

Abstract
Asthma is a chronic inflammatory disease of the airways affecting people of all ages. The disease is characterised by a variable narrowing of the bronchia, which may be accompanied by symptoms such as wheezing or shortness of breath. In GEDA 2014/2015-EHIS, 6.2% of respondents aged 18 years or older with complete information on the respective indicator (n=22,671) reported having had asthma during the past 12 months. The 12-month prevalence among women (7.1%) is higher than among men (5.4%). Overall, women and men with a low level of education more often reported having had asthma than those with a higher level of education. In analyses stratified by age and gender, differences in asthma prevalence with regard to educational level are evident among women under 30 years of age. In a comparison of federal states, the prevalence of asthma ranges from 3.0% to 9.7% among women and from 2.9% to 7.0% among men.
Keywords: ASTHMA, PREVALENCE, ADULTS, HEALTH MONITORING, GERMANY
Introduction
According to the World Health Organization (WHO), asthma is one of the most common chronic diseases affecting around 235 million people globally [1]. Asthma can occur among people of all ages [2-5]. The disease is characterised by chronic inflammation and increased sensitivity (hyperresponsiveness) of the airways to diverse inhaled stimuli [5, 6]. Asthma patients moreover suffer from variable narrowing of the bronchia (airway obstruction) accompanied by symptoms such as wheezing, shortness of breath, chest tightness or coughing which vary over time and in intensity [5, 6]. Some patients with mild asthma may experience periods when they are completely free of symptoms [5, 7]. In particular, in case of an asthma onset in childhood, remission of symptoms during puberty is frequently observed [4, 8].
Asthma is a heterogeneous disease which results from different underlying disease mechanisms [5, 9]. Allergic asthma and also other forms of non-allergic asthma are marked by a characteristic type of inflammation [5, 9]. This (TH2) type of inflammation is indicated by elevated concentrations of specific immune cells (eosinophils) in the airway mucosa and in the blood (eosinophilic asthma) [5, 6, 9]. Further, mainly adult-onset, forms of asthma exist, where such an overproduction of eosinophils cannot be observed (non-eosinophilic asthma) [5, 6, 9]. It is important to distinguish between eosinophilic and non-eosinophilic asthma, when treating patients with severe asthma [5, 6, 9].
A family history of asthma or of certain allergies (such as hay fever) is an important predisposing factor [5, 10-12]. Asthma thereby results from complex interactions between genetic and environmental factors [2, 5, 12]. Early childhood yet also prenatal influences are highly relevant in the induction of the disease [2, 5, 12]. Infections, exposure to microbes, pollutants and allergens, but also diet or psychosocial factors may contribute to asthma development [2, 5, 12]. Furthermore, occupational exposures have been identified (e.g., allergens such as flour and cow hair or chemical irritants such as disinfectants and agents used by hairstylists) which can induce or aggravate asthma in adulthood [2, 13]. Providing appropriate medical care to asthma patients is highly important to prevent episodes in which the disease worsens acutely and which can require emergency care or lead to premature mortality [5]. In the majority of patients, however, adequate treatment can minimise the symptoms of asthma and associated limitations in usual activities [5].
GEDA 2014/2015-EHIS.
Data holder: Robert Koch Institute
Aims: To provide reliable information about the population’s health status, health-related behaviour and health care in Germany, with the possibility of a European comparison
Method: Questionnaires completed on paper or online
Population: People aged 18 years and above with permanent residency in Germany
Sampling: Registry office sample; randomly selected individuals from 301 communities in Germany were invited to participate
Participants: 24,016 people (13,144 women; 10,872 men)
Response rate: 26.9%
Study period: November 2014 - July 2015
Data protection: This study was undertaken in strict accordance with the data protection regulations set out in the German Federal Data Protection Act and was approved by the German Federal Commissioner for Data Protection and Freedom of Information. Participation in the study was voluntary. The participants were fully informed about the study’s aims and content, and about data protection. All participants provided written informed consent.
More information in German is available at
Indicator
In the GEDA 2014/2015-EHIS survey, the prevalence of asthma during the past 12 months was assessed by using a self-administered paper-based or online questionnaire. Respondents were asked, ‘During the past 12 months, have you had any of the following diseases or conditions?’ This question was followed by a list of conditions that also contained ‘asthma (allergic asthma included)’. 24,016 adults aged 18 years or older (13,144 women and 10,872 men) participated in GEDA 2014/2015-EHIS. 1,345 respondents (696 women and 649 men) with missing information on the indicator on self-assessed asthma were excluded from the current analysis. The calculations were carried out using a weighting factor that corrects for deviations within the sample from the German population structure (as of 31 December 2014) with regard to gender, age, district type and education. The district type reflects the degree of urbanisation and corresponds to the regional distribution in Germany. The International Standard Classification of Education (ISCED) was used to classify the responses provided on educational level [14]. Lange et al. [15] set out the details of the methodology applied in the GEDA 2014/2015-EHIS study including the method used to calculate the weighting factor and an assessment of the response rate. Background information on the GEDA 2014/15-EHIS is also provided in the article German Health Update: New data for Germany and Europe in Issue 1/2017 of the Journal of Health Monitoring.
Results and discussion
6.2% of adults aged 18 years or older reported having had asthma during the past 12 months. Overall, women (7.1%) show a higher 12-month prevalence of asthma than men (5.4%) (Table 1). Asthma prevalence is highest in the age group 45 to 64 years among men while it remains on a similar level across all age groups among women. Overall, women and men with a low level of education more frequently reported to have had asthma than those with a medium or high level of education (7.7% vs. 5.9% and 5.7%). In analyses stratified by age and gender, these differences with regard to educational level are evident among women aged 18 to 29 years (Table 1). Prevalence estimates vary considerably between federal states ranging from 3.0% in Mecklenburg Western-Pomerania to 9.7% in Brandenburg among women and from 2.9% in Saxony-Anhalt to 7.0% in North Rhine Westphalia and Saarland among men (Figure 1).
Table 1.
12-month prevalence of asthma by gender, age and educational level (n=12,448 women; n=10,223 men)
Source: GEDA 2014/2015-EHIS
| Women | % | (95% CI) | Men | % | (95% CI) |
|---|---|---|---|---|---|
| Women total | 7.1 | (6.5-7.7) | Men total | 5.4 | (4.8-5.9) |
| 18-29 Years | 7.8 | (6.4-9.6) | 18-29 Years | 3.6 | (2.7-4.7) |
| Low education | 13.3 | (8.9-19.4) | Low education | 4.1 | (2.1-7.7) |
| Medium education | 6.5 | (5.1-8.2) | Medium education | 2.9 | (2.0-4.1) |
| High education | 5.2 | (3.3-8.2) | High education | 5.8 | (3.5-9.5) |
| 30-44 Years | 6.4 | (5.4-7.6) | 30-44 Years | 5.1 | (4.1-6.4) |
| Low education | 8.5 | (5.4-13.1) | Low education | 7.3 | (4.1-12.6) |
| Medium education | 6.1 | (4.8-7.6) | Medium education | 4.4 | (3.1-6.1) |
| High education | 6.2 | (4.8-8.0) | High education | 5.7 | (4.0-8.1) |
| 45-64 Years | 7.1 | (6.3-8.0) | 45-64 Years | 6.3 | (5.4-7.2) |
| Low education | 7.0 | (5.0-9.6) | Low education | 8.5 | (5.8-12.3) |
| Medium education | 7.1 | (6.1-8.4) | Medium education | 6.6 | (5.3-8.1) |
| High education | 7.2 | (5.8-8.8) | High education | 5.0 | (4.0-6.2) |
| ≥ 65 Years | 7.1 | (6.1-8.4) | ≥ 65 Years | 5.5 | (4.5-6.7) |
| Low education | 7.3 | (5.6-9.5) | Low education | 8.0 | (5.3-11.9) |
| Medium education | 6.7 | (5.2-8.5) | Medium education | 5.3 | (3.9-7.0) |
| High education | 6.9 | (4.7-10.1) | High education | 4.8 | (3.4-6.7) |
| Total (women and men) | 6.2 | (5.8-6.7) | Total (women and men) | 6.2 | (5.8-6.7) |
CI=Confidence interval
* n=51 additional missing values (26 women, 25 men) when stratifying by educational level
Figure 1.
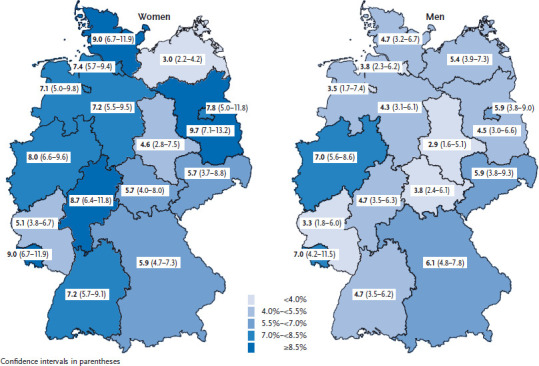
12-month prevalence of asthma by gender and federal state (n=12,448 women; n=10,223 men)
Source: GEDA 2014/2015-EHIS
The current results on the 12-month prevalence of asthma in GEDA 2014/2015-EHIS are consistent with results of the German national telephone health interview survey German Health Update (GEDA 2012) conducted by the Robert Koch Institute in 2012 [16]. This applies both to the overall prevalence of asthma among adults (6.2% vs. 6.3% in 2012) and to estimates by gender (women: 7.1% vs. 7.5%; men: 5.4% vs. 5.0%) [16]. Comparable differences between genders (an overall 1.3 to 1.5-fold higher prevalence of asthma among women) were observed in epidemiological surveys in Europe, Australia and the USA [17]. Results from longitudinal studies moreover point to an increased asthma risk for women relative to men, whereby this difference is already evident in adolescence (see also the Focus article on respiratory diseases in this issue) [17, 18]. Regarding socio-economic differences, the surveys available revealed heterogeneous results. Overall, in the majority of studies, however, a higher prevalence of asthma is related to lower social status [19]. A comparison of GEDA 2014/2015-EHIS results by gender or socio-economic criteria needs to consider further aspects. Differences in the way patients perceive symptoms, seek medical care or adhere to treatment recommendations - and resulting differences in the degree of treatment and asthma control - may all affect levels of self-reported asthma prevalence [20, 21].
Direct comparisons of prevalence estimates obtained from GEDA 2014/2015-EHIS with those obtained from previous German national health surveys need to consider some change in methods and hence preclude analyses of trends in asthma prevalence over time [16, 22-24]. In accordance with the regulation on the harmonisation of European health reporting, GEDA 2014/2015-EHIS used self-reported information on asthma prevalence based on the self-assessment of respondents. As in other large epidemiological surveys [25-34], all national health surveys previously conducted in Germany, starting with the German Health Interview and Examination Survey 1997-1999 (GNHIES98) [16, 22-24], however, collected data on self-reported physician-diagnosed asthma. In comparison with the currently applied indicator on self-assessed asthma, prior results on the prevalence of physician-diagnosed asthma may be less prone to misclassification [32]. In addition, previous national health surveys also assessed the lifetime prevalence of physician-diagnosed asthma which was consistently higher than the recorded 12-month prevalence [16, 22-24]. These differences between lifetime and 12-month prevalence indicate the varying degrees of disease activity over time in individuals with asthma [4, 7, 8]. In some patients, symptoms of asthma may resolve, at least for longer periods of time [4, 7, 8].
In Germany, an increase in the lifetime prevalence of physician-diagnosed asthma was recorded for both genders among adults (1997-1999 and 2008-2011) as well as among children and adolescents (2003-2006 and 2009-2012) [22-24]. At the same time, an increment in the 12-month prevalence was likewise observed; among adults this was attributable mainly to an increase in the prevalence among women [23, 35]. Interview survey data had already indicated a rising prevalence of asthma in the 1990s in Germany especially among children [26, 29, 36-40]. Moreover, an increase in the prevalence of asthma was also observed in other parts of the world during the second half of the last century [29]. Recent data indicates that this trend has come to a halt at least in certain regions such as Australia where prevalence is already high [25, 29, 41]. Among adults, however, a further increase in prevalence over the course of the last decade has nonetheless been recorded in several countries in Europe and in the USA [27, 28, 31, 33, 42].
High regional variation in asthma prevalence has been observed not only in GEDA 2014/2015-EHIS based on analyses stratified by federal state. Using ambulatory health care data, a recent study reported considerable variation in asthma prevalence at the county level ranging from 2.5% to 7.7% for the total population [43]. Earlier European surveys indicated significant regional differences with a high prevalence mainly in the United Kingdom and low prevalence in Eastern European regions [2, 3, 44, 45]. In line with Europe-wide data for adults [2, 46], current asthma prevalence in Germany as recorded in GEDA 2014/2015-EHIS is mid-range compared to other countries of the EU. Previous studies including a national health survey of adults in Germany indicated a lower prevalence of asthma in East than in West Germany [47-51]. The German Health Interview and Examination Survey for Children and Adolescents (KiGGS) 2003-2006, however, which was conducted among children and adolescents most of whom were born after German reunification, revealed no significant differences between East (including Berlin) and West Germany [24]. Future investigations on the regional differences in asthma prevalence among adults in Germany should thus include in-depth analyses that do not only stratify by age and birth year, respectively, but also consider the place where respondents were born and raised.
Previously observed temporal and regional differences in asthma prevalence were related to the development of time trends and the geographical distribution of several lifestyle and environmental factors [12, 29, 50]. In addition, the influence of temporal changes and regional differences in degrees of awareness and provision of care, respectively, was also discussed [27, 29, 43, 50]. The recently observed changes in asthma prevalence over time point to the importance of continuous health monitoring based on periodically repeated national health surveys using comparable instruments of data collection. Besides extending the available database from national health interview and examination surveys permitting analyses of trends in the prevalence of physician-diagnosed asthma, it will be highly important to build a reliable database for the analysis of trends in self-assessed asthma prevalence using the current indicator in the context of European health interview surveys. Moreover, clarifying the underlying causes of regional and gender-specific differences in the prevalence of asthma remains a key challenge [12].
Key statements
About 6% of adults reported having had asthma during the past 12 months.
Women (7.1%) show a higher 12-month prevalence of asthma than men (5.4%).
In a comparison of federal states, the prevalence of asthma ranges from 3.0% to 9.7% among women and from 2.9% to 7.0% among men.
Funding Statement
The GEDA study was funded by the Robert Koch Institute and the German Federal Ministry of Health.
Footnotes
Conflicts of interest
The authors declared no conflicts of interest.
Disclaimer
Note: External contributions do not necessarily reflect the opinions of the Robert Koch Institute
References
- 1.World Health Organization (2017) Asthma. Fact sheet. Updated April 2017. http://www.who.int/mediacentre/factsheets/fs307/en/ (As at 27.07.2017)
- 2.European Respiratory Society (2013) Major respiratory diseases - adult asthma. In: Gibson J, Loddenkemper R, Sibille Y, et al. (eds) The European Lung White Book - Respiratory Health and Disease in Europe. European Respiratory Society, Sheffield [Google Scholar]
- 3.European Respiratory Society (2013) Major respiratory diseases - childhood asthma. In: Gibson J, Loddenkemper R, Sibille Y, et al. (eds) The European Lung White Book - Respiratory Health and Disease in Europe. European Respiratory Society, Sheffield [Google Scholar]
- 4.Fuchs O, Bahmer T, Rabe KF, et al. (2017) Asthma transition from childhood into adulthood. Lancet Respir Med 5(3):224-234 [DOI] [PubMed] [Google Scholar]
- 5.Global Initiative for Asthma (GINA) (2017) Global Strategy for Asthma Management and Prevention. www.ginasthma.org (As at 03.08.2017)
- 6.Gillissen A, Welte T. (eds) (2014) Weißbuch Lunge 2014 – Herausforderungen, Zukunftsperspektiven, Forschungsansätze – Zur Lage und Zukunft der Pneumologie in Deutschland. Frisch Texte Verlag, Herne [Google Scholar]
- 7.Aaron SD, Vandemheen KL, FitzGerald JM, et al. (2017) Reevaluation of Diagnosis in Adults With Physician-Diagnosed Asthma. JAMA 317(3):269-279 [DOI] [PubMed] [Google Scholar]
- 8.Upham JW, James AL. (2011) Remission of asthma: The next therapeutic frontier? Pharmacol Ther 130(1):38-45 [DOI] [PubMed] [Google Scholar]
- 9.Wenzel SE. (2012) Asthma phenotypes: the evolution from clinical to molecular approaches. Nat Med 18(5):716-725 [DOI] [PubMed] [Google Scholar]
- 10.Grabenhenrich LB, Gough H, Reich A, et al. (2014) Early-life determinants of asthma from birth to age 20 years: a German birth cohort study. J Allergy Clin Immunol 133(4):979-988 [DOI] [PubMed] [Google Scholar]
- 11.Schafer T, Bauer CP, Beyer K, et al. (2014) S3-Guideline on allergy prevention: 2014 update: Guideline of the German Society for Allergology and Clinical Immunology (DGAKI) and the German Society for Pediatric and Adolescent Medicine (DGKJ). Allergo J Int 23(6):186-199 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Jarvis D. (2014) Asthma and rhinitis. In: Annesi-Maesano I, Lundbäck B, Viegi G, et al. (eds) Respiratory epidemiology. European Respiratory Society, Sheffield [Google Scholar]
- 13.Baur X. (2011) Obstructive airway disorders representing occupational diseases. Pneumologie 65(11):654-661 [DOI] [PubMed] [Google Scholar]
- 14.Eurostat (2016) International standard classification of education (ISCED). http://ec.europa.eu/eurostat/statistics-explained/index.php/Glossary:International_standard_classification_of_education_%28ISCED%29 (As at 01.03.2017)
- 15.Lange C, Finger JD, Allen J, et al. (in press) Implementation of the European Health Interview Survey (EHIS) in Germany. Further development of the German Health Update (GEDA). Archives of Public Health; [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Robert Koch-Institut (2014) Daten und Fakten: Ergebnisse der Studie “Gesundheit in Deutschland aktuell 2012”. Beiträge zur Gesundheitsberichterstattung des Bundes. RKI, Berlin: http://edoc.rki.de/documents/rki_fv/recJuHnzacx8A/PDF/28GsWuNtFjVqY.pdf (As at 27.07.2017) [Google Scholar]
- 17.Zemp E, Hansen S, Schneider C, et al. (2014) Sex, gender and respiratory health. In: Annesi-Maesano I, Lundbäck B, Viegi G, et al. (eds) Respiratory epidemiology. European Respiratory Society, Sheffield [Google Scholar]
- 18.Vink NM, Postma DS, Schouten JP, et al. (2010) Gender differences in asthma development and remission during transition through puberty: the TRacking Adolescents’ Individual Lives Survey (TRAILS) study. J Allergy Clin Immunol 126(3):498-504 e491-496 [DOI] [PubMed] [Google Scholar]
- 19.Uphoff E, Cabieses B, Pinart M, et al. (2015) A systematic review of socioeconomic position in relation to asthma and allergic diseases. Eur Respir J 46(2):364-374 [DOI] [PubMed] [Google Scholar]
- 20.Mielck A, Reitmeir P, Wjst M. (1996) Severity of childhood asthma by socioeconomic status. Int J Epidemiol 25(2):388-393 [DOI] [PubMed] [Google Scholar]
- 21.Zein JG, Erzurum SC. (2015) Asthma is Different in Women. Curr Allergy Asthma Rep 15(6):28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Langen U, Schmitz R, Steppuhn H. (2013) Prevalence of allergic diseases in Germany: results of the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsbl Gesundheitsforsch Gesundheitsschutz 56(5-6):698-706 http://edoc.rki.de/oa/articles/reUsXePiiZFs/PDF/29PNwFWSiGnGA.pdf (As at 27.07.2017) [DOI] [PubMed] [Google Scholar]
- 23.Schmitz R, Thamm M, Ellert U, et al. (2014) Verbreitung häufiger Allergien bei Kindern und Jugendlichen in Deutschland – Ergebnisse der KiGGS-Studie – Erste Folgebefragung (KiGGS Welle 1). Bundesgesundheitsbl Gesundheitsforsch Gesundheitsschutz 57(7):771-778 https://edoc.rki.de/oa/articles/reanlTxmpPiBk/PDF/27CDfhKBFstMs.pdf (As at 01.03.2017) [DOI] [PubMed] [Google Scholar]
- 24.Schlaud M, Atzpodien K, Thierfelder W. (2007) Allergische Erkrankungen – Ergebnisse aus dem Kinder- und Jugendgesundheitssurvey (KiGGS). Bundesgesundheitsbl Gesundheitsforsch Gesundheitsschutz 50(5-6):701-710 https://edoc.rki.de/oa/articles/reRhnrND9xOGA/PDF/27Kp0kRUqJI.pdf (As at 01.03.2017) [DOI] [PubMed] [Google Scholar]
- 25.Australian Centre for Asthma Monitoring (2011) Asthma in Australia 2011: with a focus chapter on chronic obstructive pulmonary disease. AIHW Asthma Series no. 4. Cat. no. ACM 22. Australian Institute of Health and Welfare, Canberra [Google Scholar]
- 26.Bergmann KC, Heinrich J, Niemann H. (2016) Current status of allergy prevalence in Germany: Position paper of the Environmental Medicine Commission of the Robert Koch Institute. Allergo J Int 25:6-10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bjerg A, Ekerljung L, Middelveld R, et al. (2011) Increased prevalence of symptoms of rhinitis but not of asthma between 1990 and 2008 in Swedish adults: comparisons of the ECRHS and GA(2)LEN surveys. PLoS One 6(2):e16082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.de Marco R, Cappa V, Accordini S, et al. (2012) Trends in the prevalence of asthma and allergic rhinitis in Italy between 1991 and 2010. Eur Respir J 39(4):883-892 [DOI] [PubMed] [Google Scholar]
- 29.Eder W, Ege MJ, von Mutius E. (2006) The asthma epidemic. N Engl J Med 355(21):2226-2235 [DOI] [PubMed] [Google Scholar]
- 30.Hohmann C, Pinart M, Tischer C, et al. (2014) The development of the MeDALL Core Questionnaires for a harmonized follow-up assessment of eleven European birth cohorts on asthma and allergies. Int Arch Allergy Immunol 163(3):215-224 [DOI] [PubMed] [Google Scholar]
- 31.Kainu A, Pallasaho P, Piirila P, et al. (2013) Increase in prevalence of physician-diagnosed asthma in Helsinki during the Finnish Asthma Programme: improved recognition of asthma in primary care? A cross-sectional cohort study. Prim Care Respir J 22(1):64-71 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kilpelainen M, Terho EO, Helenius H, et al. (2001) Validation of a new questionnaire on asthma, allergic rhinitis, and conjunctivitis in young adults. Allergy 56(5):377-384 [DOI] [PubMed] [Google Scholar]
- 33.Moorman JE, Akinbami LJ, Bailey CM, et al. (2012) National Surveillance of Asthma: United States, 2001-2010. Vital and Health Statistics. National Center for Health Statistics [PubMed] [Google Scholar]
- 34.Sembajwe G, Cifuentes M, Tak SW, et al. (2010) National income, self-reported wheezing and asthma diagnosis from the World Health Survey. Eur Respir J 35(2):279-286 [DOI] [PubMed] [Google Scholar]
- 35.Schmitz R. (2015) Trends in der Prävalenz von Asthma bronchiale und allergischer Rhinitis bei Erwachsenen in Deutschland 1997-99 und 2008-11. Fortbildungsveranstaltung für den Öffentlichen Gesundheitsdienst. Berlin. http://www.bfr.bund.de/cm/343/trends-in-der-praevalenz-von-asthma-bronchiale-und-allergischer-rhinitis.pdf (As at 01.03.2017) [Google Scholar]
- 36.Heinrich J, Hoelscher B, Frye C, et al. (2002) Trends in prevalence of atopic diseases and allergic sensitization in children in Eastern Germany. Eur Respir J 19(6):1040-1046 [DOI] [PubMed] [Google Scholar]
- 37.Kramer U, Link E, Oppermann H, et al. (2002) Studying school beginners in western and eastern Germany: allergy trends and sensitisations 1991-2000. Gesundheitswesen 64(12):657-663 [DOI] [PubMed] [Google Scholar]
- 38.Krämer U, Möllemann A, Behrendt J. (2001) Epidemiologie allergischer Erkrankungen bei Kindern. Bundesgesundheitsbl - Gesundheitsforsch - Gesundheitsschutz 44:633–642 [Google Scholar]
- 39.Landesamt für Verbraucherschutz Sachsen-Anhalt (2014) Auswirkungen der Umwelt auf die Gesundheit von Kindern. Schulanfängerstudie 1991-2014. https://verbraucherschutz.sachsen-anhalt.de/fileadmin/Bibliothek/Politik_und_Verwaltung/MS/LAV_Verbraucherschutz/service/publikationen/fb2/schulanfaengerstudie_internet.pdf (As at 01.03.2017)
- 40.Maziak W, Behrens T, Brasky TM, et al. (2003) Are asthma and allergies in children and adolescents increasing? Results from ISAAC phase I and phase III surveys in Munster, Germany. Allergy 58(7):572-579 [DOI] [PubMed] [Google Scholar]
- 41.Anandan C, Nurmatov U, van Schayck OC, et al. (2010) Is the prevalence of asthma declining? Systematic review of epidemiological studies. Allergy 65(2):152-167 [DOI] [PubMed] [Google Scholar]
- 42.Simpson CR, Sheikh A. (2010) Trends in the epidemiology of asthma in England: a national study of 333,294 patients. J R Soc Med 103(3):98-106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Pollmanns J, Romano PS, Weyermann M, et al. (2017) Impact of Disease Prevalence Adjustment on Hospitalization Rates for Chronic Ambulatory Care-Sensitive Conditions in Germany. Health Serv Res Mar 22 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Burney P, Chinn S, Jarvis D, et al. (1996) Variations in the prevalence of respiratory symptoms, self-reported asthma attacks, and use of asthma medication in the European Community Respiratory Health Survey (ECRHS). Eur Respir J 9:687-695 [DOI] [PubMed] [Google Scholar]
- 45.Jarvis D, Newson R, Lotvall J, et al. (2012) Asthma in adults and its association with chronic rhinosinusitis: the GA2LEN survey in Europe. Allergy 67(1):91-98 [DOI] [PubMed] [Google Scholar]
- 46.To T, Stanojevic S, Moores G, et al. (2012) Global asthma prevalence in adults: findings from the cross-sectional world health survey. BMC Public Health 12:204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Heinrich J, Richter K, Frye C, et al. (2002) European Community Respiratory Health Survey in Adults (ECRHS). Pneumologie 56(5):297-303 [DOI] [PubMed] [Google Scholar]
- 48.Filipiak B, Heinrich J, Nowak D, et al. (2001) The distribution in specific IgE and the prevalence of allergic symptoms in 25-64-years old inhabitants of an eastern and a western German city – results from Augsburg and Erfurt. Eur J Epidemiol 17(1):77-84 [DOI] [PubMed] [Google Scholar]
- 49.Hoffmann F. (2007) Prevalence of asthma among German adults: analysis of the German National Telephone Survey. J Asthma 44(6):433-436 [DOI] [PubMed] [Google Scholar]
- 50.Kramer U, Schmitz R, Ring J, et al. (2015) What can reunification of East and West Germany tell us about the cause of the allergy epidemic? Clin Exp Allergy 45(1):94-107 [DOI] [PubMed] [Google Scholar]
- 51.Hermann-Kunz E. (1999) Häufigkeit allergischer Krankheiten in Ost- und Westdeutschland. Gesundheitswesen 61(Sonderheft 2):100-105 [PubMed] [Google Scholar]