

Abstract
Left ventricular assist devices (LVADs) are increasingly used to treat patients with end-stage heart failure. Implantable LVADs were initially developed in the 1960s and 1970s. Because of technological constraints, early LVADs had limited durability (eg, membrane or valve failure) and poor biocompatibility (eg, driveline infections and high rates of hemolysis caused by high shear rates). As the technology has improved over the past 50 years, contemporary rotary LVADs have become smaller, more durable, and less likely to result in infection. A better understanding of hemodynamics and end-organ perfusion also has driven research into the enhanced functionality of rotary LVADs. This paper reviews from a historical perspective some of the most influential axial-flow rotary blood pumps to date, from benchtop conception to clinical implementation. The history of mechanical circulatory support devices includes improvements related to the mechanical, anatomical, and physiologic aspects of these devices. In addition, areas for further improvement are discussed, as are important future directions—such as the development of miniature and partial-support LVADs, which are less invasive because of their compact size. The ongoing development and optimization of these pumps may increase long-term LVAD use and promote early intervention in the treatment of patients with heart failure.
Keywords: Ventricular dysfunction, left; heart failure; heart-assist devices; assisted circulation
Introduction
Cardiovascular disease is the leading cause of death globally, representing 32% of all deaths worldwide.1 Heart failure (HF)—broadly defined as impairment of the heart's pumping function2—accounts for approximately 10% of the deaths attributable to cardiovascular disease.3 Each year, there are approximately 400,000 HF-related deaths in the United States, with 1.9 million such deaths worldwide.3–5
Heart failure affects approximately 6 million people in the United States, and this number is expected to increase to 8 million by 2030.3 Heart failure can present with a multitude of symptoms, primarily shortness of breath and fatigue. Patients with HF may also exhibit functional deterioration, such as a reduced stroke volume with decreased cardiac output. The decrease in cardiac output can be caused by a reduction in cardiac ejection (systolic dysfunction) or a reduction in ventricular filling (diastolic dysfunction). The New York Heart Association (NYHA) has outlined 4 levels of subjective (patient-reported) symptoms and 4 levels of objective criteria for classifying HF according to severity.6 Patient symptoms range from none (no limitation on activities) to HF symptoms at rest (inability to carry on any physical activity without discomfort). Similarly, objective criteria range from none (no symptoms and no limitations on activities) to evidence of severe cardiovascular disease (symptoms at rest, severely limited activity).6 Traditionally, HF is treated first with medication, and then, if necessary, with mechanical circulatory support (MCS).
Modern implantable MCS devices can be categorized as either a total artificial heart or a ventricular assist device (VAD). A total artificial heart replaces the native ventricles and takes over cardiac function,7 whereas a VAD assists 1 or both ventricles and relieves the sequelae of HF by improving organ perfusion and reducing pulmonary congestion.8 A VAD's pumping mechanism can be either positive displacement or, more commonly, rotary propulsion; rotary pumps can be further classified according to whether the flow path is centrifugal or axial and according to the device's physiologic interface with the heart, such as whether the pump acts in parallel with the heart or in series. Typically, centrifugal-flow pumps are large (which complicates achieving anatomical fit) and operate at low speeds. Conversely, axial-flow pumps are smaller and have higher operating speeds. Although axial pumps generally fit easily, ensuring hemocompatibility is difficult.
Here, the authors discuss the mechanical, anatomical, and physiologic aspects of the axial-flow rotary blood pump and its contributions to the history of MCS devices.
Historical Overview
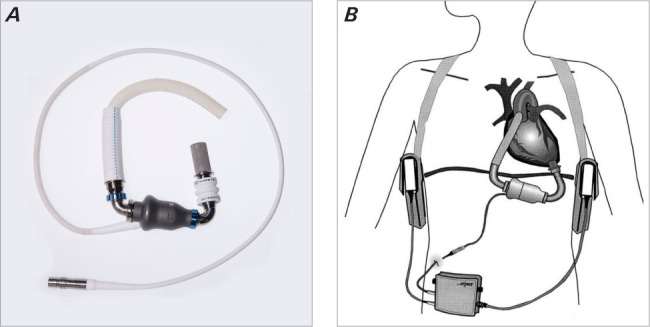
Implantable left VADs (LVADs) were developed in the 1960s and 1970s as an extension of the work of Dr Michael DeBakey, Dr Domingo Liotta, and others.9,10 Between 1976 and 1979, 22 intra-abdominal LVADs were implanted at The Texas Heart Institute in Houston, and 1 of the recipients became the first person to be bridged to transplant with an LVAD.11 Because the first era of heart transplantation (1967–1971) had largely met with failure, by 1989 the US National Institutes of Health was directing funding (eventually totaling more than $266 million) primarily toward the development of pulsatile mechanical LVADs, and the companies contracted to develop these LVADs spent at least that much.12 Laboratory work done at The Texas Heart Institute in collaboration with the engineering experts at Thermo Cardiosystems Inc resulted in the development of the pneumatic HeartMate pulsatile LVAD (Thoratec Corporation) (Fig. 1A).13,14 Around the same time, a group at Stanford University led by Peer Portner and Norman Shumway developed the Novacor electrical circulatory assist device (Baxter Healthcare Corp) (Fig. 1B).15–17 Each of these pulsatile output pumps used a compressible blood chamber with inlet and outlet valves to achieve forward flow. These devices confirmed that timely MCS could rescue patients facing imminent death from end-stage HF.
Fig. 1.

Photographs show early pulsatile circulatory assist devices: A) pneumatic HeartMate; B) Novacor. Reproduced from Farkas et al. Expert Review of Medical Devices. 4(6), 769–774. Reprinted with permission from Expert Review of Medical Devices (Copyright ©2007). Taylor & Francis Ltd. All Rights Reserved.17
Fig. 1.

Photographs show early pulsatile circulatory assist devices: A) pneumatic HeartMate; B) Novacor. Reproduced from Farkas et al. Expert Review of Medical Devices. 4(6), 769–774. Reprinted with permission from Expert Review of Medical Devices (Copyright ©2007). Taylor & Francis Ltd. All Rights Reserved.17
In 1994, the pneumatic HeartMate LVAD became the first implantable pump approved by the US Food and Drug Administration (FDA). In 1998, the Novacor LVAD and an electromechanical version of the Heart-Mate device (the XVE) were FDA approved for long-term implantation in patients with HF.18,19 However, because these early LVADs were large, their clinical application was limited by patient body size and contour. The devices also had limited durability, usually because of membrane wear, which typically resulted in device failure after 24 to 36 months.20 As a result, the only meaningful clinical use for these LVADs in patients with HF was as a bridge to transplant. Even so, heart transplant was limited from the outset by donor availability and by the likelihood of late death, primarily from chronic rejection.
In the late 1970s and early 1980s, Dr O.H. Frazier used the Biomedicus centrifugal rotary pump (Medtronic) to support circulation in patients who required extracorporeal membrane oxygenation or temporary LVAD support. In 1987, this pump was implanted in a 9-year-old child—the first pediatric patient to be bridged to transplant. During that era, advocates and skeptics alike engaged in numerous debates centered around the various issues posted by implantable continuous-flow rotary pump technology, such as physiologic aberration of the baroreceptor response, disruption of the juxtaglomerular response, having a nonlubricated bearing in the bloodstream, and blood damage from high speeds in the axial-flow pump.
In the 1980s, in an effort to create a smaller, more durable pump, laboratory researchers at The Texas Heart Institute collaborated with Drs Richard Wampler and Robert Jarvik to show the utility of 2 continuous-flow rotary LVADs: the Hemopump21 (Nimbus Medical, Inc) (Fig. 2A) and the Jarvik 2000 FlowMaker22 (Jarvik Heart Inc) (Fig. 2B), respectively. Each of these devices worked at a high rotational speed and used a nonlubricated, blood-washed bearing in its axial-flow mechanism. The first successful clinical implementations of these technologies (the Hemopump in 1988 and the Jarvik 2000 2 years later) were foundational for the development of subsequent continuous-flow LVADs.23,24
Fig. 2.

Photograph shows early continuous-flow rotary circulatory assist devices. A) Hemopump; B) Jarvik 2000.
The HeartMate II (Thoratec Corporation) (Fig. 3),25 a descendant of the Hemopump, was first successfully implanted in a patient in November 2003.26 Since then, the HeartMate II has been implanted in more patients than any other LVAD to date, with approximately 30,000 implanted in patients with HF worldwide; the longest a patient has lived with a HeartMate II is more than 15 years.12 Overall, more than 50,000 patients around the globe have been treated with long-term, continuous-flow, blood pump support.12
Fig. 3.
A) Photograph shows the HeartMate II device. B) Illustration shows the HeartMate II implant location with external batteries and controller. Reproduced from Butler et al. Annals of Thoracic Surgery. 68(2), 790–794. Reprinted with permission from Annals of Thoracic Surgery (Copyright ©1999). Elsevier. All Rights Reserved.25
The field of MCS has continued to expand over the past 15 years, with the introduction of the centrifugal-flow HeartWare (HeartWare International Inc/Medtronic), HeartMate III (Thoratec Corporation), EVAHEART (EvaHeart, Inc), and VentrAssist (Ventracor Ltd) LVADs (all of which have noncontact bearings).27–29 Progress in this field has been characterized by the improved durability of rotary blood pumps, reduction in pump size (along with a concomitant reduction in implantation morbidity), and earlier implementation.30 In the future, further reducing the pump size may allow long-term device implantation in the catheterization lab, which has the potential to further accelerate expansion of the field.
The following sections review the various mechanical, anatomical, and physiologic aspects of the major implantable axial-flow rotary blood pumps developed in the past 40 years.
Hemopump
Invented by Dr Wampler in 1975, the Hemopump (Fig. 2A) was designed and produced by Nimbus starting in 1983. Nimbus was acquired by Johnson & Johnson Interventional Systems in 1991, and then by Medtronic in 1995.31 The Hemopump was a miniature (7 mm in diameter × 20 cm in length), cable-driven, axial-flow rotary pump with an external motor.32 This device was capable of capturing up to 80% of cardiac function in short-term applications, such as during minimally invasive coronary bypass surgery and in patients with acute myocardial infarction (MI), postcardiotomy left ventricular (LV) failure, or cardiogenic shock.21,32,33 At rotational speeds of 17,000 to 26,000 rpm, the Hemopump could pump 3 to 4 L/minute.33 Approximately 300 mL of 40% dextrose purge fluid was needed per day to wash out the seal and to lubricate the drive cable and hydrodynamic bearing.31,32
The Hemopump could be inserted through the femoral artery and positioned in a transvalvular orientation with the inflow in the left ventricle and the outflow in the aorta, just distal to the left subclavian artery.32 However, this insertion path was problematic in patients with peripheral vascular disease, aortic aneurysm, or aortic valve stenosis. Although the aortic valve functions normally in most patients,34 the Hemopump was contraindicated in patients with an aortic valve replacement.35,36 Thrombus in the left ventricle also interfered with pump operation.37
Before 1988, when the FDA approved clinical studies of the Hemopump in patients with terminal cardiogenic shock, the device was tested in more than 80 calves in both long-term and short-term studies.21 In a 24-calf study (3 controls, 21 implanted with a Hemopump), plasma-free hemoglobin levels and platelet counts were found to be within the acceptable range.21 Hemodynamics were studied by turning the pump off and on while monitoring pressures during normal heart function and ventricular fibrillation. When the pump was on during normal heart function, LV pressure dropped and aortic pulsatility decreased. During induced fibrillation, the Hemopump maintained aortic pressure for 45 minutes.21 All organ function was normal after the 2-week study period concluded.
In 1988 and 1989, a pilot study of the Hemopump was performed in 20 patients; it was used effectively in 12 of them.33 The device was most often implanted under fluoroscopic guidance, with access into the femoral artery through an anastomosed Dacron graft.38 In other cases, a cannula implantation approach was used to place the pump directly through the ascending aorta.38 Of the 12 patients in this study, 10 (9 adults, 1 child) were successfully weaned from the pump, and 3 of these patients returned to normal daily activities. Ultimately, the Hemopump was implanted in more than 200 people across multiple centers.
As common practices were developed for the Hemopump, clinicians found that the most successful approach was to initially run the pump at maximum speed to unload the heart as quickly as possible, and then to wean the patient off the pump by reducing the speed as the heart recovered.35 Patient hemodynamics improved after Hemopump implementation, indicating the reversal of cardiac shock.32,34 Although driveline fracture was common (60%) in early clinical trials, a subsequent design modification reduced stress concentration points and lowered the incidence of driveline fracture.34 Other documented risks included supravalvular dislodgement and inflow cannula obstruction; generally, these complications could be detected and addressed at the bedside.35 Because the Hemopump (like all rotary blood pumps) is afterload dependent,39,40 care had to be taken to maintain adequate pressure to ensure renal perfusion without increasing pressures to the point of impeding pump flow.41
The Hemopump set a precedent for all axial-flow pumps (both short term and long term) developed since its initial clinical use in April 1988.37
Jarvik 2000
The Jarvik 2000 (Fig. 2B) is an axial-flow intraventricular pump with a length of 55 mm, a diameter of 25 mm, a weight of 85 g,37 and a flow of 3 to 7 L/minute at speeds of 8,000 to 12,000 rpm.42 From 1985 to 1991, preclinical studies at The Texas Heart Institute were conducted in 37 calves implanted with the Jarvik 2000, with chronic studies averaging 70 days. Hemolysis levels were elevated from baseline values only slightly with the administration of heparin and warfarin. Neurologic, renal, hepatic, and pulmonary functions were normal.22
In the late 1990s, clinical trials of the Jarvik 2000 were initiated in 1 man at Oxford in the United Kingdom and 1 woman and 2 men at The Texas Heart Institute in the United States. The average length of support was 65 days. During that time, the cardiac index in these patients improved by an average of almost 2.5 times that of the preimplant value, and the size of the heart decreased, as shown by echocardiographic data.22,24,37
By 2002, 37 patients had undergone implantation of the Jarvik 2000 in the United States and Europe. At 1 year, the survival rate was 57%. Twelve of those patients underwent a heart transplant, and 4 had continually functioning devices 2 years after implantation.37 Several patients survived for as long as 7.5 years with a Jarvik 2000.43,44 Although the Jarvik 2000 has not been approved by the FDA for use in the United States, it is popular in Japan because of its small size.45
HeartMate II
The HeartMate II (Fig. 3)25 is a refinement of the axial-flow technology first introduced with the Hemopump. The HeartMate technology was initiated by Dr Wampler, Dr John Moise, and Dr Ken Butler, who worked with Nimbus to address the need for long-term implantable cardiac support.
The HeartMate II is 4.0 cm in diameter, 7.0 cm long, and weighs 782 g.25 It has jewel bearings and percutaneous leads that connect it to its external power source.25,46,47 This pump is designed with a best efficiency point of 6.0 L/minute against 100 mm Hg at 11,000 rpm.48 The blood tube is surrounded by a motor stator, and the rotor contains a 2-pole magnet.49 When flow through the pump was examined using computational and experimental methods, the rotor was well washed, but some recirculation was observed on the convex side of the stator and between the rotor and stator. In addition, low flow near the pump shutoff was problematic because it created longer blood residence times resulting from greater circumferential flow than axial flow as well as large recirculation zones.47
Preliminary studies of the HeartMate II were performed in 6 calves. Studies in 2 of the 6 calves were concluded electively, whereas studies in the other 4 calves were concluded because of pump malfunction caused by high power usage and low flow rate.50 These preclinical studies were eventually expanded to include more than 40 calves47 before clinical studies began in Israel in July 2000.42,46 Unfortunately, poor clinical outcomes in patients who underwent HeartMate II implantations in Europe resulted in temporary cessation of the clinical program. This poor result was believed to be related to the sintered titanium placed on the interior surface of the HeartMate II pump. This, combined with the negative pressure required to generate meaningful flow in patients, was speculated to be the cause of early pump thrombosis and failure. In 2003, after removal of the sintered titanium surface, the first clinical implantation of the HeartMate II pump was performed in the United States. The patient had the device for 2.5 years of uncomplicated support before undergoing a heart transplant.26 The most common adverse events in the clinical studies that followed were bleeding and driveline infection.51 A study conducted at Texas Children's Hospital from 2008 through 2011 showed that patient outcomes in a pediatric population (11- to 18-year-olds) were similar to those in adult patients.52
Because the HeartMate II was the first long-term implantable rotary LVAD, much was learned about the clinical management of HF in patients with these pumps. For example, because this device is free of the valves that earlier pulsatile pumps required, pump speed must be maintained at sufficient levels to avoid retrograde flow through the pump. In addition, because of the continuous draw of negative pressure at the pump inlet, obstruction can result from a malalignment of the inlet conduit.47
Impella
The Impella (ABIOMED) (Fig. 4) device is a micro-axial pump developed at the Helmholtz Institute in Aachen, Germany. It has a diameter of 6.4 mm and a length of 60 mm. During the design process, the goal was to achieve a pump speed of 3.0 L/minute at 80 to 100 mm Hg,53 although at 32,500 rpm, the 2-blade impeller can pump 4.5 L/minute against physiologic pressures.54 The impeller is positioned in the pump housing with a 0.1-mm blade tip clearance.55
Fig. 4.

Photograph shows the Impella CP (left) and Impella 5.0 (right) devices.
In the 1990s, 3 different visualization methods were used to examine flow path in the Impella pump: particle image velocimetry (PIV), oil streaking, and flow threads. The focus of PIV was to identify stagnation regions and to visualize flow in the channel between the vanes. Oil streaking was used to qualitatively examine surface shear stresses by using a water-insoluble dye that streaks under shear forces; with this technique, dye deposits indicate stagnation regions. To examine the flow even closer to the surface than the oil dots, short silk fibers (flow threads) were glued to the hub, and their orientation was photographed during pump operation. The PIV results revealed a mismatch between flow direction and stator incidence angle.56
Computational fluid dynamics studies were conducted in an attempt to predict hemolysis by assessing the shear rates and exposure time of erythrocytes to these shear rates. In the blade tip gap, shear rates could reach as high as 1,000 Pa, but only 3.6% of the fluid was exposed to that region, whereas more than 75% of the fluid was exposed to shear rates lower than 25 Pa.54 This computational fluid dynamics study was validated with PIV data.57
Early clinical experience showed that the Impella could be used as an alternative to a heart-lung machine,55 with the most significant clinical benefit over a heart-lung machine being the drastically reduced need for blood products.58 The Impella line of pumps was therefore expanded to include other variations: the Impella 2.5, used in normothermic percutaneous coronary interventions59; the Impella 5.0, used for placement in the left ventricle via the femoral artery; the Impella LD, used for placement in the left ventricle via the aortic arch; and the Impella RP, used as a right VAD.60 Notably, the Impella has been shown to reduce infarct size after MI.61
Before clinical implementation of the Impella, other designs and manufacturing processes were considered. In 1 design, 3 impeller blades and 3 stator vanes were attempted.53 In another, the motor was magnetically coupled to the impeller with a pivot bearing at each end of the impeller. However, the magnetic coupling could not support the necessary torque and the pivot bearings were inadequate to prevent vibration above 15,000 rpm.53 Over time, the manufacturing process was refined to reduce blood trauma. Switching from machined and hand-polished surfaces to injection-molded and machine-polished surfaces improved the modified index of hemolysis from a range of 3 to 39 to consistently less than 10.62 In addition, pressure sensors were added to the inflow and outflow of the pump to facilitate positioning and to assess preload and afterload.55
HeartAssist 5
The HeartAssist 5 (ReliantHeart, Inc) (Fig. 5) was developed under the direction of Dr DeBakey and MicroMed Technology Inc as part of a collaboration between the Johnson Space Center and Baylor College of Medicine.37 The HeartAssist 5 consists of an inflow cannula, a stator fixed to the pump housing, a flow straightener, an impeller, and a diffuser.63 The front-end flow straightener acts as a mechanical pivot bearing, and the stationary diffuser downstream of the impeller contains a rear mechanical pivot bearing.37 Rare-earth magnets are embedded in the impeller blades as part of the motor driving the impeller.37,64 This pump, with a length of 75 mm and a diameter of 25 mm, uses 10 W of power to maintain a rotational speed of 10,000 rpm and produces 5 to 6 L/minute of flow against a pressure head of 100 mm Hg.37,65 The pump is capable of rotating as fast as 12,500 rpm to produce up to 10 L/minute of flow.65–68 To reduce the risk of thrombosis, the internal blood-contacting surfaces of the device are coated with CARMEDA BioActive Surface (W. L. Gore & Associates, Inc).69
Fig. 5.

Photograph shows a cross-section of the HeartAssist 5 device.
Chronic in vivo studies of the HeartAssist 5 in calves showed that 90 days after implantation, the index of hemolysis remained at less than 0.0002 g per 100 L blood,65 which is well below the accepted limit. Moreover, kidney and liver function was normal under both resting and exercise conditions in vivo, and no evidence of thrombus formation was reported.37,65 In 2000, a multicenter clinical study of the FDA-approved HeartAssist 5 was initiated.66–68 By September of that year, Baylor College of Medicine reported that 51 adult patients had received the HeartAssist 5 as a bridge to transplant.37 Before 2002, this device had been tested in 14 heart centers in 7 countries, with average flow rates of 3.6 to 5.0 L/minute.37,69 More recently, ReliantHeart reconfigured the HeartAssist 5 to eliminate the inflow cannula; this new version is called the aVAD.
Miniaturized VADs
The HeartWare Miniaturized Ventricular Assist Device system70 (HeartWare International, Inc) had a displacement volume of 15 mL and could generate flows of 1 to 8 L/minutes at operating speeds of 12,000 to 20,000 rpm.71,72 The impeller was suspended magnetically, with hydrodynamic thrust bearings on the circumferential surface of the impeller blades to provide radial stiffness. In 1 version of this device, the pump was inserted apically, with an outflow graft radially exiting the body of the pump for anastomosis to the aorta.73 In another version, a pedestal was anchored to the ventricular wall so that the pump itself was situated within the LV chamber on a standoff pipe. Blood was then drawn into the pump in the ventricle with an adjustable-length outflow cannula (14.5–15.5 cm) placed across the aortic valve to eject blood into the aorta. This pedestal and standpipe–mounted device was later known as the HeartWare Longhorn, although it was hydraulically the same as the miniaturized VAD.74 The Longhorn device was tested in a study of 10 calves in Louisville, Kentucky, and exhibited hemodynamic efficacy and low blood trauma. The calves were thrombus free for up to 30 days during the operative and postoperative periods.71
Synergy
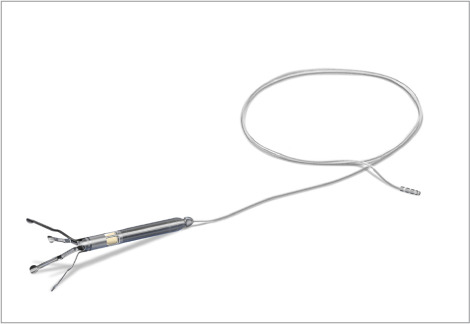
The Synergy circulatory assist device (CircuLite Inc) (Fig. 6) was developed at the Helmholtz Institute in Aachen, Germany, in the mid-1990s.75 CircuLite Inc was purchased by HeartWare International 3 years before HeartWare was purchased by Medtronic.70,76 With a diameter of 14 mm, a length of 49 mm, and a weight of 25 g, the Synergy device pumps 1.9 to 2.9 L/minute in vivo at an operating speed of 20,000 to 24,000 rpm.77
Fig. 6.

Photograph shows the Synergy system with inflow cannula and outflow graft.
Its inflow is positioned in the left atrium, and the outflow is connected to the subclavian artery. The pump itself sits subcutaneously in the pectoral region, similar to a pacemaker.78 The inflow is a 20.5-cm-long cannula made of nitinol-reinforced silicone, with an inner diameter of 6 mm; the outflow is a 15-cm-long graft made of 1-mm-thick expanded polytetrafluoroethylene, with an inner diameter of 8 mm.79 The length of the graft can be adjusted to suit the patient's anatomy. The driveline is 100 cm long and has a 16-cm veneer in the region crossing the skin barrier to prevent infection.78
In clinical trials, 7 of the first 10 patients had pump thrombosis severe enough to warrant a pump exchange within 2 months of implantation. In each of these cases, the inflow cannula was left in place while the pump and outflow graft were replaced.78 Additional studies showed that older patients (≥70 years of age) tolerated the pump well and perhaps had better recovery from the less-invasive surgery than they would from the thoracotomy required to implant a full-flow VAD.80 The Synergy pump was ultimately implanted in more than 100 patients but is no longer used.81
Berlin Heart Incor
The Incor (Berlin Heart AG) was a magnetically levitated axial-flow LVAD whose first clinical use was described in 2004.82 It weighed approximately 200 g and had a 30-mm diameter. It operated at 5,000 to 10,000 rpm to produce flows of up to 7 L/minute against a pressure rise of 150 mm Hg.83 The Incor was placed with an inlet cannula positioned in the LV apex and the outlet cannula anastomosed to the aorta. The most revolutionary feature of the Incor was its axial magnetic levitation system, which enabled contact-free rotation of the impeller to eliminate wear points and reduce blood trauma.84
Procyrion Aortix
The Aortix pump (Procyrion, Inc) (Fig. 7) is a catheter-based, intra-aortic, partial-support LVAD. To function in series with the left ventricle, it is inserted percutaneously via the femoral artery for deployment in the descending aorta and is affixed to the walls of the aorta with nitinol struts. In a mock circulatory loop, the Aortix pump was shown to decrease LV work by 15%; in a sheep model, the pump increased cardiac output from 3.5 L/minute to 4.6 L/minute.85 The Aortix pump head and motor mimic those of the Impella 5.0. In acute studies at The Texas Heart Institute, hemodynamic status during pump operation was studied in 3 pigs with pharmacologically induced HF. In 2013, the performance of the Aortix pump was reported to be similar to that of an intra-aortic balloon pump.86 Since then, clinical trials have commenced both within and outside the United States. In 2021, Procyrion announced successful treatment of the first patients with cardiorenal syndrome enrolled in the company's first-in-humans pilot trial evaluating the performance of the Aortix device.87
Fig. 7.
Photograph shows a prototype of the Aortix device.
Observations of the Past as Considerations for the Future
In the 1980s, when rotary blood pumps were first receiving serious attention from researchers, many clinicians criticized continuous-flow devices because of the altered physiology induced by their use—an issue that has yet to be satisfactorily addressed in systematic studies. Primary concerns include the effects of rotary blood pumps on the baroreceptor response, physiologic blood pressure, the juxtaglomerular apparatus, and right heart function.88 In the mid-2000s, a major clinical risk associated with continuous flow was a markedly increased incidence of hemorrhagic stroke, particularly in patients with the HeartMate II.51 This risk was believed to be related to the continuous positive pressure and flow throughout the cardiac cycle. The conversion of the normal passive diastolic flow to constant positive pressure flow was considered an important facet of this devastating complication and was addressed by aggressive pharmacologic lowering of blood pressure. In addition, aortic valve opening time typically is reduced or altogether absent in patients with continuous-flow pumps, making the measurement of blood pressure impossible with commonly used pneumatic pressure cuffs. Instead, blood pressure must be measured with a Doppler apparatus after the arterial line is removed. Atypical gastrointestinal bleeding, primarily from arteriovenous malformations in the small intestine, also has been documented in patients with a rotary blood pump.89 This response to decreased pulsatility was first documented by Dr E.C. Heyde in 1958 in patients with severe advanced aortic stenosis.90 The narrowing of the normal pulse pressure induced by constant-pressure pump flow is believed to play a similar role in this complication. Therefore, despite the clinical and engineering successes that have produced today's rotary blood pumps, challenges related to the anatomical interface and physiologic consequences of this promising technology remain to be addressed.12
Even though several LVAD designs are available for clinical use, none is perfect. This article has provided an in-depth review of many axial-flow LVADs, whose primary advantage over centrifugal pumps is size: Axial pumps have the potential to be implemented in a smaller form, which may advance both the minimally invasive LVAD field and the pediatric LVAD field. Nonetheless, whether the optimal LVAD of the future will be axial or centrifugal is yet to be determined.
In the future, reducing pump size may improve the anatomical fit of the device, but this approach often increases blood trauma because smaller pumps typically have small high-shear stress gaps.54 Given that LVAD implantation typically requires an invasive surgical procedure and increases the risk of adverse events, physicians often decide against earlier implantation (Interagency Registry for Mechanically Assisted Circulatory Support) levels 4 through 6 or NYHA class IIIb),79 choosing instead to manage the patient's condition with pharmacotherapy until MCS or heart transplant becomes inevitable.
Another area of focus besides size reduction is improved biocompatibility, both with the blood and with the tissue around the device. Relevant to hemocompatibility, rotary pumps induce hyperphysiologic shear stresses that can cause hemolysis and damage to other blood components, particularly von Willebrand factor. It is believed that the mechanical cleaving of von Willebrand factor by high shear stress leads to diminished clotting ability and the potential for bleeding.91 As for tissue compatibility, the driveline poses particular risk for infection. Research is being pursued to power the pump wirelessly through a transcutaneous energy transmission system. The first of these systems was tested in humans in 2019.92
Although HF is a disease of unknown etiology, strong evidence supports the notion that unloading the left ventricle, either by bed rest93–95 or by MCS,96–98 allows for myocardial reconditioning in some patients. Restoring the Frank-Starling response and maintaining pulsatility are both significant benefits to early LV unloading that can mitigate cardiac deterioration and improve patient quality of life. Therefore, intermittent flow devices that allow the aortic valve to briefly function more normally may be beneficial to many of these patients.
With the advances in minimally invasive cardiac interventions, focus is also being placed on developing miniature LVADs that partially support the left ventricle. More-compact, less-invasive axial-flow blood pumps are being developed for long-term use and early intervention to treat HF.99–101 Some are intended to serve as early intervention devices that target myocardial reconditioning,102 which may remove the need for chronic MCS and reduce the number of patients on the heart transplant wait list.103
Although continuous-flow devices cannot completely mimic normal physiology, future devices may mitigate the complications associated with continuous-flow pumps by providing rhythmic, reproducible changes in rotational speeds. A more physiologic arterial pulsatility can reduce peripheral resistance and improve end-organ perfusion. Because diminished pulsatility may result in elevated vascular impedance and stiffness, a rhythmic change in rotational speed may restore normal vascular impedance and compliance. An additional benefit of periodic speed variations is that they could provide washout to potentially stagnant regions. A reproducible change in rotational speeds can also modulate the aortic pressure waveform, which may enhance coronary flow by providing higher driving force for myocardial perfusion. With such improvements, blood pumps might more closely approximate normal circulatory physiology while maintaining adequate circulatory support.104
Acknowledgments
We thank Joe Brewton for providing Figure 1A, Figures 2A and 2B, Figure 3A, Figure 4, and Figure 5; George Pantalos, PhD, for providing Figure 6; and Chris Durst, PhD, for providing Figure 7. Jeanie F. Woodruff, BS, ELS, and Nicole Stancel, PhD, ELS(D), provided editorial support.
Abbreviations and Acronyms
- FDA
US Food and Drug Administration
- HF
heart failure
- LVAD
left ventricular assist device
- MCS
mechanical circulatory support
- MI
myocardial infarction
- NYHA
New York Heart Association
- PIV
particle image velocimetry
- VAD
ventricular assist device
Funding Statement
Funding/Support: No funding support was received for this work.
Footnotes
Conflict of Interest Disclosures: O.H.F. has received consultant fees from ABIOMED and receives related travel reimbursement from BiVACOR, Inc. The remaining authors have no conflicts of interest to report.
References
- 1.Cardiovascular diseases (CVDs) World Health Organization. Updated June 11, 2021 Accessed April 19, 2022. http://www.who.int/mediacentre/factsheets/fs317/en/
- 2.National Clinical Guideline Centre Chronic heart failure: NICE guideline. Royal College of Physicians. Published September 12, 2018. Accessed March 22, 2023. http://www.rcplondon.ac.uk/guidelines-policy/chronic-heart-failure-nice-guideline.
- 3.Tsao CW, Aday AW, Almarzooq ZI et al. Heart disease and stroke statistics—2022 update: a report from the American Heart Association. Circulation . 2022;145(8):e153–e639. doi: 10.1161/CIR.0000000000001052. [DOI] [PubMed] [Google Scholar]
- 4.Benjamin EJ, Blaha MJ, Chiuve SE, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics—2017 update: a report from the American Heart Association. Circulation . 2017;135(10):e146–e603. doi: 10.1161/CIR.0000000000000485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Writing Group Members. Mozaffarian D, Benjamin EJ, Go AS, et al. American Heart Association Statistics Committee; Stroke Statistics Subcommittee Heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation . 2016;133(4):e38–360. doi: 10.1161/CIR.0000000000000350. [DOI] [PubMed] [Google Scholar]
- 6.Classes of heart failure. American Heart Association Updated May 31, 2017. Accessed March 21, 2023. https://www.heart.org/en/health-topics/heart-failure/what-is-heart-failure/classes-of-heart-failure.
- 7.Copeland JG, Smith RG, Arabia FA, et al. CardioWest Total Artificial Heart Investigators Cardiac replacement with a total artificial heart as a bridge to transplantation. N Engl J Med . 2004;351(9):859–867. doi: 10.1056/NEJMoa040186. [DOI] [PubMed] [Google Scholar]
- 8.Fiane AE. Long-term left ventricle assist device (LVAD) therapy with rotary pumps. Scand Cardiovasc J . 2009;43(6):357–359. doi: 10.1080/14017430903085893. [DOI] [PubMed] [Google Scholar]
- 9.DeBakey ME. Left ventricular bypass pump for cardiac assistance. Clinical experience Am J Cardiol. 1971;27(1):3–11. doi: 10.1016/0002-9149(71)90076-2. [DOI] [PubMed] [Google Scholar]
- 10.Frazier OH, Kirklin J, editors. ISHLT Monograph Series Mechanical Circulatory Support . Vol 1. Elsevier; 2006. [Google Scholar]
- 11.Norman JC, Duncan JM, Frazier OH et al. Intracorporeal (abdominal) left ventricular assist devices or partial artificial hearts: a five-year clinical experience. Arch Surg . 1981;116(11):1441–1445. doi: 10.1001/archsurg.1981.01380230059009. [DOI] [PubMed] [Google Scholar]
- 12.Frazier OH. History of mechanical circulatory support. In: Morgan JA, Civitello AB, Frazier OH, editors. Mechanical Circulatory Support for Advanced Heart Failure A Texas Heart Institute/Baylor College of Medicine Approach . Springer International Publishing; 2018. pp. 1–13. [Google Scholar]
- 13.Tamez D, Myers TJ, Inman RW, Miller KA, Frazier OH. Clinical evaluation of the HeartPak. a new pneumatic portable driver for use with the HeartMate implantable pneumatic left ventricular assist system. ASAIO J . 1997;43(5):M797–M801. [PubMed] [Google Scholar]
- 14.Frazier OH, Rose EA, McCarthy P et al. Improved mortality and rehabilitation of transplant candidates treated with a long-term implantable left ventricular assist system. Ann Surg . 1995;222(3):327–336. doi: 10.1097/00000658-199509000-00010. discussion 336–338. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Shinn JA. Novacor left ventricular assist system. AACN Clin Issues Crit Care Nurs . 1991;2(3):575–586. doi: 10.4037/15597768-1991-3021. [DOI] [PubMed] [Google Scholar]
- 16.Starnes VA, Oyer PE, Portner PM et al. Isolated left ventricular assist as bridge to cardiac transplantation. J Thorac Cardiovasc Surg . 1988;96(1):62–71. [PubMed] [Google Scholar]
- 17.Farkas EA, Elefteriades JA. Assisted circulation: experience with the Novacor left ventricular assist system. Expert Rev Med Devices . 2007;4(6):769–774. doi: 10.1586/17434440.4.6.769. [DOI] [PubMed] [Google Scholar]
- 18.Rose EA, Gelijns AC, Moskowitz AJ, et al. Randomized Evaluation of Mechanical Assistance for the Treatment of Congestive Heart Failure (REMATCH) Study Group Long-term use of a left ventricular assist device for end-stage heart failure. N Engl J Med . 2001;345(20):1435–1443. doi: 10.1056/NEJMoa012175. [DOI] [PubMed] [Google Scholar]
- 19.Hunt SA. Comment—the REMATCH trial: long-term use of a left ventricular assist device for end-stage heart failure. J Card Fail . 2002;8(2):59–60. doi: 10.1054/jcaf.2002.32944. [DOI] [PubMed] [Google Scholar]
- 20.Cohn WE, Timms DL, Frazier OH. Total artificial hearts: past, present, and future. Nat Rev Cardiol . 2015;12(10):609–617. doi: 10.1038/nrcardio.2015.79. [DOI] [PubMed] [Google Scholar]
- 21.Wampler RK, Moise JC, Frazier OH, Olsen DB. In vivo evaluation of a peripheral vascular access axial flow blood pump. ASAIO Trans . 1988;34(3):450–454. [PubMed] [Google Scholar]
- 22.Frazier OH, Myers TJ, Jarvik RK et al. Research and development of an implantable, axial-flow left ventricular assist device: the Jarvik 2000 Heart. Ann Thorac Surg . 2001;71(3 suppl):S125–S132. doi: 10.1016/s0003-4975(00)02614-x. discussion S144–S146. doi. [DOI] [PubMed] [Google Scholar]
- 23.Kirklin JK, Mehra M, West LJ, editors. ISHLT Monograph Series History of International Heart and Lung Transplantation . Vol 4. Elsevier; 2010. [Google Scholar]
- 24.Parnis SM, Conger JL, Fuqua JM, Jr et al. Progress in the development of a transcutaneously powered axial flow blood pump ventricular assist system. ASAIO J . 1997;43(5):M576–M580. [PubMed] [Google Scholar]
- 25.Butler KC, Dow JJ, Litwak P, Kormos RL, Borovetz HS. Development of the Nimbus/University of Pittsburgh innovative ventricular assist system. Ann Thorac Surg . 1999;68(2):790–794. doi: 10.1016/s0003-4975(99)00582-2. [DOI] [PubMed] [Google Scholar]
- 26.Frazier OH, Delgado RM, III, Kar B, Patel V, Gregoric ID, Myers TJ. First clinical use of the redesigned HeartMate II left ventricular assist system in the United States: a case report. Tex Heart Inst J . 2004;31(2):157–159. [PMC free article] [PubMed] [Google Scholar]
- 27.Larose JA, Tamez D, Ashenuga M, Reyes C. Design concepts and principle of operation of the HeartWare ventricular assist system. ASAIO J . 2010;56(4):285–289. doi: 10.1097/MAT.0b013e3181dfbab5. [DOI] [PubMed] [Google Scholar]
- 28.Schmitto JD, Hanke JS, Rojas SV, Avsar M, Haverich A. First implantation in man of a new magnetically levitated left ventricular assist device (HeartMate III) J Heart Lung Transplant . 2015;34(6):858–860. doi: 10.1016/j.healun.2015.03.001. [DOI] [PubMed] [Google Scholar]
- 29.Cheung A, Chorpenning K, Tamez D et al. Design concepts and preclinical results of a miniaturized HeartWare platform: the MVAD system. Innovations (Phila) . 2015;10(3):151–156. doi: 10.1097/IMI.0000000000000155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Elliott AM, Lampert BC. Patient selection for long-term mechanical circulatory support: is it ever too early for the NYHA class III patient? Curr Heart Fail Rep . 2016;13(1):13–19. doi: 10.1007/s11897-016-0279-7. [DOI] [PubMed] [Google Scholar]
- 31.Sweeney MS. The Hemopump in 1997: a clinical, political, and marketing evolution. Ann Thorac Surg . 1999;68(2):761–763. doi: 10.1016/s0003-4975(99)00587-1. [DOI] [PubMed] [Google Scholar]
- 32.Butler KC, Moise JC, Wampler RK. The Hemopump—a new cardiac prothesis device. IEEE Trans Biomed Eng . 1990;37(2):193–196. doi: 10.1109/10.46259. [DOI] [PubMed] [Google Scholar]
- 33.Frazier OH, Nakatani T, Duncan JM, Parnis SM, Fuqua JM. Clinical experience with the Hemopump. ASAIO Trans . 1989;35(3):604–606. doi: 10.1097/00002480-198907000-00141. [DOI] [PubMed] [Google Scholar]
- 34.Wampler RK, Frazier OH, Lansing AM et al. Treatment of cardiogenic shock with the Hemopump left ventricular assist device. Ann Thorac Surg . 1991;52(3):506–513. doi: 10.1016/0003-4975(91)90913-b. [DOI] [PubMed] [Google Scholar]
- 35.Baldwin RT, Radovancević B, Duncan JM, Wampler RK, Frazier OH. Management of patients supported on the Hemopump cardiac assist system. Tex Heart Inst J . 1992;19(2):81–86. [PMC free article] [PubMed] [Google Scholar]
- 36.Meyns B, Siess T, Laycock S, Reul H, Rau G, Flameng W. The heart-Hemopump interaction: a study of Hemopump flow as a function of cardiac activity. Artif Organs . 1996;20(5):641–649. doi: 10.1111/j.1525-1594.1996.tb04496.x. [DOI] [PubMed] [Google Scholar]
- 37.Song X, Throckmorton AL, Untaroiu A et al. Axial flow blood pumps. ASAIO J . 2003;49(4):355–364. [PubMed] [Google Scholar]
- 38.Duncan JM, Frazier OH, Radovancevic B, Velebit V. Implantation techniques for the Hemopump. Ann Thorac Surg . 1989;48(5):733–735. doi: 10.1016/0003-4975(89)90810-2. [DOI] [PubMed] [Google Scholar]
- 39.Frazier OH, Wampler RK, Duncan JM et al. First human use of the Hemopump, a catheter-mounted ventricular assist device. Ann Thorac Surg . 1990;49(2):299–304. doi: 10.1016/0003-4975(90)90155-y. [DOI] [PubMed] [Google Scholar]
- 40.Cooper GJ, Loisance DY, Miyama M, Abe Y, Deleuze PH. Direct mechanical assistance of the right ventricle with the Hemopump in a porcine model. Ann Thorac Surg . 1995;59(2):443–447. doi: 10.1016/0003-4975(94)00048-c. [DOI] [PubMed] [Google Scholar]
- 41.Wiebalck AC, Wouters PF, Waldenberger FR et al. Left ventricular assist with an axial flow pump (Hemopump): clinical application. Ann Thorac Surg . 1993;55(5):1141–1146. doi: 10.1016/0003-4975(93)90021-9. [DOI] [PubMed] [Google Scholar]
- 42.Lee S, Fukamachi K, Golding L, Moazami N, Starling RC. Left ventricular assist devices: from the bench to the clinic. Cardiology . 2013;125(1):1–12. doi: 10.1159/000346865. [DOI] [PubMed] [Google Scholar]
- 43.Westaby S, Banning A, Neil D, Poole-Wilson P, Frazier OH. Optimism derived from 7.5 years of continuous-flow circulatory support. J Thorac Cardiovasc Surg . 2010;139(3):e45–e47. doi: 10.1016/j.jtcvs.2008.05.072. [DOI] [PubMed] [Google Scholar]
- 44.Capoccia M, Bowles CT, Sabashnikov A et al. A UK single centre retrospective analysis of the relationship between haemodynamic changes and outcome in patients undergoing prolonged left ventricular assist device support. Ann Thorac Cardiovasc Surg . 2015;21(2):151–156. doi: 10.5761/atcs.oa.14-00075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Kohno H, Matsumiya G, Sawa Y et al. The Jarvik 2000 left ventricular assist device as a bridge to transplantation: Japanese Registry for Mechanically Assisted Circulatory Support. J Heart Lung Transplant . 2018;37(1):71–78. doi: 10.1016/j.healun.2017.10.016. [DOI] [PubMed] [Google Scholar]
- 46.Maher TR, Butler KC, Poirier VL, Gernes DB. HeartMate left ventricular assist devices: a multigeneration of implanted blood pumps. Artif Organs . 2001;25(5):422–426. doi: 10.1046/j.1525-1594.2001.06756.x. [DOI] [PubMed] [Google Scholar]
- 47.Griffith BP, Kormos RL, Borovetz HS et al. HeartMate II left ventricular assist system: from concept to first clinical use. Ann Thorac Surg . 2001;71(3 suppl):S116–S120. doi: 10.1016/s0003-4975(00)02639-4. discussion S114–S116. [DOI] [PubMed] [Google Scholar]
- 48.Wu ZJ, Antaki JF, Burgreen GW, Butler KC, Thomas DC, Griffith BP. Fluid dynamic characterization of operating conditions for continuous flow blood pumps. ASAIO J . 1999;45(5):442–449. doi: 10.1097/00002480-199909000-00015. [DOI] [PubMed] [Google Scholar]
- 49.Thomas DC, Butler KC, Taylor LP et al. Continued development of the Nimbus/University of Pittsburgh (UOP) axial flow left ventricular assist system. ASAIO J . 1997;43(5):M564–M566. [PubMed] [Google Scholar]
- 50.Macha M, Litwak P, Yamazaki K et al. Survival for up to six months in calves supported with an implantable axial flow ventricular assist device. ASAIO J . 1997;43(4):311–315. [PubMed] [Google Scholar]
- 51.Miller LW, Pagani FD, Russell SD, et al. HeartMate II Clinical Investigators Use of a continuous-flow device in patients awaiting heart transplantation. N Engl J Med . 2007;357(9):885–896. doi: 10.1056/NEJMoa067758. [DOI] [PubMed] [Google Scholar]
- 52.Cabrera AG, Sundareswaran KS, Samayoa AX et al. Outcomes of pediatric patients supported by the HeartMate II left ventricular assist device in the United States. J Heart Lung Transplant . 2013;32(11):1107–1113. doi: 10.1016/j.healun.2013.07.012. [DOI] [PubMed] [Google Scholar]
- 53.Siess T, Reul H, Rau G. Concept, realization, and first in vitro testing of an intraarterial microaxial blood pump. Artif Organs . 1995;19(7):644–652. doi: 10.1111/j.1525-1594.1995.tb02396.x. [DOI] [PubMed] [Google Scholar]
- 54.Apel J, Paul R, Klaus S, Siess T, Reul H. Assessment of hemolysis related quantities in a microaxial blood pump by computational fluid dynamics. Artif Organs . 2001;25(5):341–347. doi: 10.1046/j.1525-1594.2001.025005341.x. [DOI] [PubMed] [Google Scholar]
- 55.Siess T, Nix C, Menzler F. From a lab type to a product: a retrospective view on Impella's assist technology. Artif Organs . 2001;25(5):414–421. doi: 10.1046/j.1525-1594.2001.025005414.x. [DOI] [PubMed] [Google Scholar]
- 56.Siess T, Reul H, Rau G. Hydraulic refinement of an intraarterial microaxial blood pump. Int J Artif Organs . 1995;18(5):273–285. [PubMed] [Google Scholar]
- 57.Triep M, Brücker C, Schröder W, Siess T. Computational fluid dynamics and digital particle image velocimetry study of the flow through an optimized micro-axial blood pump. Artif Organs . 2006;30(5):384–391. doi: 10.1111/j.1525-1594.2006.00230.x. [DOI] [PubMed] [Google Scholar]
- 58.Lamarche Y, Cheung A, Ignaszewski A et al. Comparative outcomes in cardiogenic shock patients managed with Impella microaxial pump or extracorporeal life support. J Thorac Cardiovasc Surg . 2011;142(1):60–65. doi: 10.1016/j.jtcvs.2010.07.075. [DOI] [PubMed] [Google Scholar]
- 59.Dixon SR, Henriques JP, Mauri L et al. A prospective feasibility trial investigating the use of the Impella 2.5 system in patients undergoing high-risk percutaneous coronary intervention (the PROTECT I trial): initial U.S. experience. JACC Cardiovasc Interv . 2009;2(2):91–96. doi: 10.1016/j.jcin.2008.11.005. [DOI] [PubMed] [Google Scholar]
- 60.Anderson MB, Goldstein J, Milano C et al. Benefits of a novel percutaneous ventricular assist device for right heart failure: the prospective RECOVER RIGHT study of the Impella RP device. J Heart Lung Transplant . 2015;34(12):1549–1560. doi: 10.1016/j.healun.2015.08.018. [DOI] [PubMed] [Google Scholar]
- 61.Meyns B, Stolinski J, Leunens V, Verbeken E, Flameng W. Left ventricular support by catheter-mounted axial flow pump reduces infarct size. J Am Coll Cardiol . 2003;41(7):1087–1095. doi: 10.1016/s0735-1097(03)00084-6. [DOI] [PubMed] [Google Scholar]
- 62.Herbertson LH, Olia SE, Daly A et al. Multilaboratory study of flow-induced hemolysis using the FDA benchmark nozzle model. Artif Organs . 2015;39(3):237–248. doi: 10.1111/aor.12368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Benkowski RJ, Hudson L, inventors;, Reliant Heart, Inc., assignee Rotary blood pump. US patent US8376926B2. Feb 19, 2013.
- 64.Benkowski RJ, Kiris C, Kwak D, Rosenbaum BJ, Bacak JW, DeBakey ME, inventors;, MicroMed Technology, Inc, assignee Rotary blood pump. US patent 5,947,892. September 7, 1999.
- 65.DeBakey ME. The odyssey of the artificial heart. Artif Organs . 2000;24(6):405–411. doi: 10.1046/j.1525-1594.2000.06635.x. [DOI] [PubMed] [Google Scholar]
- 66.SoRelle R. First US implantation of DeBakey ventricular assist device. Circulation . 2000;101(24):E9056–E9057. doi: 10.1161/01.cir.101.24.e9056. [DOI] [PubMed] [Google Scholar]
- 67.Noon GP, Morley DL, Irwin S, Abdelsayed SV, Benkowski RJ, Lynch BE. Clinical experience with the MicroMed DeBakey ventricular assist device. Ann Thorac Surg . 2001;71(3 suppl):S133–S138. doi: 10.1016/s0003-4975(00)02634-5. discussion S144–S146. [DOI] [PubMed] [Google Scholar]
- 68.Agati S, Bruschi G, Russo C, Colombo T, Lanfranconi M, Vitali E. First successful Italian clinical experience with DeBakey VAD. J Heart Lung Transplant . 2001;20(8):914–917. doi: 10.1016/s1053-2496(01)00256-x. [DOI] [PubMed] [Google Scholar]
- 69.Benkowski R, Morley D, Abdelsayed S, Noon GP. Clinical update and transition to destination therapy for the MicroMed DeBakey VAD. Paper presented at: International Society for Rotary Blood Pumps 10th Congress; September 11–14, 2002; Osaka, Japan. [Google Scholar]
- 70.Medtronic to expand heart failure portfolio with acquisition of HeartWare International. News release. Medtronic. June 27, 2016. Accessed April 27, 2022. https://news.medtronic.com/2016-06-27-Medtronic-to-Expand-Heart-Failure-Portfolio-with-Acquisition-of-Heartware-International.
- 71.Slaughter MS, Giridharan GA, Tamez D et al. Transapical miniaturized ventricular assist device: design and initial testing. J Thorac Cardiovasc Surg . 2011;142(3):668–674. doi: 10.1016/j.jtcvs.2011.01.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Schima H, Zrunek P, Stoiber M et al. Extended in vivo evaluation of a miniaturized axial flow pump with a novel inflow cannula for a minimal invasive implantation procedure. J Heart Lung Transplant . 2014;33(4):422–428. doi: 10.1016/j.healun.2013.10.032. [DOI] [PubMed] [Google Scholar]
- 73.Slaughter MS, Sobieski MA, Jr, Tamez D et al. HeartWare miniature axial-flow ventricular assist device: design and initial feasibility test. Tex Heart Inst J . 2009;36(1):12–16. [PMC free article] [PubMed] [Google Scholar]
- 74.Giridharan GA, Lee TJ, Ising M et al. Miniaturization of mechanical circulatory support systems. Artif Organs . 2012;36(8):731–739. doi: 10.1111/j.1525-1594.2012.01523.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Meyns B, Siess T, Nishimura Y et al. Miniaturized implantable rotary blood pump in atrial-aortic position supports and unloads the failing heart. Cardiovasc Surg . 1998;6(3):288–295. doi: 10.1016/s0967-2109(97)00170-1. [DOI] [PubMed] [Google Scholar]
- 76.Perriello B. HeartWare buys CircuLite for up to $350M. Mass Device. December 2, 2013 Accessed April 27, 2022. https://www.massdevice.com/heartware-buys-circulite-350m/
- 77.Meyns B, Rega F, Droogne W, Simon A, Klotz S, Burkhoff D. Initial clinical experience with the Circulite Synergy device for partial circulatory support [abstract] J Card Fail . 2008;14(6 suppl):S45–S46. doi: 10.1016/j.cardfail.2008.06.142. [DOI] [Google Scholar]
- 78.Klotz S, Meyns B, Simon A et al. Partial mechanical long-term support with the CircuLite Synergy pump as bridge-to-transplant in congestive heart failure. Thorac Cardiovasc Surg . 2010;58(suppl 2):S173–S178. doi: 10.1055/s-0029-1240687. [DOI] [PubMed] [Google Scholar]
- 79.Meyns BP, Simon A, Klotz S et al. Clinical benefits of partial circulatory support in New York Heart Association class IIIB and early class IV patients. Eur J Cardiothorac Surg . 2011;39(5):693–698. doi: 10.1016/j.ejcts.2010.07.049. [DOI] [PubMed] [Google Scholar]
- 80.Barbone A, Pini D, Rega F, Ornaghi D, Vitali E, Meyns B. Circulatory support in elderly chronic heart failure patients using the CircuLite Synergy system. Eur J Cardiothorac Surg . 2013;44(2):207–212. doi: 10.1093/ejcts/ezt041. discussion 212. [DOI] [PubMed] [Google Scholar]
- 81.Klotz S, Charitos EI, Meyer-Saraei R, Sievers HH. CircuLite left ventricular assist device explantation: a word of caution. J Heart Lung Transplant . 2014;33(4):451–452. doi: 10.1016/j.healun.2014.01.002. [DOI] [PubMed] [Google Scholar]
- 82.Etz C, Welp H, Rothenburger M et al. Analysis of platelet function during left ventricular support with the Incor and Excor system. Heart Surg Forum . 2004;7(5):E423–E427. doi: 10.1532/HSF98.20041073. [DOI] [PubMed] [Google Scholar]
- 83.Schmid C, Tjan TDT, Etz C et al. First clinical experience with the Incor left ventricular assist device. J Heart Lung Transplant . 2005;24(9):1188–1194. doi: 10.1016/j.healun.2004.08.024. [DOI] [PubMed] [Google Scholar]
- 84.Attisani M, Centofanti P, La Torre M, Campanella A, Sansone F, Rinaldi M. Safety and effectiveness of low dosing of double antiplatelet therapy during long-term left ventricular support with the INCOR system. J Artif Organs . 2010;13(4):202–206. doi: 10.1007/s10047-010-0527-7. [DOI] [PubMed] [Google Scholar]
- 85.Bartoli CR, Dowling RD. The future of adult cardiac assist devices: novel systems and mechanical circulatory support strategies. Cardiol Clin . 2011;29(4):559–582. doi: 10.1016/j.ccl.2011.08.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Shabari FR, George J, Cuchiara MP et al. Improved hemodynamics with a novel miniaturized intra-aortic axial flow pump in a porcine model of acute left ventricular dysfunction. ASAIO J . 2013;59(3):240–245. doi: 10.1097/MAT.0b013e31828a6e74. [DOI] [PubMed] [Google Scholar]
- 87.Procyrion announces successful first-in-human cases in cardiorenal syndrome (CRS) patients with Aortix percutaneous mechanical circulatory support device. News release. Procyrion. May 25, 2021. Accessed April 27, 2022. https://www.procyrion.com/news/procyrion-announces-successful-first-in-human-cases-in-cardiorenal-syndrome-crs-patients-with-aortix-tm-percutaneous-mechanical-circulatory-support-device.
- 88.Wu EL, Kleinheyer M, Ündar A. Pulsatile vs continuous flow. In: Gregory S, Stevens M, Fraser JF, editors. Mechanical Circulatory and Respiratory Support . Academic Press; 2017. pp. 379–406. [Google Scholar]
- 89.Miller L. We always need a pulse, or do we?? J Cardiovasc Transl Res . 2012;5(3):296–301. doi: 10.1007/s12265-012-9360-0. [DOI] [PubMed] [Google Scholar]
- 90.Heyde EC. Gastrointestinal bleeding in aortic stenosis. N Engl J Med . 1958;259:196. [Google Scholar]
- 91.Chan CHH, Pieper IL, Fleming S et al. The effect of shear stress on the size, structure, and function of human von Willebrand factor. Artif Organs . 2014;38(9):741–750. doi: 10.1111/aor.12382. [DOI] [PubMed] [Google Scholar]
- 92.Pya Y, Maly J, Bekbossynova M et al. First human use of a wireless coplanar energy transfer coupled with a continuous-flow left ventricular assist device. J Heart Lung Transplant . 2019;38(4):339–343. doi: 10.1016/j.healun.2019.01.1316. [DOI] [PubMed] [Google Scholar]
- 93.Burch GE, Giles TD. Alcoholic cardiomyopathy. Concept of the disease and its treatment. Am J Med . 1971;50(2):141–145. doi: 10.1016/0002-9343(71)90143-4. [DOI] [PubMed] [Google Scholar]
- 94.Burch GE, McDonald CD, Walsh JJ. The effect of prolonged bed rest on postpartal cardiomyopathy. Am Heart J . 1971;81(2):186–201. doi: 10.1016/0002-8703(71)90129-3. [DOI] [PubMed] [Google Scholar]
- 95.McDonald CD, Burch GE, Walsh JJ. Prolonged bed rest in the treatment of idiopathic cardiomyopathy. Am J Med . 1972;52(1):41–50. doi: 10.1016/0002-9343(72)90006-x. [DOI] [PubMed] [Google Scholar]
- 96.Frazier OH, Baldwin ACW, Demirozu ZT et al. Ventricular reconditioning and pump explantation in patients supported by continuous-flow left ventricular assist devices. J Heart Lung Transplant . 2015;34(6):766–772. doi: 10.1016/j.healun.2014.09.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Birks EJ, George RS, Hedger M et al. Reversal of severe heart failure with a continuous-flow left ventricular assist device and pharmacological therapy: a prospective study. Circulation . 2011;123(4):381–390. doi: 10.1161/CIRCULATIONAHA.109.933960. [DOI] [PubMed] [Google Scholar]
- 98.Burkhoff D, Klotz S, Mancini DM. LVAD-induced reverse remodeling: basic and clinical implications for myocardial recovery. J Card Fail . 2006;12(3):227–239. doi: 10.1016/j.cardfail.2005.10.012. [DOI] [PubMed] [Google Scholar]
- 99.Wang Y, Smith PA, Timms DL, Hsu PL, McMahon RA. In vitro evaluation of the dual-diffuser design for a reversible rotary intra-aortic ventricular assist device. Artif Organs . 2016;40(9):884–893. doi: 10.1111/aor.12746. [DOI] [PubMed] [Google Scholar]
- 100.Smith PA, Wang Y, Bieritz SA et al. Design method using statistical models for miniature left ventricular assist device hydraulics. Ann Biomed Eng . 2019;47(1):126–137. doi: 10.1007/s10439-018-02140-w. [DOI] [PubMed] [Google Scholar]
- 101.Smith PA, Wang Y, Bieritz SA et al. Hemodynamic evaluation of an intra-atrial blood pump on a pulsatile mock circulatory loop. Annu Int Conf IEEE Eng Med Biol Soc . 2018;2018:4508–4511. doi: 10.1109/EMBC.2018.8513133. [DOI] [PubMed] [Google Scholar]
- 102.Clifton WL, Heuring J, Hertzog B. Initial results with a novel intra-aortic cardiorenal support device. J Am Coll Cardiol . 2014;63(12 suppl):A813. doi: 10.1016/S0735-1097(14)60813-5. [DOI] [Google Scholar]
- 103.Smith RE, Smith PA, Cohn WE. Predicting the dimensions of an intracardiac partial-assist pump for percutaneous delivery by analytical and numerical methods. Cardiovasc Eng Technol . 2017;8(4):453–564. doi: 10.1007/s13239-017-0331-0. [DOI] [PubMed] [Google Scholar]
- 104.Ising MS, Sobieski MA, Slaughter MS, Koenig SC, Giridharan GA. Feasibility of pump speed modulation for restoring vascular pulsatility with rotary blood pumps. ASAIO J . 2015;61(5):526–532. doi: 10.1097/MAT.0000000000000262. [DOI] [PubMed] [Google Scholar]