

SUMMARY
Benign baroxysmal positional vertigo (BPPV) represents the most common peripheral vestibular dysfunction encountered in clinical practice. Although canalith repositioning procedures (CRPs) are a relatively successful treatment for BPPV, many patients suffer from recurrences. Several studies have demonstrated that various pathological conditions (diabetes, hypertension, endolymphatic hydrops, low vitamin D levels) as well as delayed BPPV treatment using CRP, multiple canal involvement may be associated with recurrence of BPPV. We evaluated the history of 1,428 patients (558 males and 870 females, age range 10-92 years) suffering from BPPV. Of 1,428 cases, 820 (77%) did not relapse in the following 20 years. Mean age and gender did not differ significantly between groups with and without recurrence. Regarding risk factors for BPPV recurrence, age, female gender, migraine, hypertension, diabetes mellitus, hyperlipidaemia, osteoporosis, vascular diseases, and vitamin D deficiency may be associated with recurrent BPPV and should be kept in mind. Osteoporosis, vitamin D deficiency as well as thyroid dysfunction should be evaluated in postmenopausal women. Treatment of these comorbidities may help to reduce the risk of BPPV recurrence.
KEY WORDS: dizziness, vertigo, benign paroxysmal positional vertigo, risk factors
RIASSUNTO
Sono stati presi in considerazione 1.428 soggetti osservati, dal primo gennaio 1996 al 31 dicembre 2000, con diagnosi di vertigine parossistica posizionale. Scopo del lavoro era di verificare il numero di recidive manifestatesi nei venti anni successivi al primo episodio vertiginoso confermato clinicamente. A questo scopo sono state controllate cartelle cliniche di ogni paziente. Su 1.428 casi (corrispondenti a 1.067 pazienti alcuni dei quali avevano avuto più di un episodio) diagnosticati quasi il 77% dei pazienti (820/1.067) non è recidivato e meno del 17% dei pazienti (180/1.067) ha presentato una sola ripresa della sintomatologia vertiginosa. Inoltre solo in 67 casi su 1.067 (poco più del 6% dei casi) si assiste a più di due recidive. La vertigine parossistica posizionale da canalolitiasi è una affezione che tende a recidivare. Le reali recidive però sembrano meno di quelle che ci si può aspettare e sembra che una profilassi farmacologica sia consigliabile solo nei pazienti con tendenza ad un numero elevato di recidive od in pazienti da valutare caso per caso. Nella quasi totalità dei pazienti sembra preferibile alla profilassi farmacologica l’esecuzione delle manovre al momento della recidiva.
PAROLE CHIAVE: vertigine parossistica posizionale benigna, dizziness, recidiva, fattori di rischio
Introduction
Benign paroxysmal positional vertigo (BPPV) is the most common peripheral vestibular dysfunction encountered in clinical practice, with a reported 1-year prevalence of 1.6% and a lifetime prevalence of 2.4% 1. BPPV is characterised by recurrent episodes of vertigo with corresponding nystagmus, generally provoked by changes in head position. BPPV accounts for 25% of all cases of vertigo that come to the attention of clinicians and can affect all ages, although it can be underdiagnosed in the elderly; the most affected age group is the fifth and sixth decade 2. Women are affected twice as often as men 3. Some studies also found that patients with BPPV were at increased risk of falls, fractures, hypertension and dementia 4-7. In addition, BPPV may cause physical and psychological distress during episodes of vertigo. Therefore, BPPV severely decreases patients’ quality of life and impairs the performance of daily activities 8. BPPV is thought to be the clinical expression of otoconial particles of utricular origin migrating into the lumen of a semicircular canal. For reasons of spatial arrangement, the gravitational field favours dislocation in the posterior and lateral semicircular canal 2,3. The possibility of migration into the anterior canal 9, which is rare and could be confused with a posterior canalolithiasis with a non-ampullary location 10, is more difficult and still debated. In most patients suffering from BPPV, there is no evident cause. In some cases, BPPV resolves spontaneously within a few weeks 11 with a slow and gradual resolution of vertigo 12. Post-traumatic causes of BPPV include whiplash injury, high-impact exercise and surgical procedures 3,13. Other conditions predisposing to the detachment of otoconia from utricular maculae are viral, ischaemic, or hydropic disorders involving the inner ear 3,14,15, migraine 16 and a prolonged recumbent position 17. Other risk factors for BPPV include female gender, age over 60 years, osteoporosis, hypertension and non-apnoea sleep disorders 2,3,18-21.
Currently, although canalith repositioning procedures (CRPs) are a relatively successful treatment for BPPV 2,3, many patients suffer from repeated episodes of BPPV, with a reported recurrence rate of approximately 50% during 10-year follow-up 22,23. Similarly, it was reported that 10% to 18% patients relapse during a 1-year follow-up period 24. In addition, a recent meta-analysis suggested that many risk factors related to the recurrence of BPPV may also be risk factors for its occurrence 25. The frequent recurrence of BPPV may cause great inconvenience in the daily life of BPPV patients. The aim of this paper is to evaluate the long-term tendency for recurrence of BPPV.
Materials and methods
For short-term evaluation (weeks), patients could undergo direct clinical follow-up, but for our purposes this is not sufficient. Considering that our patients could directly address our centre in cases of recurrence, we choose to retrospectively examine how many times patients came to us because for a new onset of positional vertigo.
This method does not exclude various critical issues:
the patient does not return to control visits;
the patient goes to another healthcare facility;
the patient, after many years, is no longer able to return (more serious illnesses, disability, death, etc.).
Point 1 seems very unlikely, and anyone familiar with this type of vertigo can agree on this point.
Point 2 is possible but unlikely, since the patient has a preferential access route to the facility (no waiting lists, limited or no expense). Experience tells us that the reverse case is much more likely, i.e. that patients return even if they do not have a recurrence of BPPV.
Point 3 obviously cannot be excluded, but it is a bias that is impossible to eliminate over long follow-up periods. The case of death is not taken into consideration because the study evaluates recurrences during life.
Finally, the repeated access retrospective study seems the most reliable way to get an idea of long-term relapses, which is what was adopted.
In the period from January 1996 - December 2000 we evaluated 6,104 patients (2,622 males and 3,482 females) complaining of vertigo and/or dizziness. From this group of patients, we selected 1,067 subjects affected by BPPV (558 males and 870 females) who were followed for 20 years. Clinical data were obtained from our records. All patients found in our clinical records were included if they fulfilled criteria for single or multiple canal BPPV 2,3. In 1,119 (78.4%) cases a posterior semicircular canal BPPV was found, and 309 (21.6%) patients resulted to be affected by horizontal semicircular canal BPPV (in 286 patients, 92.6%, ageotropic and in 34, 7.4%, apogeotropic). All patients were treated with a Semont or Epley manoeuver (in case of posterior semicircular canal BPPV) or Gufoni manoeuver followed by the Forced Prolonged Position (in case of horizontal semicircular canal BPPV). Patients were instructed to return to our vestibular unit in the event of a recurrence of symptoms to control for the presence of BPPV and to repeat the CRP.
Results
Of 1,067 patients diagnosed with BPPV, 820 (76.85%) did not show any recurrence in the following 20 years, 180 (16.87%) patients had one relapse, 41 (3.84%) had two relapses, 16 (1.5%) had three relapses, 4 patients 4 (0.37%) relapses, 4 (0.37%) patients five relapses, one patient (0.09%) and six relapses. In one patient, 9 recurrences after the first episode were seen in the following 20 years (Fig. 1). Furthermore, we evaluated if age and sex influenced the incidence of recurrence of BPPV. Having in mind the number of recurrences, we evaluated the mean age of patients (Fig. 2) and the relative differences between males and females (Fig. 3). There were no significant differences in either case.
Figure 1.
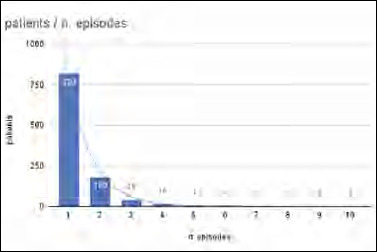
Distribution of the number of recurrencies in 1,067 patients diagnosed with BPPV during 1996-2020. The majority of patients showed no more than 2 recurrences in the 20 years following the onset of the first episode of BPPV.
Figure 2.
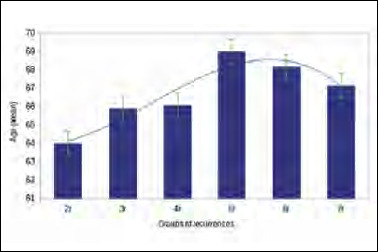
Mean age of the patients affected by recurrent BPPV distributed by the number of recurrences (r: recurrences). The patients with more than 4 recurrences showed an age > 65 years, with no statistical significance.
Figure 3.
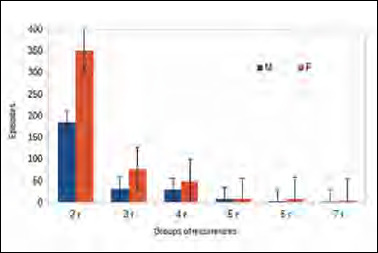
Sex distribution based on of the number of recurrences of BPPV (r: recurrences). Although recurrences are more frequent in women in any group, no significant difference was found.
Discussion
Two stages are required for the paroxysmal positional vertigo to be triggered:
the detachment of otoliths in a quantity able to induce positional vertigo;
their migration within a semicircular canal.
Each of these two moments is necessary: if the detached otoliths will not migrate in the semicircular canal, we can speculate about the existence of an abnormal macular activity leading to a disequilibrium, but not causing the positional vertigo.
Although it was revealed that more than 95% of cases can be cured by a canalith repositioning manoeuver (CRM), in some cases BPPV resolves spontaneously within a few weeks 11 with a slow and gradual resolution of vertigo probably due to a progressive dissolution (quickly or slowly, depending on the state of aggregation) in the endolymph of the dislodged otoliths 12. Consequently, the nystagmus evoked by the positioning manoeuver tends to decrease in intensity and the symptoms can change from a true rotatory positional vertigo to a sense of imbalance and instability evoked by assuming the provocative position.
Recurrent BPPV was defined as the reappearance of paroxysmal positional nystagmus after at least 2 weeks from the execution of CRM: in our opinion, it is necessary to be aware that recurrences can be of two types:
the detached otoliths return into the utricule (spontaneously or by the effect of CRM) where they may remain for a period undergoing dissolution; on the contrary, this material can again move to the semicircular canal. In the latter case this is not considered as a recurrence, because the actual symptom is caused by the same debris;
caused by a new detachment of otoliths.
In the first case, the recurrence occurs shortly after the first episode (no more than 6 to 8 weeks) given the time assumed for reabsorption of the fragments and the recurrence occurs in the same ear even if not in the same semicircular canal. Usually the patient reports that the second episode is less intense than the first. This is reasonable if we consider that resorption has occurred in the meantime, which made the fragments “lighter” and therefore giving less intense vertigo (Fig. 4).
Figure 4.
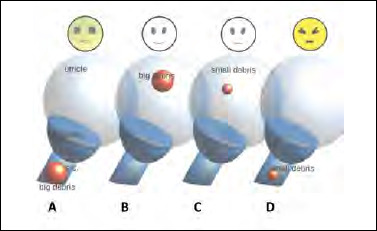
The recurrence of BPPV is caused by the same (large) debris returning to the semicircular canal (s.c.); in this case, the positional attack of vertigo occurs on the same side, no more than 6 to 8 weeks after the first episode (A-B). If the same debris re-enters the semicircular canal it induces less intense symptoms because the mass became smaller due to its partial reabsorption (C-D).
The probability of fragments moving into a critical zone must be directly proportional to the available otolithic mass: the greater the size of the mass, the greater the probability that a portion will move over time causing a recurrence of BPPV.
Consequently:

the quantity Q of otolithic fragments available for migration varies (decreases) as a function of time and is proportional, according to the constant k, to the residual mass.
Solving the differential equation:

The quantity Q of otolithic fragments available for migration at time t is dependent on the initial available mass Q0 of free otoliths, Q(t) is the quantity of fragments present at time t, k is a variable that influences the resorption time and thus in practice the duration of the disease: the higher the k coefficient (the patient moves, or exercises, or is less blocked by vertigo), the sooner the patient becomes symptom-free (Fig. 5).
Figure 5.
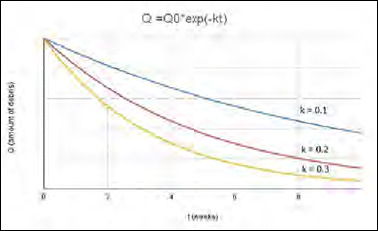
The recurrence of BPPV is influenced by the dimension of the otolithic mass (Q). The likelihood of recurrence is greater as the mass increases in size, which however decreases over time based on mobilisation (spontaneous or induced by CRM). The higher k (the variable influencing the reabsorption time) the more the patient moves and the sooner the patient recovers.
Several studies have demonstrated that various pathological conditions (diabetes, hypertension, endolymphatic hydrops, low vitamin D levels) as well as delayed BPPV treatment using CRM and multiple canal involvement may be associated with the recurrence of BPPV 25-29. Furthermore, the recurrence of BPPV is more frequent in patients affected by multiple, associated diseases 30. However, the evidence reported in the literature is conflicting. For example, some studies showed no correlation between gender, age and recurrent BPPV 31, while other studies reported that age and gender are related to recurrent BPPV 1,32. In our experience, we did not find a significant increase of the recurrence of BPPV in older patients, while regarding sex we noticed a higher incidence in females, without however reaching statistical significance.
BPPV tends to recur over time, but our data seem to indicate that the chances of a recurrent episode are less frequent than reported in the literature 22,23. Less than half of patients showed a recurrence and more than two-thirds of patients experienced only one episode of recurrence over 20 years. In our series, only 26 of 1,067 patients (just over 2%) presented with more than three episodes of paroxysmal positional vertigo in 20 years. On the other hand, there are only isolated cases of patients showing a great tendency to suffer from recurrent BPPV: in one case 10 recurrences of vertigo were observed, and in 5 cases at least 6 episodes. These patients experienced a great decrease in quality of life, especially taking in consideration that BPPV does not only affect the elderly, but often also during active life. Our results are in line with a recent study in which the recurrence rate was 22% at 5 years after initial treatment and about 70% of recurred patients had a relapse within 1 year 33.
Regarding the evaluation of risk factors for BPPV recurrence, two recent meta-analyses indicated that age (> 65 years), female gender, migraine, hypertension, diabetes mellitus, hyperlipidaemia, osteoporosis and vitamin D deficiency may be associated with recurrent BPPV 25,34. Vascular damage, ischaemia, or atherosclerosis induced by vascular comorbidities may cause displacement or degenerative changes of otoconia 35,36, which may explain why vascular comorbidities have adverse effects on BPPV 19. The pooled results of the above-mentioned meta-analyses showed that hypertension, diabetes mellitus and hyperlipidaemia may increase the risk of BPPV recurrence. Therefore, vascular comorbidities should be actively treated to eliminate potentially vascular risk factors for BPPV recurrence, which may help reduce the recurrence rate and improve te prognosis. Unfortunately, there is no consensus in the literature about the relevance of risk factors involved in the recurrence of BPPV. For example, a large single-institution study of recurrence in BPPV indicated female sex and history of previous BPPV as risk factors associated with an increased rate of recurrence, while no association with Menière’s disease, diabetes mellitus, or traumatic aetiology was found 37.
Regarding vitamin D deficiency, a previous meta-analysis demonstrated that it was an independent risk factor for BPPV occurrence and recurrence 38; this correlation may be explained by the fact that vitamin D deficiency may disrupt calcium metabolism in the inner lymphatic fluid and bone metabolism, leading to osteoporosis and increasing the risk of BPPV 39. A recent multicentric study suggested that oral nutritional supplementation with vitamin D3 may prevent relapses in patients suffering from a high number of recurrent episodes of BPPV 40. Further large-scale studies are necessary to establish the role of vitamin D supplementation in prevention of BPPV recurrence.
Migraine is reported to be a risk factor for BPPV recurrence 41,42. Migraine and BPPV are among the most frequently encountered diseases in otoneurological clinics. It is likely that patients with migraine have recurrent damage to the inner ear (due to vasospasm or some other mechanism) that predisposes them to recurrent episodes of BPPV. However, a recent meta-analysis found no significant association between migraine and the recurrence of BPPV, probably due to significant heterogeneity and the small number of included studies 25,34. Recently, the association between hypothyroidism and BPPV has been investigated 43,44. Another study demonstrated that patients with hypothyroidism treated with hormone replacement therapy have an increased risk of BPPV recurrence, which is particularly strong for patients with Hashimoto’s thyroiditis and positive thyroid antibodies, suggesting an association between autoimmunity and recurrent BPPV, and thus the importance of investigating thyroid dysfunction 45.
Conclusions
In case of recurrent BPPV, we recommend that careful medical history should be taken especially regarding cardiovascular comorbidities (hyperlipidaemia and hypertension), as well as the presence of diabetes mellitus. Good control of these comorbidities should always be maintained in these patients. In addition, osteoporosis, and vitamin D deficiency as well as thyroid dysfunction should be evaluated especially in postmenopausal women with recurrent episodes of BPPV 46. Therefore, treatment of these comorbidities may contribute to reducing the risk of BPPV recurrence, thereby improving prognosis. On the other hand, identification of these risk factors provides some insight into risk evaluation for falls and contributes to help clinicians counsel patients regarding the importance of follow-up after diagnosis of BPPV. Furthermore, considering the frequency of long-term recurrences, in most cases therapy with liberating manoeuvers seems sufficient, limiting preventive drug therapy to single selected cases. Our experience regarding the recurrence of BPPV, despite the large number of patients, does not provide definitive results about the role of some described risk factors. We evaluated only limited data (age, sex) resulting from the clinical records, thus limiting the scientific significance of our paper, which was mainly designed as a mini review about recurring BPPV. A large prospective multicentre study should be carried out to better evaluate risk factors that can potentially affect the recurrence of BPPV.
Conflict of interest statement
The authors declare no conflict of interest.
Author contributions
APC: conceptualisation, writing – review and editing and supervision; MG, APC: methodology, formal analysis, investigation, writing – original draft preparation.
All authors have read and agreed to the published version of the manuscript.
Ethical consideration
Due to the retrospective nature of this observational study (not considered as part of a research project) it did not require approvals of Ethics Committee. Furthermore, the study does not include new invasive or experimental procedures or diagnostic protocol; all patients underwent routinely performed tests only, according to national guidelines. Informed consent was obtained from all participants and the study was performed in accordance with the Declaration of Helsinki.
Figures and tables
Funding Statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- 1.Von Brevern M, Radtke A, Lezius F, et al. Epidemiology of benign paroxysmal positional vertigo: a population-based study. J Neurol Neurosurg Psych 2007;78:710-715. https://doi.org/10.1136/jnnp.2006.10042 10.1136/jnnp.2006.10042 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kim JS, Zee DS. Clinical practice. Benign paroxysmal positional vertigo. N Engl J Med 2014;370:1138-1147. https://doi.org/10.1056/NEJMcp1309481 10.1056/NEJMcp1309481 [DOI] [PubMed] [Google Scholar]
- 3.Nuti D, Zee DS, Mandalà M. Benign paroxysmal positional vertigo: what we do and do not know. Semin Neurol 2020;40:49-58. https://doi.org/10.1055/s-0039-3402733 10.1055/s-0039-3402733 [DOI] [PubMed] [Google Scholar]
- 4.Kao CL, Cheng YY, Leu HB, et al. Increased risk of ischemic stroke in patients with benign paroxysmal positional vertigo: a 9-year follow-up nationwide population study in Taiwan. Front Aging Neurosci 2014;6:108. https://doi.org/10.3389/fnagi.2014.00108 10.3389/fnagi.2014.00108 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Liao WL, Chang TP, Chen HJ, et al. Benign paroxysmal positional vertigo is associated with an increased risk of fracture: a population-based cohort study. J Orthop Sports Phys Ther 2015;45:406412. https://doi.org/10.2519/jospt.2015.5707 10.2519/jospt.2015.5707 [DOI] [PubMed] [Google Scholar]
- 6.De Stefano A, Dispenza F, Suarez H, et al. A multicenter observational study on the role of comorbidities in the recurrent episodes of benign paroxysmal positional vertigo. Auris Nasus Larynx 2014;41:31-36. https://doi.org/10.1016/j.anl.2013.07.007 10.1016/j.anl.2013.07.007 [DOI] [PubMed] [Google Scholar]
- 7.Kim SY, Yoo DM, Min C, et al. Increased risk of neurodegenerative dementia after benign paroxysmal positional vertigo. Int J Environ Res Public Health 2021;18:10553 https://doi.org/10.3390/ijerph181910553 10.3390/ijerph181910553 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lopez-Escamez JA, Gamiz MJ, Fernandez-Perez A, et al. Long-term outcome and health-related quality of life in benign paroxysmal positional vertigo. Eur Arch Otorhinolaryngol 2005;262:507-511. https://doi.org/10.1007/s00405-004-0841-x 10.1007/s00405-004-0841-x [DOI] [PubMed] [Google Scholar]
- 9.Casani AP, Cerchiai N, Dallan I, et al. Anterior canal lithiasis: diagnosis and treatment. Otolaryngol Head Neck Surg 2011;144:412-418. https://doi.org/10.1177/0194599810393879 10.1177/0194599810393879 [DOI] [PubMed] [Google Scholar]
- 10.Vannucchi P, Pecci R, Giannoni B. Posterior semicircular canal benign paroxysmal positional vertigo presenting with torsional down-beating nystagmus: a apogeotropic variant. Int J Otolaryngol 2012;2012:413603. https://doi.org/10.1155/2012/413603 10.1155/2012/413603 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Álvarez-Morujo de Sande MG, González-Aguado R, Guerra-Jiménez G, et al. Probable benign paroxysmal positional vertigo, spontaneously resolved: incidence in medical practice, patients’ characteristics and the natural course. J Otol 2019;14:111-116. https://doi.org/10.1016/j.joto.2019.04.002 10.1016/j.joto.2019.04.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zucca G, Valli S, Valli P, et al. Why do benign paroxysmal positional vertigo episodes recover spontaneously? J Vestib Res 1998;8:325-329. [PubMed] [Google Scholar]
- 13.Andersson H, Jablonski GE, Nordahl SHG. The risk of benign paroxysmal positional vertigo after head trauma. Laryngoscope 2022;132:443-448. https://doi.org/10.1002/lary.29851 10.1002/lary.29851 [DOI] [PubMed] [Google Scholar]
- 14.Kutlubaev AM, Ying Xu, Hornibrook J. Benign paroxysmal positional vertigo in Meniere’s disease: systematic review and meta-analysis of frequency and clinical characteristics. J Neurol 2021;268:1608-1614. https://doi.org/10.1007/s00415-019-09502 10.1007/s00415-019-09502 [DOI] [PubMed] [Google Scholar]
- 15.Balatsouras DG, Koukoutsis G, Ganelis P, et al. Benign paroxysmal positional vertigo secondary to vestibular neuritis. Eur Arch Otorhinolaryngol 2014;271:919-924. https://doi.org/10.1007/s00405-013-2484-2 10.1007/s00405-013-2484-2 [DOI] [PubMed] [Google Scholar]
- 16.Bruss D, Abouzari M, Sarna B, et al. Migraine features in patients with recurrent benign paroxysmal positional vertigo. Otol Neurotol 2021;42:461-465. https://doi.org/10.1097/MAO.0000000000002976 10.1097/MAO.0000000000002976 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fu CY, Zhang ZZ, Chen J, et al. Unhealthy lifestyle is an important risk factor of idiopathic BPPV. Front Neurol 2020;11:950. https://doi.org/10.3389/fneur.2020.00950 10.3389/fneur.2020.00950 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Shih CP, Wang CH, Chung CH, et al. Increased risk of benign paroxysmal positional vertigo in patients with non-apnea sleep disorders: a nationwide, population-based cohort study. J Clin Sleep Med 2018;14:20212029. https://doi.org/10.5664/jcsm.7528 10.5664/jcsm.7528 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sreenivas V, Sima NH, Philip S. The role of comorbidities in benign paroxysmal positional vertigo. Ear Nose Throat J 2021;100:NP225-NP230. https://doi.org/10.1177/0145561319878546 10.1177/0145561319878546 [DOI] [PubMed] [Google Scholar]
- 20.Abdelmaksoud AA, Fahim DFM, Bazeed SES, et al. Relation between vitamin D deficiency and benign paroxysmal positional vertigo. Sci Rep 2021;11:16855. https://doi.org/10.1038/s41598-021-96445-x 10.1038/s41598-021-96445-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Neri G, Filograna Pignatelli GR, Pacella A, et al. Recurring paroxysmal positional vertigo: evaluation of the vascular factor. Acta Otorhinolaryngol Ital 2021;41:77-83. https://doi.org/10.14639/0392-100x-n0502 10.14639/0392-100x-n0502 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Nunez RA, Cass SP, Furman JM. Short- and long-term outcomes of canalith repositioning for benign paroxysmal positional vertigo. Otolaryngol Neck Surg 2000;122:647-653. https://doi.org/10.1016/S0194-5998(00)70190-2 10.1016/S0194-5998(00)70190-2 [DOI] [PubMed] [Google Scholar]
- 23.Brandt T, Huppert D, Hecht J, et al. Benign paroxysmal positioning vertigo: a long-term follow-up (6-17 years) of 125 patients. Acta Otolaryngol 2006;126:160-163. https://doi.org/10.1080/00016480500280140 10.1080/00016480500280140 [DOI] [PubMed] [Google Scholar]
- 24.Sakaida M, Takeuchi K, Ishinaga H, et al. Long-term outcome of benign paroxysmal positional vertigo. Neurology 2003;60:1532-1534. https://doi.org/10.1212/01.wnl.0000061477.03862.4d 10.1212/01.wnl.0000061477.03862.4d [DOI] [PubMed] [Google Scholar]
- 25.Chen J, Zhang S, Cui K, et al. Risk factors for benign paroxysmal positional vertigo recurrence: a systematic review and meta-analysis. J Neurol 2020;268:4117-4127. https://doi.org/10.1007/s0041 5-020-10175-0 10.1007/s00415-020-10175-0 [DOI] [PubMed] [Google Scholar]
- 26.Choi SJ, Lee JB, Lim HJ, et al. Clinical features of recurrent or persistent benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg 2012;147:919-924. https://doi.org/10.1177/0194599812454642. 10.1177/0194599812454642 Corrigendum. Otolaryngol Head Neck Surg 2013;149:798. https://doi.org/10.1177/0194599813505840 [DOI] [PubMed] [Google Scholar]
- 27.Kim SY, Han SH, Kim YH, et al. Clinical features of recurrence and osteoporotic changes in benign paroxysmal positional vertigo. Auris Nasus Larynx 2017;44:156-161. https://doi.org/10.1016/j.anl.2016.06.006 10.1016/j.anl.2016.06.006 [DOI] [PubMed] [Google Scholar]
- 28.Perez P, Franco V, Cuesta P, et al. Recurrence of benign paroxysmal positional vertigo. Otol Neurotol 2012;33:437-443. https://doi.org/10.1097/MAO.0b013e3182487f78 10.1097/MAO.0b013e3182487f78 [DOI] [PubMed] [Google Scholar]
- 29.Tanimoto H, Doi K, Nishikawa T, et al. Risk factors for recurrence of benign paroxysmal positional vertigo. J Otolaryngol Head Neck Surg 2008;37:832-835. [PubMed] [Google Scholar]
- 30.Picciotti PM, Lucidi D, De Corso E, et al. Comorbidities and recurrence of benign paroxysmal positional vertigo: personal experience. Int J Audiol 2016;55:279-284. https://doi.org/10.3109/14992027.2016.1143981 10.3109/14992027.2016.1143981 [DOI] [PubMed] [Google Scholar]
- 31.Yeo SC, Ahn SK, Lee HJ, et al. Idiopathic benign paroxysmal positional vertigo in the elderly: a long-term follow-up study. Aging Clin Exp Res 2018;30:153-159. https://doi.org/10.1007/s40520-017-0763-2 10.1007/s40520-017-0763-2 [DOI] [PubMed] [Google Scholar]
- 32.Chau AT, Menant JC, Hübner PP, et al. Prevalence of vestibular disorder in older people who experience dizziness. Front Neurol 2015;6:268. https://doi.org/10.3389/fneur.2015.00268 10.3389/fneur.2015.00268 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kong TH, Song MH, Shim DB. Recurrence rate and risk factors of recurrence in benign paroxysmal positional vertigo: a single-center long-term prospective study with a large cohort. Ear Hear 2021;43:234-241. https://doi.org/10.1097/AUD.0000000000001093 10.1097/AUD.0000000000001093 [DOI] [PubMed] [Google Scholar]
- 34.Li S, Wang Z, Liu Y, et al. Risk factors for the recurrence of benign paroxysmal positional vertigo: a systematic review and meta-analysis. Ear Nose Throat J 2022;101:N112-N134. https://doi.org/10.1177/0145561320943362 10.1177/0145561320943362 [DOI] [PubMed] [Google Scholar]
- 35.D’Silva LJ, Staecker H, Lin J, et al. Retrospective data suggests that the higher prevalence of benign paroxysmal positional vertigo in individuals with type 2 diabetes is mediated by hypertension. J Vestib Res 2016;25:233-239. https://doi.org/10.3233/VES-150563 10.3233/VES-150563 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Cohen HS, Kimball KT, Stewart MG. Benign paroxysmal positional vertigo and comorbid conditions. ORL J Otorhinolaryngol Relat Spec 2004;66:11-15. https://doi.org/10.1159/000077227 10.1159/000077227 [DOI] [PubMed] [Google Scholar]
- 37.Luryi AL, Lawrence J, Bojrab DI, et al. Recurrence in benign paroxysmal positional vertigo: a large, single-institution study. Otol Neurotol 2018;39:622-627. https://doi.org/10.1097/mao.0000000000001800 10.1097/mao.0000000000001800 [DOI] [PubMed] [Google Scholar]
- 38.Yang X, Yang B, Wu M, et al. Association between serum uric acid levels and benign paroxysmal positional vertigo: a systematic review and meta-analysis of observational studies. Front Neurol 2019;10:91. https://doi.org/10.3389/fneur.2019.00091 10.3389/fneur.2019.00091 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Minasyan A, Keisala T, Zou J, et al. Vestibular dysfunction in vitamin D receptor mutant mice. J Steroid Biochem Mol Biol 2009;114:161-166. https://doi.org/10.1016/j.jsbmb.2009.01.020 10.1016/j.jsbmb.2009.01.020 [DOI] [PubMed] [Google Scholar]
- 40.Asprella Libonati GA, Leone A, Martellucci S, et al. Prevention of recurrent benign paroxysmal positional vertigo: the role of combined supplementation with vitamin D and antioxidants. Audiol Res 2022;12:445-456. https://doi.org/10.3390/audiolres12040045 10.3390/audiolres12040045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ishiyama A, Jacobson KM, Baloh RW. Migraine and benign positional vertigo. Ann Otol Rhinol Laryngol 2000;109:377-380. https://doi.org/10.1177/000348940010900407 10.1177/000348940010900407 [DOI] [PubMed] [Google Scholar]
- 42.Hilton DB, Luryi AL, Bojrab DI, et al. Comparison of associated comorbid conditions in patients with benign paroxysmal positional vertigo with or without migraine history: a large single institution study. Am J Otolaryngol 2020;41:102650. https://doi.org/10.1016/j.amjoto.2020.102650 10.1016/j.amjoto.2020.102650 [DOI] [PubMed] [Google Scholar]
- 43.Choi HG, Song YS, Wee JH, et al. Analyses of the relation between BPPV and thyroid diseases: a nested case-control study. Diagnostics 2021;11:329. https://doi.org/10.3390/diagnostics11020329 10.3390/diagnostics11020329 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Messina A, Casani AP, Manfrin M, et al. Italian survey on benign paroxysmal positional vertigo. Survey italiana sulla vertigine parossistica posizionale. Acta Otorhinolaryngol Ital 2017;37:328-335. https://doi.org/10.14639/0392-100X-1122 10.14639/0392-100X-1122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Tricarico L, Di Cesare T, Galli J, et al. Benign paroxysmal positional vertigo: is hypothyroidism a risk factor for recurrence? Acta Otorhinolaryngol Ital 2022;42:465-470. https://doi.org/10.14639/0392-100X-N1775 10.14639/0392-100X-N1775 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Sfakianaki I, Binos P, Karkos P, et al. Risk factors for recurrence of benign paroxysmal positional vertigo. a clinical review. J Clin Med 2021;10:4372. https://doi.org/10.3390/ jcm10194372 10.3390/jcm10194372 [DOI] [PMC free article] [PubMed] [Google Scholar]