

Abstract
Objective:
Research in psychosomatic medicine includes a long history of studying how responses to anger-provoking situations are associated with health. In the context of a marriage, spouses may differ in their anger-coping response style. Where one person may express anger in response to unfair, aggressive interpersonal interactions, his/her partner may instead suppress anger. Discordant response styles within couples may lead to increased relational conflict, which, in turn, may undermine long-term health. The current study sought to examine the association between spouses’ anger-coping response styles and mortality status 32 years later.
Methods:
The present study used data from a subsample of married couples (N = 192) drawn from the Life Change Event Study to create an actor-partner interdependence model.
Results:
Neither husbands’ nor wives’ response styles predicted their own or their partners’ mortality. Wives’ anger-coping response style, however, significantly moderated the association of husbands’ response style on mortality risk 32 years later, β = −0.18, −0.35 to −0.01, p = .039. Similarly, husbands’ response style significantly moderated the association of wives’ response style and their later mortality, β = −0.24, −0.38 to −0.10, p < .001. These effects were such that the greater the mismatch between spouses’ anger-coping response style, the greater the risk of early death.
Conclusions:
For a three-decade follow-up, husbands and wives were at greater risk of early death when their anger-coping response styles differed. Degree of mismatch between spouses’ response styles may be an important long-term predictor of spouses’ early mortality risk.
Keywords: marriage, anger-coping response styles, mortality, anger, spouse
INTRODUCTION
Over the life course, close relationships create an interpersonal context that can give rise to both good and ill health (1). Low-quality relationships are associated with increased mortality risk, in some cases more so than traditional health risk factors. Having high versus low social support, for example, is as predictive of risk for early mortality as excessive alcohol consumption, low physical activity, and elevated body mass (2). Social support and social relationships are gaining increased recognition as key factors shaping a variety of public health outcomes (3). The European Guidelines on Cardiovascular Disease Prevention in Clinical Practice (4) recently recommended that social support should be assessed as a key risk factor for cardiovascular health. The specific characteristics of close relationships—such as their quality or frequency—also impact on health. For example, marital quality predicts lower likelihood of mortality and better health overall (5), as well as greater survival rates in at risk populations (6,7). These effects on people’s likelihood of early death likely unfold over the long term, suggesting that longitudinal, life-course approaches are necessary to understand the health impact of relationship characteristics (8).
One approach to understanding dyadic social influences on health comes from the emerging science on interpersonal theory (9–11). This approach—with roots in personality, clinical, and social psychology—provide a theoretical framework with which to understand how the characteristics of one person can influence the experience of a dyadic target, acutely and longitudinally. The work of Smith and colleagues (12–14) have led to the adaptation of this theory to understand psychosocial influences in physical health risk and resilience, including in the context of sustained intimate relationships such as marriage (15,16). The interpersonal approach suggests that personality traits and individual differences moderate interpersonal dynamics to engender a congruent interpersonal experience across social audiences and contexts (14,17). Application of the interpersonal approach broadly suggests that marriage may represent a case of Person × Environment fit characterized in part by the personality/interpersonal style match between partners (18,19), where both partners bring their own individual traits and behaviors that interact with their partners’ characteristics in turn. One individual difference of note that might impact ongoing interpersonal dynamics is people’s anger-coping response style (20,21). Anger-coping responses styles describe a continuum of behaviors people exhibit in response to challenging interpersonal stimuli that range from suppression—in which individuals hide their covert negative reactions to others’ unfair or aggressive behavior—to expression, in which people overtly convey their anger in response to others’ unfair behavior. From an interpersonal approach, people’s individual anger-coping response styles cannot exist in a vacuum, but instead operate within the context of people’s ongoing social context and, especially, ongoing social interactions.
A key tenant within interpersonal theory is the principle of complementarity (17,18), which predicts that the actions of one pull for specific responses from the interpersonal target. For example, dominant behavior from one person pulls for submissive reactions. These dynamics are studied as specific units of control and affiliation and generally studied in acute contexts (22). Using measures that lack specific grounding in these behavioral dimensions can make for a less than optimal application of interpersonal theory. Nevertheless, the interpersonal approach provides a general basis for predicting that a personality mismatch is predicted to have longitudinal health consequence. For example, levels of match or mismatch in terms of anger-coping response styles may operate as a moderator of chronic interpersonal stress leading to long-term health damage (21) to the extent that extent that these response styles “restrict” or “push” for similar responses from people in the immediate environment. This is particularly important in the case of marriage; one spouse’s reactions to distressing or challenging stimuli impact and are impacted by their partner’s behavior and vice versa (22).
In the present study, we explore how spouses’ anger-coping responses—and especially the (statistical) interaction between their anger-coping responses—are associated with risk for early mortality using data from the Tecumseh Community Health Study (TCHS). The TCHS is a large study of community health that was originally focused on cardiovascular health. A subsample of the larger TCHS community sample completed a variety of psychosocial measures in 1971/1972, comprising the Life Change Event Study (LCES). In previous reports, Harburg and colleagues (20,21,23) found that suppressive anger-coping response style was associated with increased risk of mortality over 18 years. This was reflected both within individual outcomes in the broader LCES (23), as well as in couples in which both partner evidenced a suppressive anger-coping response style (21). The current analyses build on this previous work by exploring whether spouses’ anger-coping response styles are associated with risk of early mortality using a subsample of couples (N = 192) drawn from the LCES, whose mortality was tracked for the subsequent 32 years.
The primary goals of this article are to examine whether the initial findings from the LCES dyadic sample extend in time—that is, to conduct a critical follow-up of this earlier work and to examine if the 17-year follow-up findings hold at the 32-year follow-up period. In doing so, we also apply contemporary data analytic methods to the most recent follow-up sample. Modern advances in dyadic modeling, including the actor-partner interdependence model (APIM (24)), enable the direct testing of how people’s individual characteristics, such as their anger-coping response styles, might interact with their spouse’s characteristics to predict relevant outcomes. In particular, these models can investigate whether spousal match or mismatch—that is, the degree of similarity between husbands’ and wives’ suppressive or expressive response styles—might predict health outcomes beyond the main effect models. It is possible that it is not an individual’s or their spouse’s response style that predicts health outcomes, but instead a combination of the two. Although evidence supports the acute effects of match/mismatch and anger on physiological processes hypothesized to influence health (22), there is a lack of longitudinal data addressing the long-term health impact of mismatch. The current study seeks to address this gap by investigating how the interaction of spouses’ anger-coping response styles might predict their risk for early death.
Present Study
To explore the association between husbands’ and wives’ anger-coping response styles and their mortality risk 32 years later, we used the LCES data in an APIM (24) design. Based on previous findings from this sample (21,23), we hypothesized that participants would evidence significant actor and partner effects of their response styles on their later mortality status, such that a more suppressive style would predict greater risk of early death. In addition, we investigated the interaction of husbands’ and wives’ response styles would be associated with mortality status 32 years later and predicted that greater mismatch in spouses’ response styles would be associated with increased risk for early death for both husbands and wives. Although we used interpersonal theory as a broad, guiding framework for understanding how interpersonal behaviors and interactions may ultimately shape health outcomes, data from the LCES is not well-suited for studying specific hypotheses derived from the theory, largely because the available data centers on anger-coping and extant interpersonal theory centers on the interpersonal circumplex, defined by the dimensions of affiliation and dominance (14–16,22). In this way, elements of the theory—especially its focus on transactionalism—are relevant to the current study, even if deriving specific dominance/affiliation predictions is difficult.
METHODS
Participants
As described in detail by Harburg et al. (23), the current sample was drawn from the LCES. The LCES was a subsample selected from the TCHS, a larger representative, longitudinal study of more than 6000 participants from the Tecumseh area of Michigan. More detailed information on the TCHS is provided by Napier, Johnson, and Epstein (25) and Hawthorne (26).
The LCES subsample consisted of 20% of the original TCHS sample and was collected to provide additional psychological, sociological, and physiological related to participants’ life changes. Of the 1214 participants originally selected, 696 participants entered the LCES. The remaining participants were excluded because of either health status, age, or their choice not to participate in the additional study. As described in Harburg et al. (23), these participants were largely representative of the local community, which was predominantly white, middle class, and married at the time of the original data collection. Of these 696 participants, 384 were married and had a spouse who also participated in the LCES, resulting in a total of 192 couples who participated and were included in the full sample. Husbands were 49.0 (SD = 9.1) years old and wives were 46.7 (SD = 8.8) years old on average at the initial assessment collected in 1971/1972.
Measures
Demographic and Health-Related Variables
The LCES included a variety of self-reported demographic variables. The current study included age for both husbands and wives, as well as the household income. In addition to demographic variables, participants also reported on their cigarette smoking status and participants’ systolic blood pressure as measured during a laboratory visit. Smoking status was scored on an ordinal scale from 1 to 5. Responses were coded as not smoking (1), less than 1/2 a pack a day (2), between 1/2 and 1 pack a day (3), 1 and 2 packs a day (4), and more than 2 packs a day (5). Systolic blood pressure was scored continuously in terms of millimeters mercury.
Anger-Coping Response Styles
Consistent with previous investigations of anger-coping response styles (23), the current study operationalized anger-coping response styles using self-reported scores on six items assessing participants’ typical responses to anger-provoking situations developed by Harburg and colleagues (20). Three items related to anger-provoking situations from a spouse, whereas the other three related to a police officer. The three questions for both spouses and police officers assessed participants’ anger (5-point scale), guilt (4-point scale), and protest (4-point scale) related to the provided situation. The anger situation related to a policeman/spouse “blowing up” at the participants for no reason and the anger the participant might feel or not feel, with responses including “I’d get angry or mad and show it (1),” “I’d get annoyed and show it (2),” “I’d get annoyed but would keep it in (3),” “I’d get angry or mad but would keep it in (4),” and “I would not get angry, mad, or annoyed (5).” The guilt situation related to the participants’ felt guilt level if they expressed anger toward policeman/their spouse when they felt angry, with responses including, “I’d feel very guilty or sorry (4),” “I’d feel guilty or sorry (3),” “I’d feel slightly guilty or sorry (2),” and “I wouldn’t feel at all guilty or sorry (1).” Finally, the protest situation asked what the participant would most likely do if a policeman/their spouse got angry at them for no reason, with responses including “Just keep quiet (4),” “Just leave (3),” “Protest a little (2),” and “Protest strongly by doing or saying something (1).” Higher scores are believed to reflect a more suppressive anger-coping style, whereas lower scores represent a more expressive anger-coping response style across three types of responses (anger, guilt, and protest) and two situations (unfair attack by a partner or a police office).
This scale has been used in several previous studies and has shown predictive validity when related to a variety of health-related outcomes, including blood pressure (20), hypertension (27), and all-cause mortality (21,23). A full list of the items and response options are provided in Harburg et al.(23); however, unlike in previous studies (21,23), we did not dichotomize the individual item responses into “suppressive” and “expressive” options. Instead, we scored the anger-coping response style variable as a continuous variable by averaging standardized scores across the six items. Notably, all substantive results reported here replicated whether the scale was derived from the dichotomized or full items. The full six-item scale showed adequate internal reliability for both husbands (α = 0.67) and wives (α = 0.68).
Mortality
As described by Harburg et al. (23), mortality status was assessed using death certificates and medical reports from 1971/1972 until 1979. From 1979 until 2003, participants’ mortality status was assessed by screening local newspapers, contacting participants’ relatives, and data from the National Death Index. Participants not reported within the index were coded as alive. In 2003, of the original 384 participants from 1971/1972, 131 had died (40.18% of the study sample; 78 men, 53 women). The current study is the first to explore mortality risk in the 32-year follow-up data.
Data Analysis
In the current study, we specified a structural equation model using an APIM (24) to assess the association of spouses’ anger-coping responses styles and mortality status 32 years later. Our model included main effects from husbands’ and wives’ response styles, as well as the interaction of their styles predicting mortality status. We then included main effects from our covariates interest―age, smoking status, systolic blood pressure, and income―predicting husbands’ and wives’ mortality status, with each person’s covariates predicting their own mortality status. This specification allowed us to examine unique actor and partner effects, as well as an interaction effect in which spouses anger-coping styles operated together to predict mortality status. In addition, the current models address concerns with possible confounds with similarity effects that can occur in such analyses by predicting outcomes using an interaction term to represent match/mismatch (28). The final model is presented in Figure 1. We also evaluated these main outcomes when using a survival analysis (time to death) framework to ensure that our results were consistent when including time to death (rather than a binary mortality outcomes). To do so, we specified a Cox-frailty regression models within SAS. This method accounts for nonindependence within a survival analysis framework by using a random effect for the marital pair unit.
FIGURE 1.
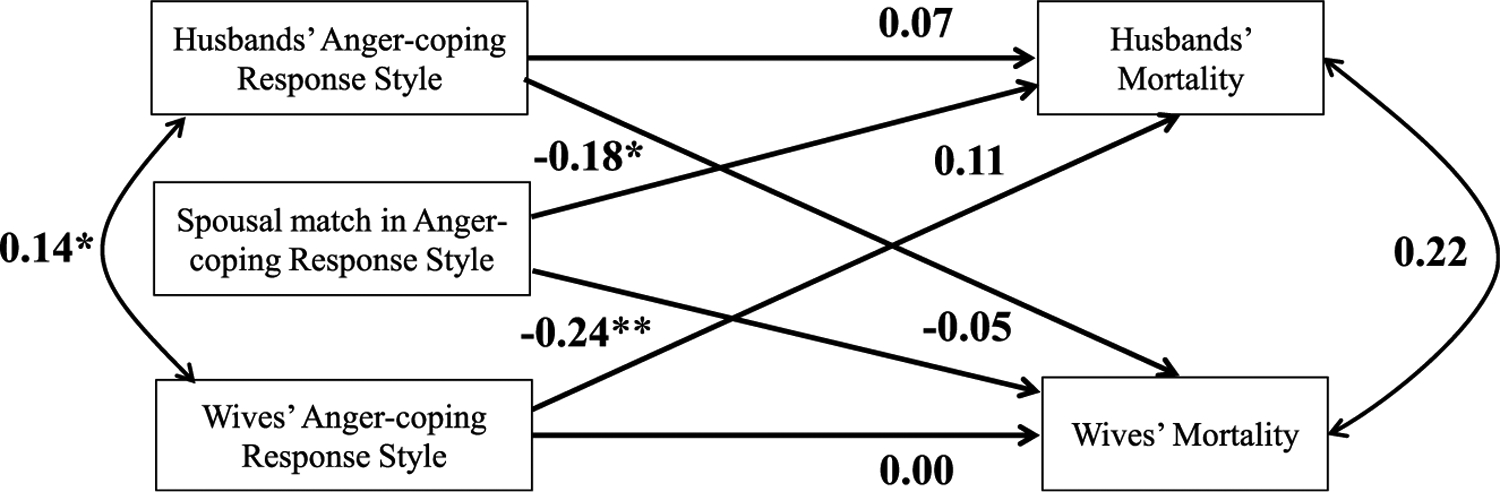
Structural equation model of the main APIM. Husbands’ and wives’ anger-coping response style actor and partner effects, as well as the interaction of the two, are predicting their mortality status 32 years later. The model also included associations from each spouses’ covariates. All estimates reported are standardized regression estimates. **p < .01, *p < .05.
We conducted our primary APIM analyses in Mplus Version 7.2 (29) using weighted least squares means and variance estimation and simultaneous regression. To assess model fit, we used the root-mean-square error of approximation and comparative fit index, in addition to χ2 tests. Estimates included standardized regression weights to allow for comparison between differently scaled predictors. The values represent the amount of a SD change in the outcome variable predicted by a 1 SD change in the predictor. The standardized values are calculated using the formula β = b × SD (x)/SD(y) for continuous predictors, and β = b/SD(y) for dichotomous variables (29).
RESULTS
Table 1 displays the descriptive statistics and correlation matrix of the variables used in the study.
TABLE 1.
Descriptive Statistics and Correlation Matrix for Study Variables
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Husband response style (1) | 1.00 | ||||||||||
| Wife response style (2) | 0.14 | 1.00 | |||||||||
| Husband mortality (3) | 0.08 | 0.05 | 1.00 | ||||||||
| Wife mortality (4) | −0.01 | −0.01 | 0.33 | 1.00 | |||||||
| Husband age (5) | 0.11 | 0.06 | 0.38 | 0.39 | 1.00 | ||||||
| Wife age (6) | 0.11 | 0.12 | 0.34 | 0.41 | 0.93 | 1.00 | |||||
| Husband smoking status (7) | −0.22 | −0.12 | 0.24 | −0.04 | −0.13 | −0.11 | 1.00 | ||||
| Wife smoking status (8) | −0.06 | −0.21 | 0.04 | 0.12 | −0.05 | −0.08 | 0.29 | 1.00 | |||
| Husband systolic BP (9) | −0.05 | −0.07 | 0.24 | 0.10 | 0.26 | 0.22 | 0.14 | 0.02 | 1.00 | ||
| Wife systolic BP (10) | −0.02 | 0.04 | 0.15 | 0.27 | 0.34 | 0.36 | −0.04 | −0.07 | 0.19 | 1.00 | |
| Income (11) | −0.06 | −0.17 | 0.02 | −0.24 | −0.43 | −0.41 | 0.12 | 0.11 | −0.11 | −0.18 | 1.00 |
| (N = 192) Mean | 2.33 | 2.35 | 40.6% | 27.6% | 49.08 | 46.62 | 2.02 | 1.56 | 80.82 | 75.26 | 8.94 |
| SD | 0.58 | 0.63 | 9.10 | 8.82 | 1.34 | 1.01 | 11.85 | 11.05 | 2.19 |
BP = blood pressure.
All values used weighted least squares means and variance for missing data. Both percentages for mortality are percent deceased.
Actor-Partner Interdependence Model
We first specified out APIM within Mplus. The model fit the data well, χ2 (6, N = 192) = 1.51, p = .96, comparative fit index = 1.00, root-mean-square error of approximation = .000. The full model results are reported in Table 2 and the primary APIM outcomes are presented in Figure 1. Of note, husbands’ and wives’ anger-coping response styles were significantly correlated, r = 0.14, p = .043, but husbands’ and wives’ mortality status in 2003 was not significantly correlated, r = 0.22, p = .14. Spouses’ anger-coping response styles—but not mortality risk—are correlated and nonindependent.
TABLE 2.
Model Results for the APIM
| Outcome: husband mortality (N = 192) | β | 95% CI | B |
|---|---|---|---|
| Husband response style | 0.07 | −0.10 to 0.23 | 0.13 |
| Wife response style | 0.12 | −0.07 to 0.31 | 0.19 |
| Husband by wife response style | −0.18* | −0.35 to −0.01 | −0.48* |
| Husband age | 0.50** | 0.32 to 0.68 | 0.06** |
| Husband smoking status | 0.29** | 0.10 to 0.48 | 0.22** |
| Husband systolic BP | 0.10 | −0.10 to 0.27 | 0.11 |
| Household income | 0.22* | 0.00 to 0.44 | 0.10* |
| Outcome: wife mortality (N = 192) | β | 95% CI | B |
| Husband response style | −0.05 | −0.23 to 0.13 | −0.09 |
| Wife response style | 0.00 | −0.18 to 0.18 | 0.00 |
| Husband by wife response style | −0.24* | −0.37 to −0.11 | −0.64** |
| Wife age | 0.37** | 0.18 to 0.56 | 0.05** |
| Wife smoking status | 0.16 | −0.01 to 0.33 | 0.16 |
| Wife systolic BP | 0.15 | −0.03 to 0.33 | 0.16 |
| Household income | −0.10 | −0.29 to 0.09 | −0.05 |
95% CI = 95% confidence interval; BP = blood pressure.
All analyses use simultaneous regression and full information likelihood estimation.
p < .05.
p < .01.
Neither husbands’ nor wives’ response styles predicted their mortality 32 years later, β = 0.07, 95% CI = −0.10 to 0.25, p = .41, β = 0.00, 95% CI = −0.18 to 0.18, p = .97. Husbands’ and wives’ response styles did not predict their partners’ later mortality status, β = −0.05, 95% CI = −0.23 to 0.13, p = .56, β = 0.12, 95% CI = −0.07 to 0.31, p = .221. However, we observed that wives’ response style significantly moderated the association of husbands’ response style on the risk for later mortality, β = −0.18, 95% CI = −0.35 to −0.01, p = .039. Similarly, husbands’ response style significantly moderated the association of wives’ response style and their later mortality, β = −0.24, 95% CI = −0.38 to −0.10, p < .001. The interaction effects explained an additional 3.5% and 5.5% of the variance in husbands’ and wives’ risk of mortality 32 years later when compared with the same model excluding the interaction effect.
Figure 2 illustrates the interaction effect for both men and women. The interaction for husbands and wives was such that spouses were at lower risk of later mortality if their response styles were more matched, whereas their risk increased as their response styles were more mismatched. For wives, there was a significant difference in mortality outcomes based on husbands’ anger-coping response styles when wives’ scores were greater than 3.81 points, which represents 1.6% of the sample. For husbands, there was a significant difference in mortality outcomes based on wives’ anger-coping response styles when husbands’ scores were less than 1.68 and greater than 3.79 points, which represents 14.6% and 1.0% of the sample, respectively. Table 3 provides the risk ratios for different combinations of husbands’ and wives’ anger-coping response styles.
FIGURE 2.
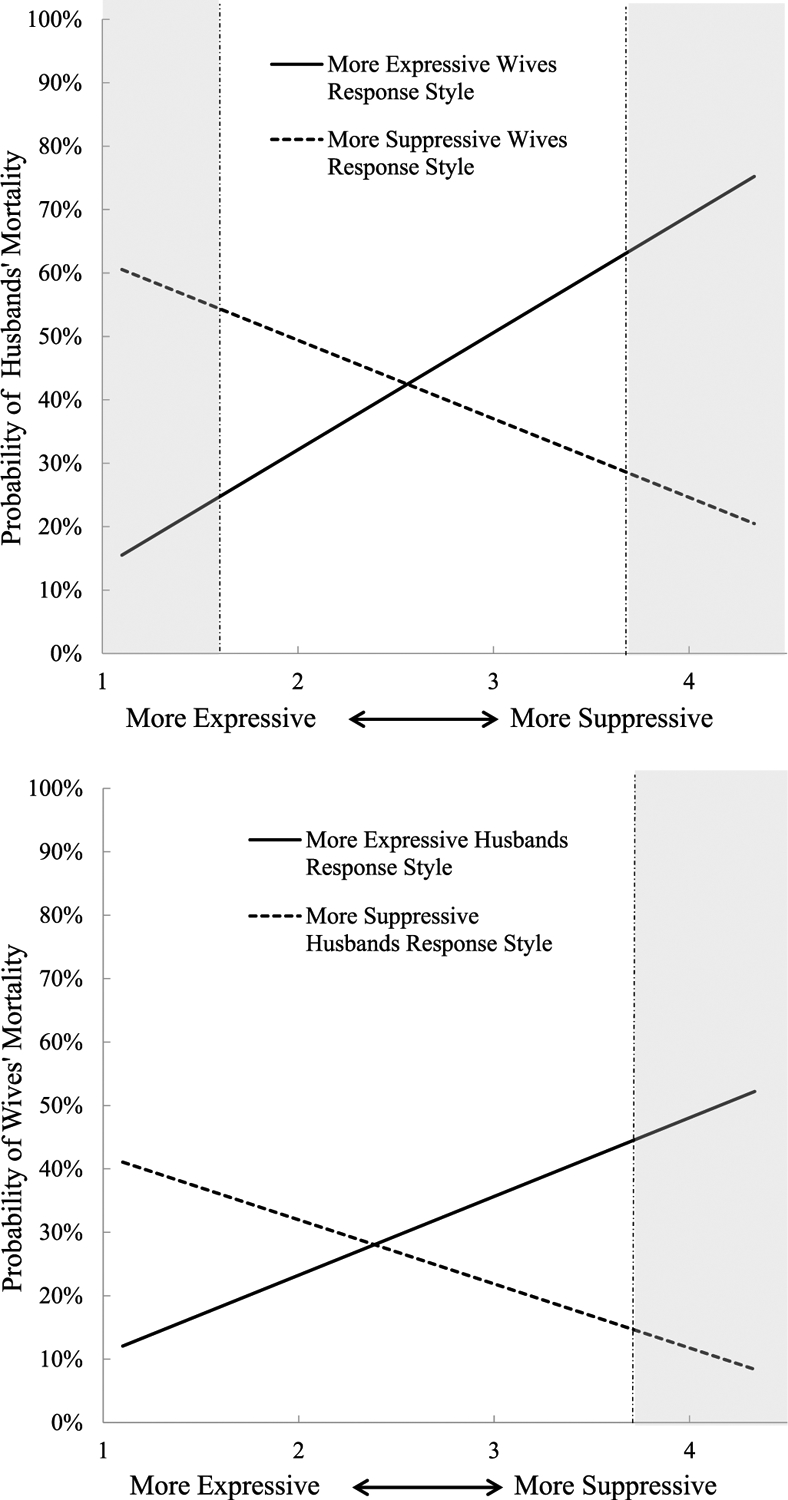
Visualization of the interaction of spouses’ anger-coping response styles predicting the percentage chance of husbands’ and wives’ death 32 years later. The two lines of best fit represent participant scores 1 SD below and 1 SD above the mean on the anger-coping response scale, corresponding to a more suppressive and expressive anger-coping response style. The shaded areas represent areas of significance, where the two lines of fit vary significantly at a p < .05 level.
TABLE 3.
Percent Mortality for Husbands’ and Wives’ Anger-Coping Response Style Levels
| Type of couple (N = 192) | Husbands’ mortality |
|---|---|
| Suppressive husband, suppressive wife | 35.5% |
| Suppressive husband, mean level wife | 41.7% |
| Suppressive husband, expressive wife | 48.8% |
| Mean level husband, suppressive wife | 43.3% |
| Mean level husband, mean level wife | 40.0% |
| Mean level husband, expressive wife | 36.1% |
| Expressive husband, suppressive wife | 51.5% |
| Expressive husband, mean level wife | 37.5% |
| Expressive husband, expressive wife | 25.4% |
| Type of couple (N = 192) | Wives’ mortality |
| Suppressive wife, suppressive husband | 18.3% |
| Suppressive wife, mean level husband | 24.6% |
| Suppressive wife, expressive husband | 35.6% |
| Mean level wife, suppressive husband | 22.8% |
| Mean level wife, mean level husband | 24.0% |
| Mean level wife, expressive husband | 25.8% |
| Expressive wife, suppressive husband | 28.1% |
| Expressive wife, mean level husband | 23.4% |
| Expressive wife, expressive husband | 17.9% |
All values reflect the actual mortality rates in the full sample. Suppressive and expressive husbands and wives are defined as people who are 1 SD above or below the mean level on the anger-coping response style scale.
We also evaluated whether there were differences in the main outcomes when using a survival analysis (time to death) framework. The results based on Cox-frailty regression were consistent with those of the APIM, and the results of the model are presented in survival curve form in Figure 3.
FIGURE 3.
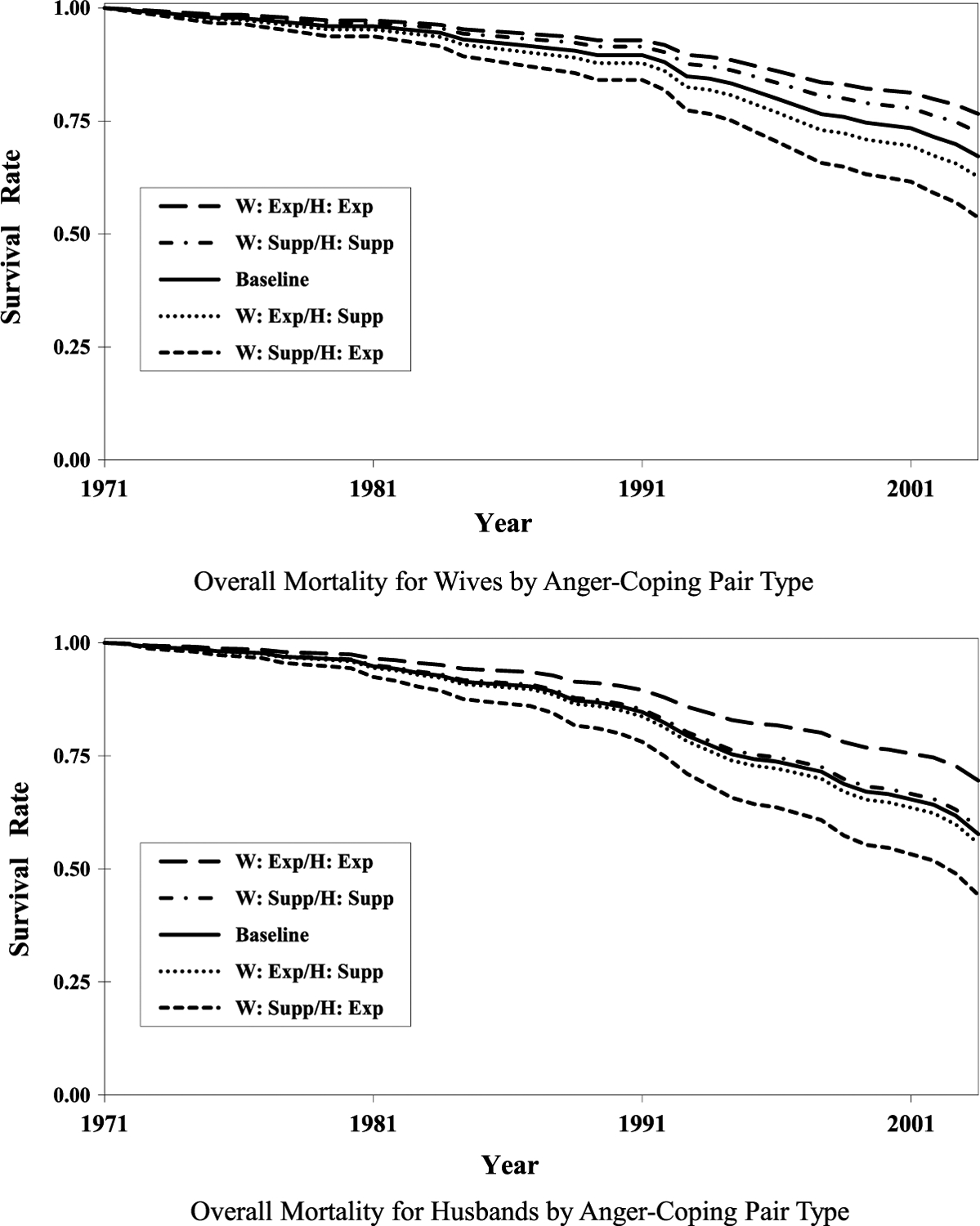
Survival curves for overall mortality by anger-coping pair types, adjusted for age, systolic blood pressure, respiratory risk, and smoking. Supp = suppressive; Exp = expressive; H = husband’s, W = wife’s.
DISCUSSION
Data from the LCES, a subsample from the TCHS, were collected in 1971/1972 and allowed for some of the first investigations of the ways in which emotion regulation differences between couples may be associated with later health outcomes. Harburg and colleagues (23) found that the interaction between spouses’ anger-coping response styles and health risk predicted 17-year mortality outcomes, and, in particular, that having both a suppressive husband and wife in the same couple predicted increased mortality compared with all other groups (21). Despite psychometric limitations due to the historical nature of the data, the current study applied contemporary data analytic methods to (a) extend this earlier work and examine whether the previous mortality risk findings held at a 32-year follow-up assessment and (b) examine whether more complex model specifications in which match/mismatch in spouses’ anger-coping response styles would predict subsequent risk. Using an APIM approach (24), we found no evidence for actor or partner effects predicting either husbands’ or wives’ mortality status, nor did we find evidence that a match in suppression coping styles was predictive of mortality at the 32-year follow-up. Rather, we found that greater mismatch in response styles significantly predicted increased risk of early mortality. These effects remained when accounting for a variety of relevant covariates―age, smoking status, systolic blood pressure, and income—and the substantive results replicated among both husbands and wives. In addition, these substantive findings were replicated when using survival analysis (time to death) models, providing additional support for the robustness of the results.
In couples with high levels of mismatch in anger-coping response style, it is possible that the ongoing interaction between partners fail to align with those partners’ preferences and/or expectations. If marriage is conceptualized as a Person × Environment fit (18,19), then mismatch in spouses’ expectations for behavior could result in increased conflict and negative interpersonal interactions, potentially evoking greater acute stress responses in the moment and increased experienced negative affect (22). If maintained for the long-term, these antecedent changes in affect and physiological reactivity may translate into increased interpersonal stress and lower marital quality, both of which contribute to poor health (5,30). It should be noted, however, that the evidence for the association between match and mismatch with dyadic outcomes is mixed. For example, previous investigations did not find strong associations between match in personality and well-being outcomes (31,32), which suggests that future investigations would benefit from alternative mediators that might explain the results of the current study beyond relationships quality or life satisfaction. It is possible that there might be specific subtypes of couples who are “mismatched” on this study’s measure of anger-coping response style but who share complementary styles that may not exhibit increased risk of early mortality compared with other “mismatched” couples when assessed on a full measure of the interpersonal circumplex (22).
The interaction of partner’s anger-coping response styles predicting mortality outcomes matches well with previous results from Harburg et al. (23), which found an interaction of bronchial problems and high blood pressure with a suppressive anger-coping response style predicting mortality risk in the larger LCES sample. Rather than simple main effects, it is the interaction of individual styles with an additional risk factor (e.g., a mismatch with a partner) that predicts mortality status. We note, however, that the assessment of anger-coping response styles—responding to vignettes imagining the way people believe they would react—may not correspond to expressed anger behavior, but instead likely assesses how people view their own responses to unfair or negative interpersonal stimuli. Although we conceptualize this work within interpersonal theory broadly, it important to note that contemporary investigations of the theory (e.g., (12,13,15,16)) primarily focus on the dual axes of dominance and affiliation, in contrast to the single axis in the anger-response style used in this study. Indeed, methods of measuring characteristics such as interpersonal match have advanced greatly in the time since the initial LCES data collection in the early 1970s. Future work examining match and mismatch within couples predicting long-term mortality would benefit from measurement that better matches current conceptualizations of interpersonal theory.
How can we explain the discrepancy in findings between earlier reports from this sample and those observed in the current study? Here, we find that the match or mismatch in partners’ anger-coping response styles, rather than a specific type of couple pairing (suppressive/suppressive, suppressive/expressive, expressive/expressive, etc.) was associated with the highest risk of early mortality, whereas previous reports found that it was primarily suppressive couples or individuals who were at the greatest risk (21,23). There are two possible methodological explanations for these discordant results. First, the act of dichotomizing people into either “suppressive” or “expressive” anger-coping response styles (as in the previous report) may explain the divergent results. Current analytic guidelines suggest that dichotomizing continuous predictors in multiple regression can lead to differences in outcomes and reduced power (33). In this respect, differences between the current and previous study may have emerged as a function of this dichotomization process. Second, we treated all covariates continuously in the current study, whereas they were dichotomized in previous investigations (23). We find that the dichotomization of age, in particular, may explain the differences between the findings, and the suppress/suppress couples were older on average compared with other groups (men: 53.0 to 48.5 years old; women: 50.7 to 46.0 years old). When age is treated continuously, the suppress/suppress combination does not seem to be as potent a predictor of mortality as mismatch at the 32-year follow-up. Regardless of the ultimate explanation, future studies assessing long-term mortality outcomes would benefit from assessing the interaction between characteristics, such as anger-coping response styles, within couples.
The results of the current study should be considered in the context of its limitations. First, although the study sample was drawn from a representative sample from the Tecumseh, Michigan area, it is possible the further selection of the LCES and the couples in the study altered the study so that it is not representative of that area or the United States broadly. Second, the current study did not assess observed behavior, and the self-reported assessments from the 1970s may not accurately represent the actual behaviors within couples that match or mismatch in terms of their anger-coping response style, or how their anger-coping response styles might change over time. Similarly, as mentioned previously, the primary scale used in the current style to assess anger-coping response style was developed and used in the 1970s. Although there is evidence for internal reliability and predictive validity for this scale (20,21,23,34), the scale was not created using contemporary psychometric standards. Third, the current study did not assess the marital relationships or other potential mediators that might explain how self-reported anger-coping response style might affect people’s long-term health. For example, it is possible that measures of marital quality could either moderate or mediate the association of anger-coping response styles and later mortality status. Unfortunately, we are unable to include measures of marital quality in this study, as this data was not collected in the original study. Any long-term follow-up study must contend with inherent measurement limitations in the baseline sample, and the knowledge gains of the study must be balanced against these limitations in measurement.
CONCLUSIONS
Using data from 192 couples collected during a previous assessment in the early 1970s, the current study assessed whether married spouses’ anger-coping response styles predicted their risk of early death. The APIMs used in the current study did not support significant associations between husbands’ or wives’ anger-coping response styles of their or their partner’s mortality status. There was, however, a significant association between the interactions of spouses’ anger-coping response style predicting mortality status. Greater mismatch between spouses’ styles was associated with increased risk of early death, whereas greater match was associated with less risk of early death for both husbands and wives. These results suggest that interpersonal match in characteristics such as anger-coping response styles between spouses can predict meaningful long-term health outcomes.
Source of Funding and Conflicts of Interest:
The second author’s work on this article was supported by a grant from the National Institute of Child Health and Human Development (HD069498). The authors report no conflicts of interest.
Glossary
- APIM
actor-partner interdependence model
- LCES
Life Change Event Study
- TCHS
Tecumseh Community Health Study
REFERENCES
- 1.Sbarra DA, Coan JA. Relationships and health: the critical role of affective science. Emot Rev 2018;10:40–54. [Google Scholar]
- 2.Holt-Lunstad J, Smith TB, Layton JB. Social relationships and mortality risk: a meta-analytic review. PLoS Med 2010;7:e1000316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Holt-Lunstad J, Robles TF, Sbarra DA. Advancing social connection as a public health priority in the United States. Am Psychol 2017;72:517–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, Graham I. 2016 European guidelines on cardiovascular disease prevention in clinical practice: the sixth joint task force of the European Society of Cardiology and Other Societies on cardiovascular disease prevention in clinical practice. Eur Heart J 2016;37:2315–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Robles TF, Slatcher RB, Trombello JM, McGinn MM. Marital quality and health: a meta-analytic review. Psychol Bull 2014;140:140–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ruiz JM, Hutchinson JG, Terrill A. For better and worse: social influences on coronary heart disease. Soc Pers Psychol Compass 2008;2:1400–14. [Google Scholar]
- 7.Coyne JC, Rohrbaugh MJ, Shoham V, Sonnega JS, Nicklas JM, Cranford JA. Prognostic importance of marital quality for survival of congestive heart failure. Am J Cardiol 2001;88:526–9. [DOI] [PubMed] [Google Scholar]
- 8.Slatcher RB, Schoebi D. Protective processes underlying the links between marital quality and physical health. Curr Opin Psychol 2017;13:148–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kiesler DJ. Contemporary Interpersonal Theory and Research: Personality, Psychopathology, and Psychotherapy. New York: John Wiley & Sons; 1996. [Google Scholar]
- 10.Ruiz JM, Hamann HA, Coyne J, Compare A. In sickness and in health: interpersonal risk and resilience in cardiovascular disease. In: Molinari E, Compare A, Parati G, editors. Clinical Psychology and Heart Disease. New York: Springer; 2006:233–72. [Google Scholar]
- 11.Sullivan HS. The Interpersonal Theory of Psychiatry. New York, NY: Norton; 1953. [Google Scholar]
- 12.Smith TW, Ruiz JM, Cundiff JM, Baron KG, Nealey-Moore JB. Optimism and pessimism in social context: an interpersonal perspective on resilience and risk. J Res Pers 2013;47:553–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Smith TW, Baucom BRW. Intimate relationships, individual adjustment, and coronary heart disease: implications of overlapping associations in psychosocial risk. Am Psychol 2017;72:578–89. [DOI] [PubMed] [Google Scholar]
- 14.Pincus AL, Ansell EB. Interpersonal theory of personality. In: Millon T, Lerner MJ, editors. Handbook of Psychology: Personality and Social Psychology vol. 5. New York, NY: Wiley; 2003:209–29. [Google Scholar]
- 15.Smith TW, Glazer K, Ruiz JM, Gallo LC. Hostility, anger, aggressiveness, and coronary heart disease: an interpersonal perspective on personality, emotion, and health. J Pers 2004;72:1217–70. [DOI] [PubMed] [Google Scholar]
- 16.Smith TW, Baron CE, Grove JL. Personality, emotional adjustment, and cardiovascular risk: marriage as a mechanism. J Pers 2014;82:502–14. [DOI] [PubMed] [Google Scholar]
- 17.Sadler P, Ethier N, Woody E. Interpersonal complementarity. In: Horowitz LM, Strack S, editors. Handbook of Interpersonal Psychology: Theory Research Assessment and Therapeutic Interventions. Hoeboken, NJ: Wiley; 2011:123–42. [Google Scholar]
- 18.Cundiff JM, Smith TW, Butner J, Critchfield KL, Nealey-Moore J. Affiliation and control in marital interaction: interpersonal complementarity is present but is not associated with affect or relationship quality. Pers Soc Psychol Bull 2015;41:35–51. [DOI] [PubMed] [Google Scholar]
- 19.Ruiz JM, Matthews KA, Scheier MF, Schulz R. Does whom you marry matter for your health? Influence of patient’s and spouse’s personality on their partner’s psychological well-being following coronary artery bypass surgery. J Pers Soc Psychol 2006;91:255–67. [DOI] [PubMed] [Google Scholar]
- 20.Harburg E, Erfurt JC, Hauenstein LS, Chape C, Schull WJ, Schork MA. Socioecological stress, suppressed hostility, skin color, and black-white male blood pressure: Detroit. Psychosom Med 1973;35:276–96. [DOI] [PubMed] [Google Scholar]
- 21.Harburg E, Kaciroti N, Gleiberman L, Julius M, Schork MA. Marital pair anger-coping types may act as an entity to affect mortality: preliminary findings from a prospective study (Tecumseh, Michigan, 1971–1988). J Fam Commun 2008;8:44–61. [Google Scholar]
- 22.Smith JL, Ruiz JM. Interpersonal orientation in context: interpersonal circumplex and five-factor model correlates and effects of social match and mismatch on intrinsic motivation and cardiovascular responses. J Pers 2007;75:679–708. [DOI] [PubMed] [Google Scholar]
- 23.Harburg E, Julius M, Kaciroti N, Gleiberman L, Schork AM. Expressive/suppressive anger-coping responses, gender, and types of mortality: a 17-year follow-up (Tecumseh, Michigan, 1971–1988). Psychosom Med 2003;65:588–97. [DOI] [PubMed] [Google Scholar]
- 24.Cook WL, Kenny DA. The actor–partner interdependence model: a model of bidirectional effects in developmental studies. Int J Behav Dev 2005;29:101–9. [Google Scholar]
- 25.Napier JA, Johnson BC, Epstein FH. The Tecumseh Michigan Community Health Study. The Community as an Epidemiologic Laboratory: A Casebook of Community Studies. Baltimore, MD: The Johns Hopkins University Press; 1970. [Google Scholar]
- 26.Hawthorne V. Tecumseh Community Health Study. ICPSR08969-v1. Ann Arbor, MI: Inter-university Consortium for Political and Social Research; [distributor]; 1989. [Google Scholar]
- 27.Gentry DW, Chesney AP, Gary HE Jr., Hall RP, Harburg E. Habitual anger-coping styles: I. effect on mean blood pressure and risk for essential hypertension. Psychosom Med 1982;44:195–202. [DOI] [PubMed] [Google Scholar]
- 28.Wood D, Furr RM. The correlates of similarity estimates are often misleadingly positive: the nature and scope of the problem, and some solutions. Pers Soc Psychol Rev 2016;20:79–99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Muthén LK, Muthén BO. Mplus User’s Guide. 7th ed. Los Angeles, CA: Muthén & Muthén; 1998–2012. [Google Scholar]
- 30.Thoits PA. Stress and health: major findings and policy implications. J Health Soc Behav 2010;51:S41–53. [DOI] [PubMed] [Google Scholar]
- 31.Dyrenforth PS, Kashy DA, Donnellan MB, Lucas RE. Predicting relationship and life satisfaction from personality in nationally representative samples from three countries: the relative importance of actor, partner, and similarity effects. J Pers Soc Psychol 2010;99:690–702. [DOI] [PubMed] [Google Scholar]
- 32.Furler K, Gomez V, Grob A. Personality similarity and life satisfaction in couples. J Res Pers 2013;47:369–75. [Google Scholar]
- 33.Royston P, Altman DG, Sauerbrei W. Dichotomizing continuous predictors in multiple regression: a bad idea. Stat Med 2006;25:127–41. [DOI] [PubMed] [Google Scholar]
- 34.Julius M, Harburg E, Cottington EM, Johnson EH. Anger-coping types, blood pressure, and all-cause mortality: a follow-up in Tecumseh, Michigan (1971–1983). Am J Epidemiol 1986;124:220–33. [DOI] [PubMed] [Google Scholar]