

Abstract
Importance:
Excess deaths provide estimates of total impact of major crises, such as the COVID-19 pandemic.
Objective:
To evaluate excess deaths trajectories during 2020–2023 across countries with accurate death registration and population age structure data; and to assess how excess death patterns and trajectories correlate with economic indicators of vulnerability overall and in different age strata.
Methods:
Data were used from the Human Mortality Database on 34 countries. Excess deaths were calculated for 2020-2023 (to 2/26/2023) using 2017-2019 as baseline reference, with weekly expected death calculations and adjustment for 5 age strata. Countries were divided into less and more vulnerable; the latter had per capita nominal GDT<$30,000, Gini>0.35 for income inequality and/or at least 2.5% of their population living in poverty.
Results:
Excess deaths (as proportion of expected deaths, p%) were strongly inversely correlated with per capita GDP (r=−0.61), strongly correlated with proportion living in poverty (r=0.65) and modestly correlated with income inequality (r=0.42). The 17 less vulnerable countries had 201,471 excess deaths versus 2,005,380 among the 17 more vulnerable countries. The USA would have had 1.50 million fewer deaths if it had the performance of Sweden, 1.13 million fewer deaths if it had the performance of Finland, and 0.93 million fewer deaths if it had the performance of France. Excess deaths started deviating in the two groups after the first wave when correlational patterns with the 3 economic indicators also started to emerge. Between-country heterogeneity diminished over time within each of the two groups. Less vulnerable countries had mean p%=−0.4% and 0.9% in 0-64 and >65 year-old strata while more vulnerable countries had mean p%=8.3% and 9.0%, respectively. Certain countries performed substantially worse (USA, Canada, Chile, UK) or better (France, Poland, Slovenia) in the non-elderly than in the elderly. Usually lower death rates were seen in children 0-14 years old during 2020-2023 versus pre-pandemic years.
Conclusion:
While the pandemic hit some countries earlier than others, country vulnerability dominated eventually the cumulative impact. Half of the analyzed countries witnessed no substantial excess deaths versus pre-pandemic levels, while the other half suffered major death tolls.
Keywords: COVID-19, mortality, excess deaths, bias, demography
INTRODUCTION
Estimates of excess deaths are considered to offer an aggregate picture of the impact on overall mortality during the COVID-19 crisis.1,2 Excess deaths capture the composite of deaths due to SARS-CoV-2, indirect effects of the pandemic, and the effects of the measures taken during the crisis (both positive and negative). Three years after COVID-19 was proclaimed as a pandemic by the WHO, one can have a mature picture of the evolution of the excess deaths in different countries over time. This is most reliable in countries that have adequately complete death registration data and information on the evolution of the age structure of their population, so that proper age-adjustments can be made.3 The performance of different countries in terms of cumulative deaths may have varied markedly. Moreover, the trajectory of excess deaths over time has also shown diverse patterns across countries over time, as different countries witnessed more excess deaths during different periods.
Here, we evaluate the trajectories of excess deaths over time in the period between January 2020 and March 2023 in 34 countries with the most reliable data. We try to get insights on how and why these trajectories have diverged across different countries overall and within different age groups. We categorize these countries in two groups of more and less vulnerable ones. Vulnerability is judged based on per capita gross domestic product (GDP) as well as income inequality and proportion of population below the poverty level, since the COVID-19 crisis disproportionately affected the poor and the disadvantaged.4-6
METHODS
Excess death calculations, eligible countries, and mortality data
We performed excess death calculations using methods similar to those we have used in our previously published work for the period of 2020-2021.3 In brief, we used the average of the years 2017-2019 as the baseline and included age-adjustment in the calculations, by considering data in 5 age strata (0–14, 15–64, 65–75, 75–85, and >85 years old). For each age stratum, we obtained the average mortality, the number of deaths per million for the population of the specific age stratum and estimated the expected deaths during each week of the pandemic periods of interest, correcting for the population size in the specific age stratum and summing expected deaths across the population strata.
We used the Human Mortality Database (https://www.mortality.org),7 specifically the Short Term Mortality Fluctuations (STMF) file (https://www.mortality.org/Public/STMF/Outputs/stmf.csv) that includes weekly all-cause deaths and mortality values allowing the population size to be calculated as their ratio for each week. Only countries that have excellent death registration and include data with weekly deaths in the STMF during the period from 2017 until at least the second half of 2022 were considered, so as to avoid spurious changes in recorded deaths over time due to changes in death registration. STMF had data from 34 such eligible countries at the time we downloaded the database (March 2023). Data extended to include part of 2023 for 31 countries (to 26 February 2023). Italy was covered to the end of 2022 and the last few weeks of 2022 were missing for Canada and Australia.
We calculated weekly excess deaths and focused on cumulative excess deaths up to the end of each week starting from the first week of 2020. We proceeded with these calculations until the latest week with available death data in each country. The Human Mortality database uses ISO weeks that end on Sunday, e.g. the first week of 2020 ends on Sunday January 5, 2020. We expressed the excess death impact as percentage above the expected deaths, p%. E.g. p%=2% means that excess deaths (observed minus expected deaths) are 2% of the expected deaths for the period of interest and p%=−1% means that the observed deaths are 1% lower than the expected deaths (“death deficit”).
All analyses use 2017-2019 as the reference period to calculate expected deaths. We have previously shown that relative country performance tends to be similar with shorter and longer windows for the reference period,8 even if exact absolute excess deaths may vary with different modeling options.8
Classification of countries in vulnerability groups
We classified the 34 countries with available eligible data into two groups of 17 countries each. The more vulnerable countries’ group included countries that had per capita nominal GDP below $30,000, large income inequality (Gini>0.35) and/or sizeable percentage (at least 2.5%) of their population in poverty (defined as living with <$5.50 per day (2011 PPP values)). The less vulnerable group countries’ group had none of these vulnerability features.
Information on these three indicators was obtained from World Bank for per capita nominal GDP (2021 estimates;9 OECD for Gini of income inequality (2020 or more recent estimates, "Income Distribution Database". OECD.org. Measure: Gini (disposable income, post taxes and transfers), coupled with data from the World Bank for countries that are not OECD members;10,11 and Wikipedia (2019 for most recent data of proportion of population living in poverty.12
The magnitude of the differences across more and more vulnerable countries can be best appreciated if one estimates how many fewer deaths a more vulnerable country would have had if it had the same performance as a less vulnerable country. To obtain this number, the absolute excess deaths of the more vulnerable country are multiplied by the difference in p% between the compared countries. Illustratively, we present such absolute numbers of deaths that could have been saved for the USA, if it had the performance of Sweden, Finland, or France.
Analyses of cumulative excess deaths over time
Cumulative excess deaths for each country were analyzed for each week starting with week 1, 2020 and until the most recent available data. For the few countries with missing data on the last few weeks in this interval, the last available value was carried forward. Main milestones were: week 12 (22-March 2020, at the start of the impact of the pandemic wave in Europe and the USA), mid-2020, end-2020, mid-2021, end-2021, mid-2022, end-2022, and latest available (26 February 2023 or latest). The mean p% and its standard deviation for cumulative excess deaths at each time point of interest was calculated separately for the more vulnerable and for the less vulnerable countries.
We also examined the Pearson and Spearman correlation coefficients for the correlation between the P at each main milestone and the three economic variables (GDP per capita, Gini coefficient, percentage of population living in poverty) across all 34 countries.
Age subgroups
We performed similar analyses splitting excess death estimates in non-elderly (0-64 years, i.e. combining the 0-14 and 15-64 years old strata) and elderly people (65 years old and above, i.e. combining the 65-74, 75-84, and over 85 years old strata). We also examined whether there were excess deaths in the 0-14 age bin, i.e. among children in particular, in any of the 34 countries.
RESULTS
Cumulative excess deaths and vulnerability indicators
Table 1 shows the estimated cumulative excess deaths during the entire pandemic period and the 3 vulnerability indicators for each of the 34 countries (scatterplot in Figure 1). The Pearson correlation coefficients of p% with GDP per capita, Gini coefficient, and percentage living in poverty across the 34 countries were −0.61, 0.42, and 0.65. The corresponding Spearman rank correlation coefficients were −0.71, 0.25, and 0.61, respectively.
Table 1.
Excess deaths and vulnerability indicators
| Country | Excess deaths, p (%)* |
Excess deaths, absolute* |
Reported COVID-19 deaths* |
Per capita nominal GDP ($) |
Gini for income inequality |
Living in poverty (%) |
|---|---|---|---|---|---|---|
| New Zealand | −3.42 | −3,931 | 2,542 | 48,781 | 0.320 | No data |
| Denmark | −2.59 | −4,821 | 8,274 | 68,008 | 0.268 | 0.40 |
| Sweden | −2.51 | −7,409 | 23,634 | 61,029 | 0.276 | 0.60 |
| Australia | −2.08 | −10,714 | 16,100 | 60,443 | 0.318 | 0.74 |
| South Korea | −2.03 | −17,373 | 7,067 | 34,998 | 0.331 | 0.74 |
| Norway | −1.62 | −2,230 | 5,175 | 89,154 | 0.263 | 0.20 |
| Luxembourg | −0.81 | −114 | 1,207 | 133,590 | 0.305 | 0.30 |
| Iceland | 0.98 | 73 | 199 | 68,728 | 0.250 | 0.04 |
| Israel | 1.47 | 2,270 | 12,236 | 52,171 | 0.342 | 2.47 |
| Switzerland | 1.50 | 3,417 | 14,203 | 91,992 | 0.316 | 0.14 |
| Finland | 1.59 | 2,847 | 8,739 | 53,655 | 0.265 | 0.10 |
| Canada | 2.33 | 20,184 | 46,931 | 51,988 | 0.280 | 0.74 |
| Netherlands | 2.93 | 15,376 | 22,990 | 57,768 | 0.304 | 0.30 |
| Germany | 3.25 | 101,657 | 167,812 | 51,204 | 0.296 | 0.50 |
| Belgium | 3.39 | 12,098 | 33,616 | 51,247 | 0.262 | 0.20 |
| France | 3.71 | 72,617 | 160,917 | 43,659 | 0.292 | 0.11 |
| Portugal# | 4.15 | 15,353 | 26,033 | 24,568 | 0.310 | 0.90 |
| Spain# | 5.09 | 69,711 | 118,434 | 30,104 | 0.320 | 2.50 |
| Slovenia# | 5.24 | 3,610 | 7,067 | 29,291 | 0.246 | 0.10 |
| UK# | 5.51 | 111,636 | 14,203 | 46,510 | 0.355 | 0.86 |
| Hungary# | 6.04 | 25,156 | 48,658 | 18,728 | 0.286 | 1.80 |
| Austria | 6.53 | 17,524 | 21,872 | 53,638 | 0.274 | 0.80 |
| Italy# | 6.63 | 134,220 | 184,642 | 35,658 | 0.330 | 3.05 |
| Estonia# | 6.76 | 3,421 | 2,926 | 27,944 | 0.305 | 1.30 |
| Greece# | 7.50 | 29,934 | 34,779 | 20,193 | 0.308 | 3.40 |
| Croatia# | 7.76 | 13,088 | 17,895 | 17,685 | 0.292 | 1.80 |
| Latvia# | 8.64 | 7,774 | 6,255 | 21,148 | 0.355 | 2.00 |
| Slovakia# | 9.97 | 17,646 | 20,938 | 21,392 | 0.222 | 1.30 |
| Czechia# | 10.26 | 34,014 | 42,303 | 26,821 | 0.248 | 0.30 |
| Poland# | 10.90 | 146,894 | 118,779 | 18,000 | 0.281 | 1.20 |
| Lithuania# | 11.40 | 13,976 | 9,535 | 23,723 | 0.357 | 1.40 |
| Chile# | 12.67 | 47,069 | 64,230 | 16,265 | 0.460 | 4.40 |
| USA# | 13.99 | 1,270,578 | 1,107,690 | 70,249 | 0.375 | 1.50 |
| Bulgaria# | 18.05 | 61,300 | 38,184 | 12,222 | 0.408 | 8.20 |
Figure 1.

Scatterplot of excess deaths p% against the per capita GDP also showing countries with substantial income inequality and/or high proportion of population living in poverty. The left panel shows the data for the entire countries’ populations and the other two panels show the strata or non-elderly and elderly using a cut-off of 65 years.
Table 1 also shows the total absolute numbers of excess deaths. Across the 34 countries they amounted to a total of 2,210,782 excess deaths, 57% of which were accounted by the USA alone (1,270,578). There were only 201,471 excess deaths in the 17 countries of the less vulnerable group (557 per million in the total population of 361,730,277 people) versus 2,005,380 in the 17 countries of the more vulnerable group (3,180 per million in the total population of 630,541,384 people).
The USA would have had 1.50 million fewer deaths if it had the performance of Sweden, 1.13 million fewer deaths if it had the performance of Finland, and 0.93 million fewer deaths if it had the performance of France.
Cumulative excess deaths in the two vulnerability groups over time
Table 2 shows the mean and standard deviation of the excess death estimates p% for more and less vulnerable countries, respectively and Figure 2 shows the trajectories in each country over time. Both groups of countries had similar estimates of modest death deficit for the first 12 weeks of 2020 as compared with the average of 2017-2019 and both groups had similar standard deviations. By mid-2020, both groups had reverted from this initial death deficit to a picture that resembled 2017-2019 for the mean p% (no sizeable excess or deficit), but there was large between-country heterogeneity already, especially in the more vulnerable group. Some countries had already reached excess deaths exceeding 8% (UK 14.9%, Spain 14.3%, Chile 11.4%, USA 9.9%, Belgium 9.0%, Italy 8.7%) – all in the more vulnerable group except for Belgium (see Figure 2).
Table 2.
Mean and standard deviation of excess deaths p% (% of expected deaths) at different time points for more and less vulnerable countries
| Time point | Excess deaths in less vulnerable countries, mean p% (standard deviation) |
Excess deaths in more vulnerable countries, mean p% (standard deviation) |
|---|---|---|
| 22 March 2020 (week 12) | −7.4 (3.7) | −7.7 (3.9) |
| Mid-2020 (week 26) | −1.6 (4.7) | 0.0 (8.2) |
| End-2020 (week 52) | 1.2 (5.7) | 8.2 (4.6) |
| Mid-2021 (week 78) | −0.7 (4.4) | 9.8 (4.4) |
| End-2021 (week 104) | 0.4 (4.2) | 11.8 (4.8) |
| Mid-2022 (weak 130) | 0.5 (3.0) | 10.4 (4.8) |
| End-2022 (weak 156) | 1.1 (3.0) | 9.8 (4.0) |
| Latest update to 26 February 2023 (weak 165) |
0.7 (2.8) | 9.1 (4.0) |
Figure 2.
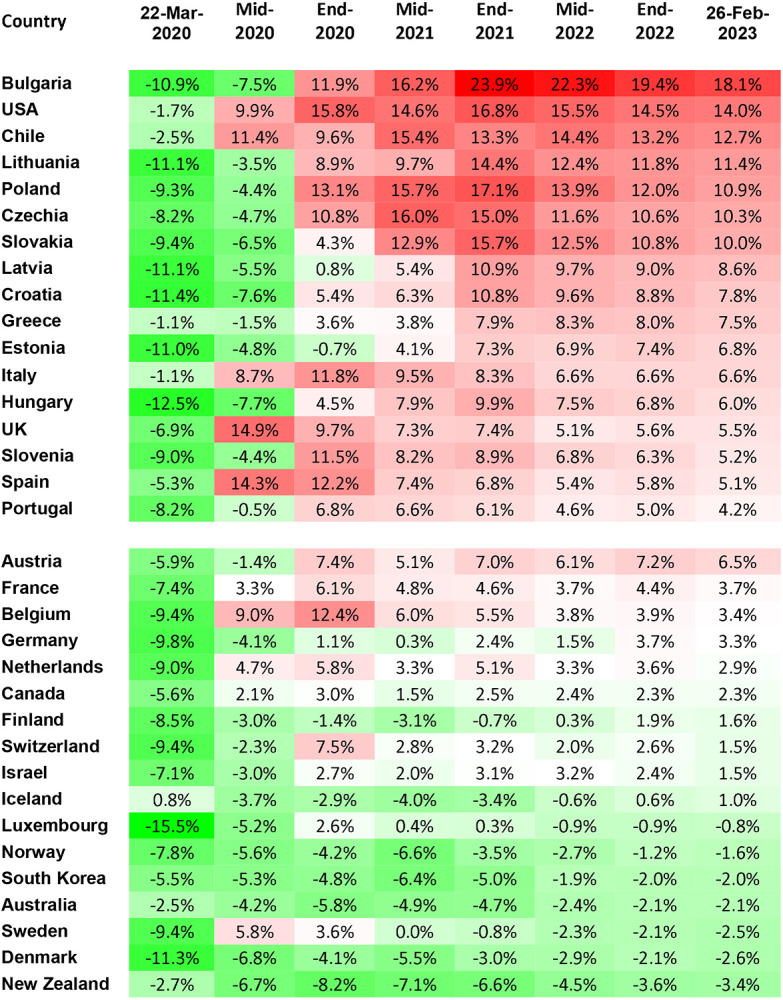
Estimated cumulative excess deaths at different timepoints during 2020-2023 in 34 countries grouped into more vulnerable (upper group) and less vulnerable (lower group). The color scale corresponds to excess deaths increasing from green to red.
After mid-2020, the less vulnerable group of countries maintained until February 2023 a very small mean of excess deaths. The mean value never exceeded 1.2% and it was just 0.7% by the latest update. Their between-country heterogeneity also diminished during 2021-2023. The standard deviation at the latest update was less than half the standard deviation of end-2020 in that group. This is because countries that initially had prominent death deficits compared with 2017-2019 lost much or all of these death deficits by the latest follow-up; while countries with substantial excess deaths in 2020 or early 2021 improved markedly their performance subsequently. As of the latest update in March 2023, with the exception of Austria (cumulative excess deaths 6.5%), all countries in the less vulnerable group had cumulative p% estimates in the narrow range −3.4% to 3.7%.
Conversely, in the group of more vulnerable countries the mean excess death estimate reached 8.2% by the end of 2020. Between-country heterogeneity diminished markedly compared with mid-2020, because although many of these countries had been spared in the first wave, only Latvia and Estonia were still spared by end-2020 (standard deviation of p% fell from 8.2% to 4.6%). The mean excess death estimate continued to increase during 2021 reaching 9.8% by mid-2021 and 11.8% by end-2021, while between-country heterogeneity remained stable at modest levels. During 2022 and into 2023, the mean excess death estimate decreased modestly over time and some further decrease was seen also in the standard deviation. As of the latest update in February 2023, all countries in the more vulnerable group have cumulative excess deaths (4.2-18.1%) exceeding the estimates of 16/17 countries in the least vulnerable group (the one exception being Austria).
As shown in table 3, there was no correlation between excess deaths p% and per capita GDP in 2020 but this changed in the next year and then it remained steady with correlation coefficients around −0.6 (Pearson) or −0.7 (Spearman). Similarly, there was no correlation between excess deaths p% and the proportion of poverty until mid-2020 but this changed in the next year and then it remained steady with correlation coefficients around 0.6 or higher. Throughout the 2020-2023 period, there was a modest correlation (correlation coefficients mostly between 0.2 and 0.4) between excess deaths p% and Gini coefficient for income inequality.
Table 3.
Correlations between excess death estimates p% and vulnerability indicators at different time points
| Time point | Pearson (Spearman) correlation with per capita nominal GDP |
Pearson (Spearman) correlation with Gini for income inequality |
Pearson (Spearman) correlation with proportion living in poverty |
|---|---|---|---|
| 22 March 2020 (week 12) | −0.07 (0.16) | 0.19 (0.18) | 0.12 (0.06) |
| Mid-2020 (week 26) | 0.02 (0.22) | 0.35 (0.22) | 0.05 (0.00) |
| End-2020 (week 52) | −0.30 (−0.34) | 0.24 (0.14) | 0.33 (0.28) |
| Mid-2021 (week 78) | −0.54 (−0.65) | 0.31 (0.19) | 0.50 (0.51) |
| End-2021 (week 104) | −0.59 (−0.69) | 0.32 (0.19) | 0.60 (0.58) |
| Mid-2022 (week 130) | −0.62 (−0.73) | 0.41 (0.24) | 0.68 (0.63) |
| End-2022 (week 156) | −0.61 (−0.71) | 0.41 (0.25) | 0.65 (0.61) |
| Latest update to 26 February 2023 (week 165) | −0.61 (−0.71) | 0.42 (0.25) | 0.65 (0.61) |
Age groups
Across all 34 countries, total excess deaths were 581,755 and 1,627,810 in the non-elderly (0-64 years) and elderly (65 and over) strata, respectively (Table 4). For the non-elderly, at the latest update on 26 February 2023, the mean of excess deaths was −0.4.% and 8.3% in the less and more vulnerable groups, respectively. For the elderly, the respective means were 0.9% and 9.0%. In the 17 less vulnerable countries, there were only 16,642 and 184,828 excess deaths in the non-elderly and non-elderly strata, respectively; non-elderly excess deaths accounted for only 8% of total excess deaths. In the 17 more vulnerable countries the respective numbers were 565,114 and 1,442,983, i.e. non-elderly excess deaths accounted for 28% of total excess deaths.
Table 4.
Excess deaths from January 2020 and up to latest update (26 February 2023) per age group*
| Country | 0-64 years, absolute |
0-64 years, p% |
65 years and over, absolute |
65 years and over, p% |
0-14 years, absolute |
0-14 years, p% |
|---|---|---|---|---|---|---|
| Denmark | −1,667 | −6.4% | −3,153 | −2.0% | −39 | −4.4% |
| Sweden | −1,828 | −6.0% | −5,581 | −2.1% | −72 | −5.7% |
| France | −10,139 | −3.4% | 82,756 | 5.0% | −561 | −5.0% |
| Luxembourg | −74 | −3.0% | −39 | −0.3% | 41 | 44% (NR) |
| Norway | −492 | −2.8% | −1,738 | −1.5% | −69 | −11.5% |
| New Zealand | −580 | −2.7% | −3,352 | −3.6% | −32 | −2.9% |
| Finland | −637 | −2.6% | 3,484 | 2.3% | −34 | −6.6% |
| Israel | −598 | −2.3% | 2,867 | 2.2% | −403 | −15.5% |
| Australia | −1,682 | −1.9% | −9,031 | −2.1% | −481 | −11.8% |
| Belgium | −690 | −1.3% | 12,788 | 4.2% | −393 | −20.6% |
| Switzerland | −160 | −0.6% | 3,577 | 1.8% | −28 | −2.2% |
| South Korea | 542 | 0.3% | −17,916 | −2.6% | −776 | −20.8% |
| Netherlands | 1,559 | 2.3% | 13,816 | 3.0% | −25 | −1.0% |
| Germany | 15,951 | 3.7% | 85,706 | 3.2% | −637 | −5.5% |
| Iceland | 47 | 3.9% | 27 | 0.4% | 20 | 60% (NR) |
| Austria | 2,409 | 6.4% | 15,115 | 6.6% | −99 | −8.8% |
| Canada | 14,682 | 9.2% | 5,501 | 0.8% | 879 | 13.4%** |
| Slovenia | −215 | −2.0% | 3,824 | 6.6% | −10 | −4.7% |
| Hungary | 2,049 | 2.3% | 23,107 | 7.0% | −113 | −7.4% |
| Croatia | 910 | 3.4% | 12,179 | 8.6% | −38 | −5.7% |
| Portugal | 2,368 | 4.7% | 12,984 | 4.1% | −108 | −9.1% |
| Poland | 14,944 | 5.0% | 131,950 | 12.6% | −845 | −12.5% |
| Spain | 11,245 | 6.2% | 58,467 | 4.9% | −203 | −4.4% |
| Czechia | 3,704 | 6.3% | 33,025 | 11.0% | −223 | −15.5% |
| Italy | 13,282 | 6.4% | 120,939 | 6.7% | −958 | −17.0% |
| Estonia | 682 | 7.3% | 2,740 | 6.6% | −7 | −3.9% |
| Slovakia | 3,039 | 7.5% | 14,607 | 10.7% | −51 | −4.0% |
| Latvia | 1,583 | 7.9% | 6,191 | 8.8% | −84 | −23.9% |
| Greece | 4,549 | 9.2% | 25,384 | 7.3% | −141 | −10.3% |
| Lithuania | 3,121 | 11.5% | 10,855 | 11.4% | −96 | −20.9% |
| UK | 35,759 | 11.8% | 75,876 | 4.4% | −805 | −6.5% |
| Bulgaria | 11,285 | 16.5% | 50,015 | 18.4% | −276 | −15.8% |
| Chile | 16,324 | 17.5% | 30,746 | 11.0% | −1,219 | −19.4% |
| USA | 440,485 | 19.0% | 830,094 | 12.3% | −3,803 | −4.0% |
Countries are listed in increasing p% among the 0-64 years old age stratum
For Canada, the 0-14 year old age band given in stmf is extrapolated from the 0-44 year age band in the original data https://www150.statcan.gc.ca/n1/tbl/csv/13100768-eng.zip. See https://www.mortality.org/File/GetDocument/Public/STMF/DOC/STMFNote.pdf for stmf methods.
NR: not reliable (given the very small population and extremely small number of deaths of children, excess deaths can be markedly influenced by single anomalies, e.g. in Iceland there were only 6 reported deaths in that age stratum in 2019 (less than a third versus 2017) and in Luxembourg there were 76 in 2022 (more than double versus the 2017-2019 average)
Most countries had similar performance in terms of p% in the non-elderly and elderly strata, with some notable exceptions (Figure 1). USA, Canada, Chile, and UK had a much higher p% in the non-elderly than in the elderly (difference >6.5%). In fact, USA had the highest excess deaths than any country among the non-elderly (p%=19.0%), while Canada had high excess deaths in the non-elderly (p%=9.2%), but no excess deaths in the elderly (p%0.8%). The higher excess death P estimates in the non-elderly rather than elderly was manifest in these countries from the first months of the pandemic and persisted subsequently. Conversely, France, Poland, and Slovenia performed much better in the non-elderly than in the elderly (difference > 7.5%); both France and Slovenia had a death deficit in the non-elderly.
For children in particular (0-14 years), all countries with sizeable population of children to have meaningful results had lower death rates during 2020-2023 versus 2017-2019 with the exception of Canada. Numerically, the largest death deficits came actually from more vulnerable countries, specifically USA (−3,803), Chile (−1,219), Poland (−845) and UK (−805).
DISCUSSION
Analysis of data during 2020-2023 from 34 countries with reliable mortality data and information of population age structure over time shows that half of these countries had minimal excess deaths or even death deficits during 2020-2023 versus the 3 pre-pandemic years, while the other half had substantial excess deaths. The performance of different countries could be grouped based on vulnerability indicators pertaining to their wealth, income inequality and poverty. Excess deaths during 2020-2023 was strongly inversely correlated with per capita income, strong correlated with proportion of the population living in poverty and modestly correlated with the Gini coefficient of income inequality. These correlational patterns were not seen during the first wave, but they became manifest and persistent subsequently.
Some less vulnerable countries transiently had notable excess deaths during 2020 and/or 2021. However, eventually by March of 2023 all of them (with the exception of Austria) had no major excess deaths considering the entire 2020-2023 period. This is consistent with the possibility that transient peaks of excess deaths in these countries were to a large extent due to the demise of frail elderly individuals, e.g. in long-term care facilities, with limited life expectancy.13 For individuals with life expectancy less than 2-3 years, premature deaths in the early phases of the pandemic, will have no impact on the excess death estimates when the whole 2020-2023 period is considered.13,14 The group of less vulnerable countries have high income, no prominent income inequalities and no major proportion of their population living in poverty. All of them also have practically universal health coverage. Thus, they may have avoided a substantial number of excess deaths among disadvantaged people. These countries also had more means to mobilize sufficient healthcare and public health resources. The exact ingredients of their success cannot be deciphered from ecological, country-level data. Regardless, these countries with large shares of elderly populations managed to pass the crisis with no more deaths than during the recent pre-pandemic years, after adjusting for their age structure.
Conversely, all countries that were categorized as more vulnerable based on their economic indicators fared poorly during 2020-2023. Their excess death estimates have decreased modestly after a peak by end-2021. This may reflect a relative contribution of the same phenomenon of some early deaths among frail elderly people with limited life expectancy, especially in Slovenia, Spain and UK, where the decrease in cumulative excess deaths was more prominent from 2020 to 2023. It may also reflect the more limited fatality of the Omicron waves in 2022-2023,15 especially given the almost ubiquitous prior infections and high rates of vaccination.16 However, cumulative excess death estimates remain high (and occasionally very high) in the more vulnerable countries. Some countries already reached high excess levels in early 2020, while others succumbed during the second wave. Again, the exact ingredients of their failure cannot be pinpointed in detail. However, the common denominator for these countries was their less robust economies and/or large share of poor, disadvantaged people. COVID-19 was a crisis of inequalities and many measures taken may even have fostered worsening inequalities.
The USA is a striking case, with extremely high cumulative excess death rates despite high per capita GDP. USA income inequality is high and many people live in poverty, while 16% lack health coverage. Up to 27-fold differences in the rates of COVID-19 death rates in strata defined by race, gender, and educational achievement have been described in the USA.6 Area deprivation may be a risk factor for COVID-19 mortality especially among minorities.17,18 Moreover, a large share of excess deaths apparently are due to sharply increasing deaths due to overdose19 and of deaths due to suboptimal access to care during 2020-2023.20 Such non-infectious causes may largely explain the exceptionally high excess death p% estimate among USA non-elderly people. It was also accompanied by a very high proportion (35%) of excess deaths contributed by the under-65 age stratum.
Income inequalities have been strongly associated with COVID-19 deaths also in other countries among the more vulnerable group, e.g. in Spain21,22 and Chile.23 The pandemic widened all-cause pre-existing mortality gaps according to income even in some less vulnerable countries, such as the Netherlands24 and Sweden.25 In a vicious circle, the pandemic caused more poverty worldwide.26
The gap between the more and less vulnerable group of countries was overall similar among the elderly and the non-elderly. However, a few countries (USA, Canada, Chile, UK) had a very poor performance specifically among the non-elderly (as compared with their performance in the elderly, while some others (France, Poland, Slovenia) showed the opposite pattern. Population obesity rates are markedly different in these two groups of countries (28-36% versus 20-23%) and additional differences in the background health status of non-elderly individuals may explain these patterns, e.g. overdose and poor health access in the USA – as discussed above. USA, Chile, and UK were categorized here are more vulnerable countries, while Canada was categorized as less vulnerable. However, the classification is not absolute. Canada also has a modest proportion of people living in poverty (0.74%), and data from Ontario suggest that low income and low educational attainment increased the risk of COVID-19 deaths.27 Also some data from Canada (British Columbia) shows that death rates from overdose more than doubled during the pandemic versus 2019).28
For children in particular, the available data suggest consistently fewer deaths during 2020-2023 compared with the pre-pandemic years. This may be due to the exceptionally low infection fatality rate of SARS-CoV-2 among children,29 plus the almost complete disappearance of influenza for 2 years. More granular data would need to be examined to see if the death deficit extends also to adolescents and very young adults.
Our study has some limitations. First, excess death estimates depend on modeling assumptions that may affect the absolute values.30,31 For example, if one were to expect a trend of decreasing mortality rates over the years, then the estimated excess deaths would be higher than what we calculated using the 2017-2019 average as reference. However, even if mortality rates have decreased in many countries over time, there is no guarantee that this pattern should continue, especially among the increasingly elderly and frail populations of high-income countries.8 Moreover, we have previously shown that different modeling assumptions do not affect the comparative performance of different countries.8 I.e. poor performers are consistently poor performers regardless of the exact modeling. Therefore, the contrast between less and more vulnerable countries is likely to be robust to modeling choices. Second, some of the data may have imperfections, e.g. some missing data on deaths in the last few weeks of the covered period, or inaccuracies in the inferred data for the population structure in each age bin and country over time. However, the data for the 34 chosen countries are likely to be the most reliable.
Extrapolations to countries with less reliable death and age structure data are precarious.32 Socioeconomic factors are likely to have had a major impact on mortality during 2020-2023 also in other countries, perhaps even to a larger extent than in the 34 countries that we analyzed.33-35 Their impact might have been even larger for non-COVID-19 deaths.33 Conversely, most countries not analyzed here have much younger populations and few frail elderly in long-term care facilities than the 34 analyzed countries, and thus deaths directly due to SARS-CoV-2 are expected to have been fewer.29,36 Third, we used three high-level economic indicators and these should be seen as surrogate of a mixture of many socioeconomic and other factors that operate at the individual, household, work, community, and societal level. Poor outcomes during the COVID-19 crisis are likely to have been determined by a large web of inter-related factors.
Acknowledging for these caveats, the country-level analyses that we performed offer a picture of how countries succeeded or failed in dealing with this major crisis. Half the countries went through the 3 crisis years without witnessing substantial excess deaths versus their pre-pandemic levels, while others suffered major death tolls. Continuous monitoring of excess death patterns may be useful, given that the consequences of the COVID-19 crisis and several measures taken may continue to have an impact for several years.
Data statement:
All data are in the manuscript and in publicly available databases.
Funding:
NIH R35 GM122543 (Levitt)
Footnotes
Conflicts of interest: None
Contributor Information
John P.A. Ioannidis, Department of Medicine, of Epidemiology and Population Health, of Biomedical Data Science, and of Statistics, and Meta-Research Innovation Center at Stanford (METRICS), Stanford University, Stanford, CA 94305, USA
Francesco Zonta, Department of Biological Sciences, Xi’An Jiaotong Liverpool University, Suzhou 215123, China.
Michael Levitt, Department of Structural Biology, Stanford University, Stanford, CA 94305, USA.
REFERENCES
- 1.Kiang MV, Irizarry RA, Buckee CO, Balsari S. Every body counts: measuring mortality from the COVID-19 pandemic. Ann Intern Med. 2020. Dec 15;173(12):1004–1007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Msemburi W, Karlinsky A, Knutson V, Aleshin-Guendel S, Chatterji S, Wakefield J. The WHO estimates of excess mortality associated with the COVID-19 pandemic. Nature. 2023;613(7942):130–137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Levitt M, Zonta F, Ioannidis JPA. Comparison of pandemic excess mortality in 2020-2021 across different empirical calculations. Envir Res. 2022;213:113754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Shiels MS, Haque AT, Haozous EA, Albert PS, Almeida JS, García-Closas M, Nápoles AM, Pérez-Stable EJ, Freedman ND, Berrington de González A. Racial and ethnic disparities in excess deaths during the COVID-19 pandemic, March to December 2020. Ann Intern Med. 2021;174(12):1693–1699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Commodore-Mensah Y, Cooper LA. Reversing the tide of racial and ethnic disparities in excess deaths during the COVID-19 pandemic. Ann Intern Med. 2021;174(12):1755–1756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pathak EB, Menard JM, Garcia RB, Salemi JL. Joint effects of socioeconomic position, race/ethnicity, and gender on COVID-19 mortality among working-age adults in the United States. Int J Environ Res Public Health. 2022;19(9):5479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wilmoth JR, Andreev K, Jdanov D, et al. Methods protocol for the human mortality database. University of California, Berkeley, and Max Planck Institute for Demographic Research, Rostock. URL: http://mortality.org [version 31/May/2007], 9, pp. 10–11. [Google Scholar]
- 8.Levitt M, Zonta F, Ioannidis JPA. Excess death estimates from multiverse analysis in 2009-2021. Eur J Epidemiol. 2023, 10.1007/s10654-023-00998-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.World Bank indicators, in: https://data.worldbank.org/indicator/NY.GDP.PCAP.CD?most_recent_value_desc=true, last accessed March 26, 2023. [Google Scholar]
- 10.Income Distribution Database. In: OECD.org, measure: Gini (disposable income, post taxes and transfers), last accessed March 26, 2023. [Google Scholar]
- 11.World Bank indicators, in: https://data.worldbank.org/indicator/SI.POV.GINI/
- 12.In: https://en.wikipedia.org/wiki/List_of_sovereign_states_by_percentage_of_population_living_in_poverty, last accessed March 26, 2023
- 13.Ballin M, Ioannidis JP, Bergman J, Kivipelto M, Nordström A, Nordström P. Time-varying risk of death after SARS-CoV-2 infection in Swedish long-term care facility residents: a matched cohort study. BMJ Open. 2022. Nov 24;12(11):e066258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Espuny Pujol F, Hancock R, Morciano M. Trends in survival of older care home residents in England: a 10-year multi-cohort study. Soc Sci Med 2021;282:113883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Friis NU, Martin-Bertelsen T, Pedersen RK, Nielsen J, Krause TG, Andreasen V, Vestergaard LS. COVID-19 mortality attenuated during widespread Omicron transmission, Denmark, 2020 to 2022. Euro Surveill. 2023. Jan;28(3). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Pilz S, Ioannidis JPA. Does natural and hybrid immunity obviate the need for frequent vaccine boosters against SARS-CoV-2 in the endemic phase? Eur J Clin Invest. 2023. Feb;53(2):e13906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Magesh S, John D, Li WT, Li Y, Mattingly-App A, Jain S, Chang EY, Ongkeko WM. Disparities in COVID-19 outcomes by race, ethnicity, and socioeconomic status: A systematic-review and meta-analysis. JAMA Netw Open. 2021. Nov 1;4(11):e2134147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Matthay EC, Duchowny KA, Riley AR, Thomas MD, Chen YH, Bibbins-Domingo K, Glymour MM. Occupation and educational attainment characteristics associated with COVID-19 mortality by race and ethnicity in California. JAMA Netw Open. 2022. Apr 1;5(4):e228406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.https://www.cdc.gov/nchs/pressroom/nchs_press_releases/2022/202205.htm, last accessed March 26, 2023.
- 20.Roth GA, Vaduganathan M, Mensah GA. Impact of the COVID-19 pandemic on cardiovascular health in 2020: JACC State-of-the-Art Review. J Am Coll Cardiol. 2022. Aug 9;80(6):631–640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Politi J, Martín-Sánchez M, Mercuriali L, Borras-Bermejo B, Lopez-Contreras J, Vilella A, Villar J; COVID-19 Surveillance Working Group of Barcelona; Orcau A, de Olalla PG, Rius C. Epidemiological characteristics and outcomes of COVID-19 cases: mortality inequalities by socio-economic status, Barcelona, Spain, 24 February to 4 May 2020. Euro Surveill. 2021. May;26(20):2001138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Fernández-Martínez NF, Ruiz-Montero R, Gómez-Barroso D, Rodríguez-Torronteras A, Lorusso N, Salcedo-Leal I, Sordo L. Socioeconomic differences in COVID-19 infection, hospitalisation and mortality in urban areas in a region in the South of Europe. BMC Public Health. 2022. Dec 12;22(1):2316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Mena G, Aburto JM. Unequal impact of the COVID-19 pandemic in 2020 on life expectancy across urban areas in Chile: a cross-sectional demographic study. BMJ Open. 2022. Aug 19;12(8):e059201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Wouterse B, Geisler J, Bär M, van Doorslaer E. Has COVID-19 increased inequality in mortality by income in the Netherlands? J Epidemiol Community Health. 2023. Apr;77(4):244–251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bell M, Hergens MP, Fors S, Tynelius P, de Leon AP, Lager A. Individual and neighborhood risk factors of hospital admission and death during the COVID-19 pandemic: a population-based cohort study. BMC Med. 2023. Jan 4;21(1):1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Decerf B, Ferreira FHG, Mahler DG, Sterck O. Lives and livelihoods: Estimates of the global mortality and poverty effects of the Covid-19 pandemic. World Dev. 2021. Oct;146:105561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wang L, Calzavara A, Baral S, Smylie J, Chan AK, Sander B, Austin PC, Kwong JC, Mishra S. Differential patterns by area-level social determinants of health in coronavirus disease 2019 (COVID-19)-related mortality and non-COVID-19 mortality: a population-based study of 11.8 million people in Ontario, Canada. Clin Infect Dis. 2023. Mar 21;76(6):1110–1120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Palis H, Bélair MA, Hu K, Tu A, Buxton J, Slaunwhite A. Overdose deaths and the COVID-19 pandemic in British Columbia, Canada. Drug Alcohol Rev. 2022. May;41(4):912–917. [DOI] [PubMed] [Google Scholar]
- 29.Pezzullo AM, Axfors C, Contopoulos-Ioannidis DG, Apostolatos A, Ioannidis JPA. Age-stratified infection fatality rate of COVID-19 in the non-elderly population. Environ Res. 2023;216(Pt 3):114655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Nepomuceno MR, Klimkin I, Jdanov DA, et al. Sensitivity analysis of excess mortality due to the COVID-19 pandemic. Population and Development Review 2022, 10.1111/padr.12475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Stang A, Standl F, Kowall B, et al. Excess mortality due to COVID-19 in Germany. J Infect. 2020;81(5):797–801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ioannidis JP, Zonta F, Levitt M. Flaws and uncertainties in pandemic global excess death calculations. Eur J Clin Invest 2023, in print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Nadarajah R, Wu J, Hurdus B, Asma S, Bhatt DL, Biondi-Zoccai G, Mehta LS, Ram CVS, Ribeiro ALP, Van Spall HGC, Deanfield JE, Lüscher TF, Mamas M, Gale CP. The collateral damage of COVID-19 to cardiovascular services: a meta-analysis. Eur Heart J. 2022. Sep 1;43(33):3164–3178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Khanijahani A, Iezadi S, Gholipour K, Azami-Aghdash S, Naghibi D. A systematic review of racial/ethnic and socioeconomic disparities in COVID-19. Int J Equity Health. 2021. Nov 24;20(1):248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Cajachagua-Torres KN, Quezade-Pinedo HG, Huayaney-Espinoza CA, Obeso-Manrique JA, Pena-Rodriguez VA, Vidal E, Huicho L. COVID-19 and drivers of excess death rate in Peru: a longitudinal ecological study. Heliyon 2022;8:e11948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Axfors C, Ioannidis JPA. Infection fatality rate of COVID-19 in community-dwelling elderly populations. Eur J Epidemiol. 2022. Mar;37(3):235–249. [DOI] [PMC free article] [PubMed] [Google Scholar]