

Abstract
Introduction:
The goal of this study was to estimate how state preemption laws that prohibit local authority to raise the minimum wage or mandate paid sick leave have contributed to working-age mortality from suicide, homicide, drug overdose, alcohol poisoning, and transport accidents.
Methods:
County-by-quarter death counts by cause and sex for 1999–2019 were regressed on minimum wage levels and hours of paid sick-leave requirements, controlling for time-varying covariates and place- and time-specific fixed effects. The model coefficients were then used to predict expected reductions in mortality if the preemption laws were repealed. Analyses were conducted during January 2022–April 2022.
Results:
Paid sick-leave requirements were associated with lower mortality. These associations were statistically significant for suicide and homicide deaths among men and for homicide and alcohol-related deaths among women. Mortality may decline by more than 5% in large central metropolitan counties currently constrained by preemption laws if they were able to mandate a 40-hour annual paid sick-leave requirement.
Conclusions:
State legislatures’ preemption of local authority to enact health-promoting legislation may be contributing to the worrisome trends in external causes of death.
INTRODUCTION
U.S. states have increasingly preempted local authority to raise the minimum wage (MW) or mandate paid sick leave (PSL), trends with potential population health consequences.1,2 States preempting local authority to enact such policies tend to be those that have experienced small gains in life expectancy3,4 and large increases in working-age mortality in recent decades.5
Preemption laws, which constrain lower-level governments’ legislative powers, have long been used to harmonize federal, state, and local policymaking or to establish minimum thresholds.6 For instance, the federal government sets a national MW, thereby preempting state and local governments from implementing a lower MW. Many state governments have set a higher MW, thereby prohibiting local governments from enacting a wage below the state’s level. Although state preemption laws are not new, their spread and intent have recently changed.6 The use of preemption accelerated after 2010, whereas its reach expanded to cover new policy domains such as labor standards, public health, environmental protections, and land use.7 Moreover, state preemption has been increasingly used to define regulatory ceilings.6
This study focuses on 2 labor-related domains for which many states have preempted local (i.e., both county and city) authority: MW and PSL.1 In 2000, just 2 states preempted MW increases, and none preempted PSL mandates. Today, 26 states pre-empt localities from raising the MW, and 23 pre-empt mandatory PSL.7,8 Furthermore, 18 of the 26 MW preemption states impose no statewide MW greater than the federal level, whereas 18 of the 23 PSL preemption states impose no statewide PSL requirement. Figure 1 shows the states that have enacted these laws, and Figure 2 plots the growth by year in each type of preemption law during 1999–2019.
Figure 1.
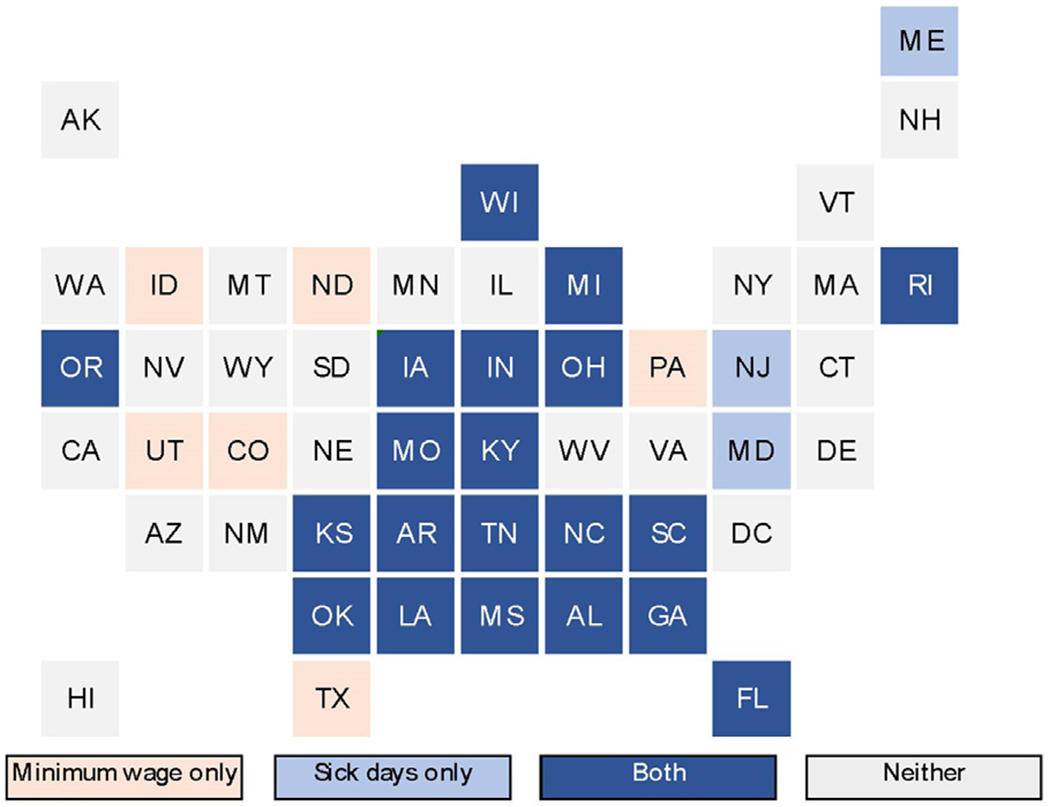
State preemption of local minimum wage and paid leave policies, 2021. AK, Alaska; AL, Alabama; AR, Arkansas; AZ, Arizona; CA, California; CO, Colorado; CT, Connecticut; DC, District of Columbia; DE, Delaware; FL, Florida; GA, Georgia; HI, Hawaii; IA, Iowa; ID, Idaho; IL, Illinois; IN, Indiana; KS, Kansas; KY, Kentucky; LA, Louisiana; MA, Massachusetts; MD, Maryland; ME, Maine; MI, Michigan; MN, Minnesota; MO, Missouri; MS, Mississippi; MT, Montana; NC, North Carolina; ND, North Dakota; NE, Nebraska; NH, New Hampshire; NJ, New Jersey; NM, New Mexico; NV, Nevada; NY, New York; OH, Ohio; OK, Oklahoma; OR, Oregon; PA, Pennsylvania; RI, Rhode Island; SC, South Carolina; SD, South Dakota; TN, Tennessee; TX, Texas; UT, Utah; VA, Virginia; VT, Vermont; WA, Washington; WI, Wisconsin; WV, West Virginia; WY, Wyoming.
Figure 2.
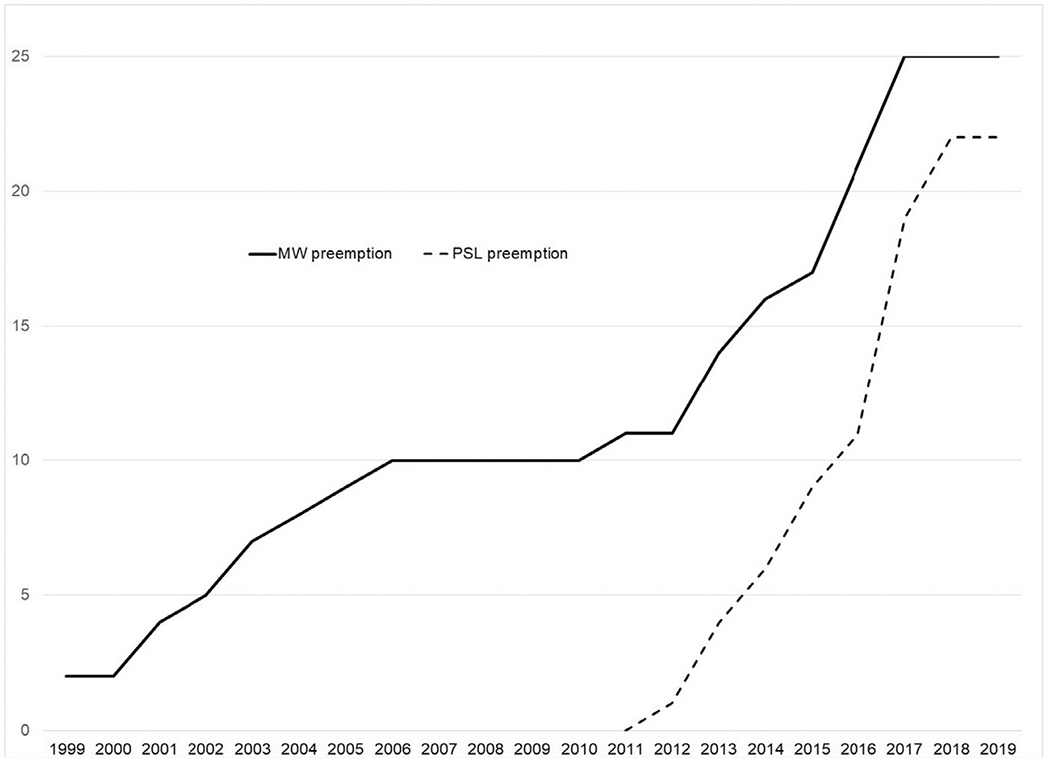
The number of states with MW and PSL preemption laws (by effective year), 1999–2019. MW, minimum wage; PSL, paid sick leave.
Preempting local authority to raise the MW could affect mortality through multiple pathways. For instance, an MW increase can alleviate financial stress,9 reduce unmet medical care needs,10 and improve life satisfaction.11 Partly as a consequence, higher MWs can reduce suicide mortality.12,13 Less attention has been given to MW impacts on other causes of death examined in this study. Effects on alcohol misuse and alcohol-related traffic accidents and mortality are mixed.14 One study of the impacts on homicide15 and another on drug overdose mortality12 found nonsignificant effects.
PSL can also affect mortality through multiple pathways. Those without PSL are more likely to forgo needed medical care and go to work despite illness than workers with PSL.16 Adults lacking PSL face higher risks of nonfatal occupational injuries17 and fatal unintentional injuries such as transport accidents.18 Lack of PSL increases the odds of economic hardship and involuntary job loss for those who take time off to recover,19 which in turn can elevate the odds of suicide,20 drug use,21 and other risky behaviors. PSL can also produce positive spillover impacts on healthy workers by reducing exposure to sick colleagues.8
Using 21 years of state- and county-level data, this study estimates how state preemption of local authority to raise MWs and require PSL may have contributed to working-age mortality from external causes that are prominent contributors to the increase in working-age mortality in recent decades: suicide, homicide, drug overdose, alcohol poisoning, and transport accidents. This study focuses on these causes because they may be impacted by MW and PSL laws, may react quickly to changes in those laws, and may have contributed to recent mortality increases among working-age adults.
METHODS
Study Sample
Mortality data come from restricted-use death certificate files obtained from the U.S. Center for Disease Control and Prevention’s National Vital Statistics System. These data identify causes of death and county of residence for death certificates filed in the U.S. The 5 nonoverlapping cause-of-death categories considered, using ICD-10 codes, are suicide (X66-X84, Y87.0), homicide (X86-X99, Y00-Y09, Y87.1), drug poisoning (X40–44, X60-X64, X85, Y10-Y14), acute alcohol poisoning (X45, X65, Y15), and transport accidents (V01-V99, Y85). Following a recent National Academies of Sciences, Engineering, and Medicine report on working-age mortality,5 drug- and alcohol-related suicides were included in the drug poisoning and acute alcohol poisoning categories, respectively.
The mortality data were organized into county-by-quarter counts of death among adults aged 25–64 years, separately for males and females, for the 21-year period of 1999–2019. Exposure to mortality risk was based on the midquarter sex-specific count of adults aged 25–64 years. The population counts use Center for Disease Control and Prevention Bridged Race Population Estimates, available for the midpoint of each calendar year.22 Linear interpolation (and for the last 2 quarters of 2019, extrapolation) was used to estimate midquarter counts. The resulting data file has 263,172 records, linked to measures of MW levels, PSL requirements, and several covariates.
Measures
For each county-quarter observation, the average inflation-adjusted MW and the required amount of employer-provided PSL hours were determined using several sources.23,24 MW was measured in dollars per hour, and PSL mandates were measured by annual hours of accrued leave required; state PSL laws generally express these requirements as “one hour of paid sick leave earned per Y hours of work time” up to a maximum accrual amount. For both policy domains, information on the dates of all changes was used to develop daily measures, which were then averaged by quarter. Most of the variation in both variables is at the state level, but for a few counties and cities, requirements that exceeded the prevailing state level were in effect at times. When a city’s MW or PSL requirement exceeded that of its parent county, an average county-level value was determined by weighting each subcounty component’s MW or PSL requirement by its share of the county population, using 2010 Census population counts. Data on the timing of preemption laws come from the Economic Policy Institute.25
The analysis also controlled for several time-varying county-level demographic covariates that are likely to influence county-level mortality from the causes of death considered. Using these criteria, for each county-quarter observation, the study included sex-specific estimates of racial/ethnic composition (percentage White [omitted], Black, Hispanic, and other non-White race), age composition (percentage aged 25–34 [omitted], 35–44, 45–54, and 55–64 years), and unemployment and employment rates. An indicator of the state’s participation in the Medicaid expansion offered through the Affordable Care Act was included to control for enhanced access to health care.26,27 Because of urban–rural differences in the propensity to enact ML and PSL laws as well as in mortality patterns, metropolitan status was included using the most current (2013) version of a 6-category Urban-Rural Classification Scheme (URCS).28
Statistical Analysis
The analysis used a 2-step approach to assess the potential consequences of MW and PSL preemption on mortality. The first step estimated the presumed impacts of MW levels and PSL hours on each cause of death, and the second step used those model results to predict the number of deaths attributable to preemption of MW and PSL laws. Negative binomial regression was used for each cause-of-death count, controlling for the size of the population exposed to the risk of death. In each county-quarter combination, the expected number of deaths equals λitRit, where λit is the intensity (or rate) parameter of the negative binomial probability distribution in location i during time-period t, and Rit represents the at-risk population. The model used a log-linear expression for the rate, that is,
where Xit represents the time-varying explanatory variables, and θl, θy and θq are fixed effects for location, year, and calendar quarter, respectively. The location fixed effects are a set of 252 state-by-URCS category combinations. Analyses were stratified by sex given observed patterns in employment, wages, and family responsibilities. The analyses were not stratified by race/ethnicity owing to small populations for certain racial/ethnic groups in many counties. ML and PSL are likely to have their strongest benefits for those with lower levels of education. However, although it is possible to obtain county-level death counts by education, these data are not available in all county-quarter observations during our study period. For example, education was not included on death certificates in some states (South Dakota, Georgia, Rhode Island) in the earlier years of the time series. SEs were clustered at the state level, which most closely corresponds to the levels at which the key treatments (MW and PSL) are assigned. Statistical significance of the regression coefficients was determined using α = 0.05.
The second step of the analysis used observations for counties that in 2019 faced both MW and PSL preemption. For those observations, the observed MW and/or PSL hours values were replaced with plausible counterfactual values, that is, the values likely to be observed in the absence of preemption. Using the estimated regression coefficients and the counterfactual levels of MW and/or PSL, the model predicted counts of 2019 deaths by cause and sex in these counties if the preemption laws had not been in effect.
RESULTS
Statistically significant associations between PSL and homicides (men and women), suicides (men), and alcohol poisonings (women) were found. There were no statistically significant associations for MW. Point and interval estimate of rate ratios (exponentiated regression coefficients) for the PSL coefficients are plotted in Figure 3; more details are provided in Appendix Tables 1 and 2 (available online). Among women, a 1-hour increase in PSL is associated with a 0.2% reduction in homicide (RR=0.998; 95% CI=0.996, 0.999) and a 0.4% reduction in alcohol deaths (RR=0.996; 95% CI=0.993, 0.999). Among men, a 1-hour increase in PSL requirements is associated with a 0.1% reduction in suicide (RR=0.999; 95% CI=0.998, 0.999) and a 0.2% reduction in homicide (RR=0.998; 95% CI=0.996, 0.999). The decreases are sizable compared with those at a zero-hours baseline; for example, according to the models, moving from 0 to 40 hours of PSL would decrease homicide mortality by more than 13% among women and by nearly 8% among men.
Figure 3.
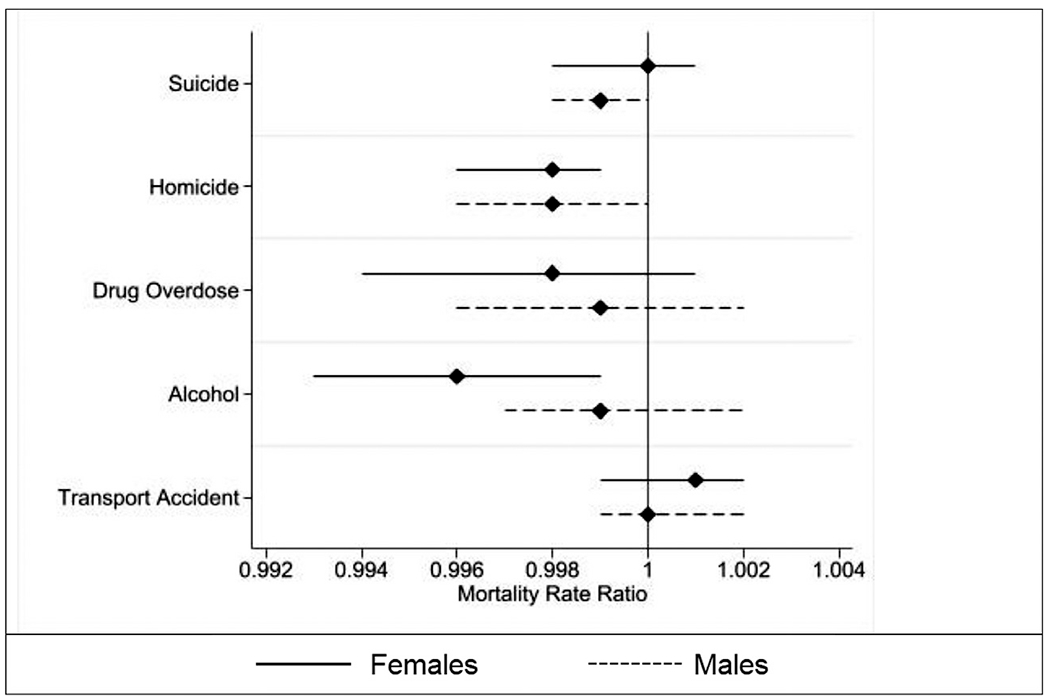
Mortality rate ratios per unit increase in requirements, 1999–2019. Note: Horizontal lines are 95% CIs. Alcohol data cover 2008 through 2019. Models adjust for the states’ Medicaid expansion, the counties’ racial composition, age structure, employment rate, and unemployment rate, and calendar year and quarter and include fixed effects for state-urbanicity combinations.
Whereas the first part of the analysis estimated the association between ML and PSL levels on mortality, the second part explicitly considers the role of preemption. That is, the models from the first part of the analysis were used to predict the number of deaths attributable to preemption or, conversely, deaths that could have been averted if preemption laws were eliminated. Several counties and cities have passed legislation raising the MW or mandating PSL only, to have those laws nullified by their state’s preemption laws. If preemption laws were overturned, those localities as well as numerous others would be expected to pass MW increases, PSL mandates, or both.
Predictions based on the range of mandated PSL hours observed in the states and localities that have imposed them are presented, illustrating the potential for mortality reduction in a counterfactual world without preemption. The counterfactual predictions are limited to PSL and focus on counties most affected by preemption laws. In 4 counties (Orange County in Florida and Bexar, Dallas, and Travis Counties in Texas), a local ordinance requiring private employers to provide PSL was passed or attempted but was prevented by state preemption law from being enacted. For these 4 counties, the PSL requirement they would have imposed, if allowed to do so, is known (details are in Appendix Tables 3, available online); these are considered observed counterfactual localities. For these 4 counties, the models predict that total deaths in 2019 would have fallen from their observed value of 885 to 819, a 7.5% reduction.
Because all the observed counterfactual counties are in the large central metropolitan URCS category, the counterfactual predictions were repeated for all large central metropolitan counties located in states that currently pre-empt both MW and PSL laws and that have neither a state MW nor PSL mandate (Alabama, Goergia, Indiana, Iowa, Kansas, Kentucky, Louisina, Mississipi, North Carolina, Oklahoma, South Carolina, Tennessee, and Wisconsin). There are 21 such hypothetical counterfactual counties, among which total deaths because of homicide (men and women), suicide (men only), and alcohol poisoning (women only) averaged 167.3 in 2019.
Figure 4 plots the predicted mortality reductions associated with alternative PSL requirements in the 21 hypothetical counterfactual counties using PSL hours requirements ranging from 20 per year to 80 per year, well within the range of observed policies. Figure 4 shows that mortality reductions ranging from about 3% to over 10%, on average, are predicted if these counties had been free to adopt PSL mandates.
Figure 4.
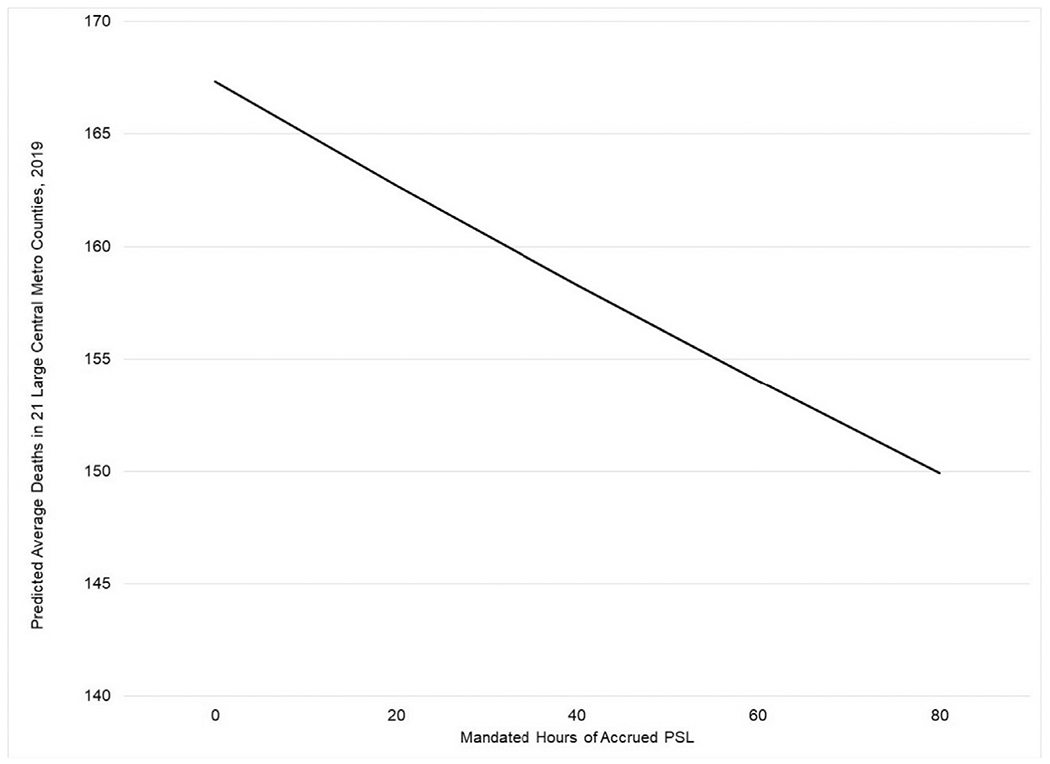
Predicted mortality reductions in the absence of state preemption laws. Note: Reductions in 2019 mortality owing to suicide, homicide, and drug poisoning are shown for 21 large central metropolitan counties located in states that had both MW and PSL preemption laws in place (in 2019) and do not have MW or PSL requirements that exceed federal levels. MW, minimum wage; PSL, paid sick leave.
DISCUSSION
Working-age mortality has increased in recent decades, a trend not experienced among infants, children, and older adults. For example, between 2010 and 2017, working-age mortality rates (ages 25–64 years) increased by 6% (from 328.5 to 348.2 deaths per 100,000 population), whereas mortality rates fell among infants and adults aged 65 years and older and were unchanged among children. Large increases in drug and alcohol poisoning and suicides over this period as well as more recent increases in homicides and transport accidents (since 2010) have contributed to this concerning trend among working-age adults.5 Improved employment conditions produced by a higher MW or hours of PSL might counteract the factors that increase deaths from these external causes, such as stress, material deprivation, adverse coping behaviors, and lack of access to health care. However, U.S. states are increasingly preempting local governments from enacting such policies. This study examined the potential for state preemption of local authority to raise the MW and mandate PSL to influence mortality from suicide, homicide, drug overdose, alcohol poisoning, and transport accidents among working-age adults from 1999 to 2019.
This study has 3 important findings. First, mandating PSL could potentially reduce deaths from several causes implicated in the high working-age adult mortality,5 including suicide and homicide among men and homicide and alcohol-related deaths among women. As one example, moving from 0 to 40 hours of PSL is predicted to decrease homicide mortality by more than 13% among women and by nearly 8% among men.
Second and in contrast to the findings of several past studies, this study did not detect significant MW effects on deaths for the 5 causes considered in this paper. Although the effect sizes of MW on working-age mortality differ across past studies (depending on covariates and the population studied), the general conclusion has been that higher MWs reduce mortality risk. There are several possible explanations for this difference, including that this study included all working-age adults rather than only those with low levels of education. Requirements that employers offer PSL have the potential to improve the situation of workers (and their families) throughout the wage distribution, whereas MW increases produce higher wages mainly for those toward the bottom of the wage distribution. For example, data on employee compensation for 2009 (before the imposition of PSL mandates everywhere but in Washington, DC) show that PSL coverage among those in the bottom quarter of the wage distribution was only 37%, and although being in the top quartile of the wage distribution was much higher (86%), there was still room for growth in PSL coverage.29 Moreover, there is no federal PSL requirement, so when a state or locality imposes a requirement of, say, a 40-hour-per-year sick-leave entitlement, it represents a large increase from the status quo value of zero. In contrast, increases in a state or local MW are relative to the long-established federal minimum. The difference may also be explained by the inclusion of both MW and PSL in the models or by the fact that clustering errors at the state level rather than at the local level can produce conservative inferences.30
The third finding builds on the first 2 and is the crux of this study. Several cities and counties have tried to raise their MW or mandate PSL but only to have their state legislatures react by preempting their authority to do so. These findings indicate that the preemption laws have the potential to exert adverse consequences on working-age mortality. The potential to save lives is greatest in the counties most affected by these preemption laws—large metropolitan counties in states that pre-empt both MW and PSL laws and do not have a state MW nor a PSL mandate. For 4 of these counties, the PSL requirement they attempted to impose is known; the models predict that had they been allowed to implement their PSL requirement, deaths by homicide, suicide, and alcohol poisoning would have been 7.5% lower in 2019. Among an additional 21 counties most likely to adopt such mandates, the analogous numbers of deaths are predicted to range from about 3% to over 10% lower than observed in 2019, depending on the generosity of PSL hours requirements chosen. These findings add to a growing literature pointing to the importance of states’ labor and economic policies on mortality among working-age adults.14,31–33
Limitations
Findings should be considered in light of some limitations. First, it was not possible to account for decedents’ duration of residence in the state or county where they died. Second, the mechanisms driving death operate across the life course, whereas these analyses consider policies in effect over a particular time period. The 5 causes of death studied in this research have relatively short developmental periods, and previous research cited in this paper has either hypothesized or shown that they are affected by labor laws. Third, death certificates may misclassify the cause of death, leading to an undercount of the causes of death examined in this study, particularly suicides. Fourth, despite careful controls for time-varying observable factors as well as unobservable factors captured by the fixed effects, the estimated effects may not be purely causal. Finally, the analysis could not disaggregate by race/ethnicity owing to small population sizes for certain racial/ethnic groups in many counties.
CONCLUSIONS
The proliferation of preemption laws has been called a “significant and quiet threat to public health.”2 This study supports that warning. Absent an increase in the federal MW, many cities and counties took the initiative. Many states reacted by suppressing those efforts. More recently, state preemption laws have figured prominently during the coronavirus disease 2019 (COVID-19) pandemic, because states such as Florida, Texas, and Georgia overrode local authority to contain the virus’s spread through mask mandates, social distancing orders, school closings, and more.7 The consequences of preemption laws are potentially profound. They stymie local government innovation, constrain opportunities to earn a living wage and take time off from work for medical care without financial repercussions, elevate the risks of death among infants33 and working-age adults, and contribute to geographic disparities in mortality.
Supplementary Material
ACKNOWLEDGMENTS
The views expressed in this article do not necessarily reflect the views of the Robert Wood Johnson Foundation or the National Institute on Aging.
Support for this article was provided by the Robert Wood Johnson Foundation’s Policies for Action program through grant number 76103 and from the Center for Aging and Policy Studies, which receives center core funding from the National Institute on Aging (P30AG66583).
No financial disclosures were reported by the authors of this paper.
Footnotes
CREDIT AUTHOR STATEMENT
Douglas A. Wolf: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing - review and editing. Jennifer Karas Montez: Conceptualization, Formal analysis, Funding acquisition, Methodology, Software, Writing - original draft. Shannon M. Monnat: Conceptualization, Data curation, Funding acquisition, Methodology, Resources, Software, Validation, Writing - review and editing.
SUPPLEMENTAL MATERIAL
Supplemental materials associated with this article can be found in the online version at https://doi.org/10.1016/j.amepre.2022.06.005.
REFERENCES
- 1.Huizar L, Lathrop Y. Fighting wage preemption: how workers have lost billions in wages and how we can restore local democracy. New York, NY: National Employment Law Project; 2019. https://www.nelp.org/publication/fighting-wage-preemption/. Accessed November 2, 2021. [Google Scholar]
- 2.Pomeranz JL, Pertschuk M. State preemption: a significant and quiet threat to public health in the United States. Am J Public Health. 2017;107(6):900–902. 10.2105/AJPH.2017.303756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Montez JK Deregulation, devolution, and state preemption laws’ impact on U.S. mortality trends. Am J Public Health. 2017;107(11):1749–1750. 10.2105/AJPH.2017.304080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Montez JK How state preemption laws prevent cities from taking steps to improve health and life expectancy. Cambridge, MA: Scholars Strategy Network. 2018. https://scholars.org/contribution/how-state-preemption-laws-prevent-cities-taking-steps-improve-health-and-life. Published March 6. Accessed November 3, 2021. [Google Scholar]
- 5.National Academies of Sciences, Engineering, and Medicine. High and Rising Mortality Rates Among Working-Age Adults. Washington, DC: The National Academies Press, 2021. 10.17226/25976. [DOI] [PubMed] [Google Scholar]
- 6.Briffault R The challenge of the new preemption. Stanford Law Rev. 2018;70:1995–2027. https://scholarship.law.columbia.edu/faculty_scholarship/2090. [Google Scholar]
- 7.The increased use and abuse of preemption. Local Solutions Support Center. March 19, 2019. https://www.supportdemocracy.org/preemption. Accessed November 2, 2021.
- 8.Pomeranz JL, Silver D, Lieff SA, Pagán JA. State paid sick leave and paid sick-leave preemption laws across 50 U.S. states, 2009–2020. Am J Prev Med. 2022;62(5):688–695. 10.1016/j.amepre.2021.11.018. [DOI] [PubMed] [Google Scholar]
- 9.Andrea SB, Messer LC, Marino M, Goodman JM, Boone-Heinonen J. The tipping point: could increasing the subminimum wage reduce poverty-related antenatal stressors in U.S. women? Ann Epidemiol. 2020;45:47–53 e6. 10.1016/j.annepidem.2020.03.007. [DOI] [PubMed] [Google Scholar]
- 10.Ibragimov U, Beane S, Friedman SR, et al. States with higher minimum wages have lower STI rates among women: results of an ecological study of 66 U.S. metropolitan areas, 2003–2015. PLoS One. 2019;14(10):e0223579. 10.1371/journal.pone.0223579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kuroki M Subjective well-being and minimum wages: evidence from U.S. states. Health Econ. 2018;27(2):e171–e180. 10.1002/hec.3577. [DOI] [PubMed] [Google Scholar]
- 12.Dow WH, Godøy A, Lowenstein C, Reich M. Can labor market policies reduce deaths of despair? J Health Econ. 2020;74:102372. 10.1016/j.jhealeco.2020.102372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kaufman JA, Salas-Hernández LK, Komro KA, Livingston MD. Effects of increased minimum wages by unemployment rate on suicide in the USA. J Epidemiol Community Health. 2020;74(3):219–224. 10.1136/jech-2019-212981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Leigh JP Treatment design, health outcomes, and demographic categories in the literature on minimum wages and health. Econ Hum Biol. 2021;43:101043. 10.1016/j.ehb.2021.101043. [DOI] [PubMed] [Google Scholar]
- 15.Fone ZS, Sabia JJ, Cesur R. Do Minimum Wage Increases Reduce Crime? Cambridge, MA: National Bureau of Economic Research, October 2020. Published. 10.3386/w25647. [DOI] [Google Scholar]
- 16.DeRigne L, Stoddard-Dare P, Quinn L. Workers without paid sick leave less likely to take time off for illness or injury compared to those with paid sick leave. Health Aff (Millwood). 2016;35(3):520–527. 10.1377/hlthaff.2015.0965. [DOI] [PubMed] [Google Scholar]
- 17.Asfaw A, Pana-Cryan R, Rosa R. Paid sick leave and nonfatal occupational injuries. Am J Public Health. 2012;102(9):e59–e64. 10.2105/AJPH.2011.300482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kim D Paid sick leave and risks of all-cause and cause-specific mortality among adult workers in the USA. Int J Environ Res Public Health. 2017;14(10):1247. 10.3390/ijerph14101247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Gould E, pay? Schieder JWork sick or lose. The high cost of being sick when you don’t get paid sick days. Washington, DC: Economic Policy Institute; June 28, 2017. https://www.epi.org/publication/work-sick-or-lose-pay-the-high-cost-of-being-sick-when-you-dont-get-paid-sick-days/. Accessed November 10, 2021. [Google Scholar]
- 20.Elbogen EB, Lanier M, Montgomery AE, Strickland S, Wagner HR, Tsai J. Financial strain and suicide attempts in a nationally representative sample of U.S. adults. Am J Epidemiol. 2020;189(11):1266–1274. 10.1093/aje/kwaa146. [DOI] [PubMed] [Google Scholar]
- 21.Nagelhout GE, Hummel K, de Goeij MCM, de Vries H, Kaner E, Lemmens P. How economic recessions and unemployment affect illegal drug use: A systematic realist literature review. Int J Drug Policy. 2017;44:69–83. 10.1016/j.drugpo.2017.03.013. [DOI] [PubMed] [Google Scholar]
- 22.Centers for Disease Control and Prevention. U.S. Census Populations With Bridged Race Categories. https://www.cdc.gov/nchs/nvss/bridged_race.htm. Accessed July 13, 2021.
- 23.National Partnership for Women & Families. Paid sick days - state and district statutes. Washington, DC: National Partnership for Women & Families. http://www.nationalpartnership.org/our-work/resources/economic-justice/paid-sick-days/paid-sick-days-statutes.pdf. Published July 2021. Accessed August 5, 2020. [Google Scholar]
- 24.Vaghul K, Zipperer B. Historical state and sub-state minimum wage data. Washington, DC: The Washington Center for Equitable Growth; 2016. https://equitablegrowth.org/working-papers/historical-state-and-sub-state-minimum-wage-data/. Published September 7, 2016. Accessed July 10, 2019. [Google Scholar]
- 25.Workers’ rights preemption in the U.S.: a map of the campaign to suppress workers’ rights in the states. Economic Policy Institute; August 2019. https://www.epi.org/preemption-map/. Accessed March 18, 2021. [Google Scholar]
- 26.Sommers BD, Baicker K, Epstein AM. Mortality and access to care among adults after state Medicaid expansions. N Engl J Med. 2012;367(11):1025–1034. 10.1056/NEJMsa1202099. [DOI] [PubMed] [Google Scholar]
- 27.Montez JK, Beckfield J, Cooney JK, et al. US state policies, politics, and life expectancy. Milbank Q. 2020;98(3):668–699. 10.1111/1468-0009.12469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ingram DD, Franco SJ. NCHS urban-rural classification scheme for counties. Vital Health Stat 2. 2012(154):1–65. https://www.cdc.gov/nchs/data_access/urban_rural.htm#Data_Files_and_Documentation. [PubMed] [Google Scholar]
- 29.Employee Benefits in the United States, March 2009. U.S. Bureau of Labor Statistics. www.bls.gov/ncs. Accessed November 21, 2021.
- 30.Abadie A, Athey S, Imbens GW, Wooldridge J. When should you adjust standard errors for clustering? Cambridge, MA: National Bureau of Economic Research, November 2017. Published. 10.3386/w24003. [DOI] [Google Scholar]
- 31.Gertner AK, Rotter JS, Shafer PR. Association between state minimum wages and suicide rates in the U.S. Am J Prev Med. 2019;56(5):648–654. 10.1016/j.amepre.2018.12.008. [DOI] [PubMed] [Google Scholar]
- 32.Van Dyke ME, Komro KA, Shah MP, Livingston MD, Kramer MR. State-level minimum wage and heart disease death rates in the United States, 1980–2015: a novel application of marginal structural modeling. Prev Med. 2018;112:97–103. 10.1016/j.ypmed.2018.04.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Wolf DA, Monnat SM, Montez JK. Effects of U.S. state preemption laws on infant mortality. Prev Med. 2021;145:106417. 10.1016/j.ypmed.2021.106417. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.