

Abstract
Background
Life expectancy is one of the key indicators for investigating the overall health status of a population. Thus, analyzing the trend of this demographic measure is of great importance for planning health and social services in different societies. In this study, we aimed to model the trends of life expectancy in Asia, regions of Asia, and Iran over the past six decades.
Methods
The annual life expectancy at birth data sets were extracted for Iran and the total Asia population between 1960 and 2020 from the database provided by the Our World in Data website. The trend analysis was performed using the joinpoint regression model.
Results
During the study period, Iranians and Asians have, respectively, experienced about 32 and 28.6 years increase in life expectancy. The results from joinpoint regression showed that the average annual percent change (AAPC) of life expectancy was positive for all regions of Asia, and ranged from 0.4% for Central Asia to 0.9% for Southern Asia. In addition, the estimated AAPC in Iranian people was about 0.1 higher than the total Asian population (0.9% vs. 0.8%).
Conclusion
Despite protracted wars, poverty, and social inequality in some parts of Asia, life expectancy has drastically increased in this continent over the last decades. However, life expectancy in Asia (and Iran) is still remarkably lower than in more developed parts of the world. To elevate life expectancy to a higher level, the policymakers in Asian countries should put more effort into improving the standards of living and access to health facilities in their societies.
Keywords: Life expectancy, Asia, Regions of Asia, Iran, Trend analysis
↑What is “already known” in this topic:
The national, regional, and global trend of life expectancy has been investigated in some previously published articles by other researchers. These articles have generally used simple descriptive statistics and graphical approaches for exploring the pattern of change in life expectancy during the period under study.
→What this article adds:
In this study, we applied inferential statistical techniques to capture the pattern of change and model the behavior of trend of life expectancy in Asia, regions of Asia, and Iran over a quite long period of time.
Introduction
Life expectancy (LE) is one of the most important measures for assessing health status in different populations. It estimates the average number of additional years that an individual of a given age is expected to live. Life expectancy at birth (LEB) is the most commonly used metric, which is defined as the average number of years a newborn is expected to live if the current age-specific mortality rates at the time of its birth do not change in the upcoming years (1). Recent reports show that the average LEB has doubled in the entire world since the beginning of the twentieth century (2). In addition, the World Health Organization (WHO) reports show about a 10% increase in the average LEB in the last two decades (from 66.8 years in 2000 to 73.4 years in 2019) (3).
Life expectancy in a population is related to its socioeconomic condition, level of public health, and healthcare resources (4). Regarding these influential factors, there are still remarkable disparities across and even within the world countries. According to the estimates in 2020, the average LEB was 79 years for males and 82 years for females in developed countries, while males and females had an average LEB of 69 and 73 in less developed territories, respectively (5). The reported estimates by the World Bank reveal a significant gap between different world regions based on the average LEB. For instance, countries in Sub-Saharan Africa had an average LEB of 62 years in 2019, while an average LEB of 81 years was reported for countries in the European Union region in the same year. Among the world countries, the lowest LEB estimates were reported for some African nations with an estimated LEB of less than 55 years in 2019. In contrast, the highest LEB values were related to some high-income countries such as Hong Kong and Japan (about 85 years) in this year (6). Apparently, there was an estimated gap of about 30 years in LEB between more developed countries and those in poorer areas of the world.
Previously, many researchers investigated the trend of life expectancy and its determinants over the past few decades in our country, Iran. These studies have generally focused on different time intervals after the Islamic Revolution in 1979, and all of them indicated an upward trend of life expectancy due to improvements in healthcare access and quality, literacy rate, and socioeconomic status (7-9). However, in our literature review, we found no published article about statistical modeling and comparing the long-term patterns of life expectancy in Iran, Asian regions and the total Asia continent. Regarding this, the novelty of the present research lies in achieving two main goals; first, to model the long-term trends of LEB in different regions of Asia and the total Asian population, and second, to compare the trend of LEB in Iran with the total Asia population in the period 1960-2020. In this context, we used convenient statistical modeling approaches to highlight the discrepancies between the trends of LEB in Iran and total Asia in the described time interval.
Methods
Life expectancy at birth and data sources
In practice, there are two common methods for calculating life expectancy for different populations, which lead to cohort and period life expectancy. While the cohort life expectancy is generally calculated based on following a cohort of newborns in a specific year until death, the period life expectancy could be computed based on a hypothetical cohort. Using the period approach is a more common methodology in estimating life expectancy because the cohort data may be inaccessible or incomplete. However, when we aim to estimate life expectancy for world regions, computing the life expectancies based on either cohort or period data is almost impossible. In these cases, a combination of period and cohort data sets might be applied to construct the relevant life tables and estimate the related life expectancies (1, 10, 11).
The life expectancy data sets for all world countries and regions in different periods of time are available in some data sources provided by Our World in Data, World Bank, and WHO. Comparing the reported life expectancies in these data sets shows that the differences between these estimates are quite negligible. In the present study, we extracted the life expectancy data for Iran, Asia, and regions of Asia (Central Asia: CA, Eastern Asia: EA, South-Eastern Asia: SEA, Western Asia: WA, and Southern Asia: SA) in the period 1960-2020 from the data source provided by the Our World in Data (2).
Statistical analysis
In this study, we used the joinpoint regression analysis to model the pattern of changes in life expectancy. The joinpoint Regression modeling approach can be thought of as a set of different linear models connected together at the joinpoints. This model is a well-known statistical tool for determining significant changes in the trends of the different outcome variables like incidence, prevalence, mortality, or DALY rates in a given population. As a piecewise linear regression model, joinpoint regression utilizes the observed data and searches for the peak points in the trend by estimating their locations and slopes.
Supposing a set of n observations (t1,y1), (t2,y2), ..., (tn,yn), the joinpoint regression model can be written as:
yi = β0 + β1 t1 + γ1 (t1-τ1) + γk (tk-τk) + εi . i = 1, ... , n
where ti indicates the study time points (1960, 1991, ..., 2020) and yi represents the life expectancy data. The parameter τk (k=1,2,...,K) indicates the location of change points, K shows the number of change points, β0, β1 and γ1, ..., γk are the regression parameters and εi is the residual term. The notation (ti - τk)+ = ti - τk if ti - τk > 0 , and (ti - τk)+ = 0 otherwise.
To interpret the estimates, Annual Percentage Change (APC) is commonly used in joinpoint analysis to characterize the behavior of the trends in the outcome variables. The estimated APC is the percentage change (increase or decrease) in the estimated values per year in the time trend. More specifically, it estimates the rate of change in life expectancy from a year to the next year. After fitting the joinpoint regression model, the estimated APC from the year τj to year (τj+1) can be computed as:
APC = 100 × (exp (β1 + γ1 + + γ2 + ... + γj) - 1)
In addition, the weighted mean of the estimated APCs can be reported as the Average Annual Percent Change (AAPC) (12).
In this study, the joinpoint software version 4.9.0.0 was used to fit the joinpoint regression models. In the model fitting process, the software applies a numerical search method and fits the linear regression between two consecutive joinpoints using an ordinary least square (OLS) technique. In this approach, the permutation test is repeatedly used for testing between two models with a different number of joinpoints. In other words, this methodology serially performs the tests of the null hypothesis of no more joinpoint against the alternative of one joinpoint. This test is applied for all possible number of joinpoints that could potentially exist in the observed data and identifies the best-fitted model with a certain number of joinpoints selected by a series of Permutation Tests Based (PTB) methodology or the Bayesian Information Criteria (BIC). To capture the pattern of change in the available data, the software chooses the minimum adequate number of joinpoints so that if one more joinpoint is added to the model, then the model becomes statistically insignificant (13).
Ethics statement
All procedures of the study were performed in accordance with the Declaration of Helsinki. In this study, we used freely available data from the Our World in Data website. Thus the requirement for informed consent was waived. The study protocol was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences (Ethics code: IR.SBMU.RETECH. REC. 1399.1139).
Results
To investigate the trends of life expectancy at birth in Iran, Asia, and five regions of Asia, we first described the pattern of changes in these areas from 1960 to 2020 (these patterns were presented in Asia and Iran by gender but, to summarize the results, they were reported only for total populations of the regions). Table 1 shows the trends of LEB in five regions of Asia over the study period.
Table 1. The trend of life expectancy in Asia, regions of Asia and Iran from 1960 to 2020.
| Region | Year | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1960 | 1965 | 1970 | 1975 | 1980 | 1985 | 1990 | 1995 | 2000 | 2005 | 2010 | 2015 | 2020 | ||
| CA | 55.71 | 57.73 | 59.58 | 60.98 | 62.19 | 63.89 | 64.25 | 63.54 | 64.51 | 66.35 | 68.26 | 70.19 | 71.66 | |
| EA | 57.86 | 60.92 | 64.62 | 67.24 | 69.06 | 70.78 | 72.33 | 73.02 | 74.25 | 76.02 | 77.39 | 78.75 | 80.05 | |
| SEA | 51.12 | 53.52 | 55.1 | 54.64 | 56.82 | 61.31 | 63.52 | 65.25 | 67.08 | 69.15 | 70.97 | 72.34 | 73.81 | |
| SA | 41.81 | 44.6 | 47.15 | 50.01 | 52.71 | 55.28 | 58.74 | 61.78 | 64.61 | 67.25 | 69.35 | 71.09 | 73.00 | |
| WA | 54.64 | 57.78 | 60.84 | 63.62 | 65.89 | 67.86 | 69.51 | 70.83 | 72.18 | 73.38 | 74.3 | 75.09 | 76.32 | |
| Iran | Male | 45.71 | 47.95 | 50.78 | 55.41 | 50.18 | 48.92 | 61.65 | 67.98 | 69.26 | 70.44 | 72.48 | 74.76 | 75.78 |
| Female | 44.15 | 47.49 | 50.94 | 55.00 | 59.33 | 63.16 | 66.26 | 68.75 | 71.13 | 73.50 | 75.43 | 76.92 | 78.09 | |
| Total | 44.95 | 47.73 | 50.86 | 55.26 | 54.11 | 55.20 | 63.84 | 68.38 | 70.18 | 71.92 | 73.91 | 75.80 | 76.93 | |
| Asia | Male | 44.36 | 48.45 | 53.67 | 56.79 | 59.04 | 61.07 | 62.73 | 64.04 | 65.72 | 67.45 | 69.02 | 70.55 | 71.69 |
| Female | 46.18 | 50.52 | 55.94 | 59.08 | 61.82 | 64.05 | 65.88 | 67.60 | 69.27 | 71.02 | 73.02 | 74.84 | 76.02 | |
| Total | 45.24 | 49.46 | 54.78 | 57.90 | 60.39 | 62.51 | 64.25 | 65.75 | 67.43 | 69.18 | 70.95 | 72.62 | 73.85 | |
CA (five countries): Tajikistan, Uzbekistan, Kazakhstan, Turkmenistan, and Kyrgyzstan.
EA (eight countries): China, Mongolia, North Korea, South Korea, Japan, Hong Kong, Taiwan, and Macau.
SEA (eleven countries): Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor Leste, and Vietnam.
SA (nine countries): Sri Lanka, Bangladesh, India, Afghanistan, Pakistan, Bhutan, Nepal, Iran, and the Maldives.
WA (eighteen countries): Georgia, Armenia, Azerbaijan, Turkey, Cyprus, Syria, Lebanon, Israel, Palestine, Jordan, Iraq, Oman, Yemen, Kuwait, Bahrain, Qatar, Saudi Arabia, and United Arab Emirates.
Table 1 shows the trends of LEB in Iran and Asia continent by gender over the study period. Regarding Table 1, one can observe about 65.8%, 76.9%, and 71.2% rise in LEB, respectively, for Iranian males, females, and the total population from 1960 to 2020. In the same period of time, the Asian male, female and total population had experienced a 61.6%, 64.6%, and 63.2% increase in LEB, respectively. Iranian people have experienced higher growth in LEB than Asians in the last six decades (about 4.2%, 12.3%, and 8%, respectively for male, female and total population). If we compare the trends of LEB in Iran and Asia more accurately, it can be concluded that while the Asian population (males, females and total population) have witnessed a continuous rise in LEB during the study period, Iranian males (and subsequently total Iranian population) had a considerable fall in LEB during the late seventies and early eighties followed by a remarkable increase until early nineties.
In the next step, we applied the joinpoint regression analysis to model the trend of LEB in different regions of Asia during the study period. Table 2 and Figure 1 show the results of the fitted joinpoint regression models.
Table 2. Joinpoint regression estimates for life expectancy in different regions of Asia continent from 1960 to 2020.
| Region | Trend | Period | APC† (95%CI) |
|---|---|---|---|
| WA | Trend 1 | 1960-1971 | 1.1* (1.1, 1.2) |
| Trend 2 | 1971-1976 | 0.7* (0.6, 0.8) | |
| Trend 3 | 1976-1990 | 0.5* (0.5, 0.5) | |
| Trend 4 | 1990-1997 | 0.2* (0.1, 0.2) | |
| Trend 5 | 1997-2005 | 0.5* (0.4, 0.5) | |
| Trend 6 | 2005-2020 | 0.3* (0.3, 0.3) | |
| AAPC‡ | 1960-2020 | 0.5* (0.5, 0.6) | |
| SAE | Trend 1 | 1960-1965 | 0.9* (0.9, 1) |
| Trend 2 | 1965-1970 | 0.6* (0.5, 0.7) | |
| Trend 3 | 1970-1977 | -0.2* (-0.3, -0.1) | |
| Trend 4 | 1977-1985 | 1.5* (1.5, 1.6) | |
| Trend 5 | 1985-2009 | 0.6* (0.6, 0.6) | |
| Trend 6 | 2009-2020 | 0.4* (0.3, 0.4) | |
| AAPC | 1960-2020 | 0.6* (0.6, 0.6) | |
| WA | Trend 1 | 1960-1969 | 1.1* (1.1, 1.1) |
| Trend 2 | 1969-1977 | 0.9* (0.9, 0.9) | |
| Trend 3 | 1977-1987 | 0.6* (0.6, 0.6) | |
| Trend 4 | 1987-2004 | 0.4* (0.4, 0.4) | |
| Trend 5 | 2004-2018 | 0.2* (0.2, 0.2) | |
| Trend 6 | 2018-2020 | 0.4* (0.3, 0.5) | |
| AAPC | 1960-2020 | 0.6* (0.6, 0.6) | |
| SA | Trend 1 | 1960-1978 | 1.2* (1.2, 1.2) |
| Trend 2 | 1978-1984 | 0.9* (0.8, 1) | |
| Trend 3 | 1984-1992 | 1.2* (1.2, 1.3) | |
| Trend 4 | 1992-2003 | 0.9* (0.9, 0.9) | |
| Trend 5 | 2003-2010 | 0.6* (0.6, 0.7) | |
| Trend 6 | 2010-2020 | 0.5* (0.4, 0.5) | |
| AAPC | 1960-2020 | 0.9* (0.9, 0.9) | |
| CA | Trend 1 | 1960-1969 | 0.7* (0.7, 0.7) |
| Trend 2 | 1969-1988 | 0.4* (0.4, 0.5) | |
| Trend 3 | 1988-1995 | -0.3* (-0.3, -0.2) | |
| Trend 4 | 1995-1999 | 0.3* (0.1, 0.4) | |
| Trend 5 | 1999-2015 | 0.6* (0.6, 0.6) | |
| Trend 6 | 2015-2020 | 0.4* (0.3, 0.4) | |
| AAPC | 1960-2020 | 0.4* (0.4, 0.4) |
† APC: Annual Percent change
‡AAPC: Average Annual Percent change
Figure 1.
Estimated trends of life expectancy in five regions of Asia from 1960 to 2020 based on joinpoint analysis
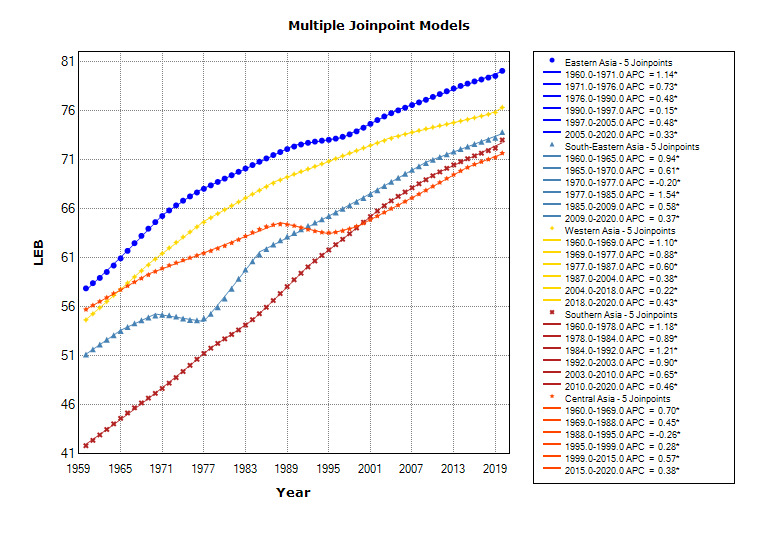
According to the estimates in Table 2, a number of immediate findings could be highlighted; first, these regions have witnessed an upward trend in LEB during all the determined time intervals, except for SEA during the period 1970 -1977 (with an APC of -0.20) and CA countries during the period 1988 -1995 (with an APC of -0.26). Second, the highest rising slope of trend in LEB for EA, WA, and CA regions could be observed in the 60s, while countries in SEA had the highest ascending slope of trend in the late 70s and early 80s. In addition, countries in SA have continuously witnessed high slopes of the trend until the early 2000s. Third, countries in SA and CA regions had the highest and lowest growth in LEB during the study period, with the estimated AAPC of 0.9 and 0.4, respectively.
Table 3, along with Figure 2 and Figure 3, show the estimated patterns from fitting the joinpoint regression models to the LEB data by gender in Iran and Asia.
Table 3. Joinpoint regression estimates for life expectancy in Asia and Iran from 1960 to 2020.
| Location | Trend | Total | Male | Female | |||
|---|---|---|---|---|---|---|---|
| Period | APC† (95 % CI) | Period | APC (95 % CI) | Period | APC (95 % CI) | ||
| Iran | Trend 1 | 1960-1969 | 1.2* (1.1, 1.3) | 1960-1969 | 1.0* (0.9, 1.1) | 1960-1971 | 1.4* (1.4, 1.4) |
| Trend 2 | 1969-1976 | 1.7* (1.5, 1.8) | 1969-1976 | 1.8* (1.5, 2.0) | 1971-1980 | 1.6* (1.5, 1.6) | |
| Trend 3 | 1976-1983 | -0.9* (-1, -0.8) | 1976-1983 | -2.9* (-3.2, -2.7) | 1980-1986 | 1.2* (1.2, 1.3) | |
| Trend 4 | 1983-1991 | 2.7* (2.6, 2.8) | 1983-1992 | 4.2* (4.0, 4.4) | 1986-1992 | 0.9* (0.8, 0.9) | |
| Trend 5 | 1991-1995 | 1.2* (0.8, 1.5) | 1992-2020 | 0.5* (0.5, 0.5) | 1992-2008 | 0.7* (0.7, 0.7) | |
| Trend 6 | 1995-2020 | 0.5* (0.5, 0.5) | --- | --- | 2008-2020 | 0.4* (0.3, 0.4) | |
| AAPC‡ | 1960-2020 | 0.9* (0.9, 9.0) | 1960-2020 | 0.9* (0.8, 0.9) | 1960-2020 | 1.0* (0.9-1.0) | |
| Asia | Trend 1 | 1960-1962 | 1.2* (1.0, 1.4) | 1960-1963 | 1.5* (1.3, 1.7) | 1960-1962 | 1.2* (0.9, 1.5) |
| Trend 2 | 1962-1969 | 2.3* (2.2, 2.3) | 1963-1969 | 2.3* (2.2, 2.4) | 1962-1969 | 2.3* (2.2, 2.3) | |
| Trend 3 | 1969-1975 | 1.2* (1.1, 1.2) | 1969-1975 | 1.2* (1.1, 1.3) | 1969-1975 | 1.1* (1.1, 1.2) | |
| Trend 4 | 1975-1985 | 0.8* (0.7, 0.8) | 1975-1985 | 0.7* (0.7, 0.7) | 1975-1984 | 0.8* (0.8, 0.9) | |
| Trend 5 | 1985-2014 | 0.5* (0.5, 0.5) | 1985-2013 | 0.5* (0.5, 0.5) | 1984-2015 | 0.5* (0.5, 0.5) | |
| Trend 6 | 2014-2020 | 0.3* (0.3, 0.4) | 2013-2020 | 0.3* (0.3, 0.4) | 2015-2020 | 0.3* (0.3, 0.4) | |
| AAPC | 1960-2020 | 0.8* (0.8, 0.8) | 1960-2020 | 0.8* (0.8, 0.8) | 1960-2020 | 0.8* (0.8, 0.8) | |
† APC: Annual Percent change
‡AAPC: Average Annual Percent change
Figure 2.
Estimated trends of life expectancy in Iran from 1960 to 2020 based on joinpoint analysis by gender
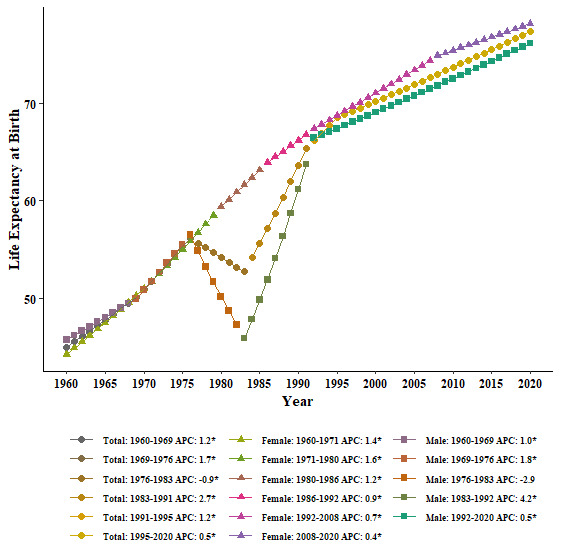
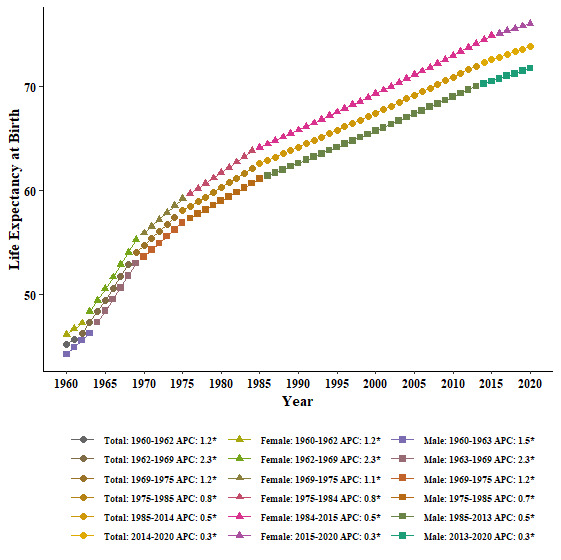
Figure 3.
Estimated trends of life expectancy in Asia from 1960 to 2020 based on joinpoint analysis by gender
The estimates for the Iranian male population show four joinpoints in 1969, 1976, 1983, and 1992. These joinpoints resulted in five segments with different LEB patterns: (1) 1960-1969 with an estimated APC of 1.0, (2) 1969-1976 with an estimated APC of 1.8, (3) 1976-1983 with an estimated APC of -2.9, (4) 1983-1992 with estimated APC of 4.2, and (5) 1992-2020 with estimated APC of 0.5. For Iranian females, a similar analysis led to five different joinpoints in 1971, 1980, 1986, 1992, and 2008. The estimated APCs for the corresponding segments were 1.4, 1.6, 1.2, 0.9, 0.7, and 0.4, respectively. Finally, the fitted regression model to the LEB data in the total Iranian population indicated five joinpoints with six segments: 1960-1969 with an estimated APC of 1.2, 1960-1969 with an estimated APC of 1.2, 1969-1976 with an estimated APC of 1.7, 1976-1983 with estimated APC of -0.9, 1983-1991 with estimated APC of 2.7, 1991-1995 with estimated APC of 1.2 and 1995-2020 with estimated APC of 0.5.
Unlike the estimated trends for Iranians, the Asian men, women, and total populations have experienced quite similar trends in the last six decades. For total Asian people, the joinpoint regression model showed five different joinpoints in 1962, 1969, 1975, 1985, and 2014. The estimated APCs for the corresponding segments were 1.2, 2.3, 1.2, 0.8, 0.5, and 0.3, respectively. The estimated AAPC of 0.8 for the total Asian population tells us that these people have annually experienced less than 1 percent increase in LEB during the study period.
Discussion
In the previous decades, people in nearly all world countries have witnessed longer lifespans because of remarkable progress in living standards, improved health condition, higher educational attainments and public access to more advanced medical technologies. Asia, the most populated continent in the world with about 60% of the entire world population, has also experienced this notable growth in life expectancy during the preceding decades. In the present study, we described and modeled the trend of life expectancy in different regions of Asia. Regarding our findings about the regions of Asia, some immediate conclusions can be made; first, countries in Eastern Asia region had the highest LEB during the whole study period. Second, countries in SA started the study with remarkably lower LEB than the other regions of Asia, while they ended the study with quite similar mean LEB as those in CA and SEA. This means that countries in SA have experienced a higher increasing slope of the trend than the other regions. Third, the variation of LEB among Asian regions at the starting point of the study was drastically higher than the variation in the ending year (2020).
As expected, almost all the Asian regions had positive slopes of trend during different time intervals of the 60-year study period. The only exceptions are related to the countries in SEA in the 70s and CA countries in the late 80s and early 90s. This declining trend in CA can be attributed to the political, social and economic consequences of the dissolution of the Soviet Union between 1988 and 1991 (14, 15). In addition, the unfortunate consequences of the Second Indochina War might be the main reason for the downward trend of life expectancy in SEA in the 70s. After this destructive war, SEA experienced a rapid decline in the mortality rate and significant economic growth which led to a remarkable improvement in life expectancy in this area (16).
Our results also showed that countries in Eastern Asia had the highest life expectancy among Asian regions during the study period. It is not a surprising finding because this region includes countries like Hong Kong, Japan, Macau, and South Korea which are among the top ten world countries with the highest life expectancies. Rapid economic growth and development led to a marked jump in life expectancy after World War II in these countries (17, 18). Although there is still a considerable gap in life expectancy between Eastern Asia and other Asian regions at the last year of the study, the diminished gap in 2020 compared to the starting year of the study seems to be promising for inhabitants living in these four regions. In addition, the estimated APCs for these regions show that the annual percent change in life expectancy has doubled for people in WA between 2018 and 2020 compared to the period 2004-2018 (0.4 for 2018-2020 versus 0.2 for 2004-2018), while people in other regions have experienced lower APCs in the latest intervals compared to the previous periods. From the estimated APCs for five regions of Asia continent, one can also conclude that the mean APC in the earliest interval (mostly in the 60s) is about 1 percent, while this mean has decreased to about 0.4 percent in the latest time intervals. This means about 60 percent reduction in the estimated APCs during recent years compared to the starting years of the study.
In this study, we also examined the six-decade (1960-2020) trend of LEB in the Iranian population. A quick look at the reported life expectancies in the results section reveals that Iranian people have experienced about 32 years increase in LEB during the study period. We also explored that Iranian females have continuously experienced an incremental life expectancy with an average annual percent change of 1.0 in the study time period, while Iranian males (and subsequently the total population) had a downward pattern between 1976 and 1983, followed by a sharp increase in the period of 1983-1992 (1983-1991). The average annual percent change of life expectancy for both male and total populations was 0.9, which means that Iranian people have annually experienced about 1% rise in LEB during the study period.
Now, to describe our findings from another point of view, we can divide the study period into two different time intervals: before and after the victory of the Islamic revolution and the beginning of the Iran-Iraq war (i.e., 1960-1980 and 1980-2020). When we compare the LEB estimates between 1980 and 1960, 9.8%, 34.4%, and 20.4% increase can be observed, respectively in males, females, and the total Iranian population. Moreover, comparing the LEB estimates between 1980 and 2020 tells us that Iranian male, female and total populations have experienced about 51.0%, 31.6%, and 42.2% rise in LEB, respectively. It seems the sharper increasing slope of LEB in Iranian men compared to Iranian women from 1980 to 2020 has compensated for the considerable gap between males and females in 1980. In other words, an estimated difference of more than 9 years in LEB in 1980 has changed to about 2 years difference in 2020. These findings are completely in line with the reported results based on the data from the GBD 2015 study (9). In addition, our reported LEB values are quite similar to those presented by other studies with different data sets (for example, national and subnational data sources) to estimate or predict life expectancy in the Iranian population (7, 8). Regardless of the destructive effect of the Iran-Iraq war on life expectancy in the early 80, the rising trend of life expectancy in Iran could be attributed to several factors such as the launching of a reformed primary health care system (PHC) after the Islamic revolution which decreased health inequality between urban and rural populations, increased socio-economic growth and literacy, improvement in access to health insurance, safe water, and sanitation as well as a decreased rate of malnutrition (7, 8, 19-21).
According to the presented LEBs, we can observe that the total Asian population has experienced about 28.6 years rise in life expectancy from 1960 to 2020. In addition to the identical average annual percent changes for both Asian genders (AAPC=0.8), comparing the estimated APCs in different time intervals shows rather similar values for males and females. However, a closer look at the LEBs shows that Asian women had about 1.8 years higher life expectancy than Asian men in 1960, while this difference increased to 4.3 years in 2020. As another noticeable result, although the Asian population has continuously experienced an upward trend of LEB over the 60-year study period, comparing the estimated APCs in different time intervals demonstrates that the steepest slope of the trend has occurred in the 60s. Afterward, a sharp decrease could be seen in the slopes of the trend until the ending point of the study (from APC of 2.3 in the 60s to APC of 0.3 in the last decade of the study). This upward trend of life expectancy at birth in Asian territories reflects remarkable declines in death rates, especially among mothers, newborns, and infants during the previous decades. Along with wider access to health services, improved lifestyles and living standards, better access to healthy food, drinking water, and sanitation facilities, increased rate of educated people are some of the most important indicators of this gain in longevity in the whole population across Asia (9, 22-24).
At a glance, comparing the trends of LEB in Iran and Asia using the estimated AAPCs shows quite similar patterns (respectively, 0.9 and 0.8). It means that Iranian and total Asian people have annually experienced less than 1% increase in LEB over the past six decades. However, some apparent discrepancies between the observed LEBs and estimated APCs for Iran and Asia could be discovered with a more precise comparison. First, in 1960 Asian people had about 0.3 years higher LEB than Iranians and this difference reached more than 6 years in 1980 and then decreased to about 0.4 years in 1990. From the early 90s, the situation was reversed in favor of Iranians so that Iranian people had a LEB of more than 3 years higher than Asians at the ending point of the study. Second, Asians had continuously positive slopes of the trend over the study period, while Iranians experienced a negative slope during 1976-1983 as a direct consequence of the Iran-Iraq war. Third, the highest slope of LEB growth in Asian populations occurred in the sixties (APC of 2.3), while Iranians witnessed the highest increasing slope in the period 1983-1991 (APC of 2.7). Although this remarkable rise in LEB during the 60s could be a direct result of the above-mentioned factors in Asia, the extraordinary upward slope of the trend during the 80s in Iran might be related to some other causes. Following the Islamic revolution in 1979 and the start of the Iran-Iraq war, the revolutionary government decided to launch new policies which encouraged marriage at younger ages and child-bearing. These policies along with an influx of Afghan refugees, raised the level of fertility significantly and led to the highest population growth rate of more than 4 percent from 1980 to 1986 in Iran (25-28).
Conclusion
In the present study, we applied an analytic approach (joinpoint regression) for modeling the pattern of change in LEB for Iran, Asia, and regions of Asia. However, this statistical model does not allow us to assess the effect of different related factors (such as socioeconomic variables and health indices) on the trend of LEB. This can be considered one of the most important limitations of the present study. As another limitation of the present work, it should be noted that the previous works in this field have generally applied descriptive statistical methods to characterize the patterns of LEB in different parts of the world. Since we interpreted our findings according to inferential measures like APC and AAPC, comparing these analytic indices with descriptive statistics was rather impossible.
In general, our findings revealed that life expectancy at birth in Iran had increased by about 32 years between 1960 and 2020, while the total Asian population has experienced less than 29 years rise in LEB during the same period of time. Comparing the pattern of change in LEB in Iran and Asia shows that Iranians have witnessed a sharper increasing trend than the total Asian population over the past six decades, except during a seven-year period in the late 70s and early 80s. However, the LEB in Iran and Asia is still lower than in some other parts of the world such as northern America, Oceania and Europe. In order to elevate life expectancy to a higher level, the policymakers in Iran and Asian countries should put more effort into promoting the quality of health systems, fair distribution of wealth, improvement in access to health facilities and providing proper nutrition in the upcoming decades.
Conflict of Interests
The authors declare that they have no competing interests.
Acknowledgement
The proposal for this research project was approved by the Faculty of Allied Medical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran (Project Code: 26472). The authors would like to express their gratitude to the Research Deputy of this faculty for the facilitation of the process.
Author Contributions
Conceptualization: MS, FZ. Formal analysis: MAM. FM. Writing-original draft: MS, FZ, MAM, FM. Writing - review & editing: MS, FZ.
Cite this article as : Salehi M, Aziz-Mohammdlooha M, Masaebi F, Zayeri F. Six-Decade Trend Analysis of Life Expectancy at Birth in Asia, Regions of Asia and Iran: A Joinpoint Analysis. Med J Islam Repub Iran. 2022 (23 Dec);36:166. https://doi.org/10.47176/mjiri.36.166
References
- 1.Bilas V, Franc S, Bošnjak M. Determinant factors of life expectancy at birth in the European Union countries. Coll Antropol. 2014;38(1):1–9. [PubMed] [Google Scholar]
- 2. Roser M, Ortiz-Ospina E, Ritchie H. Life Expectancy [cited 2021 Aug 15]. Available from: https://ourworldindata.org/life-expectancy.
- 3. World Health Organization. The global health observatory: Life expectancy and healthy life expectancy [cited 2021 Aug 15]. Available from: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-life-expectancy-and-healthy-life-expectancy.
- 4.Ho JY, Hendi AS. Recent trends in life expectancy across high income countries: retrospective observational study. BMJ. 2018;362:k2562. doi: 10.1136/bmj.k2562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Szmigiera M. Average life expectancy in industrial and developing countries for those born in 2020, by gender [cited 2021 Aug 15]. Available from: https://www.statista.com/statistics/274507/life-expectancy-in-industrial-and-developing-countries/.
- 6. The World Bank Group. Life expectancy at birth, total (years) [cited 2021 Jun 15]. Available from: https://data.worldbank.org/indicator/SP.DYN.LE00.IN.
- 7.Delavari S, Zandian H, Rezaei S, Moradinazar M, Delavari S, Saber A. et al. Life Expectancy and its Socioeconomic Determinants in Iran. Electron Physician. 2016;8(10):3062. doi: 10.19082/3062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ebrahimi N, Mehdipour P, Mohebi F, Ghanbari A, Azmin M, Farzadfar F. Improved population health in Iran from 1979 to 2019; Decreasing mortality rates and increasing life expectancy. Arch Iran Med. 2020;23(2):61. [PubMed] [Google Scholar]
- 9.Sepanlou SG, Parsaeian M, Krohn KJ, Afshin A, Farzadfar F, Roshandel G. et al. Disability-adjusted life-years (dalys) for 315 diseases and injuries and healthy life expectancy (HALE) in Iran and its neighboring countries, 1990-2015: Findings from Global Burden of Disease study 2015. Arch Iran Med. 2017;20(7):403. [PubMed] [Google Scholar]
- 10.Perron L, Simard M, Brisson J, Hamel D, Lo E. Standard period life table used to compute the life expectancy of diseased subpopulations: more confusing than useful. Am J Public Health. 2017;107(10):1615. doi: 10.2105/AJPH.2017.303932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Riley JC. Estimates of Regional and Global Life Expectancy, 1800–2001. Popul Dev Rev. 2005;31(3):537. [Google Scholar]
- 12.Kim HJ, Fay MP, Yu B, Barrett MJ, Feuer EJ. Comparability of segmented line regression models. Biometrics. 2004;60(4):1005. doi: 10.1111/j.0006-341X.2004.00256.x. [DOI] [PubMed] [Google Scholar]
- 13. National Cancer Institute: Division of cancer control and population. Joinpoint trend analysis software, Version 4.9.0.0 [cited 2021 Aug 20]. Available from: https://surveillance.cancer.gov/joinpoint/.
- 14.Batsaikhan U, Dabrowski M. Central Asia - twenty-five years after the breakup of the USSR. Russ J Econ. 2017;3(3):296–320. [Google Scholar]
- 15. Rechel B, Richardson E, McKee M. Trends in health systems in the former Soviet countries [cited 2021 Aug 15]. Available from: https://www.euro.who.int/__data/assets/pdf_file/0019/261271/Trends-in-health-systems-in-the-former-Soviet-countries.pdf. [PubMed]
- 16. Kajimura M. Changes in the demographic structure and economic growth in East and Southeast Asia. ISEAS-Yusof Ishak institute [cited 2021 Aug 15]. Available from: https://www.iseas.edu.sg/wp-content/uploads/2020/06/ISEAS_EWP_2020-5_Kajimura.pdf.
- 17.Mason A, Ogawa N. Population, Labor force, saving and Japan’s future. In Japan’s new economy: continuity and change in the twenty-first century. London: Oxford University Press. 2001
- 18.Ogawa N, Norma M, Lee SH, Abrigo MRM, Aris T. Population aging and the three demographic dividends in Asia. Asian Dev Rev. 2021;38(1):32–67. [Google Scholar]
- 19.Mohammadi Y, Parsaeian M, Mehdipour P, Khosravi A, Larijani B, Sheidaei A. et al. Measuring Iran’s success in achieving Millennium Development Goal 4: a systematic analysis of under-5 mortality at national and subnational levels from 1990 to 2015. Lancet Glob Health. 2017;5(5):e537–e544. doi: 10.1016/S2214-109X(17)30105-5. [DOI] [PubMed] [Google Scholar]
- 20.Moradi-Lakeh M, Esteghamati A. National Immunization Program in Iran: whys and why nots. Hum Vaccin Immunother. 2013;9(1):112. doi: 10.4161/hv.22521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Naghavi M, Shahraz S, Sepanlou SG, BESc PN, Pourmalek F, Lozano R. et al. Health transition in Iran toward chronic diseases based on results of Global Burden of Disease 2010. Arch Iran Med. 2014;7(5):321. [PubMed] [Google Scholar]
- 22.Bayati M, Akbarian R, Kavosi Z. Determinants of life expectancy in Eastern Mediterranean region: A health production function. Int J Health Policy Manag. 2013;1(1):57–61. doi: 10.15171/ijhpm.2013.09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chan MF, Kamala Devi. Factors affecting life expectancy: evidence from 1980-2009 data in Singapore, Malaysia, and Thailand. Asia Pacific J Public Health. 2015;27(2):136–146. doi: 10.1177/1010539512454163. [DOI] [PubMed] [Google Scholar]
- 24.Lin RT, Chen YM, Chien LC, Chan CC. Political and social determinants of life expectancy in less developed countries: a longitudinal study. BMC Public Health. 2012;12:85. doi: 10.1186/1471-2458-12-85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Aghajanian A, Mehryar AH. Fertility transition in the Islamic Republic of Iran: 1976-1996. Asia Pac Popul J. 1999;14(1):21–42. [PubMed] [Google Scholar]
- 26.Aghajanian A. Population change in Iran, 1966-1986: a stalled demographic transition. Popul Dev Rev. 1999;17(4):703. [Google Scholar]
- 27.Abbasi-Shavazi MJ, McDonald P, Hosseini-Chavoshi M. The Fertility Transition in Iran: Revolution and Reprouction. Springer; 2009
- 28.Malekafzali H. Population Control and reproductive health In the Islamic Republic of Iran Arch Iran Med. 2004;7(4):247. [Google Scholar]