in these same proposed psychosocial mechanisms following different types of yoga (e.g., Bikram, pranayama), since it is likely that different practices will have very different effects on psychosocial mechanisms and change in perceived stress and stress reactivity (Park, Finkelstein-Fox, Groessl, Lee, & Elwy, 2020). It may also be the case that change in psychological responses to stress (i.e., mindfulness, self-compassion, self-control) after a longer periods of regular yoga practice than what was necessitated by the present study, whereas attention to internal states (i.e., interoceptive awareness) changes more quickly. It will be very interesting for future research to examine change in mindfulness, self-compassion, and self-control after several months of regular yoga practice, particularly among a non-clinical sample of novice practitioners like the one included here.
Of note, the results reported here suggest that most of the hypothesized mechanisms demonstrated patterns of change concurrent with, rather than prior to, changes in stress. This finding highlights an important distinction between Kripalu yoga’s utility as a stress management resource vs. standalone clinical intervention. Even a single session of yoga practice has demonstrated significant pre-post effects on positive and negative affective experience (Park et al., 2020), and regular, repeated yoga practice has been associated with positive stress-related outcomes (Gard et al., 2014; Greenberg et al., 2018). In contrast to talk-based cognitive behavioral therapies that provide explicit discussion of disordered emotion regulation abilities (Hofmann, Sawyer, Fang, & Asnaani, 2012), mechanisms of yoga interventions such as Kripalu may act much more quickly upon perceptions of acute stress by directing non-judgmental attention toward physical experience, and thus require different methods of assessing change in real time (e.g., ecological momentary assessment, measurement of affective states pre- and post- practice). Future research on yoga interventions will benefit from creative measurement individual variation in cognitions, affect, and stress reactivity.
Third, all of the proposed mechanisms, with the exception of self-control, demonstrated substantial associations with both aspects of stress by T2 and continued to show statistically significant associations only with psychological stress by T3. Changes in self-compassion continued to correlate with change in both aspects of stress by T3. Importantly, the strength of covariation between mechanisms and both psychological stress and stress reactivity was similar. This is with exception to the association between residual change in spiritual well-being and mindfulness from T1 to T2 and change in stress from T1 to T2 and T1 to T3, respectively, which was much stronger for psychological stress than for stress reactivity. This finding supports the possibility that spiritual well-being and mindfulness may more strongly act upon psychological stress within a temporal pathway, in contrast to more simultaneous covariation demonstrated with stress reactivity.
Finally, by examining the intercorrelations between changes in multiple mechanisms over time, we also highlight the extent to which various psychosocial resources covary during the course of a mindful yoga intervention; for example, results suggest that self-compassion and mindfulness may change at a similar rate, whereas changes in mindfulness and self-control or spiritual well-being may follow different patterns of change across a 12-week yoga intervention. These preliminary findings may have implications for the design of larger clinical trials targeting psychosocial mechanisms of change in stress; it will be particularly interesting for future studies to test the covariance between distinct correlated variables such as self-compassion and interoceptive awareness over multiple timepoints to parse apart causal or lagged associations between these constructs.
Limitations of our study must be acknowledged. We do not have a control group against which we could compare our findings, although it would be valuable to determine the extent to which stress and psychosocial resources changed over time independently of the yoga intervention. The strongest design would be an active comparison arm that controlled for nonspecific effects, but even an assessment-only group would allow ruling out temporal or seasonal effects (Park et al., 2014). Our study was also underpowered to detect longitudinal effects of smaller magnitude due to a high non-completion rate and participant scheduling difficulties; it is likely that a larger sample would have elucidated more reliable changes in both stress and psychological resources and provided more generalizable findings. Our measures were all self-report and thus liable to all the biases inherent in self-report measures (Paulhus & Vazire, 2007). Further, our set of psychological resources, while broad, likely leaves out other important psychological resources that may be important mechanisms of yoga’s effects on stress. In addition, we tested only one type of yoga; different types of yoga may have different effects on stress and resources. Further, our findings were associative and causal inferences cannot be directly made.
Although these many limitations render our findings suggestive rather than conclusive, they provide direction for subsequent research aimed at better understanding how yoga exerts salutary effects on stress. Future research should examine each of the potential mechanisms identified in the present study, as all five showed significant increases over time and four demonstrated significant roles within the hypothesized pathways linking yoga and stress. Clinical trials to test these pathways should be fully powered and include a strong comparison condition to verify them. Testing different types of yoga with different emphases may further illuminate which aspects of yoga exert stronger effects on specific psychological resources.
These results may have clinical implications for yoga therapists as well as other healthcare providers aiming to reduce stress. Given the different patterns demonstrated in our data, therapists treating stress-related complaints might consider the different kinds of impact that psychological resources have on global psychological stress and reactivity, which have the potential to inform treatment planning and even intervention optimization for highly stressed populations.
Our results suggest that Kripalu yoga may have beneficial effects for positive psychological resources such as interoceptive awareness, mindfulness, spiritual well-being, and self-compassion, all of which may have temporal effects on within-person change in perceived stress over time. Further, experiences of stress reactivity appear to decline significantly over the course of a mindful yoga intervention, suggesting that Kripalu yoga may be especially beneficial for individuals experiencing marked arousal and overreactions to stress exposure. Given increasing evidence of yoga’s effects on stress, future research may build on these results to better understand the specific pathways through which different aspects and types of yoga can reduce different types of stress, ultimately leading the way to personalized yoga interventions for stress reduction.
Funded by:
NIH NCCIH (grant 1R34AT007197)
References
- Adam TC, & Epel ES (2007). Stress, eating and the reward system. Physiology & Behavior, 91, 449–458. [DOI] [PubMed] [Google Scholar]
- Aldwin CM (2007). Stress, coping and development. New York, NY: Guilford. [Google Scholar]
- Allen AB, & Leary MR (2010). Self-Compassion, stress, and coping. Social and Personality Psychology Compass, 4, 107–118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baer RA, Smith GT, Hopkins J, Krietemeyer J, & Toney L (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment, 13, 27–45. [DOI] [PubMed] [Google Scholar]
- Bohlmeijer E, ten Klooster PM, Fledderus M, Veehof M, & Baer R (2011). Psychometric properties of the Five-Facet Mindfulness Questionnaire in depressed adults and development of a short form. Assessment, 18, 308–320. [DOI] [PubMed] [Google Scholar]
- Braun TD, Park CL, Gorin AA, Garivaltis H, Noggle JJ, & Conboy LA (2016) Group-based yogic weight loss with Ayurveda-inspired components: A pilot investigation of female yoga practitioners and novices. International Journal of Yoga Therapy, 26, 55–72. [DOI] [PubMed] [Google Scholar]
- Büssing A, Hedtstück A, Khalsa SBS, Ostermann T, & Heusser P (2012). Development of specific aspects of spirituality during a 6-month intensive yoga practice. Evidence-Based Complementary and Alternative Medicine, 2012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chiesa A, & Serretti A (2009). Mindfulness-based stress reduction for stress management in healthy people: A review and meta-analysis. The Journal of Alternative and Complementary Medicine, 15, 593–600. [DOI] [PubMed] [Google Scholar]
- Chong CSM, Tsunaka M, Tsang HW, Chan EP, & Cheung WM (2011). Effects of yoga on stress management in healthy adults: A systematic review. Alternative Therapies in Health and Medicine, 17, 32–38. [PubMed] [Google Scholar]
- Cohen BE, Edmondson D, & Kronish IM (2015). State of the art review: Depression, stress, anxiety, and cardiovascular disease. American Journal of Hypertension, 28, 1295–1302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen S, Kamarck T, Mermelstein R (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, 385–396. [PubMed] [Google Scholar]
- Cohen S, Williamson G. (1988). Perceived stress in a probability sample of the United States. In Spacapan S & Oskam S (Eds.), The social psychology of health: Claremont symposium on applied social psychology. 31–67. Sage: Newbury Park, CA. [Google Scholar]
- Crawford JR, & Henry JD (2003). The Depression Anxiety Stress Scales (DASS): Normative data and latent structure in a large non clinical sample. British Journal of Clinical Psychology, 42, 111–131. [DOI] [PubMed] [Google Scholar]
- Dick AM, Niles BL, Street AE, DiMartino DM, & Mitchell KS (2014). Examining mechanisms of change in a yoga intervention for women: The influence of mindfulness, psychological flexibility, and emotion regulation on PTSD symptoms. Journal of Clinical Psychology, 70, 1170–1182. [DOI] [PubMed] [Google Scholar]
- DiGreeson JM, Webber DM, Smoski MJ, Brantley JG, Ekblad AG, Suarez EC, & Wolever RQ (2011). Changes in spirituality partly explain health-related quality of life outcomes after Mindfulness-Based Stress Reduction. Journal of Behavioral Medicine, 34, 508–518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Domingues RB (2018). Modern postural yoga as a mental health promoting tool: A systematic review. Complementary Therapy and Clinical Practice, 31, 248–255. [DOI] [PubMed] [Google Scholar]
- Faulds R (2005). Kripalu yoga: A guide to practice on and off the mat. New York, NY: Bantam Dell. [Google Scholar]
- First MB, Spitzer R, Gibbon M, & Williams JB (1995). Structured clinical interview for DSM-IV Axis I disorders—Patient edition (SCID—I/P, version 2.0). New York, NY: New York State Psychiatric Institute. [Google Scholar]
- Flett GL, Nepon T, Hewitt PL, & Fitzgerald K (2016). Perfectionism, components of stress reactivity, and depressive symptoms. Journal of Psychopathology and Behavioral Assessment, 38, 645–654. [Google Scholar]
- Gaiswinkler L, & Unterrainer HF (2016). The relationship between yoga involvement, mindfulness and psychological well-being. Complementary Therapies in Medicine, 26, 123–127. [DOI] [PubMed] [Google Scholar]
- Gard T, Brach N, Hölzel BK, Noggle JJ, Conboy LA, & Lazar SW (2012). Effects of a yoga-based intervention for young adults on quality of life and perceived stress: the potential mediating roles of mindfulness and self-compassion. The Journal of Positive Psychology, 7, 165–175. [Google Scholar]
- Gard T, Noggle JJ, Park CL, Vago DR, & Wilson A (2014) Potential self-regulatory mechanisms of yoga for psychological health. Frontiers in Human Neuroscience, 8, 770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gerbarg PL, & Brown RP (2015). Yoga and neuronal pathways to enhance stress response, emotion regulation, bonding, and spirituality. In Horovitz EG & Elgelid S (Eds.), Yoga Therapy: Therapy and Practice (pp. 67–82). New York, NY: Routledge. [Google Scholar]
- Greenberg J, Braun TD, Schneider ML, Finkelstein-Fox L, Conboy LA, Schifano ED, Park CL, & Lazar SW (2018). Is less more? A randomized comparison of home practice in a mind-body program. Behavior Research & Therapy, 111, 52–56. doi: 10.1016/j.brat.2018.10.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goyal M, Singh S, Sibinga EM, Gould NF, Rowland-Seymour A, Sharma R, …Haythornthwaite JA (2014). Meditation programs for psychological stress and well-being: A systematic review and meta-analysis. JAMA Internal Medicine, 174, 357–368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haskell WL, Lee I-M, Pate RR, Powell KE, Blair SN, Franklin BA, … Bauman A (2007). Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Medicine and Science in Sports and Exercise, 39, 1423–1434. [DOI] [PubMed] [Google Scholar]
- Hofmann SG, Sawyer AT, Fang A, & Asnaani A (2012). Emotion dysregulation model of mood and anxiety disorders. Depression and Anxiety, 29, 409–416. doi: 10.1002/da.21888 [DOI] [PubMed] [Google Scholar]
- Iglesias SL, Azzara S, Argibay JC, Arnaiz ML, de Valle Carpineta M, Granchetti H, & Lagomarsino E (2012). Psychological and physiological response of students to different types of stress management programs. American Journal of Health Promotion, 26, 149–158. [DOI] [PubMed] [Google Scholar]
- Kinser PA, Goehler LE, & Taylor AG (2012). How might yoga help depression? A neurobiological perspective. Explore, 8, 118–126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindsay EK, Young S, Smyth JM, Brown KW, & Creswell JD (2018). Acceptance lowers stress reactivity: Dismantling mindfulness training in a randomized controlled trial. Psychoneuroendocrinology, 87, 63–73 [DOI] [PubMed] [Google Scholar]
- Lovibond PF, & Lovibond SH (1995). The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behavior Research and Therapy, 33, 335–343. [DOI] [PubMed] [Google Scholar]
- Mehling WE, Price C, Daubenmier JJ, Acree M, Bartmess E, & Stewart A (2012). The Multidimensional Assessment of Interoceptive Awareness (MAIA). PLoS One, 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mehling WE, Wrubel J, Daubenmier JJ, Price CJ, Kerr CE, Silow T, … & Stewart AL (2011). Body awareness: A phenomenological inquiry into the common ground of mind-body therapies. Philosophy, Ethics, and Humanities in Medicine, 6, 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mehling WE, Chesney MA, Metzler TJ, Goldstein LA, Maguen S, Geronimo C, … & Neylan TC (2018). A 12-week integrative exercise program improves self reported mindfulness and interoceptive awareness in war veterans with posttraumatic stress symptoms. Journal of Clinical Psychology, 74, 554–565. [DOI] [PubMed] [Google Scholar]
- Muscatell KA, & Eisenberger NI (2012). A social neuroscience perspective on stress and health. Social and Personality Psychology Compass, 6, 890–904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neff KD (2003). The development and validation of a scale to measure self-compassion. Self and Identity, 2, 223–250. [Google Scholar]
- Neff KD & Germer CK (2012). A pilot study and randomized controlled trial of mindful self-compassion program. Journal of Clinical Psychology, 69, 28–44. [DOI] [PubMed] [Google Scholar]
- Neukirch N, Reid S, & Shires A (2019). Yoga for PTSD and the role of interoceptive awareness: A preliminary mixed-methods case series study. European Journal of Trauma & Dissociation, 3, 7–15. [Google Scholar]
- Oken BS, Chamine I, & Wakeland W (2015). A systems approach to stress, stressors and resilience in humans. Behavioural Brain Research, 282, 144–154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Park CL, Elwy AR, Maiya M, Sarkin AJ, Riley KE, Eisen SV, Gutierrez IA, .. Groessl EJ (2018). The Essential Properties of Yoga Questionnaire (EPYQ): Psychometric properties. International Journal of Yoga Therapy, 28, 23–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Park CL, Finkelstein-Fox L, Groessl EJ, Lee SY, & Elwy AR (2020). Exploring how different types of yoga change psychological resources and emotional well-being across a single session. Complementary Therapies in Medicine, 49, 102354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Park CL, Groessl E, Maiya M, Sarkin A, Eisen S, Riley KE, & Elwy ER (2014). Comparison groups in yoga research: A systematic review and critical evaluation of the literature. Complementary Therapies in Medicine, 22, 920–929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Park CL, Riley KE, Braun TD, Jung JY, Suh HG, Pescatello LS, & Antoni MH (2017). Yoga and cognitive-behavioral interventions to reduce stress in incoming college students: A pilot study. Journal of Applied Biobehavioral Research, 22, e12068. [Google Scholar]
- Park CL, & Slattery JM (2013). Religion and emotional health and well-being. In Paloutzian RF & Park CL (Eds.), Handbook of the psychology of religion and spirituality, 2nd Edition (pp. 540–559). New York, NY: Guilford. [Google Scholar]
- Park CL, Wright BEW, Pais J, & Ray DM (2016). Reciprocal relations between daily stressful events and ego depletion: A smartphone-based experience sampling study. Journal of Social and Clinical Psychology, 35, 738–753. [Google Scholar]
- Pascoe MC, & Bauer IE (2015). A systematic review of randomised control trials on the effects of yoga on stress measures and mood. Journal of Psychiatric Research,, 68, 270–282. [DOI] [PubMed] [Google Scholar]
- Pascoe MC, Thompson DR, & Ski CF (2017). Yoga, mindfulness-based stress reduction and stress-related physiological measures: A meta-analysis. Psychoneuroendocrinology, 86, 152–168. [DOI] [PubMed] [Google Scholar]
- Paulhus DL, & Vazire S (2007). The self-report method. In Robins RW, Fraley RC, & Krueger R (Eds.), Handbook of research methods in personality psychology. 224–239. New York, NY: Guilford Press. [Google Scholar]
- Peterman AH, Fitchett G, Brady MJ, Hernandez L, & Cella D (2002). Measuring spiritual well-being in people with cancer: The Functional Assessment of Chronic Illness Therapy--Spiritual Well-being Scale (FACIT-Sp). Annals of Behavioral Medicine, 24, 49–58. [DOI] [PubMed] [Google Scholar]
- Ramadoss R, & Bose B (2010). Transformative life skills: Pilot study of a yoga model for reduced stress and improving self-control in vulnerable youth. International Journal of Yoga Therapy, 20, 73–78. [Google Scholar]
- Raes F, Pommier E, Neff KD, & Van Gucht D (2011). Construction and factorial validation of a short form of the Self-Compassion Scale. Clinical Psycology and Psychotherapy, 18, 250–255. [DOI] [PubMed] [Google Scholar]
- Riley KE, & Park CL (2015). How does yoga reduce stress? A systematic review of mechanisms of change and a guide to future inquiry. Health Psychology Review, 9, 379–396. [DOI] [PubMed] [Google Scholar]
- Sheehan D, Lecrubier Y, Sheehan H, Amorim P, Janavs J, Weiller E, … Dunbar G (1998). The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. Journal of Clinical Psychiatry, 59, 22–23. [PubMed] [Google Scholar]
- Streeter CC, Gerbarg PL, Saper RB, Ciraulo DA, & Brown RP (2012). Effects of yoga on the autonomic nervous system, gamma-aminobutyric-acid, and allostasis in epilepsy, depression, and post-traumatic stress disorder. Medical Hypotheses, 78, 571–579. [DOI] [PubMed] [Google Scholar]
- Tangney JP, Baumeister RF, & Boone AL (2004). High self-control predicts good adjustment, less pathology, better grades, and interpersonal success. Journal of Personality, 72, 271–324. [DOI] [PubMed] [Google Scholar]
- Wieland LS, Skoetz N, Pilkington K, Vempati R, D’Adamo CR, & Berman BM (2017). Yoga treatment for chronic non-specific low back pain. Cochrane Database of Systematic Reviews. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woda A, Picard P, & Dutheil F (2016). Dysfunctional stress responses in chronic pain. Psychoneuroendocrinology, 71, 127–135. [DOI] [PubMed] [Google Scholar]