

Abstract
Background: Ketamine has bronchodilation properties. The aim of the single-centre, evaluator-blinded, randomised clinical trial study was to evaluate whether continuous infusion of ketamine is associated with improvement in respiratory mechanics correlated with bronchospasm relief, as compared with continuous infusion of fentanyl.
Methods: Adult patients submitted to invasive mechanical ventilation were included if they had an acute severe bronchospasm, due to status asthmaticus or COPD exacerbation. They were randomised to ketamine or a standard IV analgesia with fentanyl, both in bolus and continuous infusion. Measurements of respiratory mechanics (airway resistance – Rsmax, dynamic compliance – Cdyn and intrinsic PEEP – PEEPi) both at baseline and 3 and 24 h after randomisation were performed. The main outcome of this study was to evaluate the improvement of Rsmax in 3 h of continuous infusion of the study drugs.
Results: Ketamine use was not associated with greater reduction in Rsmax when compared with fentanyl, either after 3 h (0 cm H2O L−1 s−1 ± 6 vs. −3 cm H2O L−1 s−1 ± 7.7, respectively; P = 0.16) or after 24 h (−3 cm H2O L−1 s−1 ± 17 vs. −3.5 cm H2O L−1 s−1 ± 13.7, respectively; P = 0.73). Patients randomized to the ketamine group did not have better improvements in delta PEEPi as compared with fentanyl in 3 h (P = 0.77) or in 24 h (P = 0.72).
Conclusions: In this study, ketamine use was not associated with improvement in ventilatory variables associated with bronchospasm.
Keywords: ketamine, fentanyl, COPD, asthma, bronchospasm, mechanical ventilation
Asthma and chronic obstructive pulmonary disease (COPD) are conditions characterised by airflow limitation. When not responding to standard treatments, both mandate critical care management and are potential life-threatening medical conditions [1, 2]. In acute exacerbations, an unwanted complication is severe bronchospasm, which may require the use of invasive mechanical ventilation (IMV) for its adequate management. Patients with these conditions usually present increased airway resistance, pulmonary hyperinsufflation and a large physiological dead space [3]. Usual pharmacological management of severe asthma and COPD exacerbation aims to resolve these alterations, and includes inhaled β-2 agonists, inhaled anticholinergics and glucocorticoids. Despite optimal pharmacological therapy, acute exacerbation of asthma that requires IMV is associated with a major economic and health burden, and COPD exacerbations in this scenario are associated with prolonged hospital stay and significant mortality [1, 2, 4]. Ketamine is a general anaesthetic molecule with sedative and analgesic properties [5]. Ketamine is supposed to produce airway relaxation and is commonly prescribed with this purpose, but the evidence supporting this effect is still scarce, especially in acute COPD exacerbations [6–8]. We aimed to evaluate whether continuous infusion of ketamine is associated with improvement in respiratory mechanics correlated with bronchospasm relief, as compared with continuous infusion of fentanyl – the most common IV continuous analgesia used, in critically ill, mechanically ventilated patients.
METHODS
This was a randomised, single-centre, evaluator-blinded, parallel-group trial, performed in a 59-bed tertiary intensive care unit (ICU) in Brazil, between January 2015 and December 2017. The protocol was approved by the local ethics committee (Plataforma Brasil 42324015.0.0000.5530) and was registered in ClinicalTrials.gov (NCT03000413).
Adult IMV ICU patients (age ≥ 18 years) were included if they had an acute severe bronchospasm, due to status asthmaticus or COPD exacerbation, with inspiratory resistance (Rsmax) ≥ 12 cm H2O L−1 s−1 and receiving at least intravenous corticosteroid, inhaled β-2 agonist and continuous intravenous analgosedation for optimisation of ventilator synchrony (Figures 1 and 2). All patients required neuromuscular blockade with continuous intravenous atracurium. Patients were excluded if they had a known adverse reaction to ketamine or an increase in Rsmax not associated with acute bronchospasm (bronchial obstruction, acute distress respiratory syndrome, pulmonary fibrosis) or if they had spontaneous ventilation. Patients were allocated using computer-generated block randomisation of size 8, and allocation concealment was provided by sequentially numbered, opaque, sealed envelopes. Patients received R-(−)ketamine (dextroketamine chloridrate, Laboratorio Cristália, Brazil) in a bolus dose of 2 mg kg−1 IV and a 24 hours (h) maintenance continuous infusion of 2 mg kg−1 h−1 or a standard IV continuous analgesia with fentanyl (bolus of 1 μg kg−1 min−1 and continuous infusion of 1 μg kg−1 min−1). Prolonged use of the study drugs (> 24 h) was at the discretion of the attending physician. All patients received IV continuous sedation (midazolam of propofol) according to the decision of the attending physician. Before the protocol was begun, baseline measurements were obtained for inspiratory pressure (Pinsp), Rsmax, intrinsic positive end-expiratory pressure (PEEPi) and dynamic compliance (Cdyn). The same variables were obtained at 3 and 24 h after randomisation. We performed the measurements of respiratory mechanics (Rsmax,, Cdyn, PEEPi) according to the literature on the topic [9]. All patients were ventilated in a Servo-i mechanical ventilator (Maquet, Getinge Group, Rastatt, Germany). The main outcome of this study was to evaluate the improvement of Rsmax in 3 h of continuous infusion of the study drugs. Secondary objectives were improvement in Rsmax in 24 h, improvement in Cdyn and PEEPi (3 and 24 h), duration of MV (in days) and ICU mortality.
FIGURE 1.
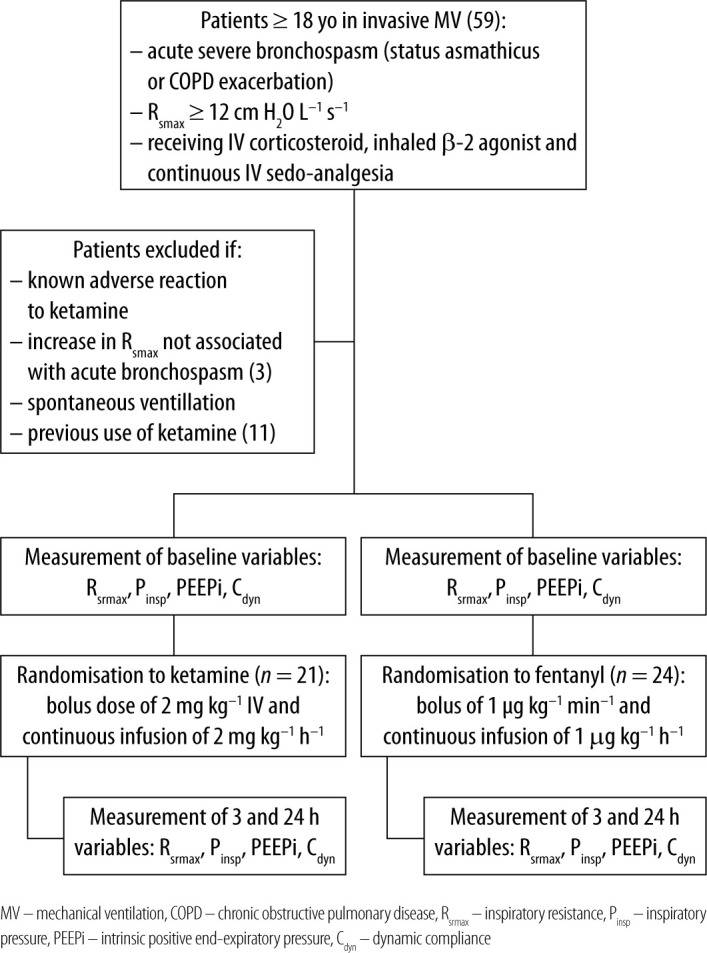
Flowchart of the study
FIGURE 2.
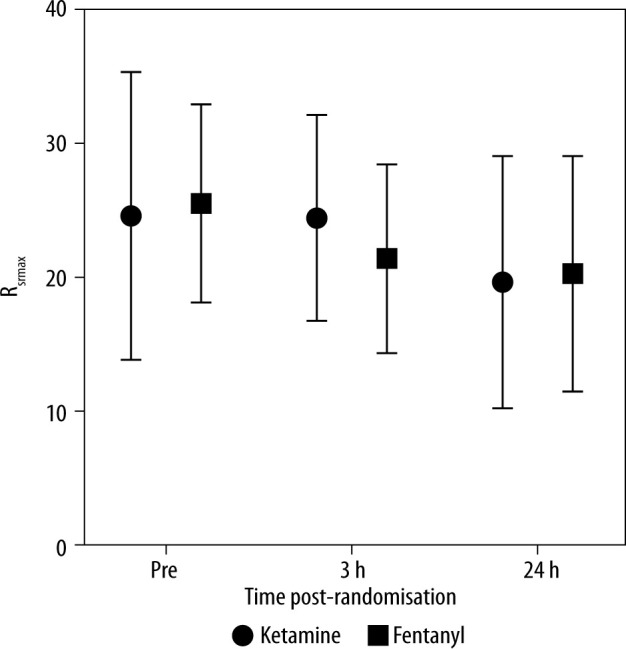
Variation in inspiratory resistance
Statistical analysis
Data are reported as the median (± IQR). Differences between groups were assessed by the Mann-Whitney test with a P significance limit < 0.05. The statistical analyses were all performed using SPSS software (version 17.0). The trial was stopped after enrolling 45 patients (21 in the ketamine group and 24 in the fentanyl group) due to time expiration, despite the initial plan of 90 patients to be included in the analysis. The lack of evidence quantitatively estimating a superior benefit of ketamine over fentanyl did not allow an accurate sample size calculation to be performed.
RESULTS
The main clinical charts are presented in Table 1. Overall ICU mortality of patients was high (65%) in a population with a high predicted mortality (mean SAPS 3 – Simplified Acute Physiology Score 3, score of 68 points). Ketamine was not associated with greater reduction in Rsmax compared to fentanyl, either after 3 h (0 ± 6 vs. −3 ± 7.7, respectively; P = 0.16) or after 24 h (−3 ± 17 vs. −3.5 ± 13.7, respectively; P = 0.73) (Figure 1). Delta Rsmax at 3 h was 0 cm H2O L−1 s−1 (CI 95%: −3.5 to 2.5) in the ketamine and −3 cm H2O L−1 s−1 (CI 95%: −12 to 1.7) in the fentanyl group (P = 0.16). At 24 h, delta Rsmax was −3 cm H2O L−1 s−1 (CI 95%: −15.5 to 1.5) in the ketamine and −3.5 cm H2O L−1 s−1 (CI 95%: −12 to 1.7) in the fentanyl group (P = 0.73). Patients randomised to the ketamine group did not have better improvements in delta PEEPi as compared with fentanyl at 3 h: 0 cm H2O (CI 95%: −1 to 1.5) vs. −0.5 cm H2O (CI 95%: −7.7 to 0), P = 0.77, respectively. Also, at 24 h there was no difference between treatments in delta PEEPi: −1 cm H2O (CI 95%: −3 to 1) in ketamine and −0.5 cm H2O (CI 95%: −4.7 to 1.7) in fentanyl group (P = 0.72). There was no difference between groups in delta Cdyn at 3 h: ketamine 0 mL cm H2O−1 (CI 95%: −2 to 2) and fentanyl 0 mL cm H2O−1 (CI 95%: −2 to 3), P = 0.85; as well as at 24 h: ketamine 1 mL cm H2O−1 (CI 95%: −6.5 to 3.5) and fentanyl 0.5 mL cm H2O−1 (CI 95%: −11.2 to 3.2), P = 0.35. In an exploratory subgroup analysis, asthma patients using ketamine had no difference in 3 h-delta Rsmax (P = 0.07). The subgroup of patients with COPD also showed no differences between groups in 3h-delta Rsmax (P = 0.19). Patients randomised to the ketamine group had a median of 7 (± 10) days, compared with 8.5 (± 9.7) days in the fentanyl group (P = 0.55). Patients in the ketamine group required a higher cumulative dose of fenoterol within 24 h of randomization compared to those receiving fentanyl (P = 0.04). Patients in the ketamine group did not receive a greater cumulative dose of midazolam in 24 h (P = 0.06) and 72 h (P = 0.57) compared to fentanyl but received a greater cumulative dose in 48 h (P = 0.01). Baseline, 3 h and 24 h heart rates were not different between groups; nor was median noradrenaline dose at the same time points.
TABLE 1.
Baseline clinical variables
| Variable | Ketamine (n = 21) | Fentanyl (n = 24) |
|---|---|---|
| Age (years) | 60 (±17) | 65 (±14) |
| Male sex (n) | 10 | 13 |
| COPD (n) | 16 | 18 |
| Class IV COPD (n) | 8 | 7 |
| Asthma (n) | 7 | 6 |
| Active tobaccoism (n) | 16 | 11 |
| Chronic heart failure (n) | 2 | 3 |
| Cirrhosis (n) | 0 | 2 |
| Tuberculosis (n) | 2 | 0 |
| Acute pulmonary embolism (n) | 1 | 0 |
| Solid neoplasm (n) | 1 | 3 |
| Chronic kidney disease (n) | 0 | 1 |
| HIV infection (n) | 1 | 1 |
| Ambulatorial oxygen therapy (n) | 1 | 3 |
| Ambulatorial corticosteroid use (n) | 11 | 13 |
| SAPS 3 score (points) | 68 (± 13) | 71 (± 19) |
| Inhaled β-2 agonist dose, 24 h pre-randomisation (μg) | 800 (± 1200) | 1200 (± 1400) |
| IV salbutamol 24 h pre-randomisation (n) | 10 | 9 |
| IV salbutamol 24 h pre-randomisation (n) | 22 (8.25) | 24 (10.5) |
| Rsmax pre-randomization (cm H2O L−1 s−1) | 23 (14.5) | 21 (11) |
| Rsmax 3 h (cm HO L−1 s−1) | 18.5 (14.25) | 20.2 (8.5) |
| Rsmax 24 h (cm H2O L−1 s−1) | 5.5 (7.25) | 5 (6) |
| PEEPi pre-randomisation (cm H2O) | 7 (8) | 5 (7.5) |
| PEEPi 3 h (cm H2O) | 5 (4.75) | 6 (6.5) |
| PEEPi 24 h (cm H2O) | 17 (10.75) | 16 (9) |
| Cdyn pre-randomisation (mL cm H2O−1) | 16 (7.75) | 16 (7) |
| Cdyn 3 h (mL cm H2O−1) | 17 (10.5) | 16 (7) |
| Cdyn 24 h (mL cm H2O−1) | 17 (10.5) | 16 (7) |
DISCUSSION
In this study, ketamine administration did not reduce inspiratory airway resistance or PEEPi, a surrogate of dynamic hyperinflation. Patients with COPD have an elevation in inspiratory Rsmax secondary to bronchospasm, airway inflammation and mucous production, whereas PEEPi signals obstruction to the expiratory flow present in patients with asthma or exacerbation of COPD. Ketamine was ineffective in improving respiratory mechanics in this scenario compared to fentanyl, and was not associated with a reduction in the number of days on mechanical ventilation, nor was it associated with lower mortality.
Few data support the use of ketamine in the management of acute bronchospasm, basically in the treatment of asthmatic conditions [5], in very heterogeneous populations and with the measurement of very different variables, mostly in retrospective studies [10]. In emergency department patients with acute asthma exacerbation, ketamine did not increase the bronchodilatory effect compared with standard therapy [7]. Our study included a more severe population, admitted to the ICU and submitted to IMV.
This study has the merit of prospectively evaluating a therapy sometimes used in the management of acute bronchospasm but with scarce evidence supporting its use. However, it has several limitations. First, it failed to reach the initially proposed number of randomised patients, because of a low inclusion rate. Second, adherence to the protocol was complete only for the first 24 h after inclusion, and it was at the discretion of the attending team whether to maintain therapy afterwards. Third, the high mortality rate of the patients studied may limit the extrapolation of these data to other clinical scenarios. Fourth, the joint analysis of patients with bronchospasm, with asthma or COPD does not allow a robust analysis of each subgroup of diseases, due to the low sample size. However, management of acute bronchospasm in patients submitted to IMV is broadly similar in both, despite different mechanisms of disease [11, 12]. The pharmacological treatment is quite similar, justifying the analysis of ketamine in this clinical setting. Fifth, we cannot estimate how many of the patients included had asthma–COPD overlap, a condition associated with defined characteristics of COPD as well as features of asthma, generally associated with a worse prognosis [12].
Until new evidence suggests otherwise, however, at least in this clinical setting, ketamine has not been shown to be more effective in the management of acute bronchospasm compared with standard fentanyl-based analgesia.
CONCLUSIONS
Intravenous ketamine infusion is not associated with higher resolution of bronchospasm compared with standard continuous IV analgesia in patients undergoing fentanyl-based invasive mechanical ventilation.
ACKNOWLEDGEMENTS
Financial support and sponsorship
none.
Conflicts of interest
none.
REFERENCES
- 1.Rowe BH, Sevcik W, Villa-Roel C.. Management of severe acute asthma in the emergency department. Curr Opin Crit Care 2011; 17: 335-341. doi: 10.1097/MCC.0b013e328348bf09. [DOI] [PubMed] [Google Scholar]
- 2.Brown H, Dodic S, Goh SS, et al. . Factors associated with hospital mortality in critically ill patients with exacerbation of COPD. Int J Chron Obstruct Pulmon Dis 2018; 13: 2361-2366. doi: 10.2147/COPD.S168983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Vicente EG, Sandoval Almengor JC, Díaz Caballero LA, Salgado Campo JC.. Invasive mechanical ventilation in COPD and asthma. Med Intensiva 2011; 35: 288-298. doi: 10.1016/j.medin.2010.11.004. [DOI] [PubMed] [Google Scholar]
- 4.Lindenauer PK, Stefan MS, Shieh MS, Pekow PS, Rothberg MB, Hill NS.. Outcomes associated with invasive and noninvasive ventilation among patients hospitalized with exacerbations of chronic obstructive pulmonary disease. JAMA Intern Med 2014; 174: 1982-1993. doi: 10.1001/jamainternmed.2014.5430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Goyal S, Agrawal A.. Ketamine in status asthmaticus: a review. Indian J Crit Care Med 2013; 17: 154-161. doi: 10.4103/0972-5229.117048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Aroni F, Iacovidou N, Dontas I, Pourzitaki Ch, Xanthos T.. Pharmacological aspects and potential new clinical applications of ketamine: reevaluation of an old drug. J Clin Pharmacol 2009; 49: 957-964. doi: 10.1177/0091270009337941. [DOI] [PubMed] [Google Scholar]
- 7.Howton JC, Rose J, Duffy S, Zoltanski T, Levitt MA.. Randomized, double-blind, placebo-controlled trial of intravenous ketamine in acute asthma. Ann Emerg Med 1996; 27: 170-175. doi: 10.1016/S0196-0644(96)70319-0. [DOI] [PubMed] [Google Scholar]
- 8.Hemming A, MacKenzie I, Finfer S.. Response to ketamine in status asthmaticus resistant to maximal medical treatment. Thorax 1994; 49: 90-91. doi: 10.1136/thx.49.1.90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Iotti GA, Braschi A.. Measurements of Respiratory Mechanics During Machanical Ventilation. Hamilton Medical Scientific Library, Rhazuns: 1999. [Google Scholar]
- 10.Miller AC, Jamin CT, Elamin EM.. Continuous intravenous infusion of ketamine for maintenance sedation. Minerva Anestesiol 2011; 77: 812-820. [PubMed] [Google Scholar]
- 11.Gibson PG, McDonald VM.. Asthma-COPD overlap 2015: now we are six. Thorax 2015; 70: 683-691. doi: 10.1136/thoraxjnl-2014-206740. [DOI] [PubMed] [Google Scholar]
- 12.Buist AS. Similarities and differences between asthma and chronic obstructive pulmonary disease: treatment and early outcomes. Eur Respir J 2003; 21: 30s-35s. doi: 10.1183/09031936.03.00404903. [DOI] [PubMed] [Google Scholar]