

Abstract
Germinal matrix and intraventricular hemorrhage (GM-IVH) are the major causes of intracranial hemorrhage in premature infants. Cranial ultrasound (cUS) is the imaging modality of choice for diagnosing and classifying GM-IVH. Magnetic resonance imaging (MRI), usually performed at term-equivalent age, is more sensitive than cUS in identifying hemorrhage in the brain. Post-hemorrhagic ventricular dilatation is a significant complication of GM-IVH and correlates with adverse neurodevelopmental outcomes. In this review, we discuss the various imaging findings of GM-IVH in premature infants, focusing on the role of cUS and MRI.
Keywords: Premature infant, Hemorrhage, Ultrasonography, Magnetic resonance imaging
INTRODUCTION
Germinal matrix and intraventricular hemorrhage (GMIVH) are common and characteristic problems in premature infants, especially very low birth weight (VLBW; <1500 g) or gestational age (GA) <32 weeks [1,8,33]. The incidence increases as GA and body weight decrease. The germinal matrix is a transient, highly vascular structure, with thin-walled vessels, that is susceptible to hemorrhage. Hemorrhage can be confined to the GM or spread into the lateral ventricles, which can lead to post-hemorrhagic ventricular dilatation (PHVD) [8,31]. Traditionally, GM-IVH has been classified into four categories [25,33]. Cranial ultrasound (cUS) is the primary imaging modality for premature infants owing to its portability and avoidance of ionizing radiation. Recently, the use of magnetic resonance imaging (MRI), usually performed at near-term-equivalent age (TEA), has increased in premature infants. MRI is not only superior in identifying hemorrhage in the brain but also in identifying white matter injury and cerebellar hemorrhage [14]. This review focuses on the role of cUS and MRI in premature infants and discusses the various imaging findings of GM-IVH and PHVD.
ULTRASONOGRAPHIC DIAGNOSIS OF GM-IVH
Cranial ultrasound is the imaging modality of choice for diagnosis, determination of severity, and progression of GM-IVH. It can be performed at the bedside, providing high-resolution images without ionizing radiation.
Techniques in cranial ultrasound
On coronal and sagittal planes, images of various angles were obtained by tilting the microconvex (5–8 MHz) and high-frequency (10–12 MHz) linear transducers through the fontanelles (anterior, posterior, sphenoid, and mastoid). The anterior fontanelle, the largest fontanelle at the junction of the coronal and sagittal sutures, is the optimal sonic window for the supratentorial structures. The mastoid fontanelle is suitable for evaluating the posterior fossa, such as the cerebellum. The American Academy of Pediatrics (AAP) recommended that cUS screening include the anterior fontanelle and the mastoid fontanelle [15]. High-frequency linear transducers provide detailed visualization of the brain and better resolution, which helps evaluate GM-IVH and brain parenchymal lesions. Usually, we recognize the presence of GM-IVH on coronal scans and determine the amount of hemorrhage on parasagittal scans. Doppler images are obtained through the anterior fontanelle using the anterior cerebral artery in the sagittal plane or the middle cerebral artery in the coronal plane [21]. Pulsed wave Doppler US showed peak systolic velocity (PSV), end-diastolic velocity (EDV), and resistive index (RI; PSV−EDV/PSV), which represent intracranial hemodynamics. The average RI declines with GA, and 0.6–0.9 can be used as the normal range for both term and premature infants [33].
Timing of cranial ultrasound
GM is most prominent at the caudothalamic groove, which is the most common site of germinal matrix hemorrhage (GMH), from 28 to 32 weeks. The precursor cells in the GM show exuberant proliferation until 28 weeks of gestation, then rapidly decline and involute almost completely by approximately 36 weeks. In premature infants, most cases of GM-IVH occur within the first 3 days after birth. Approximately 95% of GM-IVH cases occur within 7 days. There are some guidelines for screening cUS in premature infants [7,13,15,22].
The AAP recommends cUS for screening and serial evaluation of GM-IVH and periventricular leukomalacia in premature (<30 weeks gestation or >30 weeks gestation with significant risk factors) and VLBW infants [15]. They recommend an initial screening cUS within 7 days. Repeat screening cUS is recommended at 4–6 weeks of age to identify PVL and at TEA or before discharge to determine the permanent effect of brain injury, which can be related to adverse neurodevelopmental outcomes in premature infants.
Grading of GM-IVH
The most used grading system for GM-IVH (Table 1) was reported in 1978 by Papile et al. [25], which was based on computed tomography; however, it is no longer the recommended imaging modality for premature infants owing to ionizing radiation. In the Papile system, grade I was defined as subependymal hemorrhage, grade II as IVH without ventricular dilatation, grade III as IVH with ventricular dilatation, and grade IV as IVH with parenchymal hemorrhage. Based on the understanding of the drainage of the medullary vein in the deep white matter, parenchymal hemorrhage is considered periventricular hemorrhagic infarction (PVHI) owing to impaired venous drainage and not a parenchymal extension of IVH [30].
Table 1.
Grading systems of GM-IVH and related statistics
| Grade | Papile (1978) based on CT | Volpe (2008) based on cUS | Percentage of GM-IVH | Mortality rate | Incidence of definite neurological sequelae |
|---|---|---|---|---|---|
| I | Subependymal hemorrhage | GMH with no or minimal IVH (<10% on parasagittal view) | 40% | 0–12% | 15% |
| II | IVH without ventricle dilatation | IVH (10–50% on parasagittal view) | 25% | 2–24% | 25% |
| III | IVH with ventricle dilatation | IVH (>50% on parasagittal view; usually distends lateral ventricle) | 20% | 8–32% | 50% |
| IV | IVH with parenchymal hemorrhage | Periventricular echodensity (called PVHI) | 15% | 22–45% | 75% |
GM-IVH : germinal matrix and intraventricular hemorrhage, CT : computed tomography, cUS : cranial ultrasound, GMH : germinal matrix hemorrhage, IVH : intraventricular hemorrhage, PVHI : periventricular hemorrhagic infarction
The Papile system was adapted by Volpe in 2008 on the basis of US findings, including the presence of GM-IVH and the amount of blood in the lateral ventricles (Table 1) [33]. In the Volpe system, grade I was defined as GMH with no or minimal IVH (<10% of the ventricular area on parasagittal view), grade II as IVH occupying 10% to 50% of the ventricular area in the parasagittal view, grade III as IVH occupying >50% of the ventricular area on parasagittal view with usually distending the lateral ventricle, and the separate notation of periventricular echodensity (location and extent). Periventricular echodensity (i.e., PVHI) can occur in any grade (I–III) of GM-IVH. However, because PVHI is usually accompanied by severe GM-IVH (grade III), most reports continue to use the term “grade IV” GM-IVH in the presence of PVHI, according to the Papile system.
Cranial ultrasound findings of GM-IVH
Grade I hemorrhage restricted to the subependymal germinal matrix typically shows a hyperechoic globular lesion located in the caudothalamic groove (Fig. 1A and B) [8,27,29]. Over time, the hematoma becomes heterogeneous and undergoes cystic changes (Fig. 2A and B). The recognition of minimal IVH using cUS is still challenging.
Fig. 1.

Cranial ultrasound grading of germinal matrix and intraventricular hemorrhage (GM-IVH). A and B : Grade 1 GM-IVH. Coronal scan and parasagittal scans show echogenic globular hemorrhage (arrows) at the bilateral caudothalamic groove, a typical location of GMH. C and D : Grade 2 GM-IVH. Bilateral IVH (arrows) extending anteriorly to the caudothalamic groove occupy more than 10% of ventricle without ventricular dilatation. E and F : Grade 3 GM-IVH. Coronal scan shows left IVH (arrow) with ventricular dilatation (dashed arrow). Parasagittal scan shows IVH (arrows) occupying more than 50% of ventricle. G and H : Grade 4 GM-IVH. Coronal and left parasagittal scans show fan-shaped echogenic periventricular hemorrhagic infarction (arrows) with ipsilateral grade III IVH (dashed arrows).
Fig. 2.

Cystic degeneration of grade II germinal matrix and intraventricular hemorrhage (GM-IVH) in preterm infant (gestational age gestational age 26+2 weeks). Coronal (A) and right parasagittal (B) scans of cranial ultrasound show heterogeneous hematoma (arrow) at caudothalamic groove with cystic degeneration (arrow). C and D : Magnetic resonance imaging at term-equivalent age, 4 months later. Axial T2-weighted image (C) shows cysts with low signal intensity rim (white arrows) at bilateral caudothalamic groove and low signal intensity along bilateral choroid plexus (black arrows) indicate previous hemorrhage. Susceptibility-weighted imaging (D) shows linear dark signal intensity (black arrows) along wall of bilateral occipital horns of lateral ventricles, indicating minimal IVH, not detectable at cranial ultrasound.
Grade II hemorrhage is IVH without ventricular dilatation (Fig. 1C and D). If the echogenic lesions are anterior to the caudothalamic groove or at the dependent portion of the occipital horns, this suggests IVH [29]. The choroid plexus does not extend into the frontal or occipital horns passing the atrium [20]. The echogenic wall of the ventricle, owing to proliferating subependymal glial cells approximately 1 week after GMIVH, is an indirect sign suggestive of GM-IVH, which might help identify mild GM-IVH (grades I and II) [11].
In grade III hemorrhage, cUS shows ventricular dilatation due to IVH (Fig. 1E and F). Progressive ventricular dilatation after grade II GM-IVH should not be considered grade III [17,27]. We now understand that parenchymal hemorrhage in grade IV GM-IVH of the Papile system is PVHI rather than a parenchymal extension of the hemorrhage [30,33]. It is usually a unilateral, triangular, or “fan-shaped” periventricular echodensity associated with ipsilateral GM-IVH (Fig. 1G and H). Periventricular hemorrhagic infarction can evolve into a porencephalic cyst that often communicates with the adjacent lateral ventricle (Fig. 3).
Fig. 3.

Porencephalic cyst after periventricular hemorrhagic infarction (PVHI). Coronal (A) and left parasagittal (B) scans at 10 weeks of age show focal cystic change (arrows) of PVHI. Follow up coronal (C) and left parasagittal (D) scans at 4 months of age show large porencephalic cyst (arrows) at the site of PVHI with dilatation of left lateral ventricle (dashed arrows).
MAGNETIC RESONANCE IMAGING OF GM-IVH
Although cUS is sensitive for detecting GM-IVH, MRI is superior for detecting small intracranial hemorrhages, which are difficult to diagnose with cUS [14,16,23,26]. Minimal IVH noted grade I GM-IVH is also easily identified on MRI by showing changes in the signal intensity of the ventricular wall (Fig. 2D). Susceptibility-weighted imaging (SWI) and T2*-weighted gradient echo imaging (GRE) are more sensitive in detecting microhemorrhage in the brain than conventional MRI sequences (T1- or T2-weighted images). Up to 50% of patients with a normal cUS show mild GM-IVH (grade I to II) on MRI at the TEA [23]. While most parenchymal hemorrhages show low signal intensity on SWI or GRE on MRI at TEA, not all GMH confined to GM show hemosiderin deposition on MRI [23]. When considering the time between cUS performed serially from birth and MRI performed at TEA, hemorrhage could have been absorbed or have undergone cystic changes. Magnetic resonance imaging of the TEA may show a thin-walled cyst at the caudalthalamic groove, which represents cystic change of GMH (Fig. 2C).
Germinal matrix is also located in the granular layer of the cerebellum, and cerebellar hemorrhage occurs concomitantly with GM-IVH [8]. Large (>4–5 mm) cerebellar hemorrhages can be identified on cUS, and the use of the mastoid fontanelle also improve detection (Fig. 4A and B). MRI is superior to detect and evaluate detailed findings of cerebellar hemorrhage better than cUS, especially microhemorrhage in the cerebellum that may be under-recognized by cUS (Fig. 4C and D). However, the AAP does not recommend brain MRI as a routine imaging protocol for premature infants born at <30 weeks [15]. The difficulty of transporting the infant to the scanner and the long scan time make it difficult to perform MRI in the acute stage. Therefore, MRI is usually performed at TEA or before discharge, and if possible, it is recommended to use the “feed and wrap” technique without sedation. And gadolinium-based contrast materials are not routinely used.
Fig. 4.

Cerebellar hemorrhage identified on cranial ultrasound (A and B) and brain magnetic resonance imaging (C and D) in preterm infants with germinal matrix and intraventricular hemorrhage. Coronal (A) and trans-mastoid (B) scans show intraparenchymal hemorrhage (arrows) in the right cerebellar hemisphere. Axial T2-weighted image (C) and susceptibility-weighted imaging (D) at term-equivalent age of other preterm infant show punctate microhemorrhages (arrows) in cerebellum, not detectable at cranial ultrasound.
POSTHEMORRHAGIC VENTRICULAR DILATATION
PHVD is a substantial complication of GM-IVH in premature infants and develops a few days to a few weeks after GM-IVH [31,33]. The onset and rapidity of PHVD progression are related to the severity of GM-IVH and approximately 65% of infants with progressive PHVD will often arrest within 4 weeks with partial or total resolution of ventricular dilatation (Fig. 5) [33]. Most PHVD are of the communicating type and aqueductal obstruction by blood clot or debris also result acute PHVD [33]. Approximately 30–50% of infants with severe GM-IVH show PHVD, associated with adverse neurodevelopmental outcomes [33].
Fig. 5.

The natural history of posthemorrhagic ventricular dilation in premature infant (gestational age 29+1 weeks). A : Coronal scan on day 2 shows right grade III and left grade IV germinal matrix and intraventricular hemorrhage (GM-IVH). Echogenic hemorrhage in third ventricle (arrow) and both lateral ventricles. B : Echogenic ependymal lining (arrows) and ventricular dilatation begins 1 week after GM-IVH. C : Coronal scan on month 1 shows progression of ventricular dilatation (arrows). D : Coronal scan on month 2 shows spontaneous improvement in ventricular dilatation without treatment.
Ventricle measurements
There are numerous methods for the measurement of the lateral ventricles using cUS (Fig. 6). The ventricular index (VI) and anterior horn width (AHW) are commonly used measurements that showed good intra- and inter-observer agreements [19]. Both measurements were performed using a coronal scan. The VI is the distance between the falx and lateral border of the anterior horn at the level of the foramen of Monro. The AHW is the widest diagonal width of the anterior horn. Another measurement is the thalamo-occipital distance (TOD), which is assessed in the parasagittal scan. The thalamo-occipital distance is the distance between the thalamus and the occipital horn; it has additional value because occipital horn dilatation often precedes frontal horn dilatation. Although normal and cut-off values of variable ventricular measurements have been reported, it is unclear which ventricular measurement in cUS best represents an increase in intracranial pressure (ICP) [2,3].
Fig. 6.
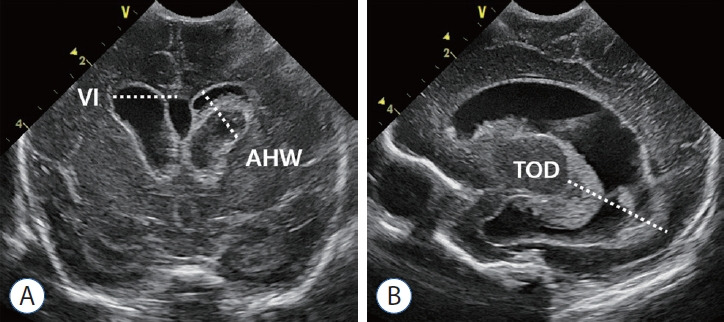
Ventricle measurements on cranial ultrasound. A : Measurements of the ventricular index (VI) and anterior horn width (AHW) on coronal scan. B : Measurements of the thalamo-occipital distance (TOD) on parasagittal scan.
Role of cranial ultrasound in PHVD
Recognition of PHVD is the first step in management. Early identification and quantification of ventricular dilatation using serial cUS are necessary after GM-IVH because ventricular dilatation often precedes clinical symptoms and signs of increased ICP. Frequent follow-up cUS after GM-IVH is recommended at least weekly or more than twice a week until resolution of IVH and stabilization of ventricular dilatation [13,15,33].
In a recently reported framework for managing PHVD, ventricular measurements, including VI, AHW, and TOD, are used as key criteria for risk stratification [10]. In the ELVIS trial (Early vs. Late Ventricular Intervention Study) which included premature infants (≤34 weeks) with progressive PHVD after severe IVH, ventricular measurements were used to determine the threshold that determines the timing of treatment (low threshold : VI >97th percentile and AHW >6 mm and/or TOD >25 mm; and high threshold : VI >97th percentile + 4 mm and AHW >10 mm) [5,6].
In addition to ventricular measurements, RI obtained from pulsed-wave Doppler US could provide important information for treatment decisions. An elevated RI indicates an increased ICP, which may require neurosurgical intervention for PHVD [21]. However, because PDA is a common cause of increased RI, caution is needed in interpreting RI in premature infants.
There is still controversy about when and what type of surgical treatment is needed. A recent randomized controlled trial showed that early intervention with reduced ventricular dilatation could improve neurodevelopmental outcomes [6]. Posthemorrhagic ventricular dilatation can be managed with various neurosurgical procedures: lumbar puncture, ventricular drainage, ventriculoperitoneal shunt, and external third ventriculostomy. We can estimate the effect of treatments by performing serial cUS (Fig. 7).
Fig. 7.

Response of posthemorrhagic ventricular dilatation to ventricular drainage in premature infant. Serial cranial ultrasound images before (A) and after (B) drainage device insertion show change in degree of ventricular dilatation (bidirectional arrows) after procedure. C and D : Coronal scans show the drainage device (arrow).
NEUROIMAGING AS PREDICTIVE TOOLS
Severe GM-IVH (grades III and IV) and PHVD are known to be associated with adverse neurodevelopmental outcomes in premature infants [9,24]. Even mild GM-IVH (grades I and II) could be a risk factor for cerebral palsy and cognitive, hearing, and visual impairment [28].
Attempts have been made to predict short- and long-term neurodevelopmental outcomes in premature infants using neuroimaging. There have been may attempts to predict short- and long-term neurodevelopmental outcome for premature infants using neuroimaging [4,12,18,32]. The predictive value of cUS and brain MRI varies according to several factors [14]. Compared with cUS, brain MRI at the TEA is a useful tool to identify brain injury, but not all imaging findings provide predictive values for neurodevelopmental outcomes [1].
SUMMARY
Cranial US is the best imaging tool for premature infants, not only for the diagnosis and follow-up of GM-IVH. It also plays a major role in the early recognition and management of PHVD after GM-IVH. Brain MRI at the TEA has become an important imaging modality to evaluate various findings associated with GM-IVH that overcome the limitations of cUS. Understanding various neuroimaging findings related to GM-IVH in premature infants and using neuroimaging appropriately at an appropriate time will help improve the prognosis of premature infants with GM-IVH.
Footnotes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Informed consent
This type of study does not require informed consent.
Author contributions
Conceptualization : SKY; Project administration : SKY; Writing - original draft : SKY; Writing - review & editing : SKY
Data sharing
None
Preprint
None
References
- 1.Arulkumaran S, Tusor N, Chew A, Falconer S, Kennea N, Nongena P, et al. MRI findings at term-corrected age and neurodevelopmental outcomes in a large cohort of very preterm infants. AJNR Am J Neuroradiol. 2020;41:1509–1516. doi: 10.3174/ajnr.A6666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Brouwer MJ, de Vries LS, Pistorius L, Rademaker KJ, Groenendaal F, Benders MJ. Ultrasound measurements of the lateral ventricles in neonates: why, how and when? A systematic review. Acta Paediatr. 2010;99:1298–1306. doi: 10.1111/j.1651-2227.2010.01830.x. [DOI] [PubMed] [Google Scholar]
- 3.Brouwer MJ, de Vries LS, Groenendaal F, Koopman C, Pistorius LR, Mulder EJ, et al. New reference values for the neonatal cerebral ventricles. Radiology. 2012;262:224–233. doi: 10.1148/radiol.11110334. [DOI] [PubMed] [Google Scholar]
- 4.Camfferman FA, de Goederen R, Govaert P, Dudink J, van Bel F, Pellicer A, et al. Diagnostic and predictive value of Doppler ultrasound for evaluation of the brain circulation in preterm infants: a systematic review. Pediatr Res. 2020;87(Suppl 1):50–58. doi: 10.1038/s41390-020-0777-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cizmeci MN, Khalili N, Claessens NHP, Groenendaal F, Liem KD, Heep A, et al. Assessment of brain injury and brain volumes after posthemorrhagic ventricular dilatation: a nested substudy of the randomized controlled ELVIS trial. J Pediatr. 2019;208:191–197.e2. doi: 10.1016/j.jpeds.2018.12.062. [DOI] [PubMed] [Google Scholar]
- 6.Cizmeci MN, Groenendaal F, Liem KD, van Haastert IC, BenaventeFernández I, van Straaten HLM, et al. Randomized controlled early versus late ventricular intervention study in posthemorrhagic ventricular dilatation: outcome at 2 years. J Pediatr. 2020;226:28–35.e3. doi: 10.1016/j.jpeds.2020.08.014. [DOI] [PubMed] [Google Scholar]
- 7.Çizmeci MN, Akın MA, Özek E. Turkish neonatal society guideline on the diagnosis and management of germinal matrix hemorrhage-intraventricular hemorrhage and related complications. Turk Arch Pediatr. 2021;56:499–512. doi: 10.5152/TurkArchPediatr.2021.21142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Coley BD. Caffey’s pediatric diagnostic imaging E-book, ed 13. Philadelphia: Elsevier - OHCE; 2018. p. 257. [Google Scholar]
- 9.Dorner RA, Burton VJ, Allen MC, Robinson S, Soares BP. Preterm neuroimaging and neurodevelopmental outcome: a focus on intraventricular hemorrhage, post-hemorrhagic hydrocephalus, and associated brain injury. J Perinatol. 2018;38:1431–1443. doi: 10.1038/s41372-018-0209-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.El-Dib M, Limbrick DD, Jr, Inder T, Whitelaw A, Kulkarni AV, Warf B, et al. Management of post-hemorrhagic ventricular dilatation in the infant born preterm. J Pediatr. 2020;226:16–27.e3. doi: 10.1016/j.jpeds.2020.07.079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gaisie G, Roberts MS, Bouldin TW, Scatliff JH. The echogenic ependymal wall in intraventricular hemorrhage: sonographic-pathologic correlation. Pediatr Radiol. 1990;20:297–300. doi: 10.1007/BF02013158. [DOI] [PubMed] [Google Scholar]
- 12.George JM, Fiori S, Fripp J, Pannek K, Bursle J, Moldrich RX, et al. Validation of an MRI brain injury and growth scoring system in very preterm infants scanned at 29- to 35-week postmenstrual age. AJNR Am J Neuroradiol. 2017;38:1435–1442. doi: 10.3174/ajnr.A5191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Guillot M, Chau V, Lemyre B. Routine imaging of the preterm neonatal brain. Paediatr Child Health. 2020;25:249–255. doi: 10.1093/pch/pxaa033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Guillot M, Sebastianski M, Lemyre B. Comparative performance of head ultrasound and MRI in detecting preterm brain injury and predicting outcomes: a systematic review. Acta Paediatr. 2021;110:1425–1432. doi: 10.1111/apa.15670. [DOI] [PubMed] [Google Scholar]
- 15.Hand IL, Shellhaas RA, Milla SS, Committee on Fetus and Newborn, Section on Neurology, Section on Radiology Routine neuroimaging of the preterm brain. Pediatrics. 2020;146:e2020029082. doi: 10.1542/peds.2020-029082. [DOI] [PubMed] [Google Scholar]
- 16.Intrapiromkul J, Northington F, Huisman TA, Izbudak I, Meoded A, Tekes A. Accuracy of head ultrasound for the detection of intracranial hemorrhage in preterm neonates: comparison with brain MRI and susceptibility-weighted imaging. J Neuroradiol. 2013;40:81–88. doi: 10.1016/j.neurad.2012.03.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Jhaveri MD. Diagnostic Imaging: Brain E-Book, ed 4. Philadelphia: Elsevier - OHCE; 2020. pp. 271–274. [Google Scholar]
- 18.Kidokoro H, Neil JJ, Inder TE. New MR imaging assessment tool to define brain abnormalities in very preterm infants at term. AJNR Am J Neuroradiol. 2013;34:2208–2214. doi: 10.3174/ajnr.A3521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Leijser LM, Scott JN, Roychoudhury S, Zein H, Murthy P, Thomas SP, et al. Post-hemorrhagic ventricular dilatation: inter-observer reliability of ventricular size measurements in extremely preterm infants. Pediatr Res. 2021;90:403–410. doi: 10.1038/s41390-020-01245-0. [DOI] [PubMed] [Google Scholar]
- 20.Lowe LH, Bailey Z. State-of-the-art cranial sonography: part 2, pitfalls and variants. AJR Am J Roentgenol. 2011;196:1034–1039. doi: 10.2214/AJR.10.6203. [DOI] [PubMed] [Google Scholar]
- 21.Lowe LH, Bailey Z. State-of-the-art cranial sonography: part 1, modern techniques and image interpretation. AJR Am J Roentgenol. 2011;196:1028–1033. doi: 10.2214/AJR.10.6160. [DOI] [PubMed] [Google Scholar]
- 22.Ment LR, Bada HS, Barnes P, Grant PE, Hirtz D, Papile LA, et al. Practice parameter: neuroimaging of the neonate: report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology. 2002;58:1726–1738. doi: 10.1212/wnl.58.12.1726. [DOI] [PubMed] [Google Scholar]
- 23.Nataraj P, Svojsik M, Sura L, Curry K, Bliznyuk N, Rajderkar D, et al. Comparing head ultrasounds and susceptibility-weighted imaging for the detection of low-grade hemorrhages in preterm infants. J Perinatol. 2021;41:736–742. doi: 10.1038/s41372-020-00890-x. [DOI] [PubMed] [Google Scholar]
- 24.Nongena P, Ederies A, Azzopardi DV, Edwards AD. Confidence in the prediction of neurodevelopmental outcome by cranial ultrasound and MRI in preterm infants. Arch Dis Child Fetal Neonatal Ed. 2010;95:F388–390. doi: 10.1136/adc.2009.168997. [DOI] [PubMed] [Google Scholar]
- 25.Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr. 1978;92:529–534. doi: 10.1016/s0022-3476(78)80282-0. [DOI] [PubMed] [Google Scholar]
- 26.Parodi A, Morana G, Severino MS, Malova M, Natalizia AR, Sannia A, et al. Low-grade intraventricular hemorrhage: is ultrasound good enough? J Matern Fetal Neonatal Med 28 Suppl. 2015;1:2261–2264. doi: 10.3109/14767058.2013.796162. [DOI] [PubMed] [Google Scholar]
- 27.Parodi A, Govaert P, Horsch S, Bravo MC, Ramenghi LA. Cranial ultrasound findings in preterm germinal matrix haemorrhage, sequelae and outcome. Pediatr Res. 2020;87(Suppl 1):13–24. doi: 10.1038/s41390-020-0780-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rees P, Callan C, Chadda KR, Vaal M, Diviney J, Sabti S, et al. Preterm brain injury and neurodevelopmental outcomes: a meta-analysis. Pediatrics. 2022;150:e2022057442. doi: 10.1542/peds.2022-057442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Riedesel EL. Neonatal cranial ultrasound: advanced techniques and image interpretation. J Pediatric Neurology. 2018;16:106–124. [Google Scholar]
- 30.Takashima S, Mito T, Ando Y. Pathogenesis of periventricular white matter hemorrhages in preterm infants. Brain Dev. 1986;8:25–30. doi: 10.1016/s0387-7604(86)80116-4. [DOI] [PubMed] [Google Scholar]
- 31.Valdez Sandoval P, Hernández Rosales P, Quiñones Hernández DG, Chavana Naranjo EA, García Navarro V. Intraventricular hemorrhage and posthemorrhagic hydrocephalus in preterm infants: diagnosis, classification, and treatment options. Childs Nerv Syst. 2019;35:917–927. doi: 10.1007/s00381-019-04127-x. [DOI] [PubMed] [Google Scholar]
- 32.Van’t Hooft J, van der Lee JH, Opmeer BC, Aarnoudse-Moens CS, Leenders AG, Mol BW, et al. Predicting developmental outcomes in premature infants by term equivalent MRI: systematic review and metaanalysis. Syst Rev. 2015;4:71. doi: 10.1186/s13643-015-0058-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Volpe JJ. Volpe’s Neurology of the Newborn, ed 6. Philadelphia: Elsevier; 2018. pp. 637–698. [Google Scholar]