

Abstract
Background
Treatment of acute asthma is based on rapid reversal of bronchospasm and arresting airway inflammation. There is some evidence that intravenous magnesium can provide additional bronchodilation when given in conjunction with standard bronchodilating agents and corticosteroids. No systematic review of this literature has been completed on this topic.
Objectives
To examine the effect of additional intravenous magnesium sulfate in patients with acute asthma managed in the emergency department.
Search methods
Randomised controlled trials were identified from the Cochrane Airways Review Group register. Bibliographies from included studies, known reviews and texts were searched. Primary authors and content experts were contacted.
Selection criteria
Randomised controlled trials or quasi‐randomised trials were eligible for inclusion. Studies were included if patients presented with acute asthma and were treated with IV magnesium sulfate versus placebo.
Data collection and analysis
Data were extracted and methodological quality was assessed independently by two reviewers. Missing data were obtained from authors.
Main results
Seven trials were included (5 adult, 2 pediatric). A total of 665 patients were involved. Patients receiving magnesium sulfate demonstrated non‐significant improvements in peak expiratory flow rates when all studies were pooled (weighted mean difference: 29.4 L/min; 95% confidence interval: ‐3.4 to 62). In studies of people with severe acute asthma, peak expiratory flow rate improved by 52.3 L/min (95% confidence interval: 27 to 77.5). The forced expiratory volume in one second also improved by 9.8 % predicted (95% confidence interval: 3.8 to 15.8). Overall, admission to hospital was not reduced, odds ratio: 0.31 (95% confidence interval: 0.09 to 1.02). In the severe subgroup, admissions were reduced in those receiving magnesium sulfate (odds ratio: 0.10, 95% confidence interval: 0.04 to 0.27). No clinically important changes in vital signs or adverse side effects were reported.
Authors' conclusions
Current evidence does not support routine use of intravenous magnesium sulfate in all patients with acute asthma presenting to the emergency department. Magnesium sulfate appears to be safe and beneficial in patients who present with severe acute asthma.
Keywords: Adult; Child; Humans; Emergency Service, Hospital; Acute Disease; Adrenal Cortex Hormones; Adrenal Cortex Hormones/therapeutic use; Asthma; Asthma/drug therapy; Bronchodilator Agents; Bronchodilator Agents/therapeutic use; Drug Therapy, Combination; Infusions, Intravenous; Magnesium Sulfate; Magnesium Sulfate/administration & dosage; Magnesium Sulfate/therapeutic use
Plain language summary
Magnesium sulfate for treating exacerbations of acute asthma in the emergency department
In an asthma attack, the airways (passages to the lungs) narrow from muscle spasms and swelling (inflammation). Bronchodilator drugs (reliever inhalers) can be used to relax the muscles and open the airways, and corticosteroid drugs to reduce the inflammation. Magnesium sulfate is a drug that can also affect muscles, and may reduce inflammation as well. It can be given through a drip in the veins (intravenously). The review of trials found that intravenous magnesium sulfate in addition to bronchodilators seems to be safe and beneficial for people with severe asthma attacks, or those for whom bronchodilators are not working.
Background
Acute presentations to the emergency department (ED) are common and potentially serious complications of asthma. Approximately 10‐25% of patients presenting to the ED will require admission to the hospital, however this rate varies depending on the age group studied, the treatments received (Rowe 1992) and the setting. Treatment of acute asthma is based on pathophysiologic considerations including treatment of bronchospasm and airway inflammation. Practice variation exists with respect to treatment approaches and this may be due in part to a lack of evidence‐based summaries of the research pertinent to this field (Camargo 1998). Generally, the initial treatment agents include beta‐2 agonists which specifically target adrenergic receptors (Beveridge 1996; BTS 1997; Lipworth 1997; NAEPP 1997). Among children, quaternary agents administered in conjunction with beta‐2 agonists have been shown to potentially increase the magnitude and duration of bronchodilation over that achieved with beta‐2 agonists alone (Plotnik 1997). Additional treatment of oedema is usually initiated with corticosteroids (Rowe 1992).
Given the need for rapid bronchodilation, there has been a wealth of research on the use of bronchodilators in the initial management of acute asthma (Cates 1998). However, the potential role of other agents in the initial management of acute asthma is still unclear. A meta‐analysis of aminophylline performed a decade ago indicated no benefit in acute asthma (Littenberg 1988). On the other hand, steroids appear to reduce admissions to hospital and relapse following discharge (Rowe 1992). Significant debate exists with respect to the benefit of other agents such as magnesium sulfate in the treatment of acute asthma. Magnesium is an important cofactor in many enzymatic reactions and is linked to cellular homeostasis. In addition, magnesium has an effect on smooth muscle cells, with hypomagnesaemia causing contraction and hypermagnesaemia causing relaxation. There is some evidence that when magnesium is infused into asthmatic patients, it can provide additional bronchodilation (Okayama 1987; Rolla 1988). In addition, evidence suggests that magnesium may reduce the neutrophilic burst seen with the inflammatory response (Cairns 1996). Thus, there is reason to believe that magnesium treatment, in the form of intravenous magnesium sulfate, may be beneficial in the treatment of acute asthma.
This systematic overview examines evidence for the effectiveness of intravenous magnesium treatment in acute asthma. No systematic review of the magnesium sulfate literature has been published to date.
Objectives
The objective of this review was to determine the effect of intravenous magnesium sulfate in people with acute asthma treated in the emergency department.
Specific Aims
To quantify the effect of the combination of magnesium sulfate with other agents compared to the effect of these other agents alone. The specific outcomes include: (1) Admissions (e.g. time to decision, % admission) (2) Pulmonary functions (3) Side effects and vital signs such as heart rate, respiratory rate and blood pressure (BP).
Methods
Criteria for considering studies for this review
Types of studies
To be considered, reported studies had to be randomised controlled trials (RCT) or quasi RCTs (e.g. allocation on days of the week).
Types of participants
Studies including either children or adult patients presenting to an emergency department for treatment of acute asthma were considered for inclusion in the overview. Age was one of the sub‐groups examined.
Types of interventions
Studies reporting results of patients randomised to receive magnesium sulfate compared to placebo early in the emergency department treatment were included. Since acute asthmatics require additional treatments (e.g. beta‐agonists, corticosteroids, ipratropium bromide, etc.) data for any co‐interventions were recorded or requested from the authors when not reported in the studies.
Types of outcome measures
Primary outcomes
Admission to hospital
Secondary outcomes
Pulmonary function tests including: peak expiratory flow rates (PEFR), forced expiratory volume in one second (FEV‐1), and % predicted PEFR or FEV‐1
Vital signs (heart rate, respiratory rate, BP)
Adverse outcomes and side effects
Attempts were made to contact the primary investigators of included studies to obtain individual patient data, however this was unsuccessful.
Search methods for identification of studies
Electronic searches
The Cochrane Airways Review Group asthma register was searched using the following terms:
Asthma OR Wheez* AND Emerg* OR acute OR status AND Discharge OR admi* OR hospit* Mag* OR magnesium sulfate OR MS
Searching other resources
Reference lists of all available primary studies and review articles were reviewed to identify potentially relevant citations. An advanced search of CENTRAL was completed using the terms: magnesium AND asthma. Inquiries were made regarding other published or unpublished studies known and/or supported by the authors of the included studies. Finally, personal contact with colleagues, collaborators and other trialists working in the field of asthma was made to identify potentially relevant studies.
Data collection and analysis
Selection of studies
From the title, abstract, or descriptors, two reviewers (BR, JB) independently reviewed literature searches to identify potentially relevant trials for full review. Searches of bibliographies and texts were conducted to identify additional studies. From the full text, using specific criteria, two reviewers (CB, GB) independently selected trials for inclusion. Agreement was measured using kappa statistics. Disagreement was resolved by consensus or third party adjudication (BR).
Data extraction and management
Data for the trials were extracted by two reviewers (BR, JB). Primary study authors were requested to confirm data extraction and provide additional clarification and information for the review. Unfortunately, most authors could not access their original data to perform supplemental analyses. In some cases, expansion of graphic representations of data from the manuscripts were used to estimate missing data. Lung function data were entered as negative values to conform to the Cochrane convention whereby effects that favour the treatment under review move to the left.
Assessment of risk of bias in included studies
Assessment of methodological quality: Methodological quality assessment was performed by two reviewers working independently. Both used two different methods of assessment. First, using the Cochrane approach to assessment of allocation concealment, all trials were scored and entered using the following scale: Grade A: Adequate concealment Grade B: Uncertain Grade C: Clearly inadequate concealment Inter‐rater reliability was measured by using simple agreement and kappa weighted statistics.
In addition, each study was assessed using a 0‐5 scale (Jadad 1996) and summarized as follows: 1) Was the study described as randomised (1=yes; 0=no)? 2) Was the study described as double‐blind (1=yes; 0=no)? 3) Was there a description of withdrawals and dropouts (1=yes; 0=no)? 4) Was the method of randomisation well described and appropriate (1=yes; 0=no)? 5) Was the method of double blinding well described and appropriate (1=yes; 0=no)? 6) Deduct 1 point if methods for randomisation OR blinding were inappropriate. Inter‐rater reliability was measured by using kappa, and weighted kappa statistics.
Data synthesis
Statistical considerations: All trials were combined using the Review Manager. Subgroup comparisons are identified in the Comparisons section. For dichotomous variables, individual and pooled statistics were calculated as odds ratios (OR) with 95% confidence intervals (95% CI); a random effects model was used. For continuous outcomes, individual and pooled statistics were calculated as weighted mean differences (WMD) and 95% CIs using a random effects model.
Subgroup analysis and investigation of heterogeneity
Two specific subgroups were planned a priori. One was to compare adults with children. The other was to compare patients with severe asthma to those with less severe asthma. Other sensitivity analyses were conducted on mixed vs. random effects and methodological quality (high versus low).
Results
Description of studies
Results of the search
The initial search yielded 90 references of which 68 (76%) were identified as being original publications. Independent review of the abstracts and titles of these identified 8 potentially relevant studies. The simple agreement for relevance was 98% with a kappa of 0.76 (very good agreement). Additional references were sought from bibliographic searching of relevant articles and overviews (n=13), and from contact with authors (n=5), and one through journal searching. A total of 27 studies were reviewed for inclusion. Independent review of these potentially relevant articles resulted in 6 studies meeting the inclusion criteria for this meta‐analysis; no relevant article was found from the journal search, bibliographic search or recommendations from authors. An updated search strategy was completed (Spring 1998) with the addition of one trial (Devi 1997). The review is considered updated to January of 1999.
Included studies
The majority of studies were reported after 1989. Six were from centres in the United States; one was from India.
Populations: Two studies were conducted in children (Ciarallo 1997; Devi 1997) and five in adults (Skobeloff 1989; Green 1992; Bloch 1995; Tiffany 1993; Silverman 1996). The populations varied from "all patients" with acute asthma (n = 2), to only those with severe attacks (n = 5). However, examination of the definitions used to designate the severe group (see below) reveals that patients had a combination of clinical findings, airflow measurements, and/or response to therapy that placed them in a more severe category.
I. Severe subgroup:
Bloch (sub‐group only): FEV‐1 < 25% predicted after a single beta‐2 agonist treatment. Admission rate in the placebo treated patients 79%. Ciarallo: Children with PEFR < 60% predicted following three beta‐2 agonist nebuliser treatments. Admission in the placebo treated patients 100%. Devi: Children with "severe" asthma AND a poor response to initial therapy (no airflow measurements). Admission rate in placebo treated patients 94%. Skobeloff: Adults with initial PEFR < 200 L/min AND did not double following two beta‐2 agonists and > 1 hour of treatment. Admission rate in the placebo treated patients 88%. Silverman: Adults with initial FEV‐1 < 30% predicted. Admission rates in the placebo group unavailable. Tiffany: Adults with initial PEFR < 200 L/min, AND failed to double PEFR after two treatments of albuterol. Admission rates in the placebo group unavailable.
II. Mild‐Moderate Group:
Bloch (mild‐moderate subgroup): Adults with 25‐75% predicted FEV‐1 after a single beta‐2 agonist treatment. Admission rate in the placebo treated patients 24%. Green: Adults who were "unresponsive" to a single beta‐2 agonist treatment. Unresponsiveness was defined as not improving to a point where discharge was possible. Admission rate in the placebo treated patients 18%.
The admission rate was not used a priori to classify the severity sub‐group, but does lend some support to the use of this method of clinical categorisation of severity. For example, the severe sub‐groups have admission rates of > 75% whereas the mild‐moderate sub‐group has admission rates of < 25%.
Interventions: magnesium was administered early in the course of the emergency department treatment; two studies were within 30 minutes (Bloch 1995; Silverman 1996), three were at approximately 1 hour (Skobeloff 1989; Tiffany 1993; Devi 1997) and one was unstated (Ciarallo 1997). The route of administration was via the intravenous route in all studies and was administered as a bolus in all but one study where bolus +/‐ a continuous infusion was employed (Tiffany 1993). The dosage of intravenous magnesium sulfate delivery varied among studies however. All studies used a placebo of similar appearance. The dose in adults ranged from 1.2 gm to 2 gm IV and was generally administered over 20 minutes. In the pediatric studies, children received 25 mg/kg (Ciarallo 1997) or 100 mg/kg (Devi 1997) (up to a maximum of 2 gm) IV over 20 minutes.
Co‐interventions
Co‐interventions included various beta‐agonists in all studies. Theophylline administration was left to the discretion of the treating physician in all but two studies (Tiffany 1993; Devi 1997) in which patients were started on intravenous aminophylline. Corticosteroids were routinely administered to all patients in 6 studies, and to those with the most severe asthma in the other (Bloch 1995). Adult patients received 125 mg (Green 1992; Skobeloff 1989; Silverman 1996; Tiffany 1993) and children 2 mg/kg of IV methylprednisolone (Ciarallo 1997) or either IV or oral corticosteroids (Devi 1997). Ipratropium bromide was administered at the discretion of the treating physician in one study (Green 1992).
Outcomes
Outcomes were determined at variable times but usually included admission to hospital/discharge assessment, and a variety of pulmonary function results. Short‐term follow‐up was provided in two studies (Ciarallo 1997; Green 1992) and at 1 week (Bloch 1995) to determine the rate of relapse to additional care. The variability of treatment approaches following discharge makes comparisons invalid. Side effects and vital signs were reported frequently enough to permit pooling.
Excluded studies
See Excluded studies.
Risk of bias in included studies
Overall, the methodological quality of the included studies was rated as high. Many of the studies were double‐blind, placebo controlled, demonstrated an appreciation of the need for concealment of allocation, and reported a sufficient number of outcomes.
Using the Jadad method, 6 studies were rated as "strong" (Tiffany 1993; Silverman 1996; Bloch 1995; Ciarallo 1997; Devi 1997; Skobeloff 1989), and 1 was rated as "weak" (Green 1992). A full manuscript was not available from one research group, so methodological quality was verified through author contact and review of the methods and results sections (Silverman 1996). Using the Cochrane methodology: five studies were rated as having blinded allocation (Tiffany 1993; Ciarallo 1997; Bloch 1995; Silverman 1996; Devi 1997). It was unclear whether allocation was blinded in one study (Skobeloff 1989), and in another study, allocation was clearly unblinded (Green 1992).
Effects of interventions
Results from this meta‐analysis are reported by outcome. The main results are reported as overall effects of IV magnesium sulfate versus placebo. In addition, the main subgroup based on asthma severity is also reported.
Admission to Hospital
No significant difference was identified between patients treated with magnesium sulfate or placebo with respect to hospital admission at the end of the study period (OR: 0.31; 95% CI: 0.09 to 1.02, Analysis 1.1). However, this pooled result demonstrated significant heterogeneity (Chi‐squared = 19.53; df = 5; p < 0.05). In patients within the severe asthma subgroup, hospital admissions in those treated with magnesium sulfate were lower than in those treated with placebo (OR: 0.10; 95% CI: 0.04 to 0.27). This pooled result did not demonstrated significant heterogeneity (Chi‐squared = 0.26; df = 3; p > 0.1). There was no difference in hospitalisation for the studies where participants had mild‐moderate asthma (OR: 1.36; 94% CI: 0.72 to 2.55).
1.1. Analysis.
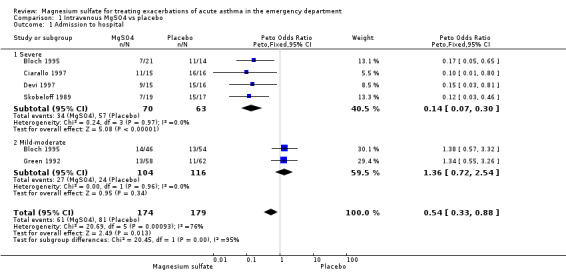
Comparison 1 Intravenous MgSO4 vs placebo, Outcome 1 Admission to hospital.
Emergency Department Pulmonary Function Results
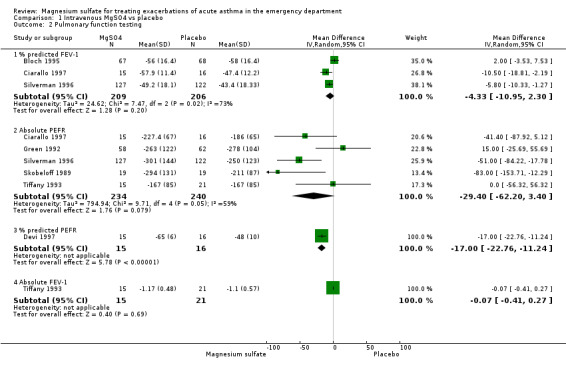
The PEFR and % predicted FEV‐1 were the most commonly reported tests, usually at the completion of the trial (or as close to 6 hours as possible). Patients receiving magnesium sulfate demonstrated non‐significant improvements in PEFR (WMD: 29.4; 95% CI: ‐3.4 to 62) and % predicted FEV‐1 (WMD: 4.3; 95% CI: ‐2.3 to 10.9) when all studies were pooled. Statistically significant heterogeneity was identified for the results when all studies were pooled: PEFR (Chi‐squared = 9.7; df = 4; p < 0.05); % predicted FEV‐1 (Chi‐squared = 7.47; df = 2; p < 0.01). Improvement in lung function tests was more pronounced for those patients in the severe subgroup. These results are tabulated:
Lung function test
| Outcome | All studies WMD (95% CI) | N of studies | Severe subgroup WMD & 95% CI | N of studies |
| PEFR (Litres/min) | 29.4 (‐3.4 to 62)* | 5 | 52.3 (27 to 77.5) | 3 |
| PEFR % predicted | 17 (11.2 to 27.8) | 1 | 17 (11.2 to 27.8) | 1 |
| FEV1 litres | 0.1 (‐0.3 to 0.4) | 1 | 0.1 (‐0.3 to 0.4) | 1 |
| FEV1 % predicted | 4.3 (‐2.3 to 10.9)* | 3 | 9.8 (3.8 to 15.8) | 3 |
Note: * heterogeneity testing = Chi‐squared p < 0.05
Tolerability
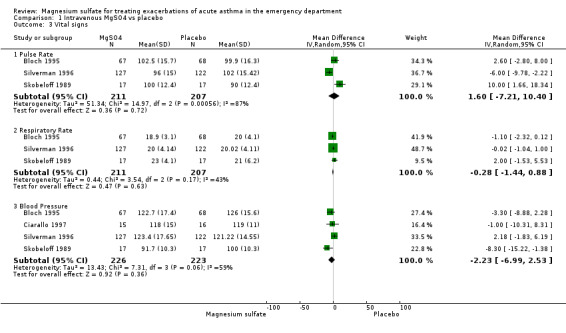
Vital signs were recorded and reported in many of the included studies; pooled results did not demonstrate statistical or clinical heterogeneity. These results indicate that heart rate (WMD: 5.6 beats/minute; 95% CI: ‐1.5 to 12.7) and respiratory rates (WMD: ‐0.01 breaths/minute; 95% CI: ‐2.9 to 2.9) did not change with IV magnesium sulfate treatment. Systolic blood pressure was slightly decreased (WMD: ‐4.5 mm Hg; 95% CI: ‐8.4 to ‐0.6). However, a change of this magnitude would not be considered clinically important. Overall, vital signs remained "stable" during the period immediately after administration of IV magnesium.
Side Effects
Side effect monitoring was common in these studies, but few adverse events were reported. Magnesium appears to be a safe drug to administer to asthmatics in the acute state. Four trials reported no major side effects; minor side effects (burning at IV site, flushing, fatigue) were reported by 58% of patients in one trial (Bloch 1995). Insufficient numbers of studies were available to provide meaningful sensitivity and sub‐group comparisons or to draw firm conclusions about side effects and adverse events.
Subgroup/Sensitivity Analyses
For pooled admission rates, children improve similarly to adults who have severe asthma (2 pediatric studies). Using a fixed effects model, the admission rate was lower in the magnesium sulfate treated patients (WMD: 0.54; 95% CI; 0.33 to 0.87), but significant heterogeneity remained. When the study of lowest quality was eliminated (Green 1992), the pooled admission rate remained statistically lower for magnesium sulfate than placebo (WMD: 0.25; 95% CI: 0.08 to 0.25) and the heterogeneity was not significant (p > 0.05).
Discussion
This systematic review examined the use of IV magnesium sulfate in the emergency department management of acute asthma. The pooled results failed to demonstrate statistically significant evidence of a beneficial effect of magnesium sulfate in terms of admission rates or pulmonary functions. While the drug was well tolerated, the lack of effect argues against its indiscriminate use in the emergency department treatment of acute asthma.
This being said, there is evidence to suggest that a sub‐group of patients experiencing a more severe asthma attack may respond differently to those with a less severe exacerbation. Patients who presented with severe asthma appeared to benefit from the use of IV magnesium sulfate, both in terms of pulmonary functions and admission rates. The clinical significance of the magnitude of the pulmonary function improvement is difficult to determine, since the minimally clinically important difference for lung function tests in acute asthma have not been determined. In chronic asthma an improvement of 12% predicted has been used (NAEPP 1997) and for acute studies, some have suggested an increase in PEFR of 30 L/min is clinically important (Tiffany 1993). The improvement of approximately 10% predicted FEV‐1 or 50 L/min PEFR represent what we believe are important lung function test changes, especially considering the severity at the start of therapy. Moreover, these lung function test changes appear important enough to reduce admissions.
Severe asthma was defined differently across studies: i. 25‐30% predicted PEFR at presentation (adults) ii. Failure to respond to initial treatments (adults and children), iii. Failure to improve beyond 60% predicted after 1 hour of care (children).
A consistent marker of the severity was a failure to respond to initial beta‐2 agonist treatment. For example, four studies in this review used this to define severity (Ciarallo 1997; Devi 1997; Skobeloff 1989; Tiffany 1993). This observation leads to the suggestion that a failure to respond to initial beta‐2 agonist treatment may be an appropriate method of identifying those individuals who may benefit from magnesium sulfate treatment.
It is important to discuss the validity of subgroup analyses. Guidelines for subgroup analyses have been published (Oxman 1992), and should be considered within the context of this review. This meta‐analysis used a sub‐group based on baseline asthma severity which meets the above guidelines, given that it was an a priori decision and one which has been used in other Cochrane Airways Group reviews. In addition, the effect sizes were large, demonstrated no heterogeneity across five studies, and were physiologically reasonable. Furthermore, the subgroup results generated from both within (Bloch 1995) and between study comparisons were consistent.
Intravenous administration of magnesium sulfate was shown to be safe in those studies where vital signs and side effects were recorded. For example, magnesium sulfate treatment did not change pulse or respiratory rates; the minor change in systolic blood pressure was clinically insignificant. While this may seem counter‐intuitive, we suggest that the poor reliability and validity of respiratory rate measurement might explain these findings. For example, in one large emergency department study, almost all of the respiratory rates were recorded as 20/minute (Camargo 1998). When interpreting the safety and adverse reaction data, caution is advised since the total sample size of the pooled sample was insufficient to detect rare adverse events.
There is a possibility of publication bias in this meta‐analysis. For example, by missing unpublished negative trials we may be over‐estimating the effect of magnesium treatment. However, a comprehensive search of the published literature for potentially relevant studies was conducted, using a systematic strategy to avoid bias. This was followed by attempts to contact corresponding and first authors. One unpublished trial was identified and several negative trials were uncovered; however, we recognise that more of these types of trials may exist.
There is also a possibility of study selection bias. However, we employed two independent reviewers, and feel confident that the studies excluded were done so for consistent and appropriate reasons. Our search was comprehensive and has been updated, so it is unlikely that there are any trials in publication which were missed.
Authors' conclusions
Implications for practice.
In this review, parenteral magnesium sulfate was provided as 2 gm IV over 20 minutes to adults and 25‐100 mg/kg IV to children.
Many patients who present for assessment and treatment to the emergency department with an asthmatic exacerbation may not benefit from early treatment with magnesium sulfate.
Patients with severe acute asthma appear to benefit in terms of pulmonary function improvements and reduced admissions. In this context, severe asthma is defined as peak expiratory flow rates of less than 25‐30% predicted after initial beta2‐agonist therapy in adults and/or non‐response to treatment (adults and children), or peak expiratory flow rates of less 60% predicted (children).
A clinical approach may be to identify candidates for magnesium sulfate therapy among those patients who do not respond to initial beta2‐agonists treatment.
Two studies examined the use of magnesium in children. Given the similarity of the findings in children, it should have the same indications in the adult population. Only one study examined its use in children aged less than six, but the numbers were small.
In addition to any magnesium intervention, standard acute asthma therapy must be administered to these patients early in the emergency department treatment.
Implications for research.
Many questions regarding the treatment of acute asthma with magnesium remain unanswered.
Most importantly, additional research is required to determine the optimal dose and duration of therapy.
Additional studies are needed to confirm the sub‐group findings from this review suggesting a beneficial effect of magnesium sulfate only in severe acute asthma. In future studies, severity must be clearly defined and based on presenting pulmonary function results AND response to initial beta‐agonist therapy whenever possible.
Studies involving very young children need to be performed to determine the effect of magnesium sulfate in this age group.
Further studies are required to examine the effect of magnesium sulfate based on the prior inhaled steroid use in patients presenting to the emergency department with an asthma exacerbation. The effect of treatment may differ based on inhaled steroid use, and the answer to this question remains unclear. Inhaled steroids are increasingly employed and the development of high dose inhaled steroids with lower systemic activity suggests that this would be an important area for future research.
Future research on acute asthma must concentrate on well defined outcomes which may lead to more informative reviews in the future. More specifically, criteria for discharge and reporting of lung function test data in a systematic fashion would assist in further work. Finally, better description of the methodology would also be beneficial.
What's new
| Date | Event | Description |
|---|---|---|
| 18 May 2016 | Amended | This review has been updated and replaced following the publication of two new reviews on the same topic in adults and children: Intravenous magnesium sulfate for treating adults with acute asthma in the emergency department (http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD010909.pub2/full), and Intravenous magnesium sulfate for treating children with acute asthma in the emergency department (http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD011050.pub2/abstract). Readers of this review should refer to the two above more recent updates of this topic area for the most recent evidence. |
History
Protocol first published: Issue 2, 1996 Review first published: Issue 3, 1999
| Date | Event | Description |
|---|---|---|
| 6 August 2008 | Amended | Converted to new review format. |
| 22 October 1999 | New citation required and conclusions have changed | Substantive amendment |
Notes
This review has been updated and replaced following the publication of two new reviews on the same topic in adults and children:
Intravenous magnesium sulfate for treating adults with acute asthma in the emergency department (http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD010909.pub2/full), and
Intravenous magnesium sulfate for treating children with acute asthma in the emergency department (http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD011050.pub2/abstract).
Readers of this review should refer to the two above more recent updates of this topic area for the most recent evidence.
Acknowledgements
The authors wish to acknowledge the assistance of Stephen Milan, Anna Bara, and Jane Dennis of the Cochrane Airways Review Group. We would also like to acknowledge the assistance of the following corresponding authors: Dr. R Silverman, Dr. SM Green, Dr. E Skobeloff, and Dr. B Tiffany. Finally, the assistance of Professor Paul Jones (Cochrane Airways Review Group Coordinating Editor) was greatly appreciated.
Data and analyses
Comparison 1. Intravenous MgSO4 vs placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Admission to hospital | 5 | 353 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.54 [0.33, 0.88] |
| 1.1 Severe | 4 | 133 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.14 [0.07, 0.30] |
| 1.2 Mild‐moderate | 2 | 220 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.36 [0.72, 2.54] |
| 2 Pulmonary function testing | 7 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 % predicted FEV‐1 | 3 | 415 | Mean Difference (IV, Random, 95% CI) | ‐4.33 [‐10.95, 2.30] |
| 2.2 Absolute PEFR | 5 | 474 | Mean Difference (IV, Random, 95% CI) | ‐29.40 [‐62.20, 3.40] |
| 2.3 % predicted PEFR | 1 | 31 | Mean Difference (IV, Random, 95% CI) | ‐17.0 [‐22.76, ‐11.24] |
| 2.4 Absolute FEV‐1 | 1 | 36 | Mean Difference (IV, Random, 95% CI) | ‐0.07 [‐0.41, 0.27] |
| 3 Vital signs | 4 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3.1 Pulse Rate | 3 | 418 | Mean Difference (IV, Random, 95% CI) | 1.60 [‐7.21, 10.40] |
| 3.2 Respiratory Rate | 3 | 418 | Mean Difference (IV, Random, 95% CI) | ‐0.28 [‐1.44, 0.88] |
| 3.3 Blood Pressure | 4 | 449 | Mean Difference (IV, Random, 95% CI) | ‐2.23 [‐6.99, 2.53] |
| 4 Major Side Effects | 4 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Subtotals only | |
| 5 ED Treatment Time | 2 | 167 | Mean Difference (IV, Random, 95% CI) | ‐5.28 [‐9.34, ‐1.21] |
1.2. Analysis.
Comparison 1 Intravenous MgSO4 vs placebo, Outcome 2 Pulmonary function testing.
1.3. Analysis.
Comparison 1 Intravenous MgSO4 vs placebo, Outcome 3 Vital signs.
1.4. Analysis.
Comparison 1 Intravenous MgSO4 vs placebo, Outcome 4 Major Side Effects.
1.5. Analysis.
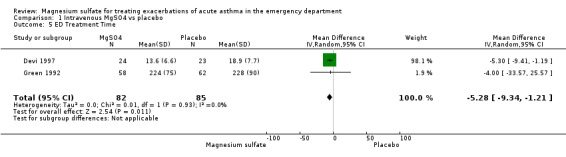
Comparison 1 Intravenous MgSO4 vs placebo, Outcome 5 ED Treatment Time.
Comparison 2. Intravenous MgSO4 vs Placebo (Severe Asthma subgroup).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Pulmonary function testing | 6 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 % predicted FEV‐1 | 3 | 315 | Mean Difference (IV, Random, 95% CI) | ‐9.81 [‐15.82, ‐3.80] |
| 1.2 Absolute PEFR | 3 | 318 | Mean Difference (IV, Random, 95% CI) | ‐52.25 [‐77.50, ‐27.00] |
| 1.3 % predicted PEFR | 1 | 31 | Mean Difference (IV, Random, 95% CI) | ‐17.0 [‐22.76, ‐11.24] |
| 1.4 Absolute FEV‐1 | 1 | 36 | Mean Difference (IV, Random, 95% CI) | ‐0.07 [‐0.41, 0.27] |
2.1. Analysis.
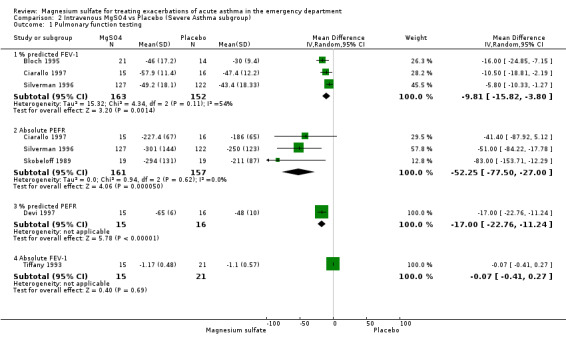
Comparison 2 Intravenous MgSO4 vs Placebo (Severe Asthma subgroup), Outcome 1 Pulmonary function testing.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Bloch 1995.
| Methods | Randomisation: Using a central pharmacy employing a random numbers table. Concealment of allocation was appropriate. Blinding: double‐blind, similar appearance of the study drugs. Number dropped/lost: 14 patients excluded after enrolment; second visits (12), non‐reversible airway diease (1), and heart failure (1). | |
| Participants | Location: two adult hospitals, New York, USA. Participants: 135 asthmatics aged 18 to 65 years with acute asthma and FEV‐1 less than 75% predicted both before and after a single albuterol treatment. Exclusions: a history of congestive heart failure, diabetes mellitus, angina, renal insufficiency, T >38 degrees C, pneumonia, or if pregnant. Patients requiring intubation, unable to perform spirometry, or unable to give informed consent were also excluded. Those with FEV‐1 greater than 75% before or after the single albuterol treatment were also excluded. Severity: Based on PF data. Severe: < 25% predicted FEV‐1; moderate: 25‐75% predicted FEV‐1. | |
| Interventions | Standard of care: All patients received nebulised albuterol (2.5 mg in 2.5 ml) and an IV was started. Patients who had % predicted FEV‐1 < 40% or those who had received oral prednisone within 6 months of the study were given 125 methylprednisolone. Treatment: At T= 30 minutes, patients were randomised to receive either 2 gm of IV magnesium sulfate or 50 ml saline IV (placebo) as an adjunct to standardised emergency department procedure for acute asthma. | |
| Outcomes | Clinical Score: Borg index. Admission to hospital: criteria applied (% predicted FEV‐1 > 50% by 120 minutes) = discharge; or at 240 minutes (< 50% predicted FEV‐1, OR RR > 27 OR shortness of breath at rest or minimal exertion). Pulmonary Functions: FEV‐1 and % predicted FEV‐1. Lab values: Mg, CBC, electrolytes, blood urea, nitrogen, creatinine, theophylline level. Urine pregnancy test in women of childbearing age. Vital Signs: PR, RR, BP. Side effects: not reported. Timing: Outcomes were determined at 0, 30, 60, 120, 360 minutes following baseline. | |
| Notes | Attempts to contact the primary author were unsuccessful. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | Using a central pharmacy employing a random numbers table. Concealment of allocation was appropriate. |
Ciarallo 1997.
| Methods | Randomisation: in blocks of 10, patients randomised by the pharmacy department, using a random numbers table. Blinding: double‐blind. Solutions were pre‐packaged by the pharmacy and were similar in appearance. | |
| Participants | Location: Pediatric teaching hospital, Boston, USA. Participants: 31 patients 6 to 18 years of age presenting to the emergency department with an acute asthma attack were enrolled in the study. Children with PEFR < 60% predicted following three ß‐agonist nebuliser treatments. Exclusions: PEFR > 60% of the predicted value after receiving three beta‐adrenergic nebulizer treatments; T > 38.5 C, systolic BP < 25th percentile for age, history of cardiac, renal or pulmonary disease, pregnancy, or recent use of theophylline. | |
| Interventions | Standard of care: All patients given oxygen, nebulized beta‐agonists (0.15 mg/kg in 3 ml of saline), and approximately 75% of both groups received intravenous methylprednisolone. Treatment: magnesium sulfate infusion, 25 mg/kg (maximum 2 gm) over 20 minutes. Control: equivolume saline solution (placebo) over 20 minutes. The solutions were identical in appearance. | |
| Outcomes | Clinical score: none. Admission to hospital: Criteria applied (SaO2 > 94%, no evidence of respiratory distress, minimal or no wheezing, PEFR > 70% predicted, and normal cerebral function for 3 hours after last nebulization). Pulmonary functions: serial PEFR, FVC, FEV‐1. Lab values: serum Mg was measured before and after the 20 minute infusion. Vital signs: BP, PR, SaO2. Side effects: major and minor side effects were recorded. Timing: serially recorded for 110 minutes. | |
| Notes | Attempts to contact the primary author were unsuccessful. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | Randomised by the pharmacy department, using a random numbers table |
Devi 1997.
| Methods | Randomisation: central pharmacy, no other information provided. Blinding: double‐blind, similar appearance of the study drugs. Number lost/dropped: 2 patients meeting the inclusion criteria for sub‐optimal response were later excluded due to the development of a febrile response. | |
| Participants | Location: Pediatric Emergency Department of teaching hospital, Chamadigarh, India. Participants: 47 children, aged 1‐12, presenting to the ED with severe asthma with a poor response to initial therapy. Exclusions: T > 38.0 C (axillary), BP < 50% for age and gender. Severity: mild, moderate, severe based on a rating system from the National Heart, Lung and Bolood Institute (USA). | |
| Interventions | Standard of care: all patients received nebulised salbutamol (0.15 mg/kg/dose) every 20 minutes for 1 hour, IV/po corticosteroids, aminophylline infusion, oxygen, and +/‐ subcutaneous epinephrine. Treatment: 0.2ml of 50% MgSO4 in 30 ml (100 mg/kg) in 5% dextrose over 35 minutes. Control: normal saline in 30 ml of 0.25 saline in 5% dextrose over 35 minutes | |
| Outcomes | Clinical scoring: modified Pulmonary Index Score (RR, wheeze, accessory muscle use, dyspnea; scores ranged from 0 to 12) for ages > 6. Admission to hospital: criteria applied (PEFR > or + 70% predicted, normal PR, < 10 mmHg pulsus paradoxus, normal RR, minimal or no wheeze, mild to no accessory muscle use, and minimal to absent dyspnea), timing of admission assessment not defined. Pulmonary Functions: absolute and % predicted PEFR. Lab values: serum Mg. Vital signs: PR, RR, T and oximetry. Side effects: major and minor, knee jerk assessment. Timing: at time of infusion, 1, 2, 3, 7, and 15 hours. | |
| Notes | Author's response to questions not obtained. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | Central pharmacy randomisation |
Green 1992.
| Methods | Randomisation: Patients presenting on odd days were given the treatment infusion of magnesium sulfate. Patients presenting on even days received nothing (no placebo). Blinding: single‐blind. Number dropped/lost: 97 excluded from analysis (120 included in analyses) ‐ second visits (80), pneumonia (4), missing PEFR data (7), lost charts (2), heart failure (2), lung cancer (1), intubation (1). | |
| Participants | Location: urban teaching hospital in Riverside, USA. Participants: 217 patients consecutive patients aged 18 to 65 years with acute asthma (ATS criteria) unresponsive to a single albuterol treatment were enrolled. Exlusions: heart disease, chest pain, uncontrolled hypertension, congestive heart failure, heart block, cancer, renal disease, pneumonia, or pregnancy. | |
| Interventions | Standard of care: All patients received oxygen, 125 mg IV methylprednisolone, and hourly albuterol nebulised albuterol (0.5 ml in 2.5 ml saline). Theophylline administered if serum level was sub‐therapeutic. Treatment: 2 grams IV magnesium sulfate diluted in 50 mL 5% dextrose solution infused over 20 minutes. Control: Patients presenting on even days did not receive magnesium; no placebo was administered. | |
| Outcomes | Clinical scores: not reported. Hospital admission: no specific criteria ("dyspnea relieved and auscultation demonstrated clear breath sounds or minimal wheezing"). Relapse rates, time in emergency department were also recorded. Pulmonary functions: PEFRs. Lab values: CBC, theophylline level. Vital signs: PR, RR, T. Side effects: major (hypotension, bradycardia) or minor (flushing, malaise, etc) recorded. Timing: hourly until discharge. | |
| Notes | Dr. Green responded to queries; unfortunately, data were not available for re‐analyses. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | High risk | Alternate allocation by days of the week. |
Silverman 1996.
| Methods | Randomisation: blocked randomisation, stratified by center in a 1:1 ratio, and controlled by a central pharmacy. Blinding: double‐blind; both placebo and magnesium were placed by the study pharmacist in identical vials with only the study number and administration instructions printed on the label. Number dropped/lost: unclear. | |
| Participants | Location: 8 adult teaching hospitals in USA. Participants: Acute asthma (criteria: asthma "diagnosis" and receiving treatment within the past 6 months) ages 18‐60 years with % predicted FEV‐1 < or equal to 30% at presentation to the emergency departments. Exclusions: pregnancy, T > 102 F, suspected to have pneumonia OR history of COPD, heart failure, coronary artery disease, diabetes mellitus, renal insufficiency, or hypertension treated with medication | |
| Interventions | Standard of care: All patients received oxygen, nebulised inhaled albuterol (2.5 mg) @ 0, 30, 60, 120, 180 minutes. IV 125 mg methylprednisolone was administered @ time 0 to all patients. Treatment: 2 gm of IV magnesium sulfate at 30 minutes. Control: 50 cc saline (placebo) at 30 minutes. | |
| Outcomes | Clinical score: Borg index. Admission to hospital: offered to patients if they had any of the following: FEV‐1 < 50% predicted, respiratory rate > 25/minute, no improvement in shortness of breath or wheezing, or significant dyspnea on ambulation. Out‐patient follow‐up at 1 and 7 days. Pulmonary functions: absolute and % predicted FEV‐1 and PEFR. Lab values: Serum Mg at start and 4 hours later. Vital Signs: PR, RR, systolic BP. Side effects: unavailable. Timing: Hourly, and a maximum of 240 minutes (4 hours) after enrolment in the study. | |
| Notes | Published abstract; Dr. Robert Silverman provided the preliminary methods manuscript and the additional results as required for this meta‐analysis. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | Central pharmacy randomisation |
Skobeloff 1989.
| Methods | Randomisation: random numbers table generated by the pharmacy. Blinding: double‐blind; placebo and Mg were similar in appearance. Number dropped/lost: repeat enrolment (1), protocol violation (1). | |
| Participants | Location: Adult teaching hospital, Philadelphia, USA. Participants: 40 patients between the ages of 18 and 70 with acute asthma (ATS criteria) participated in the study if their initial PEFR was < 200 L/min. Exclusions: rectal T > 38 C, history of kidney disease, purulent sputum, infiltrate on chest radiography, or pregnancy. Patients with an initial PEFR > 200 L/min or PEFR that doubled following therapy were also excluded. | |
| Interventions | Standard of care: all patients with a PEFR < 200 L/min received a nebulised treatment of metaproterenol sulfate (0.3 mL in 3.0 mL saline) or albuterol sulfate (0.5 mL in 2.5 mL of saline) at the discretion of the physician. All patients received 125 mg of methylprednisolone intravenously. Theophylline loading based on serum levels. Forty‐five to sixty minutes after the first nebulisation treatment, a second nebulisation treatment was given. Fifteen minutes later a repeated PEFR was obtained. Patients who did not double their PEFR were considered poor responders and were randomised Treatment: infusion of 1.2 g of magnesium sulfate in 50 mL of saline over 20 minutes. Control: saline placebo in 50 mL of saline over 20 minutes. | |
| Outcomes | Clinical score: not reported. Admission to hospital: no criteria; based on assessment by the treating physician. Pulmonary functions: PEFR. Lab values: serum Mg and theophylline levels. Vital signs: PR, RR, BP. Side effects:deep tendon reflexes. Timing: 5, 10, 15, 20, 30, 45 minutes after infusion. | |
| Notes | Dr. Skobeloff contacted and provided additional references. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | Central pharmacy randomisation |
Tiffany 1993.
| Methods | Randomisation: computerised, random‐number generation under the control of the hospital pharmacy. Concealment of allocation was appropriate. Blinding: double‐blind, similar appearance of the study drugs. Number dropped/lost: not reported. | |
| Participants | Location: single adult teaching hospital, Detroit, USA. Participants: 48 asthmatic patients (ATS Criteria) aged 18 to 60 years with initial PEFR less than 200 L/min who failed to double their initial PEFR after two standardized albuterol treatments. Exclusions: PEFR > 200 L/min pre‐treatment, first episode of wheezing, history of chronic bronchitis or emphysema, oral T >38.2, history of renal failure, history of congestive heart failure, or requiring tracheal intubation. | |
| Interventions | Standard of care: All subjects received nebulised albuterol (2.5 every 30 minutes), standarized aminophylline (loading dose and infusion to keep serum levels at 15mg/l) and steroid therapy (125 mg methylprednisolone IV). Treatment: two groups: A loading dose of magnesium sulfate, 2g IV over 20 minutes followed by 2 g/h over 4 hours (infusion) or magnesium sulfate, 2 g over 20 minutes followed by placebo infusion (bolus). Control: saline loading dose and infusion (placebo). | |
| Outcomes | Clinical scores: none Admission: no criteria applied (at the discretion of the treating physician). Pulmonary Functions: PEFR and FEV‐1. Lab values: serum Mg level. Vital signs: not reported. Side effects: not reported. Timing: measurements were recorded at the start of the loading dose, and 20, 50, 80, 200, and 260 minutes later. | |
| Notes | Dr. Tiffany responded to correspondence but unable to provide additional data. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | Central pharmacy randomisation |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Bernstein 1995 | Patients were chronic, stable asthmatics. |
| Brunner 1985 | A laboratory study of the effect of parenteral magnesium on pulmonary function, plasma cAMP and histamine in bronchial asthma. |
| Cairns 1996 | A laboratory study of the effect of IV magnesium in the neutrophil superoxide production in asthmatic patients. |
| Chande 1992 | Patients were chronic, stable asthmatics; patients did not present to the emergency room setting. |
| Hicks Keen 1995 | A review of intravenous magnesium sulfate for acute asthma. |
| Kufs 1990 | Letter to the editor. |
| Kuitert 1991 | A case report rather than a RCT. |
| Landon 1993 | A review of the role of magnesium in regulation of lung function. |
| McDonald 1994 | Review of the new approaches to management of asthma. |
| McLean 1994 | A review of magnesium and its therapeutic uses. |
| McNamara 1989 | A case report rather than a RCT. |
| Meral 1996 | Not a RCT. |
| Noppen 1990 | Patients were not randomized to receive magnesium sulfate or placebo treatment early in the ED treatment. Patients received treatment first morning after admission at 8:00 AM. |
| Okayama 1987 | Half of the patients included in the study were inpatients and could not be separated out from the patient sample. |
| Pabon 1994 | A case report rather than a RCT. |
| Rolla 1987 | Patients were chronic, stable asthmatics. |
| Rolla 1988 | Patients were not randomised to receive magnesium sulfate or placebo early in the ED treatment. Long‐acting theophylline preparations were stopped 24 hours before each study day. Subjects were studied on two separate occasions, one to seven days apart. All studies began between 8:30 and 9:00 AM. (Not an ED study; patients were only recruited from the ED.) |
| Schiermeyer 1994 | A case report rather than a RCT. |
| Sharma 1994 | A laboratory study of the effect of parenteral magnesium sulfate on pulmonary sulfate on pulmonary functions in bronchial asthma. |
| Sydow 1993 | A case report rather than a RCT. |
Contributions of authors
BHR: Initiated the review, wrote the protocol, performed searches, assessments, analysis, and primary author of review. Bretzlaff JA: assisted with searches, performed selection for inclusion and quality assessments, data extraction and data entry, and manuscript review. Bourdon C: Protocol development, study assessment and manuscript review. Bota GW: Protocol development, study assessment and manuscript review. Camargo CA Jr: Provided methodological input, statistical support, and assumed major editorial role.
Sources of support
Internal sources
University of Alberta, Edmonton, Alberta, Canada.
Acute Care Research Group, Sudbury Regional Hospital, Sudbury, Ontario, Canada.
NHS Research and Development, UK.
External sources
Canadian Association of Emergency Physicians, Ottawa, Ontario, Canada.
National Institute of Health (NIH HL‐03533), Bethesda, Maryland, USA.
Declarations of interest
The authors who have been involved in this review have done so without any known conflicts of interest. They are neither involved with the primary studies nor affiliated with any pharmaceutical company that produces magnesium sulfate.
Edited (no change to conclusions)
References
References to studies included in this review
Bloch 1995 {published data only}
- Bloch H, Silverman R, Mancherje N, Grant S, Jagminas L, Scharf SM. Intravenous magnesium sulfate as an adjunct in the treatment of acute asthma. Chest 1995;107:1576‐81. [DOI] [PubMed] [Google Scholar]
Ciarallo 1997 {published data only}
- Ciarallo L, Sauer AH, Shannon MW. Intravenous magnesium therapy for moderate to severe pediatric asthma: Results of a randomized, placebo‐controlled trial. The Journal of Pediatrics 1996;129:809‐14. [DOI] [PubMed] [Google Scholar]
Devi 1997 {published data only}
- Devi PR, Kumar L, Singhi SC, Prasad R, Singh M. Intravenous magnesium sulfate in acute severe asthma not responding to conventional therapy. Indian Pediatrics 1997;34:389‐97. [PubMed] [Google Scholar]
Green 1992 {published data only}
- Green SM, Rothrock SG. Intravenous magnesium for acute asthma: Failure to decrease emergency treatment duration or need for hospitalization. Annals of Emergency Medicine 1992;21(3):260‐5. [DOI] [PubMed] [Google Scholar]
Silverman 1996 {published and unpublished data}
- Silverman R, Osborne H, Runge J, Feldman J, Scharf S, Mancherje N, et al. Magnesium sulfate as an adjunct to standard therapy in acute severe asthma [abstract]. Academic Emergency Medicine 1996;3:467‐8. [Google Scholar]
Skobeloff 1989 {published data only}
- Skobeloff EM, Spivey WH, McNamara RM, Greenspoon L. Intravenous magnesium sulfate for the treatment of acute asthma in the emergency department. JAMA 1989;262:1210‐3. [PubMed] [Google Scholar]
Tiffany 1993 {published data only}
- Tiffany BR, Berk WA, Todd IK, White SR. Magnesium bolus or infusion fails to improve expiratory flow in acute asthma exacerbations. Chest 1993;104:831‐4. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Bernstein 1995 {published data only}
- Bernstein WK, Khastgir T, Khastgir A, et al. Lack of effectiveness of magnesium in chronic stable asthma. A prospective, randomized, double‐blind, placebo‐controlled, crossover trial in normal subjects and in patients with chronic stable asthma. Archives of Internal Medicine 1995;155:271‐6. [DOI] [PubMed] [Google Scholar]
Brunner 1985 {published data only}
- Brunner EH, Delabroise AM, Haddad ZH. Effect of parenteral magnesium on pulmonary function, plasma cAMP, and histamine in bronchial asthma. Journal of Asthma 1985;22:3‐11. [DOI] [PubMed] [Google Scholar]
Cairns 1996 {published data only}
- Cairns CB, Kraft M. Magnesium attenuates the neutrophil respiratory burst in adult asthmatic patients. Academic Emergency Medicine 1996;3:1093‐7. [DOI] [PubMed] [Google Scholar]
Chande 1992 {published data only}
- Chande VT, Skoner DP. A trial of nebulized magnesium sulfate to reverse bronchospasm in asthmatic patients. Annals of Emergency Medicine 1992;21:1111‐5. [DOI] [PubMed] [Google Scholar]
Hicks Keen 1995 {published data only}
- Hicks Keen J. Intravenous magnesium sulfate for acute asthma. Journal of Emergency Nursing 1995;21:44‐6. [DOI] [PubMed] [Google Scholar]
Kufs 1990 {published data only}
- Kufs WM. Intravenous magnesium sulfate in acute asthma (letter). Journal of American Medical Association 1990;263:516‐7. [PubMed] [Google Scholar]
Kuitert 1991 {published data only}
- Kuitert LM, Kletchko SK. Intravenous magnesium sulfate in acute, life‐threatening asthma. Annals of Emergency Medicine 1991;20:1243. [DOI] [PubMed] [Google Scholar]
Landon 1993 {published data only}
- Landon RA, Young EA. Role of magnesium in regulation of lung function. Journal of the American Dietetic Association 1993;93:674‐7. [DOI] [PubMed] [Google Scholar]
McDonald 1994 {published data only}
- McDonald AJ. New approaches to emergency management of asthma. Respiratory Management 1994;21:52‐8. [Google Scholar]
McLean 1994 {published data only}
- McLean RM. Magnesium and its therapeutic uses: A review. The American Journal of Medicine 1994;96:63‐76. [DOI] [PubMed] [Google Scholar]
McNamara 1989 {published data only}
- McNamara RM, Spivey WH, Skobeloff E, Jacubowitz S. Intravenous magnesium sulfate in the management of acute respiratory failure complicating asthma. Annals of Emergency Medicine 1989;18:197‐9. [DOI] [PubMed] [Google Scholar]
Meral 1996 {published data only}
- Meral A, Coker M, Tanac R. Inhalation therapy with magnesium sulfate and salbutamol sulfate in bronchial asthma. Turkish Journal of Pediatrics 1996;38:169‐75. [PubMed] [Google Scholar]
Noppen 1990 {published data only}
- Noppen M, Vanmaele L, Impens N, Schandevyl W. Bronchodilating effect of intravenous magnesium sulfate in acute severe bronchial asthma. Chest 1990;97:373‐6. [DOI] [PubMed] [Google Scholar]
Okayama 1987 {published data only}
- Okayama H, Aikawa T, Okayama M, Sasaki H, Mue S, Takishima T. Bronchodilating effect of intravenous magnesium sulfate in bronchial asthma. Journal of American Medical Association 1987;257:1076‐8. [PubMed] [Google Scholar]
Pabon 1994 {published data only}
- Pabon H, Monen G, Kissoon N. Safety and efficacy of magnesium sulfate infusions in children with status asthmaticus. Pediatric Emergency Care 1994;10:200‐3. [DOI] [PubMed] [Google Scholar]
Rolla 1987 {published data only}
- Rolla G, Bucca C, Bugiani M, Arossa W, Spinachi S. Reduction of histamine‐induced bronchoconstriction by magnesium in asthmatic patients. Allergy 1987;42:186‐8. [DOI] [PubMed] [Google Scholar]
Rolla 1988 {published data only}
- Rolla G, Bucca C, Caria E, Arossa W, Bugiani M, Cesano L, et al. Acute effect of intravenous magnesium sulfate on airway obstruction of asthmatic patients. Annals of Allergy 1988;61:388‐91. [PubMed] [Google Scholar]
Schiermeyer 1994 {published data only}
- Schiermeyer RP, Finkelstein JA. Rapid infusion of magnesium sulfate obviates need for intubation in status asthmaticus. American Journal of Emergency Medicine 1994;12:164‐8. [DOI] [PubMed] [Google Scholar]
Sharma 1994 {published data only}
- Sharma SK, Bhargava A, Pande JN. Effect of parenteral magnesium sulfate on pulmonary functions in bronchial asthma. Journal of Asthma 1994;31:109‐15. [DOI] [PubMed] [Google Scholar]
Sydow 1993 {published data only}
- Sydow M, Crozier TA, Zielmann S, Radke J, Burchardi H. High‐dose intravenous magnesium sulfate in the management of life‐threatening status asthmaticus. Intensive Care Medicine 1993;19:467‐71. [DOI] [PubMed] [Google Scholar]
Additional references
Beveridge 1996
- Beveridge RC, Grunfeld AF, Hodder RV, Verbeek PR. Guidelines for the emergency management of asthma in adults. Canadian Medical Association Journal 1996;155:25‐37. [PMC free article] [PubMed] [Google Scholar]
BTS 1997
- BTS. The British guidelines on asthma management: 1995 review and position statement. Thorax 1997;52:152‐6. [Google Scholar]
Camargo 1998
- Camargo CA Jr, on behalf of the MARC Investigators. Management of acute asthma in US emergency departments: The Multicenter Asthma Research Collaboration [abstract]. American Journal of Respiratory and Critical Care Medicine 1998:157. [Google Scholar]
Cates 1998
- Cates C. Comparison of holding chambers and nebulisers for beta‐agonists in acute asthma (Cochrane Review). Cochrane Library 1998, Issue Issue 3. [Google Scholar]
Jadad 1996
- Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ. Assessing the quality of reports of randomized clinical trials: is blinding necessary?. Controlled Clinical Trials 1996;17:1‐12. [DOI] [PubMed] [Google Scholar]
Lipworth 1997
- Lipworth BJ. Treatment of acute asthma. Lancet 1997;350(Suppl):18‐23. [DOI] [PubMed] [Google Scholar]
Littenberg 1988
- Littenberg B. Aminophylline treatment in severe acute asthma: A meta‐analysis. Journal of American Medical Association 1988;259:1678‐84. [PubMed] [Google Scholar]
NAEPP 1997
- National Asthma Education and Prevention Program. Expert Panel Report II: Guidelines for the Diagnosis and Management of Asthma. National Institutes of Health 1997:Bethesda, MD.
Oxman 1992
- Oxman AD, Guyatt GH. A consumer's guide to subgroup analyses. Annals of Internal Medicine 1992;116:78‐84. [DOI] [PubMed] [Google Scholar]
Plotnik 1998
- Plotnik LH, Ducharme FM. Efficacy and safety of combined inhaled anticholinergics and beta‐2‐agonists in the initial management of acute pediatric asthma (Cochrane Review). The Cochrane Library 1998, Issue Issue 3. [Google Scholar]
Rowe 1992
- Rowe BH, Keller JL, Oxman AD. Steroid use in the emergency department treatment of asthma exacerbations: A meta‐analysis. American Journal of Emergency Medicine 1992;10:301‐10. [DOI] [PubMed] [Google Scholar]
Rowe 1997
- Rowe BH, Spooner CH, Ducharme FM, Bretzlaff JA, Bota GW. The effectiveness of corticosteroids in the treatment of acute exacerbations of asthma: A meta‐analysis of their effect on relapse following acute assessment (Cochrane Review). Cochrane Library 1997, Issue Issue 2. [Google Scholar]