

Abstract
Background
The purpose of this research was to assess the relationship between infection by severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2) containment measures implemented in Mozambique and the spread of SARS-CoV-2 from March 17, 2020, to September 30, 2021.
Materials and Methods
The number of SARS-CoV-2 tests conducted, the positivity rate for SARS-CoV-2, the daily hospitalization due to COVID-19, and the average number of patients hospitalized with COVID-19 each day were all documented in a database, from which the positivity rate and weekly growth rate were calculated. Seven milestones were specified, each corresponding to a critical date in the legal measures linked to confinement and relaxation of measures. To compare SARS-CoV-2 data, three periods were created for each milestone: Period 1 = 15 days before the date of the decree; Period 2 = Date of the decree to the 15th day after; and Period 3 = from the 16th day to the 30th day of the decree date. ANOVA was used to compare the average values for each indicator between the three times for each milestone.
Results
A comparison of all indicators in each milestone’s three periods reveals no consistent significant impact of the measures, regardless of the tendency to lockdown or provide relief.
Conclusion
No relationship was discovered between the legal measures for SARS-CoV-2 pandemic control and the positive rate and growth rates, as well as the number of hospitalized people. Because it was not feasible to determine the degree of efficacy of each specific measure, this conclusion is related to the measures as a whole.
Key words: Africa, SARS-cov-2, covid-19, Mozambique, pandemic
Introduction
The lack of practical and scientific knowledge about the way SARS-COV-2 manifests and spreads led to the adoption of containment measures based on little robust scientific information available to the world.
Following a global trend, the containment measures adopted were more of a generalized practice of hygienic behavior, mask use and social distancing.1 Trying to guarantee that those behaviors become effective, governments around the world have adopted different legal actions that aim to promote social distancing, social gathering, and enforcement to use of facial masks and hygienic practices. Other legal actions included the closing of country borders, closing schools, and stopping cultural and sport events as well as religious acts/festivities. Altogether, those laws had a negative impact on social well-being and the economy, causing a substantial reduction in family income,2-4 and a strong impact on childhood and youth development, among others.5
Finding a balance between the containment needs, with the aim of saving human lives, and the reduction of the negative impact on people’s lives, has been complex and controversial.6
In Mozambique, the containment measures for SARS-CoV-2 have been regulated by the declaration of the State of Emergency (March 30, 2020), and afterward, the State of Calamity,7 both stated by successive legal decrees across time. After 18 months of the first measures, it seems important to evaluate its efficacy, particularly because it is predicted that the coronavirus pandemic will last for a long and unknown time. This evaluation is of particular importance since measures with a high impact on social and economic life may be justified by a positive impact in saving lives or, otherwise, they will have a negative effect without bringing any benefits.8,9 The goal of the present study is to evaluate the association of the coronavirus containment measures adopted in Mozambique with the spread of SARS-CoV-2 between April 1st, 2020, to September 30th, 2021.
Materials and Methods
This evaluation was performed using the daily reports issued by the Ministry of Health of Mozambique. Based on these reports, a database was created using the number of SARS-CoV-2 tests performed, the positivity rate, the daily number of patients hospitalized, and the average number of patients in the hospital in each day.
The positivity rate (the number of SARS-CoV-2 cases diagnosed over a number of SARS-CoV-2 tests performed) and growth rate (the weekly number of SARS-CoV-2 positive cases over the number of cases reported in the previous week) were calculated.
For evaluation purposes, seven milestones corresponding to the crucial dates of the legal actions related to confinement and the relaxation of measures were defined and accordingly described in Table 1.
Assuming a maximum incubation period of 15 days, it will be expected that an efficient measure will have an impact, at least, after the 15th day. Thus, three periods were established to compare COVID-19 data such as: Period 1 = 15 days before the date of the decree; Period 2 = Date of the decree to the 15th day after; Period 3 = from the 16th day to the 30th day of the decree date. Comparison of the average number of positive cases, positivity rate, growth rate and hospitalization were made using ANOVA followed by a Bonferroni test for the evaluation of the differences between periods, of each milestone. The SPSS package (version 25.0) was used, and the value of significance of 0.05 was determined.
Results
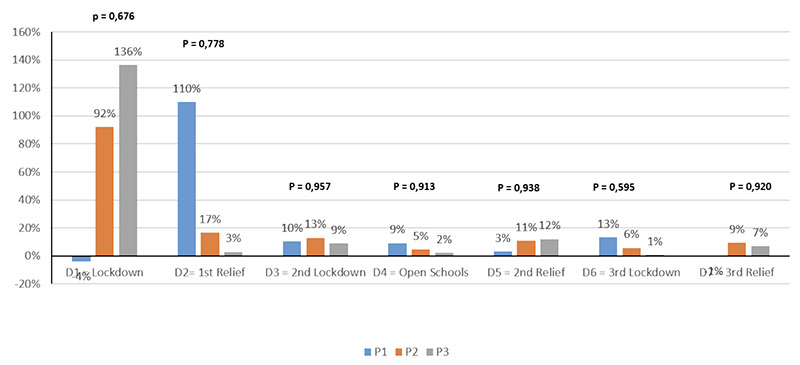
Figure 1 shows the evolution of positive cases, by week, from March 17, 2020, to September 30, 2021. Ascendant lines are situated at the final of the first lockdown, although at a low rate (August 2020), at the final of the first relief phase (December 2020) and at the middle of the 2nd relief phase (June 2021). More relevant descending lines are situated in the middle of the 2nd lockdown (February 2021) and at the beginning of the 3rd lockdown (August 2021). From the last relief phase to the end, the number of cases reduced to almost zero.The comparison between the average numbers of positive cases, between the three periods, for each milestone, is shown in Figure 2. The 3rd period is higher than the second period in milestone 2 (relief) and 3 (lockdown) and lower in 4, 5, and 7 (relief) as well as in 6 (lockdown).
The comparison between positivity rates is distinct from each milestone (Figure 3). There was no significant difference in milestone 1. In milestone 2 (relief), the values increased from period 1 to period 2 and stabilized in period 3. In milestone 3 (lockdown), the values increased from 6.5% to 32.3% from period 1 to 2 and 29.7% from period 2 to 3. At all following relief milestones, positivity rates decreased from period 1 to 3 as well as at milestone 6 (lockdown) from period 2 to 3.
Figure 1.

Evolution of positive cases per week in Mozambique from march 17, 2020, to september 30, 2021 (dash lines indicated dates of main government restrictions/announcements (see Table 1).
Table 1.
Milestones and summary of the content of the legal action.
| Marco | Data | Trend | Main measures |
|---|---|---|---|
| 1 | March 30, 2020 | 1st Lockdown | Shut down of schools, sports events, gyms, cultural and recreational events, online work, and closing of borders |
| 2 | September 4, 2020 | 1st Relief | Reopening of schools, cultural events, individual sports, gyms and borders |
| 3 | January 13, 2021 | 2nd Lockdown | Shut down of schools, sports events, gyms, cultural and recreational events, online work and curfew |
| 4 | March 5, 2021 | Open schools | Reopening of schools |
| 5 | April 26, 2021 | 2nd Relief | Reopening of cultural events, individual sports, gyms and borders |
| 6 | June 16, 2021 | 3rd Lockdown | Shut down of schools, sports events, gyms, cultural and recreational events |
| 7 | August 27, 2021 | 3rd Relief | Reopening of schools, cultural events, individual sports, gyms and borders |
Comparison amongst growth rates does not show any statistical significance (Figure 4). Although differences were high in the two first milestones the absence of statistical significance may be related to the lower absolute value for the number of cases.
The comparison by hospitalization is demonstrated in Figure 5. The average number of hospitalized patients by period was similar and very low at milestone 1, and no different from the 3 periods, regardless of the trend of the legal measures implemented. During milestone 3 (lockdown), the number of cases increased significantly, whilst for milestones 4, 5, and 7 (relief), the number of cases decreased, which was also observed during milestone 6 (lockdown).
Discussion
The present study evaluated the impact of the containment measures on SARS-CoV-2 cases, positivity rates, growth rates and hospitalization because of COVID-19 in Mozambique. The study was based on official data reported by the MoH of Mozambique assuming that any effective measure will have an impact 15 days after it starts, with a reduction in contamination. The evolution of curves and the comparison between the two-week periods around the 7 milestones did not suggest any cause-and-effect relationship.
Using data from 27 countries to verify the efficacy of the official containment measures for SARS-CoV-2, a similar approach was used by others.9 The authors did find that 15 days after the lockdown, daily cases of COVID-19 and the growth factor of the disease showed a declining trend which is different from the one reported in our study. However, although the growth rate declined after 15 days, it remained higher than 1, which means that the measures were not effective in stopping the spread of SARS-CoV-2.
Figure 2.

Comparison between average positive cases between the 3 periods for each milestone; p values resulted from ANOVA.
Figure 3.

Comparison between average positivity rates between the 3 periods for each milestone; p-values resulted from ANOVA.
The search for the efficacy of the measures by the method used in the present study is limited by the fact that the evaluation has been made by looking at the measures without discriminating between each specific measure. Although we did not find a relationship between the measures as a whole and the reduction of the cases and hospitalization, there is no evidence to show what results would have been found if any of those measures had not been taken. Another limitation is that we did not evaluate the compliance degree of the measures since we only considered the law and not its practice.However, other studies have suggested that the number of persons using masks and increasing the washing of hands are significant in Mozambique.4,11 Considering these limitations, there are aspects that must be considered. Firstly, the fact that the January 2021 “wave” followed the great agglomeration and circulation of people that is characteristic of the Christmas and New Year period, with the huge migration of people from South Africa, which leads to large social events and gatherings. However, in June 2021, a higher magnitude “wave”, in a number of new cases reported and deaths has been observed, which is a lower season for events and circulation when compared with the month of January. Some authors have suggested that it could be attributed to the circulation of the Delta variant, which has been classified as more transmissible.12
The second observation is the fact that some lockdown periods show higher incidence rates for all indicators than other relief periods. The comparison between the 3rd periods (3rd and 4thweeks after the decrees) and the first two weeks after de decrees does not suggest any relationship between the measures and the reduction of the indicators. Although it may be recognized thatthere is considerable data error; it is presumable that the dimension error can be negligible when the goal is to determine the evolution across time.
Figure 4.
Comparison between average growth rates between the 3 periods for each milestone; p-values resulted from ANOVA.
Figure 5.

Comparison between the average of daily hospitalized patients between the 3 periods for each milestone; p-values resulted from ANOVA.
Athird relevant finding is that the opening of the schools (milestone 4), which had been closed for a year, did not cause any increase in the number of cases, hospitalization or deaths. In fact, after the reopening of the schools, the numbers decreased for all indicators and only four months later, an increase was observed. Moreover, in months like September to December 2020 andApril to June 2021, when cultural events and recreational and sports activities were allowed, there was a negative impact on the epidemiological frame. The contribution of school closure to the control of the COVID epidemic seems not to be demonstrated. For instance, Vinner et al.5 performed a literature review and did not find any evidence that maintains having schools open will improve the control of the epidemic. Others have claimed that despite the scientific uncertainty about the topic, there is a large spectrum of disadvantages affecting children when schools are open.13-15 Our results do not show any negative effect on the number of cases after schools reopened. To note it is unknown how compliant containment measures rules which impair the estimation of the impact of the real behavior in the variables observed in this study. It is known that virus dissemination tends to be done by waves and therefore, there are periods that are sensitive to a higher transmission rate than others. In these periods, the containment measures are put in place essentially to decrease the transmission rate but not its existence. In this context, measures should be adjusted with the periods where it is known to be susceptible to higher dissemination.
This is even more important when the containment measures affect several aspects of social and economic life, which is the case of the present pandemic measures. Thus, the search for an explanation for the relationship between the measures and the positivity rates, hospitalization and deaths is extremely important.
From our point of view, there are two hypotheses that can guide topics in future research. First, the fact that in urban centers in Mozambique, activities more prone to agglomeration remained intact during the pandemic time observed. Agglomeration in public transport, markets and official meetings did not change across all the periods, a l t h o u g h the use of masks was largely observed. The potential focus of contamination was permanent and with the same characteristics in all seasons. Thus, one can hypothesize the lack of a relationship between the measures and epidemiological results, because the contamination focus was maintained active and similar in all phases.
A second hypothesis relates to the demographic contact with South Africa, where case numbers were much higher but with the same patterns. The standardized pattern of the positive cases from both countries per week plotted against time shows a very similar behavior with a small delay for Mozambique data (Figure 6). Testing those two hypotheses simultaneously could, eventually, bring important information to establish a better balance between the efficacy of the measures and the reduction of social and economic impact of the measures.
Managing the pandemic is very complex and the bases to establish the containment measures are far behind the scope of the present study. However, the high impact of the containment measure requires an evaluation in such a way that one could reduce the collateral effects and increase the prevention, which is particularly important in low-income regions such as African countries.16-19 In a country like Mozambique, where the infrastructures and resources are very limited, creativity and contextualization must be used, instead of mechanical copies of other social cultural and economic realities. The justified fear and the large scope of scientific unfamiliarity about SARS-CoV-2may cause inefficient actions that must be changed according to the practical and theoretical evidence.
Conclusions
Using official data on the SARS-CoV-2 pandemic in Mozambique, a relationship between the legal measures for the control of the pandemic and the evolution of cases, growth rates and hospitalization was not found. This conclusion is related to the measures since it was not possible to determine the degree of efficacy of each specific measure.
Figure 6.

Standardized number of cases per day (z score) of Mozambique and South Africa across all the pandemic time (march 2020 to september 2021).
Acknowledgments
The author would like to thank Jorge Uate for the assistance in the database development, Adriana Jonhson and Godfrey Johnson for editing the manuscript and Dr. Nilesh Batt for the comments.
Funding Statement
Funding: none
References
- 1.Alwan NA, Burgess RA, Ashworth S, et al. Scientific consensus on the COVID-19 pandemic: we need to act now. Lancet 2020;31:e71-e72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chang AY, Cullen MR, Harrington RA, Barry M. The impact of novel coronavirus COVID-19 on non communicable disease patients and health systems: a review. J Intern Med 2021;289:450-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sweeney S, Capeding TPJ, Eggo R, et al. Exploring equity in health and poverty impacts of control measures for SARSCoV- 2 in six countries. BMJ Glob Health 2021;6:e005521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Prista A, Damasceno A, Lauchande C, et al. Compliance and impact of Mozambican state of emergency on covid-19 containment measures: a cross-sectional study in an urban setting. S Afr J Res Sport Educ Recreat 2022;43:31-48. [Google Scholar]
- 5.Viner RM, Russell SJ, Croker H, et al. School closure and management practices during coronavirus outbreaks including COVID-19: a rapid systematic review. Lancet Child Adolesc Health 2020:4:397-404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Haider N, Osman AY, Gadzekpo A, et al. Lockdown measures in response to COVID-19 in nine sub-Saharan African countries. BMJ Glob Health 2020;5:e003319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Conselho de Ministros de Moçambique. Decreto Presidencial nº11/2020. Boletim da Republica Série I, 62, Março 30 2020. Available from: https://www.portaldogoverno.gov.mz/por/Declaracao-do-Estado-de-Emergencia [Google Scholar]
- 8.Mboera LEG, Akipede GO, Banerjee A, et al. Mitigating lockdown challenges in response to COVID-19 in Sub-Saharan Africa. Int J Infect Dis 2020;96:308-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Egger EM, Jones S, Justino P, et al. Africa’s lockdown dilemma High poverty and low trust. In: University UN, editor 2020. Available from: https://www.wider.unu.edu/publication/africa%E2%80%99s-lockdown-dilemma [Google Scholar]
- 10.Meo SA, Abukhalaf AA, Alomar AA, et al. Impact of lockdown on COVID-19 prevalence and mortality during 2020 pandemic: observational analysis of 27 countries. Eur J Med Res 2020;10;25:56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Júnior A, Dula J, Mahumane S, et al. Adherence to COVID-19 Preventive Measures in Mozambique: Two Consecutive Online Surveys. Int J Environ Res Public Health 2021;26;18:1091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Al-Beltagi S, Goulding LV, Chang DKE, et al. Emergent SARS-CoV-2 variants: comparative replication dynamics and high sensitivity to thapsigargin. Virulence 2021;12:2946-2956. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ziauddeen N, Woods-Townsend K, Saxena S, et al. Schools and COVID-19: Reopening Pandora's box? Public Health Pract (Oxf) 2020;1:100039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Viner R, Russell S, Saulle R, et al. School Closures During Social Lockdown and Mental Health, Health Behaviors, and Well-being Among Children and Adolescents During the First COVID-19 Wave: A Systematic Review. JAMA Pediatr 2022;18. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 15.Calear AL, McCallum S, Morse AR, et al. Psychosocial impacts of home-schooling on parents and caregivers during the COVID-19 pandemic. BMC Public Health 2022;17;22:119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Renzaho AMN. The Need for the Right Socio-Economic and Cultural Fit in the COVID-19 Response in Sub-Saharan Africa: Examining Demographic, Economic Political, Health, and Socio-Cultural Differentials in COVID-19 Morbidity and Mortality. Int J Environ Res Public Health 2020;15;17:3445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Dzobo M, Chitungo I, Dzinamarira T. COVID-19: a perspective for lifting lockdown in Zimbabwe. Pan African Medical Journal 2020;35:13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Coetzee BJ, Kagee A. Structural barriers to adhering to health behaviours in the context of the COVID-19 crisis: Considerations for low- and middle-income countries. Global Public Health 2020;20:1-10. [DOI] [PubMed] [Google Scholar]
- 19.Buonsenso D, Cinicola B, Raffaelli F, et al. Social consequences of COVID-19 in a low resource setting in Sierra Leone, West Africa. Int J Infect Dis 2020;9712:30411-2. [DOI] [PMC free article] [PubMed] [Google Scholar]