

Abstract
Objectives:
Native Americans (NAs) have the highest prevalence of chronic pain of any racial/ethnic group. This issue has received little attention from the scientific community. One factor that may contribute to racial pain disparities is pain catastrophizing. Pain catastrophizing is a construct related to negative pain outcomes in persons with/without chronic pain. It has been suggested that the relationship between trait catastrophizing and pain is mediated by situation-specific (state) catastrophizing. The present study has 2 aims: 1) to investigate whether state pain catastrophizing mediates the relationship between trait catastrophizing and experimental pain (eg, cold, ischemic, heat and electric tolerance), and 2) to investigate whether this relationship is stronger for NAs.
Methods:
145 non-Hispanic Whites (NHWs) and 137 NAs completed the study. Bootstrapped indirect effects were calculated for 4 unmoderated and 8 moderated mediation models (4 models with path a moderated and 4 with path b).
Results:
Consistent with trait-activation theory, significant indirect effects indicated a tendency for trait catastrophizing to be associated with greater state catastrophizing which in turn is associated with reduced pain tolerance during tonic cold (a*b = −.158) and ischemia stimuli (a*b = −.126), but not during phasic electric and heat stimuli. Moderation was only noted for the prediction of cold tolerance (path a). Contrary to expectations, the indirect path was stronger for NHWs (a*b for NHW = −1.22).
Conclusion:
Together, these findings suggest that state catastrophizing mediates the relationship between trait catastrophizing and some measures of pain tolerance but this indirect effect was non-significant for NAs.
Keywords: Pain, Catastrophizing, Diversity, Coping, Clinical health psychology
1.0. Introduction
Native Americans (NA) have the highest rates of chronic pain of any U.S. racial/ethnic group but have received little scientific attention (1–3). Pain catastrophizing is a cognitive-emotional process characterized by pain rumination, magnification and helplessness, and is among the strongest psychosocial predictors of pain and pain-related sequelae (4–9). Recent results from the Oklahoma Study of Native American Pain Risk (OK-SNAP) found that NAs reported greater state pain catastrophizing in response to painful stimuli than non-Hispanic Whites (NHWs), but no difference in dispositional catastrophizing (10–12). Hence, it is important understand the role of pain catastrophizing in hyperalgesia among NAs (ie, reduced pain tolerance - a risk factor for chronic pain)(13).
The Cultural Cognitive-Affective Processing System (C-CAPS(14, 15)) is a theory developed to understand the high interindividual variability in the link between traits and behaviors. The system suggests that situations differentially activate a dynamic array of interacting mediating units (eg, beliefs, values) that together elicit a behavioral response. Culture – socially shared beliefs, customs, values – can mold mediating units and produce similar behavioral responses in a group of people while still allowing for intraindividual variability.
In line with C-CAPS, it has been proposed that pain catastrophizing is a trait-like disposition that must be activated for it to produce its hyperalgesic effects (9, 16). This hypothesis draws a distinction between dispositional (trait) pain catastrophizing that assesses a person’s catastrophic thoughts/emotions across past painful situations, versus situation-specific (state) pain catastrophizing that refers to thoughts/emotions that happen during, and in response to, a painful event. To support this, state catastrophizing is a stronger predictor of experimental pain outcomes than trait-like catastrophizing (17, 18).
To date, little work has been done to test a trait-activation model of pain catastrophizing (9, 14) in which trait pain catastrophizing acts as a predisposition that promotes state catastrophizing in the moment to enhance pain. To our knowledge, all of studies assessing both dispositional and situational pain catastrophizing and experimental pain have focused on bivariate relationships between the 3 variables and not a model explaining their relationship (17, 19).
Moreover, there may be important individual differences in the relationship between trait and state catastrophizing and/or the relationship between state catastrophizing and pain processing that might moderate pain catastrophizing’s hyperalgesic effects. Moderators of the trait-state relationship (path a) would mean that people differ in the extent of trait-activation, whereas moderators of the state catastrophizing-pain relationship (path b) would mean that people differ in the extent that state catastrophizing promotes hyperalgesia (see Fig 1). Given the strong relationship between pain catastrophizing and pain exacerbation, it is imperative to fully understand its conceptual underpinning and its differential activation across groups that are overrepresented with pain conditions (e.g., NAs).
Fig. 1.
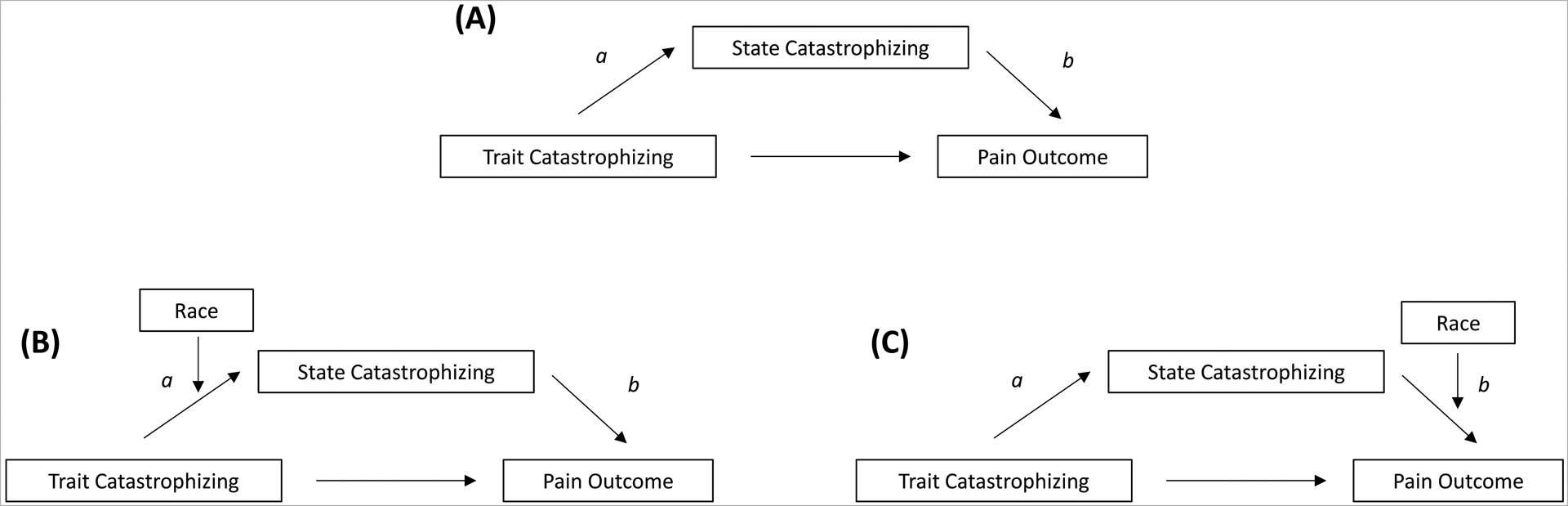
Mediation models. (A) mediation model with no moderators (PROCESS Model 4). (B) mediation model with race as a moderator on the a path (PROCESS Model 7). (C) mediation model with race as a moderator on the b path (PROCESS Model 14).
Thus, the present ancillary analyses from OK-SNAP has 2 aims: 1) to investigate whether state pain catastrophizing mediates the relationship between trait-like catastrophizing and pain tolerance (ie, trait-activation model of catastrophizing), and 2) to investigate whether this mediated relationship is moderated by race/ethnicity (ie, moderated mediation). To achieve these aims, pain catastrophizing (state and trait) was recorded, and pain tolerance was measured from 4 stimulus modalities (cold, ischemic, heat, and electric). Since we previously demonstrated the NAs report higher levels of state catastrophizing (10), we hypothesize that NAs would show a stronger positive state-trait pain catastrophizing association, and a stronger negative state catastrophizing-pain tolerance relationship than NHWs.
2.0. Materials and Methods
2.1. Participants
The parent study, OK-SNAP, had two primary aims: 1) to identify pain processing differences between NAs and NHWs that contribute to the NA pain disparity, and 2) to identify individual differences variables (e.g., catastrophizing) that contribute to the NA pain disparity (See Supplemental Table 1 for OK-SNAP manuscripts). NA and NHW healthy, pain-free participants were recruited so that pain amplifying processes could be determined before the onset of chronic pain when access to treatment or disparities in chronic pain severity might confound the identification of risk factors. Participants were recruited using newspapers ads (tribal and non-tribal), fliers, personal communications, and online strategies (e.g., Facebook, Craigslist, and email announcements).
Exclusion criteria were: 1) <18 years old, 2) history of cardiovascular, neuroendocrine, musculoskeletal, neurological disorders, and/or chronic pain, 3) BMI≥35, 4) use of central acting medications (e.g., anti-depressants, anxiolytic, analgesic, stimulant, and anti-hypertensive medication), 5) current psychotic symptoms (assessed by Psychosis Screening Questionnaire(20)), 6) problems with substance use, and/or 7) an inability to read/speak English. Data collection occurred between March 2014 and October 2018.
To qualify as part of the Native American group, individuals had to present either a Certificate of Degree of Indian Blood (CDIB) card or a tribal membership card. To respect the confidentiality of tribes, tribal affiliation is not reported, but most NAs represent tribal nations predominately from the southern plains and eastern Oklahoma tribes. The study was approved by Institutional Review Boards of The University of Tulsa (13–67R1), Cherokee Nation (Oklahoma Study of Native American Pain Risk), and Indian Health Service Oklahoma City Area Office (P-15–07-OK OK-SNAP). Participants were given an overview of all procedures and informed they could withdraw at any time. All participants provided verbal and written informed consent prior to enrollment and inclusion/exclusion determination. Participants received a $100 honorarium for the completion of each testing day (or $10/hour of non-completed days).
2.3. General Overview of Procedures/Testing
OK-SNAP data were gathered over 2 days. For a full overview of procedures, the interested reader is referred to our prior paper(21). All 4 pain tasks for the current study were assessed on the same day. Electric and heat tolerance were assessed earlier in the day (order counterbalanced), whereas cold pressor tolerance and ischemia tolerance were measured later in the day (order counterbalanced). Breaks were provided between tasks to avoid sensitization and fatigue. Trait pain catastrophizing was assessed at the beginning of the first day of testing. State catastrophizing was assessed immediately after each tolerance task.
2.4. Apparatus
Questionnaires were administered by a computer with dual monitor capacity and A/D board (PCI-6071E; National Instruments, Austin, TX). Custom built LabVIEW software (National Instruments) was used to control timing of the experimental protocol and all off-line data reduction. One computer monitor was used by the experimenter to monitor signals and experimental timing, whereas the second monitor was used by the participant to complete questionnaires and to make ratings of stimuli. Testing was completed in a sound attenuated and electrically shielded testing chamber, and participants were monitored from an adjacent control room via a video camera connected to a flat panel monitor. Participants wore sound attenuating headphones that allowed them to hear the experimenter.
2.5. Electric Tolerance
To assess electric tolerance, a bipolar electrode (Nicolet; 30 mm inter-electrode distance) was placed over the retromalleolar surface of the left ankle and filled with conductive gel (Grass Technologies, West Warwick, RI; EC60). Prior to any sensor placement the skin was cleaned using isopropyl alcohol and exfoliated using an exfoliation cream (Nuprep; Weaver and Company, Aurora, CO) in order to reduce skin impedance below 5 kΩ. Stimulations were delivered by a Digitimer isolated, constant current stimulator (DS7A; Hertfordshire, England). Each stimulus was a train of five 1 ms rectangular wave pulses with a 3 ms inter-pulse interval (250 Hz); however, the train was always experienced as a single stimulation. Electric pain tolerance was assessed using a single ascending staircase of stimulations that started at 0-mA and increased in 2-mA steps until the participant rated a stimulus as maximum tolerable pain on an electronic visual analog scale (VAS) that ranged from “no pain” to “maximum tolerable pain”(22). The maximum stimulation intensity was set at 50-mA to ensure safety.
2.6. Heat Pain Tolerance
Heat stimuli were generated using a Medoc (Haifa, Israel) Pathway device with a Contact Heat Evoked Potential Stimulator (CHEPS) thermode. The thermode was attached to the volar forearm of participant’s non-dominant hand using a Velcro strap. Heat pain tolerance was each assessed 4 times after an initial practice trial. Each trial started from a baseline of 32°C and warmed at a rate of 0.5°C/s until the participant made a button press. Participants were told to push the button when the heat became intolerable. To avoid sensitization, the thermode was moved slightly between trials. Heat pain tolerance was defined as the average of the 4 trials(23). The maximum intensity of the heat stimulus was set to 51°C.
2.7. Cold Pressor Tolerance
To assess cold tolerance, participants were asked to submerge their hand and forearm into a circulating water bath (Thermo Fischer Scientific, Pittsburgh, PA) held at 6±0.1°C (23–25). Participants were instructed to keep their fingers spread apart and to place their hand on the bottom of the water tank and keep it there for as long as they could tolerate it. During the task, a computer timed the duration of the hand/arm immersion. Participants made continuous pain ratings of the cold using on the electronic VAS described above. Cold pressor tolerance was defined as the time from when the participant placed their hand in the water until the participant rated the maximum tolerable pain on the VAS. The maximum cold water exposure was set to 5 min, but the participant was not informed of the limit.
2.8. Ischemia Pain Tolerance
To assess ischemia tolerance, a standard forearm tourniquet test was employed(26). First, participants used their left hand to conduct hand exercises with a dynamometer (Lafayette Hand Dynamometer, Lafayette Instrument Company, IN) at 50% grip strength for 2 min (1x/sec). Immediately after the last exercise, the left arm was raised for 15 s to allow the blood to drain from the forearm and then a blood pressure cuff was inflated to 220 mm/Hg around the left biceps to occlude blood flow to the forearm. During occlusion, participants made continuous pain ratings using the VAS described above. Ischemic tolerance was defined as the time from arm occlusion until the participant made a rating of maximum tolerable pain. The maximum exposure to ischemic pain was set to 20 min, but the participant was not made aware of this limit.
2.9. Pain Catastrophizing Scale
2.9.1. Traditional (Trait) Pain Catastrophizing.
The Pain Catastrophizing (PCS) is a reliable and valid 13-item scale that assesses catastrophic thoughts associated with pain(27). In the current sample (see (28) for details), the PCS has been shown to have construct validity in NAs with an invariant factor structure across NAs and non-Hispanic whites (NHWs). Participants made responses on a 5-point scale that ranged from 0 (not at all) to 4 (all of the time). Higher scores are indicative of greater tendency for pain catastrophizing. To assess trait catastrophizing, traditional instructions were used that ask participants: “Using the scale, please indicate the degree to which you have these thoughts and feelings when you are experiencing pain.” Trait catastrophizing was assessed at the beginning of the study before participants were exposed to any painful stimuli. In the current study, Cronbach’s alpha (internal consistency) for the trait version of the PCS was 0.934 (NHW) and .925 (NA).
2.9.2. Situation-Specific (State) Pain Catastrophizing.
To assess state pain catastrophizing, the PCS was administered, but the instructions were altered to ask about pain catastrophizing specific to each pain task (e.g., “Thinking back to your experience during the [specific pain task], please indicate the degree to which you had these thoughts and feelings”). In the current study, Cronbach’s alpha (internal consistency) for the state version of the PCS ranged were (NHW/NA): α=.945/.950 (cold tolerance), α=.938/.947 (electric tolerance), α=.942/.936 (heat tolerance), α=.942/.962 (ischemia tolerance). The correlations between trait and state catastrophizing ranged from r = .37 to .45.
2.10. Data Analysis
Prior to analyses, variable distributions were screened using boxplots, histograms, and normality statistics. Those that were skewed were log or square transformed to reduce positive and negative skew, respectively. Next, outliers were identified using Wilcox’s MAD-median procedure (using the recommended 2.24 cutoff) and then winsorized by replacing the outlier with the next nearest non-outlier value(29). Multicollinearity diagnostics of all mediation models were acceptable (Tolerances>.4)
The present data were analyzed using PROCESS, a SPSS macro by Hayes (30, 31), in order to conduct the moderated mediation models. Importantly, PROCESS constructs bootstrapped confidence intervals for the mediation effects (ie, indirect effects)(30), such that if the confidence interval for the indirect effect does not contain 0 then the mediation is considered statistically significant. In order to investigate aim 1, a mediation model was used (model 4 in PROCESS). To investigate aim 2, two moderated mediation models were selected. In the first one, race/ethnicity moderated path a (Fig 1b; model 7 in PROCESS). In the other, race/ethnicity moderated path b (Fig 1c: model 14 in PROCESS). Continuous predictors used to create interaction terms were centered in each model (i.e., trait catastrophizing in PROCESS model 7 and state catastrophizing in PROCESS model 14). Race/ethnicity was coded as NHW = 0 and NA = 1. The state catastrophizing used in each PROCESS model was specific to the painful stimulus (e.g., state catastrophizing during electric tolerance was used as a mediator in the model predicting electric tolerance).
3.0. Results
3.1. The Final Sample
282 individual participants were included in the study. 29 participants quit before completing tolerance measures, and 16 only completed the experimental testing day in which tolerances were not recorded. The final sample for the mediation analyses consisted of 237 individuals. Table 1 notes sample characteristics by race/ethnicity. The results suggest there were more women in the NA group, and NAs had higher BMIs compared to the NHW group. Hence, Sex [Male = 0; Female = 1], and BMI were added as covariates in all mediation models. The results from correlations (See Table 2) suggests that trait catastrophizing was not significantly correlated with any pain tolerance outcome (average r = .02) whereas state catastrophizing was significantly negatively correlated to cold (r = −.34) and ischemic tolerances (r = −.23).
Table 1.
Participant characteristics by racial/ethnic group
| Missing Data | NHW (N=145) | NA (N=137) | ||||
|---|---|---|---|---|---|---|
| Continuous Variable | N | M | SD | M | SD | t |
| Age (years) | 0 | 28.50 | 13.48 | 31.28 | 13.26 | 2.79 |
| Body Mass Index (kg/m2) | 7 | 24.25 | 3.80 | 26.05 | 4.60 | 1.80 |
| Categorical Variable | N | % | N | % | Χ2 | |
| Sex (female) | 0 | 68 | 46 | 87 | 63 | 7.85 |
| Education | 2 | 4.74 | ||||
| <7th grade | 1 | 0.4 | 1 | 0.4 | ||
| <High school | 2 | 0.7 | 7 | 2.5 | ||
| High school grad | 20 | 7.1 | 23 | 8.2 | ||
| Partial college | 75 | 26.8 | 59 | 21.1 | ||
| College grad | 36 | 69.2 | 37 | 13.2 | ||
| Graduate/professional school | 10 | 3.6 | 9 | 3.2 | ||
| Marital Status | 2 | 8.72 | ||||
| Single | 108 | 38.6 | 82 | 29.3 | ||
| Married | 23 | 8.2 | 29 | 10.4 | ||
| Separated/Divorced | 11 | 3.9 | 14 | 5.0 | ||
| Cohabitating | 2 | 0.7 | 9 | 3.2 | ||
| Widowed | 1 | 0.4 | 1 | 0.4 | ||
| Employment | 5 | 3.47 | ||||
| >40 hours / week | 30 | 10.8 | 39 | 14.1 | ||
| <40 hours / week | 65 | 23.5 | 50 | 18.1 | ||
| Retired | 5 | 1.8 | 3 | 1.1 | ||
| Unemployed | 42 | 15.2 | 43 | 15.5 | ||
| Income | 9 | 6.76 | ||||
| <$9,999 | 55 | 20.1 | 36 | 13.2 | ||
| $10,000-$14,999 | 16 | 5.9 | 15 | 5.5 | ||
| $15,000-$24,999 | 16 | 5.9 | 19 | 7.0 | ||
| $25,000-$34,999 | 12 | 4.4 | 16 | 5.9 | ||
| $35,000-$49,999 | 13 | 4.8 | 20 | 7.3 | ||
| $50,000-$74,999 | 9 | 3.3 | 10 | 3.7 | ||
| $75,000-$99,999 | 8 | 2.9 | 6 | 2.2 | ||
| $100,000-$149,999 | 8 | 2.9 | 7 | 2.6 | ||
| $150,000-$199,999 | 2 | 0.7 | 2 | 0.7 | ||
| >$200,000 | 2 | 0.7 | 1 | 0.4 | ||
Note. Some variables had missing data, therefore not all counts sum to the total N. NA=Native American. NHW=non-Hispanic White. Bolded values are significant at α=.05.
Table 2.
Intercorrelations of Study Variables.
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 11 | 12 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Cold Tolerance (Log[s+1]) | |||||||||||
| 2 | Ischemia Tolerance (Log[s+1]) | 0.42a | ||||||||||
| 3 | Heat Tolerance (C°) | 0.44a | 0.47a | |||||||||
| 4 | Electric Tolerance (mA) | 0.44a | 0.37a | 0.40a | ||||||||
| 5 | State Catas Cold Tolerance (Log[PCS+1]) | −0.34a | −0.15a | −0.07 | −0.09 | |||||||
| 6 | State Catas Ischemia Tolerance (Log[PCS+1]) | 0.001 | −0.23a | −0.03 | −0.01 | 0.68a | ||||||
| 7 | State Catas Heat Tolerance (Log[PCS+1]) | 0.03 | −0.10 | 0.06 | 0.05 | 0.65a | 0.71a | |||||
| 8 | State Catas Electric Tolerance (Log[PCS+1]) | −0.06 | −0.23a | −0.13 | −0.10 | 0.66a | 0.73a | 0.70a | ||||
| 9 | Trait Catas Day 1 (Log[PCS+1]) | 0.03 | −0.04 | 0.04 | 0.04 | 0.37a | 0.41a | 0.45a | 0.44a | |||
| 10 | Race/Ethnicity (NHW=0, NA=1) | −0.14a | −0.14a | −0.13 | −0.02 | 0.13a | 0.03 | 0.11 | 0.08 | 0.03 | ||
| 11 | Sex (Male=0, Female=1) | −0.15a | −0.17a | −0.34a | −0.06 | −0.07 | −0.09 | −0.14a | 0.01 | −0.13a | 0.17a | |
| 12 | BMI (kg/m2) | −0.09 | −0.15a | 0.03 | 0.05 | 0.10 | −0.04 | 0.02 | 0.01 | 0.06 | 0.21a | −0.04 |
Note.
p < .05. s=seconds. Catas=Catastrophizing.
3.2. Evidence for a Trait-Activation Model of Pain Catastrophizing (Aim 1)
To test aim 1, the present study conducted 4 mediation models in which state catastrophizing was used as a mediator for the relationship between trait catastrophizing and each of the 4 pain tolerance variables (electric, heat, cold, ischemia). Results are presented in Table 3. In 2 out of the 4 mediation models (cold and ischemia tolerance) the indirect effects are significant. Interestingly, the direct effect (c’) was positive in both the models but was only significant in the cold tolerance model.
Table 3.
Indirect Tests for the Trait Activation Model of Pain Catastrophizing
| 95% CI | |||||
|---|---|---|---|---|---|
| Dependent Variable | Path Tested | Effect | SE | Lower | Upper |
| Electric Tolerance (mA) | Cˈ | 3.741 | 2.634 | −1.450 | 8.932 |
| Indirect (a*b) | −2.188 | 1.271 | −4.851 | .178 | |
| Heat Tolerance (C°) | Cˈ | −.044 | .337 | −.710 | .621 |
| Indirect (a*b) | .066 | .150 | −.221 | .364 | |
| Cold Tolerance (Log[s+1]) | Cˈ | .175 | .071 | .036 | .315 |
| Indirect (a*b) | −.158 | .039 | −.241 | −.088 | |
| Ischemia Tolerance (Log[s+1]) | Cˈ | .077 | .081 | −.081 | .236 |
| Indirect (a*b) | −.126 | .038 | −.206 | −.050 | |
Note. Cˈ=direct effect. a*b =indirect effect. SE = Standard Error. s=seconds. CI = confidence Interval for indirect effects were bootstrapped at 10000 samples. Bolded effects are significantly different from 0. Sex and BMI were included as covariates.
3.3. Evidence for a Moderated Effect by Race/Ethnicity (Aim 2)
To test aim 2, 2 sets of 4 mediated moderation models were conducted. In set 1, race/ethnicity moderated path a (X->M; Fig 1b). In set 2, race/ethnicity moderated path b (M->Y; Fig 1c).
3.4.1. Moderation of Trait-Activation of Pain Catastrophizing (path a).
One model out of the 4 (cold tolerance) had a significant moderated mediation (See Table 4). Results indicated that NHWs had a significant indirect effect (axb = −.142), but NAs did not (axb = .003). This suggests that the trait-activation hypothesis for pain catastrophizing was not significant in the NA sample regarding cold pain tolerances.
Table 4.
Results of Moderated Mediation for the Relationship between Trait and State Pain Catastrophizing (moderated a-paths)
| 95% CI | |||||
|---|---|---|---|---|---|
| Dependent Variable | Tests of Moderation and Indirect Paths | Effect | SE | Lower | Upper |
| Electric Tolerance (mA) | Test of Moderated Mediation | .623 | .710 | −.530 | 2.279 |
| Conditional Indirect Effects | |||||
| a*b for NHWs | −2.097 | 1.247 | −4.640 | .248 | |
| a*b for NAs | −1.474 | 1.111 | −4.080 | .182 | |
| Heat Tolerance (C°) | Test of Moderated Mediation | −.021 | .067 | −.170 | .114 |
| Conditional Indirect Effects | |||||
| a*b for NHWs | .063 | .144 | −.212 | .354 | |
| a*b for NAs | .042 | .113 | −.160 | .313 | |
| Cold Tolerance (Log[s+1]) | Test of Moderated Mediation | .146 | .059 | .041 | .271 |
| Conditional Indirect Effects | |||||
| a*b for NHWs | −.142 | .037 | −.223 | −.077 | |
| a*b for NAs | .003 | .059 | −.115 | .119 | |
| Ischemia Tolerance (Log[s+1]) | Test of Moderated Mediation | .040 | .045 | −.045 | .135 |
| Conditional Indirect Effects | |||||
| a*b for NHWs | −.123 | .037 | −.206 | −.058 | |
| a*b for NAs | −.083 | .056 | −.205 | .017 | |
Note. Bolded values are significantly different from 0. A significant Test of Moderated Mediation indicates that there was a significant difference between the indirect path for non-Hispanic Whites (NHWs) and the indirect path for Native Americans (NAs). Cˈ=direct effect. SE = Standard Error. s=seconds. CI = confidence Interval for indirect effects were bootstrapped at 10,000 samples. NA=Native American. NHW=non-Hispanic Whites. Sex and BMI were included as covariates.
3.4.2. Moderation of the Pain Enhancing Effects of State Catastrophizing.
One model (heat tolerance) out of the 4 had significant moderated mediation (Table 5); hviewowever, neither of the simple indirect effects for NAs or NHWs was significant. This suggests that the indirect effects in NA and NHW are significantly different from each other, but they are not significantly different than 0. Thus, NAs and NHWs did not differ in the way that state catastrophizing impacted pain tolerance.
Table 5.
Results of Moderated Mediation for the Relationship between State Pain Catastrophizing and Pain Tolerance (moderated b-paths)
| 95% CI | |||||
|---|---|---|---|---|---|
| Dependent Variable | Tests of Moderation and Indirect Paths | Effect | SE | Lower | Upper |
| Electric Tolerance (mA) | Test of Moderated Mediation | −.612 | 2.348 | −5.377 | 3.9087 |
| Conditional Indirect Effects | |||||
| a*b for NHW | −2.140 | 1.317 | −4.862 | .338 | |
| a*b for NA | −2.752 | 2.915 | −8.804 | 2.767 | |
| Heat Tolerance (C°) | Test of Moderated Mediation | −.628 | .282 | −1.221 | −.114 |
| Conditional Indirect Effects | |||||
| a*b for NHW | .077 | .149 | −.210 | .380 | |
| a*b for NA | −.551 | .314 | −1.20 | .037 | |
| Cold Tolerance (Log[s+1]) | Test of Moderated Mediation | −.035 | .050 | −.142 | .061 |
| Conditional Indirect Effects | |||||
| a*b for NHW | −.150 | .037 | −.230 | −.086 | |
| a*b for NA | −.185 | .062 | −.320 | −.076 | |
| Ischemia Tolerance (Log[s+1]) | Test of Moderated Mediation | −.069 | .059 | −.191 | .045 |
| Conditional Indirect Effects | |||||
| a*b for NHW | −.122 | .037 | −.202 | −.056 | |
| a*b for NA | −.192 | .073 | −.345 | −.058 | |
Note. Bolded values are significantly different from 0. A significant Test of Moderated Mediation indicates that there was a significant difference between the indirect path for non-Hispanic Whites (NHWs) and the indirect path for Native Americans (NAs). Cˈ=direct effect. SE = Standard Error. s=seconds. CI = confidence Interval for indirect effects were bootstrapped at 10,000 samples. NA=Native American. NHW=non-Hispanic Whites. Sex and BMI were included as covariates.
4.0. Discussion
The present study had 2 aims: 1) to investigate if state pain catastrophizing mediated the relationship between trait catastrophizing and pain outcomes (trait-activation hypothesis), and 2) to see if this mediated relationship was moderated by race.
In relation to aim 1, results indicated that state catastrophizing mediated the relationship between trait catastrophizing and cold and ischemic pain tolerances. These results partially support a trait-activation model in which trait pain catastrophizing promotes state pain catastrophizing which then in turn reduces pain tolerance(9). As such, trait pain catastrophizing is activated during a painful event and produces hyperalgesia by causing the individual to engage in state catastrophizing.
The present study is the first to formally test the trait-activation model of pain catastrophizing. Historically, pain catastrophizing has been conceptualized as a dispositional variable that remains relatively stable over time(32). However, recent studies have noted that pain catastrophizing, when measured in response to a painful task, can vary from one context to another(9). These results extend past literature that suggest that measures of trait-like personality features only predispose individuals to behaviors. However, traits must be activated by situational cues which trigger myriad of psychological mediating factors that influence behavior(14).
Previous studies suggest state catastrophizing is a predictor of pain in both healthy and clinical populations(16, 18, 33, 34). When studies compare the effect of dispositional and state catastrophizing, state catastrophizing is typically a better predictor of experimental and clinical pain(16, 19, 35). In the present study, zero-order correlations indicated that state catastrophizing predicted pain tolerance (cold, ischemia) whereas trait catastrophizing did not. This is in line with previous studies suggesting a small (and sometimes non-significant) relationship between trait catastrophizing and experimental pain. Indeed, some studies did not find a relationship between trait catastrophizing and pressure (muscle and bone), thermal, and visceral (thermal and electric) experimental pain(36). On the other hand, in-vivo manipulation of state catastrophizing has been fruitful in detecting state catastrophizing-related pain changes. Notably, 2 studies provide compelling evidence linking state pain catastrophizing with hyperalgesia. One study experimentally decreased state pain catastrophizing with the use of positive coping statements/mental imagery in the presence of a painful threat which resulted in lower pain(37). Another study, increased and decreased state pain catastrophizing with hypnotic suggestions, resulting in increased and decreased pain, respectively(38). This underscores the importance of assessing both trait and state catastrophizing to fully understand the relationship between catastrophizing and pain. This could be achieved by through the implementation of diary studies. For example, one study suggested the relationship between daily pain and trait catastrophizing is amplified by state catastrophizing(39).
Interestingly, indirect effects were not significant for the heat and electric tolerance models. It is possible that prolonged, tonic, noxious stimulation is needed to elicit state catastrophizing’s hyperalgesic effects. Indeed, it has been suggested that the hyperalgesic effects from state pain catastrophizing increase over the duration of the stimuli(36). As such, tonic pain stimuli would provide enough time for pain catastrophizing to exert its hyperalgesic effects on pain. This effect was evident in a multimodal (ie, heat, cold, pressure), multi-tissue (ie, somatic, visceral) experimental study that found that only cold pressor pain was related to trait pain catastrophizing(36). Although the study did not measure state catastrophizing, it can be inferred that psychological states during painful events modify pain (e.g., state) (40). Thus, many studies that investigate state catastrophizing’s influence on experimental pain use tonic noxious stimuli such as a cold pressor(17, 19, 35).
In relation to aim 2, our results indicate that in response to certain experimental pain procedures, race/ethnicity moderates the indirect effects. When path a was moderated, the simple indirect effect of trait pain catastrophizing on cold tolerance was significant for NHWs but not for NAs. This suggests that the path by which trait catastrophizing influences pain is not constant across people or stimuli. Indeed, the concept that activated traits do not release the same mediating factors (which ultimately influence behavior) is central to C-CAPS(14). Mediating factors are individualized beliefs, memories, values, and a host of other psychological variables, all of which are influenced by culture. As such, train pain catastrophizing may release different mediating factors in NAs than in NHWs after being activated by the painfully cold water. Indeed, prior studies in NAs have suggested that the increased state catastrophizing in NAs is driven by prior adverse experiences and psychological distress(11). As such, it is possible that adverse experiences and psychological distress may influence the relationship between trait and state pain catastrophizing.
An interesting finding is that the direct effects (c’ path) predicting cold tolerance scores were positive. These results indicate that when the relationship between state catastrophizing and tolerance is controlled, there is a positive relationship between trait catastrophizing and cold tolerance (hypoalgesia). This contrasts literature indicating that trait pain catastrophizing is also hyperalgesic(9). However, the results may represent an artificial scenario in which the hyperalgesic relationship between state catastrophizing and pain tolerance is controlled for, which may erase trait pain catastrophizing’s negative influence on pain.
4.3. Potential Implications for Reducing Pain Disparities
Pain catastrophizing mediates improvement in psychological pain interventions including Cognitive Behavioral Therapy (CBT)(41), and Acceptance and Commitment Therapy (ACT)(42, 43). The results from the present study support the treatment target and suggest that psychological interventions may benefit from increased focus on the reduction of pain catastrophizing particularly in response to tonic pain. Further research is needed on the most effective way to reduce state catastrophizing. Nevertheless, we can hypothesize that this may be accomplished with live coaching while participants are exposed to uncomfortable sensations much akin to exposure-based psychological interventions, which have a history of successfully treating fear-based psychological disorders(44–48). However, since trait and state pain catastrophizing are weakly correlated, this would suggest that reducing trait catastrophizing may lead to clinical improvements by lowering state catastrophizing (and more so in NHWs); however, this must be empirically tested.
Further, the results from this study suggest the existence of differential relationships between state and trait catastrophizing by race/ethnicity in some instances. Since trait catastrophizing acts through state catastrophizing to influence pain, this would suggest that the most effective treatment targets for chronic pain interventions may differ by race/ethnicity. However, this must be further tested, and currently appears impractical as it is unlikely that a reduction in trait catastrophizing can occur without modifying state catastrophizing.
4.3. Strengths and Limitations
To our knowledge, this is the first study to formally assess the trait-activation model of pain catastrophizing. Further, we assessed whether components of the model can be moderated by race/ethnicity. The present study had several other strengths. First, we had a large sample that allowed us to investigate individual, as well as group, differences. Second, this study used several pain modalities to investigate any possible differences between pain characteristics (e.g., tonic vs phasic stimuli). Third, we investigated race/ethnic differences. NA status was corroborated with CDIB card and tribal membership cards. Fourth, we used state-of-the-art data analysis techniques to bolster statistical inferences.
Despite these strengths, a few limitations should be noted. First, we recruited only healthy, pain-free individuals so results may not generalize to participants with chronic pain or other health problems. Future studies could recruit participants with chronic pain to help overcome this limitation. Second, NAs in OK-SNAP were primarily from urban areas in northeastern Oklahoma; there may be important differences associated with NAs from other regions that could alter responses to the pain catastrophizing questionnaires. Indeed, tribes are not monolithic, and each may have their own unique cultural practices and beliefs about pain. Third, although the use of modern statistical analysis (e.g., bootstrapped moderated-mediation models) is a strength, these models did not correct for family-wise error which is a possible limitation.
4.2. Summary
The present study is the first to give support to the idea that state catastrophizing mediates the relationship between trait catastrophizing and tonic pain outcomes. Further, this relationship, in some instances, is moderated by race/ethnicity which gives insight into treatment targets and a mechanistic theory of pain catastrophizing and pain.
Supplementary Material
Disclosures:
This research was supported by the National Institute on Minority Health and Health Disparities of the National Institute of Health under Award Number R01MD007807. Edward Lannon, Shreela Palit, and Yvette Güereca were supported by a National Science Foundation Graduate Research Fellowship Program. Edward Lannon was also supported by T32DA035165. The content is solely the responsibility of the authors and does not necessarily reflect the views of the National Institutes of Health, National Science Foundation, Indian Health Service, or the Cherokee Nation. The authors report no conflicts of interest.
Footnotes
Competing Interests: Authors state no conflict of interest
Informed Consent: Informed consent has been obtained from all individuals included in this study.
Ethical Approval: Research involving human subjects complied with all relevant national regulations, institutional policies and is in accordance with the tenets of the Helsinki Declaration (as amended in 2013), and has been approved by the authors’ Institutional Review Board.
References
- 1.USDHHS. Summary of health statistics for U.S. Adults: National health interview survey, 2009. In: Services HaH, editor. Hyattsville, Maryland: DHHS; 2010. [Google Scholar]
- 2.Barnes PM, Adams PF, Powell-Griner E. Health characteristics of the American Indian or Alaska Native adult population: United States, 2004–2008. In: Services USDoHaH, editor. Hyattesville, MD: National Center for Health Statistics; 2010. [PubMed] [Google Scholar]
- 3.Jimenez N, Garroutte E, Kundu A, Morales L, Buchwald D. A Review of the Experience, Epidemiology, and Management of Pain among American Indian, Alaska Native, and Aboriginal Canadian Peoples. Journal of Pain. 2011;12(5):511–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gracely R, Geisser M, Giesecke T, Grant M, Petzke F, Williams D, et al. Pain catastrophizing and neural responses to pain among persons with fibromyalgia. Brain. 2004;127(4):835–43. [DOI] [PubMed] [Google Scholar]
- 5.Keefe FJ, Brown GK, Wallston KA, Caldwell DS. Coping with rheumatoid arthritis pain: Catastrophizing as a maladaptive strategy. Pain. 1989;37(1):51–6. [DOI] [PubMed] [Google Scholar]
- 6.Keefe FJ, Rumble ME, Scipio CD, Giordano LA, Perri LM. Psychological Aspects of Persistent Pain: Current State of the Science. Journal of Pain. 2004;5(4):195–211. [DOI] [PubMed] [Google Scholar]
- 7.Seminowicz DA, Davis KD. Cortical responses to pain in healthy individuals depends on pain catastrophizing. Pain. 2006;120(3):297–306. [DOI] [PubMed] [Google Scholar]
- 8.Sullivan MJ, Thorn B, Haythornthwaite JA, Keefe F, Martin M, Bradley LA, et al. Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain. 2001;17(1):52–64. [DOI] [PubMed] [Google Scholar]
- 9.Quartana PJ, Campbell CM, Edwards RR. Pain catastrophizing: a critical review. Expert Rev Neurother. 2009;9(5):745–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rhudy JL, Lannon EW, Kuhn BL, Palit S, Payne MF, Sturycz CA, et al. Sensory, affective, and catastrophizing reactions to multiple stimulus modalities: results from the Oklahoma Study of Native American Pain Risk. The Journal of Pain. 2019;20(8):965–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Huber FA, Kell PA, Kuhn BL, Lannon EW, Palit S, Payne MF, et al. The Association Between Adverse Life Events, Psychological Stress, and Pain-Promoting Affect and Cognitions in Native Americans: Results from the Oklahoma Study of Native American Pain Risk. Journal of Racial and Ethnic Health Disparities. 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Toledo TA, Kuhn BL, Payne MF, Lannon EW, Palit S, Sturycz CA, et al. The effect of pain catastrophizing on endogenous inhibition of pain and spinal nociception in Native Americans: Results from the Oklahoma Study of Native American Pain Risk. Annals of Behavioral Medicine. 2020;54(8):575–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Braun M, Bello C, Riva T, Hönemann C, Doll D, Urman RD, et al. Quantitative Sensory Testing to Predict Postoperative Pain. Curr Pain Headache Rep. 2021;25(1):1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mendoza-Denton R, Mischel W. Integrating system approaches to culture and personality. Handbook of cultural psychology. 2007:175–95. [Google Scholar]
- 15.Mischel W, Shoda Y. Toward a unified theory of personality: Integrating dispositions and processing dynamics within the cognitive-affective processing system. 2008.
- 16.Campbell CM, Kronfli T, Buenaver LF, Smith MT, Berna C, Haythornthwaite JA, et al. Situational versus dispositional measurement of catastrophizing: associations with pain responses in multiple samples. The Journal of Pain. 2010;11(5):443–53. e2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Dixon KE, Thorn BE, Ward LC. An evaluation of sex differences in psychological and physiological responses to experimentally-induced pain: a path analytic description. Pain. 2004;112(1–2):188–96. [DOI] [PubMed] [Google Scholar]
- 18.Edwards RR, Smith MT, Stonerock G, Haythornthwaite JA. Pain-related catastrophizing in healthy women is associated with greater temporal summation of and reduced habituation to thermal pain. The Clinical journal of pain. 2006;22(8):730–7. [DOI] [PubMed] [Google Scholar]
- 19.Edwards RR, Campbell CM, Fillingim RB. Catastrophizing and experimental pain sensitivity: only in vivo reports of catastrophic cognitions correlate with pain responses. The Journal of Pain. 2005;6(5):338–9. [DOI] [PubMed] [Google Scholar]
- 20.Bebbington P, Nayani T. The psychosis screening questionnaire. Int J Methods Psychiatr Res. 1995. [Google Scholar]
- 21.Rhudy JL, Lannon EW, Kuhn BL, Palit S, Payne MF, Sturycz CA, et al. Assessing peripheral fibers, pain sensitivity, central sensitization, and descending inhibition in Native Americans: main findings from the Oklahoma Study of Native American Pain Risk. Pain. 2020;161(2):388–404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Rhudy JL, France CR, Bartley EJ, McCabe KM, Williams AE. Psychophysiological responses to pain: further validation of the nociceptive flexion reflex (NFR) as a measure of nociception using multilevel modeling. Psychophysiology. 2009;46(5):939–48. [DOI] [PubMed] [Google Scholar]
- 23.Campbell CM, Edwards RR, Fillingim RB. Ethnic differences in responses to multiple experimental pain stimuli. Pain. 2005;113(1–2):20–6. [DOI] [PubMed] [Google Scholar]
- 24.Meagher MW, Arnau RC, Rhudy JL. Pain and emotion: effects of affective picture modulation. Psychosom Med. 2001;63(1):79–90. [DOI] [PubMed] [Google Scholar]
- 25.Rhudy JL, Dubbert PM, Parker JD, Burke RS, Williams AE. Affective modulation of pain in substance-dependent veterans. Pain Med. 2006;7(6):483–500. [DOI] [PubMed] [Google Scholar]
- 26.Fillingim RB, Maixner W, Girdler SS, Light KC, Sheps DS, Mason GA. Ischemic but not thermal pain sensitivity varies across the menstrual cycle. Psychosom Med. 1997;559:512. [DOI] [PubMed] [Google Scholar]
- 27.Sullivan MJL, Bishop SR, Pivik J. The Pain Catastrophizing Scale: Development and validation. Psychological Assessment. 1995;7(4):524–32. [Google Scholar]
- 28.Rhudy JL, Arnau RC, Huber FA, Lannon EW, Kuhn BL, Palit S, et al. Examining Configural, Metric, and Scalar Invariance of the Pain Catastrophizing Scale in Native American and Non-Hispanic White Adults in the Oklahoma Study of Native American Pain Risk (OK-SNAP). J Pain Res. 2020;13:961–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Wilcox RR. Understanding and applying basic statistical methods using R: John Wiley & Sons; 2016. [Google Scholar]
- 30.Bolin JH, Hayes Andrew F. (2013). Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression‐Based Approach. New York, NY: The Guilford Press. Journal of Educational Measurement. 2014;51(3):335–7. [Google Scholar]
- 31.Hayes AF. PROCESS: A versatile computational tool for observed variable mediation, moderation, and conditional process modeling. University of Kansas, KS; 2012. [Google Scholar]
- 32.Sullivan MJ, Thorn B, Haythornthwaite JA, Keefe F, Martin M, Bradley LA, et al. Theoretical perspectives on the relation between catastrophizing and pain. The Clinical journal of pain. 2001;17(1):52–64. [DOI] [PubMed] [Google Scholar]
- 33.France CR, France JL, al’Absi M, Ring C, McIntyre D. Catastrophizing is related to pain ratings, but not nociceptive flexion reflex threshold. Pain. 2002;99(3):459–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Thorn BE, Clements KL, Ward LC, Dixon KE, Kersh BC, Boothby JL, et al. Personality factors in the explanation of sex differences in pain catastrophizing and response to experimental pain. The Clinical journal of pain. 2004;20(5):275–82. [DOI] [PubMed] [Google Scholar]
- 35.Grosen K, Drewes AM, Pilegaard HK, Pfeiffer-Jensen M, Brock B, Vase L. Situational but not dispositional pain catastrophizing correlates with early postoperative pain in pain-free patients before surgery. The Journal of Pain. 2016;17(5):549–60. [DOI] [PubMed] [Google Scholar]
- 36.Kristiansen FL, Olesen AE, Brock C, Gazerani P, Petrini L, Mogil JS, et al. The role of pain catastrophizing in experimental pain perception. Pain Practice. 2014;14(3):E136–E45. [DOI] [PubMed] [Google Scholar]
- 37.Terry EL, Thompson KA, Rhudy JL. Does pain catastrophizing contribute to threat-evoked amplification of pain and spinal nociception? Pain. 2016;157(2):456–65. [DOI] [PubMed] [Google Scholar]
- 38.Kjøgx H, Kasch H, Zachariae R, Svensson P, Jensen TS, Vase L. Experimental manipulations of pain catastrophizing influence pain levels in patients with chronic pain and healthy volunteers. Pain. 2016;157(6):1287–96. [DOI] [PubMed] [Google Scholar]
- 39.Sturgeon JA, Zautra AJ. State and trait pain catastrophizing and emotional health in rheumatoid arthritis. Annals of Behavioral Medicine. 2013;45(1):69–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Rhudy JL. Chapter 3 - Emotional Modulation of Pain. In: al’Absi M, Flaten MA, editors. Neuroscience of Pain, Stress, and Emotion. San Diego: Academic Press; 2016. p. 51–75. [Google Scholar]
- 41.Turner JA, Holtzman S, Mancl L. Mediators, moderators, and predictors of therapeutic change in cognitive-behavioral therapy for chronic pain. Pain. 2007;127(3):276–86. [DOI] [PubMed] [Google Scholar]
- 42.Buhrman M, Skoglund A, Husell J, Bergström K, Gordh T, Hursti T, et al. Guided internet-delivered acceptance and commitment therapy for chronic pain patients: a randomized controlled trial. Behaviour research and therapy. 2013;51(6):307–15. [DOI] [PubMed] [Google Scholar]
- 43.Vowles KE, McCracken LM, Eccleston C. Processes of change in treatment for chronic pain: the contributions of pain, acceptance, and catastrophizing. Eur J Pain. 2007;11(7):779–87. [DOI] [PubMed] [Google Scholar]
- 44.Foa EB. Prolonged exposure therapy: past, present, and future. Depression and anxiety. 2011. [DOI] [PubMed] [Google Scholar]
- 45.Resick PA, Monson CM, Chard KM. Cognitive processing therapy for PTSD: A comprehensive manual: Guilford Publications; 2016. [Google Scholar]
- 46.Sloan DM, Marx BP, Bovin MJ, Feinstein BA, Gallagher MW. Written exposure as an intervention for PTSD: A randomized clinical trial with motor vehicle accident survivors. Behaviour research and therapy. 2012;50(10):627–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Lindsay M, Crino R, Andrews G. Controlled trial of exposure response prevention in obsessive-compulsive disorder. The British Journal of Psychiatry. 1997;171:135. [DOI] [PubMed] [Google Scholar]
- 48.Gilroy L, Kirkby KC, Daniels BA, Menzies R, Montgomery I. Controlled comparison of computer-aided vicarious exposure versus live exposure in the treatment of spider phobia. Behav Ther. 2001;31:733–44. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.