

Screening for adverse childhood and adult experiences in prenatal care allows clinicians to address past and present adversity and trauma, with a goal of improving perinatal outcomes.
Abstract
Adverse childhood and adult experiences can affect health outcomes throughout life and across generations. The perinatal period offers a critical opportunity for obstetric clinicians to partner with patients to provide support and improve outcomes. This article draws on stakeholder input, expert opinion, and available evidence to provide recommendations for obstetric clinicians' inquiry about and response to pregnant patients' past and present adversity and trauma during prenatal care encounters. Trauma-informed care is a universal intervention that can proactively address adversity and trauma and support healing, even if a patient does not explicitly disclose past or present adversity. Inquiry about past and present adversity and trauma provides an avenue to offer support and to create individualized care plans. Preparatory steps to adopting a trauma-informed approach to prenatal care include initiating education and training for practice staff, prioritizing addressing racism and health disparities, and establishing patient safety and trust. Inquiry about adversity and trauma, as well as resilience factors, can be implemented gradually over time through open-ended questions, structured survey measures, or a combination of both techniques. A range of evidence-based educational resources, prevention and intervention programs, and community-based initiatives can be included within individualized care plans to improve perinatal health outcomes. These practices will be further developed and improved by increased clinical training and research, as well as through broad adoption of a trauma-informed approach and collaboration across specialty areas.
It is well established that “childhood adversity casts a long shadow.”1 The landmark 1998 ACEs (Adverse Childhood Experiences) study2 demonstrated ways in which childhood experiences of abuse, neglect, and vulnerabilities such as parental substance misuse or mental illness may be associated with adverse physical and mental health outcomes throughout life. Large-scale efforts to translate scientific understanding of links between early adversity and health outcomes3,4 into trauma-informed clinical care are underway.5–7 Aligned with these efforts, the American College of Obstetricians and Gynecologists has recommended that obstetrician–gynecologists adopt a trauma-informed approach across all levels of practice, including routine screening for past and present trauma.8
Trauma is defined as an event or series of events experienced as life threatening or overwhelming with lasting physical, psychological, social, emotional, or spiritual effects.6 Trauma is common, with more than 70% of respondents in multiple samples reporting at least one traumatic event in their lifetime.9 Although adversity and trauma affect people across racial, ethnic, and socioeconomic classes, Black individuals, Indigenous people, people of color, and individuals living in low-income communities face a disproportionately high exposure to trauma compared with those who are White or economically advantaged.10,11 In addition, trauma has an intergenerational pattern, with biological effects and increased susceptibility to mental health conditions observed among children of trauma-exposed individuals.12 Trauma-informed care is a strengths-based model of care delivery that incorporates an understanding of how trauma affects people in routine clinical practice.6 It is a universal intervention that can proactively address trauma and support healing, even if a patient does not explicitly disclose past or present adversity.
Pregnancy is a pivotal time in the lives of people who have experienced early adversity and trauma. It is a time characterized by increased medical and psychosocial risk,13 as well as greater engagement with health care,11,14 greater motivation for health behavior change,15,16 and increased plasticity of both the maternal and fetal brain.17–20 Obstetric clinicians routinely address challenging and complex psychosocial and medical situations that may result from or be influenced by trauma. By practicing trauma-informed care, clinicians may significantly reduce patient fear and distress and improve their counseling effectiveness and patient adherence to clinical recommendations.21
Existing data indicate that screening for ACEs in prenatal care is feasible and acceptable to patients and results in improved patient–clinician relationships.22 Although obstetrics and gynecology residents believe in the importance of assessing and addressing their patients' histories of trauma, abuse, and interpersonal violence, most feel unprepared and insufficiently trained to effectively evaluate and manage this aspect of prenatal care.23 Education about trauma-informed care can increase clinicians' knowledge of, attitudes about, and confidence in providing psychosocial support,24 which may also improve their job satisfaction and reduce their risk for burnout.25
Although universal screening for past and present trauma in prenatal care is recommended and is increasingly being implemented,26 there is a paucity of research to guide clinicians on how to implement these recommendations.27 The objectives of this article are to provide an overview of fundamental trauma-informed care concepts and to recommend practices informed by available evidence and stakeholder input, tailored to obstetric clinicians interested in inquiring about and responding to adverse childhood and adult experiences in prenatal encounters.
METHODOLOGY
This project was undertaken as a collaborative effort by the California Maternal Quality Care Collaborative and key stakeholders. The California Maternal Quality Care Collaborative identified and engaged 17 key stakeholders from the American College of Obstetricians and Gynecologists and other professional organizations (n=6), academic institutions (n=2), obstetric and pediatric settings (n=2; including professionals serving perinatal populations with the highest rates of maternal and infant death, morbidity, and adversity), and government (n=4) and community members representing individuals with lived experience of childhood adversity (n=3).28 Stakeholders met frequently as a group over 5 months to review concepts and emerging practices for addressing past and present adversity, trauma, and resilience in prenatal care. The group considered scientific evidence; patient, clinician, and researcher perspectives; standards of obstetric and perinatal care; multiple practice models; and practical, feasible steps toward implementation of practice change. Using a consensus-based approach, we developed a set of recommendations for obstetric clinicians to guide inquiry about and response to adversity, trauma, and resilience in prenatal care. In addition to key stakeholder input, comprehensive review and feedback were provided by an external expert review panel including 15 clinician and research leaders. Concurrently, a scoping review following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) extension guidelines for scoping reviews29 was carried out to critically appraise the evidence on associations between adverse childhood experiences identified during pregnancy and maternal perinatal and neonatal health outcomes. Although the findings informed recommendations, this review is being published separately, and the protocol has been made available through the Open Science Framework at https://osf.io/hbrz7 (registration DOI: https://doi.org/10.17605/OSF.IO/HBRZ7).
BASIC PRINCIPLES FOR A TRAUMA-INFORMED APPROACH
The goals of trauma-informed care are to realize and recognize the effects of trauma, respond with support and pathways for healing, and resist retraumatization. Fundamental to this is an understanding of how adversity and trauma manifest in prenatal care. Among pregnant patients, past and present adversities may interact and have cumulative effects, contributing to stress-related pathology (Fig. 1).10,30–42 Early exposure to sexual abuse, for example, is associated with increased risk of experiencing sexual assault and intimate partner violence in adulthood, each of which has been associated with adverse birth outcomes.38,39 Early adversity is also associated with an increased risk of health conditions that heighten susceptibility to adverse perinatal outcomes such as obesity, hypertension, and diabetes.2,36
Fig. 1. Personal life course: web of stresses. Adverse childhood experiences interact with other sources of personal stress that can cumulatively affect perinatal and infant outcomes.
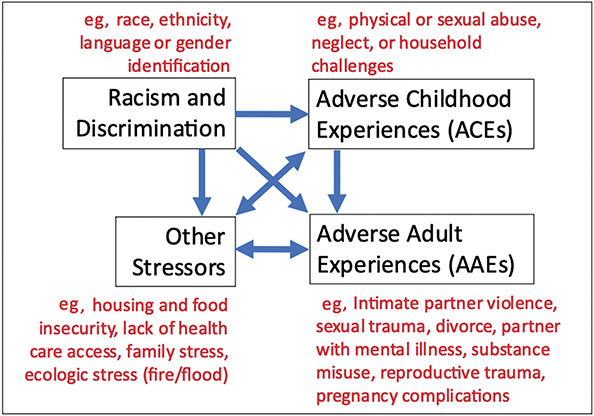
Johnson. Adverse Childhood and Adult Experiences. Obstet Gynecol 2023.
It is important to note that adversity does not always result in pathology. Responses to stressors can be conceptualized on a continuum, from positive to tolerable to toxic. A toxic stress response4 can occur when strong, frequent, or prolonged adversity (eg, physical, emotional or sexual abuse, chronic neglect or caregiver mental illness, accumulated burdens of racism, discrimination, or economic hardship) is experienced without adequate support. Prolonged activation of biological stress response systems can disrupt the development of brain architecture and other physiological processes, as well as behavioral and psychological adaptation, and increase the risk of stress-related disease and neurocognitive impairment well into adulthood.43 Whether biological changes resulting from stress are toxic or adaptive depends on a range of individual and environmental factors.4,13 Weathering is a construct that emerged from observations of racial disparities in perinatal outcomes and refers to the cumulative effects of long-term stress exposure (eg, racism, political marginalization, economic hardship) contributing to early and ongoing health deterioration, including adverse pregnancy and birth outcomes.44,45 Although toxic stress highlights the disruption of early developmental trajectories and weathering focuses on premature health deterioration, both constructs place emphasis on the biological embedding of lived experiences contributing to adverse health outcomes (Table 1).
Table 1.
Key Terms and Definitions

Understanding how past and present experiences and socioecologic contexts affect biology, psychology, and behavior can reduce stigma associated with conditions often attributed to poor individual choices (eg, obesity, substance misuse) and inform more effective recommendations. Through this lens, nonadherence to clinical recommendations, rather than being a personal shortcoming, may derive from a lack of basic resources, such as transportation or health insurance, or symptoms of posttraumatic stress, such as avoidance, which can affect one's ability to attend appointments. In the perinatal period, resilience and protective factors, such as early positive experiences, social support, psychotherapy, and healthy coping skills, can moderate the effects of stress and adversity on health outcomes.46,47 Multidimensional approaches to fostering resilience and wellbeing in adulthood, such as compassionately underscoring the importance of healthy relationships, regular physical activity, good nutrition, adequate sleep, experiences in nature, and access to timely, evidence-based mental health care when needed, may be especially helpful to patients who have experienced adversity and trauma3,48 (Fig. 2).
Fig. 2. Relationship of life stresses and adverse perinatal and infant outcomes. The cumulative effect of life stresses can directly or indirectly lead to weathering, chronic stress, and adverse pregnancy outcomes with at least three points for mitigation. ACEs, adverse childhood experiences; AAEs, adverse adult experiences.
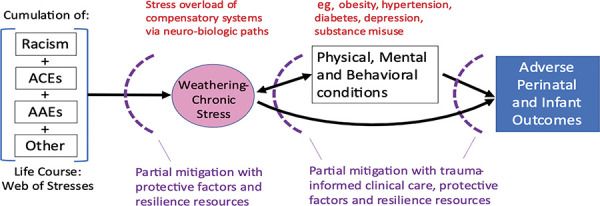
Johnson. Adverse Childhood and Adult Experiences. Obstet Gynecol 2023.
A Trauma-Informed Approach to Prenatal Care
A trauma-informed approach emphasizes patient choice and empowerment, creates a safe environment for discussion of traumatic experiences and effects on health behavior, is nonjudgmental and supportive, emphasizes strengths and resilience, and is sensitive to triggers that may lead to retraumatization.21 Core principles include safety, trustworthiness, transparency, collaboration, peer support, cultural humility and responsiveness, and empowerment (Table 2). Trauma-informed care seeks a fundamental shift away from a focus on pathology (eg, “What's wrong with you?”) to a focus on events, experiences, and effects (eg, “What happened to you?”). Asking “What helps?” enables a focus on strengths and resilience.
Table 2.
Components of Trauma-Informed Care and Prenatal Practice Examples

For patients with a trauma history, aspects of the experience of pregnancy and prenatal care, labor and birth, breastfeeding, and infant care may be empowering, feel challenging, or evoke reminders of past trauma. Experiences of childbirth, for example, can remind patients with a history of childhood maltreatment of previous experiences of loss of control and may serve as a catalyst to re-experiencing abuse or dissociation.49,50 Reminders of past trauma may also arise from power imbalances inherent in the doctor–patient relationship, as well as abdominal or pelvic examinations,51 pelvic pain,49 breastfeeding,52 or infant crying.53 In one study of adolescent mothers who had experienced childhood trauma, 65% reported experiencing triggers of past trauma during pregnancy and postpartum.51 In addition to having an opportunity to discuss past trauma, patients with a history of childhood adversity have identified continuity of care and clinicians (so as to not have to retell their story multiple times) and integrated mental health services54 as elements that enhance trust in and improve experiences of perinatal care.51
Engaging Patients in Conversations About Past and Present Trauma, Adversity, and Resilience
Prenatal patients' interest in discussing experiences of adversity and trauma with prenatal clinicians is well documented.55–57 Flanagan et al22 showed that most prenatal patients (85%) strongly or somewhat strongly agreed that clinicians should ask their prenatal patients about ACEs, and 91% were comfortable discussing ACEs with their clinician. The purpose of inquiry is to identify patients who have experienced adversity and trauma and to respond with support and an appropriate plan for care. Although the optimal mode of screening and the optimal clinical response have not been established, the following best practices informed by available evidence, stakeholder perspectives, and prenatal care standards will help with developing an initial approach to inquiry and response.
HOW TO PREPARE THE PRENATAL PRACTICE
Form a Team and Engage Leadership
At an organizational or clinical practice level, trauma-informed care involves recognizing the effects that trauma has on both prenatal patients and staff. Steps for practice participation include the following:
Identify a prenatal practice champion. How to start and whom to engage can look different across different settings. Smaller practices may begin with a single champion. In larger practices, a small team of clinicians and staff may work together to engage leadership and peers. Regardless of the size of the practice, building support within the practice is critical to success.
Engage clinical leadership and key decision makers within the practice. Having the support of leadership and key decision makers within the practice is important to ensuring successful and sustainable change. Crafting a plan that empowers staff to be part of the transformation process can help generate buy-in throughout the practice. Leadership will need to establish strategies for implementing the changes and clearly communicate the rationale and benefits to both patients and staff.
Engage clinicians and staff within the practice, and provide opportunities to learn about trauma-informed care and how trauma can affect individuals, families, groups, organizations, and communities.
Form an implementation team to develop key processes, procedures, roles and responsibilities, and a timeline with milestones. Depending on the practice setting, the team could include representation from clinicians (eg, obstetricians, nurses, medical assistants, midwives, psychologists, psychiatrists, social workers, peer support specialists), practice administration (eg, office manager, senior leadership, administrative staff, front desk staff, information technology), community-based services (eg, leaders of community-based organizations, social services, early intervention services, faith-based organizations, government programs), and patients. Larger practices may form a patient advisory board; smaller practices may invite a few patients to represent the patient voice. Examples of toolkits addressing practice change include the ACEs Aware implementation toolkit (https://acesaware.org/implement-screening/), the National Health Resource Center on Domestic Violence practice preparation toolkit (http://ipvhealth.org/health-professionals/), and the library of resources offered by the Trauma-Informed Care Implementation Resource Center (https://traumainformedcare.chcs.org/resources-for-becoming-trauma-informed/).
Initiate Education and Training for Clinicians and Staff
Training in trauma-informed care will ideally occur for all clinicians and staff and is essential for anyone involved in the screening process. For obstetrics and gynecology residents, recent data indicate that the most useful elements of didactic training for assessing trauma history in pregnancy are demonstration and practice of interview skills using simulation or role play.58 In this study, which includes a freely available training and role-play module, basic skills in empathic communication were found to be useful but not essential. Another freely available option for trauma-informed care training is the ACEs Aware core curriculum (https://training.acesaware.org).
Support Clinician and Staff Wellbeing
Clinicians and staff may experience traumatic stress in the context of addressing patients' trauma attributable to vicarious trauma (eg, stress related to hearing patients' stories) or reminders of past personal adverse experiences.58 Providing obstetric care can itself be a source of traumatic stress.59,60 Leaders can normalize and validate these experiences and encourage clinicians and staff to seek support through confidential employee assistance programs, psychologists and other mental health professionals, or peer support and community-based programs. Organizational culture, policies, and practices that embrace the principles of trauma-informed care can support clinician and staff wellbeing and minimize retraumatization.61 The Adult Resilience Curriculum, available through the Mental Health Technology Transfer Center Network, is a 10-module training for implementing practices that support staff wellbeing at the individual and organizational level (https://mhttcnetwork.org/centers/mid-america-mhttc/professional-well-being).
Prepare a List of Available Resources and Referral Options
Begin to develop a list of support services and interventions available to perinatal patients to prevent and treat high levels of stress or distress, to support healthy coping and resilience, and to foster positive relationships. What is recommended to patients will depend on the resources in the clinical setting and the community. This process may take some time and effort and include outreach to and partnering with community-based organizations in the network of care. The local county maternal and child health personnel may be of assistance in the preparation of local resources (Table 3).
Table 3.
Example Resources and Community-Based Programs*

Prioritize Education and Training Addressing Racism and Discrimination
Addressing racism, discrimination, and health disparities is a priority in obstetrics and gynecology62 and an essential component of a trauma-informed approach.63 Engaging in ongoing training on unconscious bias and employing more clinicians and staff who come from diverse backgrounds and reflect the community being served can begin to address the warranted mistrust of the medical system commonly reported by marginalized birthing people.
Gradually Implement Inquiry About or Screening for Past and Present Adversity and Trauma
Ensure safety and transparency. Screening for past and present adversity and trauma should always be conducted in private, and participation should be optional. It may be useful to provide information about screening before the visit so that patients are informed and can decide whether to bring a friend, family member, or other supportive person.
.Include resilience. When screening for adversity and trauma, we strongly recommend also inquiring about strengths and resilience. A strengths-based approach acknowledges the importance of protective factors in determining health outcomes57,58 and is favored by patients.49 During our engagement with key stakeholders, many expressed concerns about the term resilience, perceived as potentially making patients, especially Black birthing people, feel that they were required to personally overcome burdens resulting from long-standing structural inequities. A list of screening tools to assess resilience and strengths is provided in Appendix 1, available online at http://links.lww.com/AOG/D156.
Use open-ended questions, structured survey measures, or both. There is no one established way to screen for adversity, trauma, strengths, and resilience in the prenatal setting.47 Box 1 provides examples of open-ended questions informed by scientific evidence, clinical experience, and stakeholder engagement. These questions are designed to guide conversations about experiences of resilience, stress, and trauma.
Box 1. Sample Questions to Engage Prenatal Patients in Conversations About Resilience, Stress, and Trauma*.
Sample questions to engage prenatal patients in conversation about stress, adversity, and trauma
1. What is going well right now?
To frame the conversation in patients' strengths
2. What things worry you about this pregnancy?
To assess obstetric stressors
3. What are stressful, overwhelming, or scary things that are affecting you now?
To assess present traumatic experiences
4. What are the stressful, overwhelming, or scary things from your past that are still affecting you?
To assess past traumatic experiences
5. If in the future you would like to share concerns or experiences with me or our staff, we are available.
To acknowledge that it can take time, trust, and a sense of safety before patients are able to share experiences of adversity or trauma, and to indicate that this is an ongoing conversation with health care professionals who are willing to meet patients where they are
Sample questions to engage prenatal patients in conversation about experiences of resilience
1. What helps you cope with stress and feelings of being overwhelmed?
To assess coping skills as a source of resilience
2. Are there people you can turn to for help?
To assess support as a source of resilience
3. What can I offer you? You may not know what would be helpful now. We can explore this together. Our practice has a list of supports and resources you might like to consider.
To ensure that clinical responses are patient centered and offer patient choice and opportunities for empowerment
4. I see you are having a hard time. What has helped you overcome challenges in the past?
To elicit strengths and supports from the past that may be applied to the present
A list of structured screening tools used to screen for childhood and adult adverse experiences is provided in Appendix 2, available online at http://links.lww.com/AOG/D156. The 10-item ACEs Questionnaire2,64 is one option for screening for childhood adversity and is increasingly being used in pediatric and adult health care settings.65,66 The ACEs Questionnaire can be completed in identified or deidentified formats, and language translations are available. The total score indicates the number of ACEs an individual has experienced. There is no validated cutoff score, and assessment of ACEs alone does not indicate whether a person is experiencing high levels of stress or distress; however, attending to the type of ACEs experienced may be important in informing the clinician's approach to the patient.46,67 In California, the ACEs Aware initiative has trained more than 20,000 health care professionals in screening for ACEs, and more than 700,000 total screenings have been carried out with the ACEs Questionnaire,26 with reimbursement provided by Medicaid. Limitations of the ACEs Questionnaire include the limited types of adversity assessed and the lack of psychometric data, including measures of reliability and validity,68 indicating a need for continued research.
Position Screening for Adversity and Trauma as an Extension of Current Screening
Screening for adversity, trauma, and resilience aligns with other sensitive screenings that are part of standard prenatal care, such as screening for intimate partner violence,69 substance misuse, 70 depression,71 and social determinants of health.72 These related workflows can be integrated and aligned, and screening for adversity, trauma, and resilience can occur at any time during pregnancy. An appropriate time may be at a visit when trust had been established and the demands of entry into care have been met (eg, at approximately 18–20 weeks of gestation).22
Document Findings
When documenting screening findings, there must be a balance between patient privacy and the need to communicate across settings and health care professionals, including coordination with primary care practitioners. It is essential to communicate relevant information, such as a birth plan made in response to a patient's experiences of adversity and trauma, to the birth team. Limiting the description to a general, headline approach can protect patient privacy and limit secondary (or vicarious) trauma for health care professionals reading the description.
Prepare Yourself
The “4 Cs” from Kimberg and Wheeler73 are techniques that health care professionals can embrace to successfully adopt trauma-informed care (Box 2).
Box 2. The “4 Cs”: Techniques for Health Care Professionals to Use When Adopting Trauma-Informed Care.
• Be calm. Pay attention to how you are feeling when you are caring for the patient. Breathe deeply and calm yourself to model and promote calmness for the patient, yourself, and your coworkers.
• Contain the interaction. Limit trauma history detail to maintain psychological and physical safety. Consider asking for “headlines” as opposed to a detailed narrative about traumatic experiences. For example: “You don't have to share details if you don't want to. Just saying, ‘I have a history of [whatever happened, for example sexual abuse as a child]’ is good enough. It may also help to describe your experience of the event and how it affects you. An example is, ‘at the time I felt ___, and now I need help with ___.’”
• Care for the patient and yourself. Self-care and compassion, for both the patient and you, are vitally important. This can include cultivating supportive relationships, engaging in regular physical activity, good nutrition, adequate sleep, meditation and mindfulness practice, experiencing nature, and professional mental health care when needed.
• Focus on coping. Emphasize healthy coping skills, positive and supportive relationships, and interventions that foster psychological well-being and resilience.
Data from Raja S, Hasnain M, Hoersch M, Gove-Yin S, Rajagopalan C. Trauma informed care in medicine: current knowledge and future research directions. Fam Community Health 2015;38:216–26. doi: 10.1097/FCH.0000000000000071
HEALTH CARE PROFESSIONAL RESPONSE TO DISCLOSURE OF ADVERSITY AND TRAUMA
Engage Patients in an Ongoing Conversation With a Focus on Building Trust
Responding to disclosures of adversity and trauma with acknowledgement and active listening is a vital next step. Using statements such as, “I appreciate your sharing this,” or “You have been through some very difficult experiences, and I want you to know that we are going to keep this in mind as we provide care…” can be highly effective in conveying compassion and understanding. Physicians may feel uncomfortable expressing empathy and may feel that a focus on emotional support could interfere with the primary role of providing obstetric information74; however, acknowledging and addressing patient distress may lower emotional and physiologic responses to stress and, in turn, improve information processing and later recall.75 Emotionally distressed patients retain only 20–60% of information provided in medical visits.76
Studies examining physician–patient interactions indicate that directly and sensitively acknowledging patients' emotional responses, encouraging questions and shared decision making, and demonstrating compassion and dependability are associated with greater patient satisfaction and perceived quality of care77–81 and better psychological adjustment. Consistent with this approach, many patients may be interested in learning about how adversity and traumatic stress can affect health and the ways in which healing is possible throughout life,57 and health professionals working in the prenatal care setting are well suited to provide this information. These conversations can shed light on conditions not previously connected to past events and experiences, opening new avenues for understanding, healing, and support.82 Moreover, a trusting patient–clinician relationship can itself provide a source of healing.
Assess Physical and Psychological Safety
An immediate priority is assessing the patient's physical and psychological safety. As is standard prenatal care practice, this includes assessing current exposure to intimate partner violence and risk of self-harm or harm to others and offering appropriate, culturally sensitive referral to support services and resources. This may include providing a warm handover to a mental health professional or community-based service or case management for those with more complex needs.
Assess Basic Needs and Engage Patients in Determining Their Own Starting Point
Depending on past and present experiences and current circumstances, a patient may initially prioritize addressing food insecurity, for example, over previous intimate partner violence. Meeting and supporting the patient where they are, without judgment, is most likely to yield the greatest benefit. Strengths-based tools, such as motivational interviewing, which is a guiding style of communication that sits between listening and providing information and advice,83 can help align patient priorities, preferences, capacities, and strengths with healthy behaviors.
Create a Prenatal Plan
After offering an empathic response and providing evidence-based information, the clinician can then move to a conversation about current needs and available resources to support the patient. Even when time is limited, clinicians can provide a list of services and resources with personalized recommendations highlighted, and these can be discussed further or in more detail at a future visit. In a study adopting this approach, most patients used at least one resource from the list provided.57 Available resources will vary according to practice setting. Drawing on spirituality, faith, religion, and culture82,84; reading; meditation; physical activity84; peer support85; and service to others84 are strategies that pregnant patients who have experienced early adversity describe as helpful in healing. Case examples are provided in Appendix 3, available online at http://links.lww.com/AOG/D156.
Promote Social Support
Social support during pregnancy, including both instrumental (practical) and emotional support, is strongly associated with greater psychological health and wellbeing86–88 and more positive parent–infant interactions89 among individuals with and without a history of childhood adversity.90,91 Social support can be provided by a partner,92,93 family members, friends, and the broader community, as well as by models of group-based prenatal care and by home visiting programs such as Nurse Family Partnership94 and Healthy Families America. Patients may also be interested in referrals to services such as Black Infant Health; home visiting programs; fatherhood programs; community-based groups such as prenatal support groups led by psychologists, social workers, or therapists; birth preparation classes; or informal parent groups.
Provide Referral to Prevent or Treat Mental Health Conditions
Mental health conditions are more prevalent among prenatal patients who have experienced childhood maltreatment, and early intervention and treatment offer an important opportunity to improve both parent and child health,95,96 to support the developing parent–infant bond, and to interrupt intergenerational patterns of trauma and adversity.95 Psychotherapy has been shown to be superior to psychopharmacotherapy alone97 and is especially important to consider given that many patients do not find medication to be acceptable during the perinatal period. For patients experiencing perinatal depression in the context of a history of childhood trauma, interpersonal psychotherapy and cognitive behavioral therapy have demonstrated efficacy in reducing depressive symptoms.95 It is important to note that many interventions such as cognitive behavioral therapy and interpersonal psychotherapy, which have a strong evidence base for anxiety and depression reduction among White pregnant people in the United States,98–101 do not show similar benefit for populations of Black people, Indigenous individuals, or people of color.102 Integrated mental health services, embedded within prenatal care, are optimal but may not always be available. Mental health professionals and other resources such as perinatal depression support groups may be identified through county mental health services, health insurance plans, hospitals, websites, and community-based organizations.
Adopt a Holistic Approach
In addition to professional mental health care and social support, a holistic approach including balanced nutrition,103,104 physical activity and exercise,105,106 restorative sleep,107 and relaxation and meditation108 may provide benefit for perinatal health outcomes and may be especially useful for pregnant patients who are reluctant to engage in mental health care11 or psychopharmacotherapies.109 Prior miscarriage,110 sexual assault,111 or living in an unsafe neighborhood,112 for example, may influence whether and how a patient wants to exercise. Asking strengths-based questions such as, “What kind of movement do you enjoy?” or “What helps you feel calm and relaxed?” may help identify a starting point. In collaboration with their patients, clinicians can also provide personalized “prescriptions” for exercise, outdoor activities, or evidence-based websites or applications (apps) (eg, https://calm.com, https://headspace.com, https://www.mindthebump.org.au, https://mumspace.com.au).
Address Birth-Related Needs
Clinicians working with patients who have experienced trauma can avoid retraumatization in predictable situations such as vaginal examinations88,113 and support planning for labor and delivery,114 including offering birth preparation classes and nonpharmacologic methods for coping during labor.115 Continuous one-to-one emotional support before, during, and after birth from doulas or nonclinical labor support professionals is associated with improved outcomes116 and has been found to be especially important for birthing individuals who are Black, Indigenous, or people of color. Having a birth plan can enable a greater sense of autonomy and control during labor.117 A qualitative meta-synthesis identified a need for control, difficulties with disclosure, dissociation, a discomfort with vulnerability, and wanting to maintain hope for healing as common themes for patients with a history of childhood sexual abuse as they engaged in birth planning.113
Create a Postpartum Plan
Robust postpartum care is increasingly recognized as key for optimizing short- and longer-term parent and child outcomes, as well as outcomes in subsequent pregnancies and lifelong health.43,118 Coordination with primary care practitioners is needed to continue treatment planning and to address traumatic stress (including potential posttraumatic stress symptoms), chronic conditions, and persistent health risks. Coordination with the pediatric health care professional, perinatal and infant mental health services, referral to parenting classes and support groups, lactation support, and home visiting programs that are dyadic and attachment focused can promote healing and support both generations.
DISCUSSION AND CALL TO ACTION
Given the medical focus of obstetric training and the myriad demands of prenatal care, addressing adversity, trauma, and resilience may seem daunting to clinicians, but doing so can help address a root cause of many conditions we treat and improve our patients' experience of care at a critical moment in their lives. In this article, we offer an initial approach to support obstetric clinicians and staff to address past and present stress, adversity, and trauma in outpatient prenatal encounters to improve perinatal outcomes (Box 3). Patient–clinician conversations that offer active listening, compassion, and information can form part of the healing process. In partnership with patients, obstetric clinicians can draw on existing resources to offer social support and mental health services and to develop care plans with options to promote wellbeing and address pregnancy, birth, and postpartum needs. These practices can be adopted gradually over time as an extension of current screenings and models of care and can be strengthened, expanded, and refined through experience, research, and expanded resources and networks of care.
Box 3. Initial Recommendations for Prenatal Clinicians, Staff, and Researchers.
Initial recommendations for prenatal clinicians and staff
• Engage practice leadership and identify “champions” of trauma-informed care.
• Initiate education and training for health care professionals and staff.
• Prepare a list of available resources and referral options.
• Incrementally implement inquiry about or screening for past and present adversity and trauma, as well as resilience.
• Prepare yourself, taking the “4 Cs” approach.
• Create a holistic plan in partnership with the patient, linking with hospital, primary care, and other health care professionals as necessary.
Initial recommendations for researchers
• In partnership with perinatal patients, identify the most important ACEs to assess.
• Determine optimal way(s) to assess ACEs and resilience factors in prenatal settings, taking individual, environmental, and perinatal health equity factors into consideration.
• Test the efficacy and acceptability of psychological, mind–body, and complementary therapies on several domains of distress (eg, depression, posttraumatic stress disorder, anxiety, somatization) among diverse perinatal samples. Test for moderation of outcomes by sociodemographic and cultural factors.
• Examine how the effects of ACEs change over the life course. Are there predictable trajectories? Can these be modified to improve outcomes?
• Investigate which models of care are likely to yield the greatest benefit for patients with past or present adversity and trauma.
• Assess how ACEs screening may improve perinatal and infant health outcomes.
• Examine whether interventions to improve health behaviors (eg, sleep, physical activity, exercise, nutrition, meditation, mindfulness practice) improve perinatal outcomes.
• Identify optimal strategies for the codesign of ACEs screening measures and implementation practices. Are new measures needed?
ACEs, adverse childhood experiences.
Further research is needed to refine screening measures for use in prenatal settings, ensuring the inclusion of a broader range of potential adversities and the use of accessible and nonstigmatizing language. Studies of trauma screening protocols in primary care have evaluated effects on patient attendance, engagement with referrals, health outcomes, and long-term patient–clinician relationships119; similar metrics can be considered in the evaluation of screening in prenatal care and will be increasingly feasible given large-scale efforts to adopt universal screening in clinical settings such as the ACEs Aware initiative in California.120 To strengthen the clinical response, trauma-specific perinatal interventions of various formats must be further developed, researched for effectiveness, and made more broadly available.117
Optimal perinatal care involves collaboration across settings and medical specialties. Further training in a trauma-informed approach is needed for all clinicians and staff in perinatal settings, including hospitals and private practices. Development of a tailored toolkit could offer additional background and training in the perinatal and interpregnancy periods to identify and address the effects of adversity. Navigating perinatal care resources can be challenging, especially for patients who are Black, Indigenous, or people of color.53,121 Public health personnel such as county maternal and child health leaders can assist local practices with the identification and development of local resources and referrals.
Although full implementation of trauma-informed care in obstetrics and gynecology will require large-scale change and coordination involving many levels of stakeholders, multidisciplinary teams, and a systems approach, obstetric clinicians and practices need not wait for system-level change to begin learning and practicing principles of trauma-informed care and implementing inquiry about patients' past and present trauma and adversity. Inquiry about and screening for adversity, trauma, and resilience and responding with conversations and supportive plans can help heal the effects of adversity and trauma and set our patients—and the next generation—on a path to health and thriving.
CME FOR THE CLINICAL EXPERT SERIES
Learning Objectives for “Addressing Adverse Childhood and Adult Experiences During Prenatal Care.”
After completing this continuing education activity, you will be able to:
Discuss the concept of “trauma-informed care”;
List possible adverse outcomes in the perinatal setting that accrue from past trauma, racism, and health inequities; and
Implement practice changes, including using open-ended questions, structured survey measures, or a combination of both techniques to enhance trauma-informed prenatal care.
Instructions for Obtaining AMA PRA Category 1 Credits™
Continuing Medical Education credit is provided through joint providership with The American College of Obstetricians and Gynecologists.
Obstetrics & Gynecology includes CME-certified content that is designed to meet the educational needs of its readers. This article is certified for 2 AMA PRA Category 1 Credits.™ This activity is available for credit through June 30, 2026.
Accreditation Statement
ACCME Accreditation
The American College of Obstetricians and Gynecologists is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians.
AMA PRA Category 1 Credit(s)™
The American College of Obstetricians and Gynecologists designates this journal-based CME activity for a maximum of 2 AMA PRA Category 1 Credits.™ Physicians should claim only the credit commensurate with the extent of their participation in the activity.
College Cognate Credit(s)
The American College of Obstetricians and Gynecologists designates this journal-based CME activity for a maximum of 2 Category 1 College Cognate Credits. The College has a reciprocity agreement with the AMA that allows AMA PRA Category 1 Credits™ to be equivalent to College Cognate Credits.
Disclosure of Faculty and Planning Committee Industry Relationships
In accordance with the College policy, all faculty and planning committee members have signed a conflict of interest statement in which they have disclosed any financial interests or other relationships with industry relative to article topics. Such disclosures allow the participant to evaluate better the objectivity of the information presented in the articles.
How to Earn CME Credit
To earn CME credit, you must read the article in Obstetrics & Gynecology and complete the quiz, answering at least 70 percent of the questions correctly. For more information on this CME educational offering, visit the Lippincott CMEConnection portal at https://cme.lww.com/browse/sources/196 to register and to complete the CME activity online. ACOG Fellows will receive 50% off by using coupon code, ONG50.
Hardware/software requirements are a desktop or laptop computer (Mac or PC) and an Internet browser. This activity is available for credit through June 30, 2026. To receive proper credits for this activity, each participant will need to make sure that the information on their profile for the CME platform (where this activity is located) is updated with 1) their date of birth (month and day only) and 2) their ACOG ID. In addition, participants should select that they are board-certified in obstetrics and gynecology.
The privacy policies for the Obstetrics & Gynecology website and the Lippincott CMEConnection portal are available at http://www.greenjournal. org and https://cme.lww.com/browse/sources/196, respectively.
Contact Information
Questions related to transcripts may be directed to cme@acog.org. For other queries, please contact the Obstetrics & Gynecology Editorial Office at obgyn@greenjournal.org. For queries related to the CME test online, please contact ceconnection@wolterskluwer.com or 1-800-787-8985.
Footnotes
This project was funded by California Department of Health Care Services. The contents may not necessarily reflect the official views or policies of the State of California. Contract No. 19-96247 A02. Additional support was provided by the School of Medicine, Stanford University.
Presented at the 2023 Maternal Mental Health FORUM, held virtually, March 22–24, 2023.
Financial Disclosure The authors did not report any potential conflicts of interest.
The authors thank the Maternal Adverse Childhood Experiences (ACEs) Task Force, whose grounded experience in serving prenatal patients across perinatal settings and populations brought practical guidance to the development of this article; Chris Dunkel Schetter, PhD, Shantay Davies-Balch, MBA, CLE, Judy Mikacich, MD, Lisa Korst, MD, Amanda Williams, MD, Douglas Fenton, MD, and Holly Smith, CNM, for their thoughtful feedback on an earlier draft of the manuscript; and the California Office of the Surgeon General and affiliated researchers, medical directors, and contractors for their guidance and insight.
The opinions and recommendations in this article are from the authors alone.
Each author has confirmed compliance with the journal's requirements for authorship.
Peer reviews and author correspondence are available at http://links.lww.com/AOG/D157.
REFERENCES
- 1.Rutter M, Mercuro N, Rutter ML, Giller H, Hagell A. Antisocial behavior by young people: a major new review. Cambridge University Press; 1998. [Google Scholar]
- 2.Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the Adverse Childhood Experiences (ACE) study. Am J Prev Med 1998;14:245–58. doi: 10.1016/s0749-3797(98)00017-8 [DOI] [PubMed] [Google Scholar]
- 3.Bhushan D, Kotz K, McCall J, Wirtz S, Gilgoff R, Rishi Dube S, et al. Roadmap for resilience: the California Surgeon General’s report on adverse childhood experiences, toxic stress, and health. Office of the California Surgeon General. 2020. Accessed December 5, 2022. doi: 10.48019/PEAM8812 [DOI] [Google Scholar]
- 4.Garner A, Yogman M; Committee on Psychosocial Aspects of Child and Family Health, Section on Developmental and Behavioral Pediatrics, Council on Early Childhood. Preventing childhood toxic stress: partnering with families and communities to promote relational health. Pediatrics 2021;148:e2021052582. doi: 10.1542/peds.2021-052582 [DOI] [PubMed] [Google Scholar]
- 5.Machtinger EL, Cuca YP, Khanna N, Rose CD, Kimberg LS. From treatment to healing: the promise of trauma-informed primary care. Womens Health Issues 2015;25:193–7. doi: 10.1016/j.whi.2015.03.008 [DOI] [PubMed] [Google Scholar]
- 6.Substance Abuse and Mental Health Services Administration. SAMHSA's concept of trauma and guidance for a trauma-informed approach. Department of Health and Human Services. Accessed December 5, 2022. https://ncsacw.acf.hhs.gov/userfiles/files/SAMHSA_Trauma.pdf [Google Scholar]
- 7.Machtinger EL, Lieberman A, Lightfoot M. Research, practice, and policy implications of adverse childhood events. JAMA Pediatr 2021;175:866–7. doi. 10.1001/jamapediatrics.2021.0810 [DOI] [PubMed] [Google Scholar]
- 8.Caring for patients who have experienced trauma. ACOG Committee Opinion No. 825.American College of Obstetricians and Gynecologists. Obstet Gynecol 2021;137:e94–9. doi: 10.1097/AOG.0000000000004326 [DOI] [PubMed] [Google Scholar]
- 9.Benjet C, Bromet E, Karam EG, Kessler RC, McLaughlin KA, Ruscio AM, et al. The epidemiology of traumatic event exposure worldwide: results from the World Mental Health Survey Consortium. Psychol Med 2016;46:327–43. doi: 10.1017/S0033291715001981 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Dierkhising CB, Ko SJ, Woods-Jaeger B, Briggs EC, Lee R, Pynoos RS. Trauma histories among justice-involved youth: findings from the National Child Traumatic Stress Network. Eur J Psychotraumatol. 2013;4:ejpt.v4i0.20274. doi: 10.3402/ejpt.v4i0.20274 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Narayan AJ, Thomas M, Nau M, Rivera LM, Harris WW, Bernstein RE, et al. Between pregnancy and motherhood: identifying unmet mental health needs in pregnant women with lifetime adversity. Zero to Three 2017;37:14–23. [Google Scholar]
- 12.Daskalakis NP, Xu C, Bader HN, Chatzinakos C, Weber P, Makotkine I, et al. Intergenerational trauma is associated with expression alterations in glucocorticoid- and immune-related genes. Neuropsychopharmacology 2021;46:763–73. doi: 10.1038/s41386-020-00900-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Davis EP, Narayan AJ. Pregnancy as a period of risk, adaptation, and resilience for mothers and infants. Dev Psychopathol 2020;32:1625–39. doi: 10.1017/S0954579420001121 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.River LM, Narayan AJ, Galvan T, Rivera L, Harris WW, Lieberman AF. On the verge of motherhood and mental illness: prenatal mental health service utilization among women at highest risk. Zero to Three 2019;39:33–42. [Google Scholar]
- 15.Lindqvist M, Lindkvist M, Eurenius E, Persson M, Mogren I. Change of lifestyle habits: motivation and ability reported by pregnant women in northern Sweden. Sex Reprod Healthc 2017;13:83–90. doi: 10.1016/j.srhc.2017.07.001 [DOI] [PubMed] [Google Scholar]
- 16.O'Brien OA, Lindsay KL, McCarthy M, McGloin AF, Kennelly M, Scully HA, et al. Influences on the food choices and physical activity behaviours of overweight and obese pregnant women: a qualitative study. Midwifery 2017;47:28–35. doi: 10.1016/j.midw.2017.02.003 [DOI] [PubMed] [Google Scholar]
- 17.Glynn LM. Giving birth to a new brain: hormone exposures of pregnancy influence human memory. Psychoneuroendocrinology 2010;35:1148–55. doi: 10.1016/j.psyneuen.2010.01.015 [DOI] [PubMed] [Google Scholar]
- 18.Glynn LM. Increasing parity is associated with cumulative effects on memory. J Womens Health 2012;21:1038–45. doi: 10.1089/jwh.2011.3206 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Glynn LM, Davis EP, Sandman CA. New insights into the role of perinatal HPA-axis dysregulation in postpartum depression. Neuropeptides 2013;47:363–70. doi: 10.1016/j.npep.2013.10.007 [DOI] [PubMed] [Google Scholar]
- 20.Davis EP, Hankin BL, Glynn LM, Head K, Kim DJ, Sandman CA. Prenatal maternal stress, child cortical thickness, and adolescent depressive symptoms. Child Dev 2020;91:e432–50. doi: 10.1111/cdev.13252 [DOI] [PubMed] [Google Scholar]
- 21.Raja S, Hasnain M, Hoersch M, Gove-Yin S, Rajagopalan C. Trauma informed care in medicine: current knowledge and future research directions. Fam Community Health 2015;38:216–26. doi: 10.1097/FCH.0000000000000071 [DOI] [PubMed] [Google Scholar]
- 22.Flanagan T, Alabaster A, McCaw B, Stoller N, Watson C, Young-Wolff KC. Feasibility and acceptability of screening for adverse childhood experiences in prenatal care. J Womens Health 2018;27:903–11. doi: 10.1089/jwh.2017.6649 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.LaPlante LM, Gopalan P, Glance J. Addressing intimate partner violence: reducing barriers and improving residents' attitudes, knowledge, and practices. Acad Psychiatry 2016;40:825–8. doi: 10.1007/s40596-016-0529-8 [DOI] [PubMed] [Google Scholar]
- 24.Hall SL, Famuyide ME, Saxton SN, Moore TA, Mosher S, Sorrells K, et al. Improving staff knowledge and attitudes toward providing psychosocial support to NICU parents through an online education course. Adv Neonatal Care 2019;19:490–9. doi: 10.1097/ANC.0000000000000649 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Schulman M, Menschner C. Laying the groundwork for trauma-informed care. Accessed December 5, 2022. https://chcs.org/media/Laying-the-Groundwork-for-TIC_012418.pdf [Google Scholar]
- 26.New data report: 781,400 screenings for ACEs. ACEs Aware. April 21, 2022. Accessed December 5, 2022. https://acesaware.org/blog/new-data-report-781400-screenings-for-aces/
- 27.Raja S, Rabinowitz EP, Gray MJ. Universal screening and trauma informed care: current concerns and future directions. Fam Syst Health 2021;39:526–34. doi: 10.1037/fsh0000585 [DOI] [PubMed] [Google Scholar]
- 28.Holden K, Akintobi T, Hopkins J, Belton A, McGregor B, Blanks S, et al. Community engaged leadership to advance health equity and build healthier communities. Soc Sci 2015;5:2. doi: 10.3390/socsci5010002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 2018;169:467–73. doi: 10.7326/M18-0850 [DOI] [PubMed] [Google Scholar]
- 30.Steele H, Bate J, Steele M, Dube SR, Danskin K, Knafo H, et al. Adverse childhood experiences, poverty, and parenting stress. Can J Behav Sci 2016;48:32–8. doi: 10.1037/cbs0000034 [DOI] [Google Scholar]
- 31.Berlin LJ, Appleyard K, Dodge KA. Intergenerational continuity in child maltreatment: mediating mechanisms and implications for prevention. Child Dev 2011;82:162–76. doi: 10.1111/j.1467-8624.2010.01547.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Noll JG, Schulkin J, Trickett PK, Susman EJ, Breech L, Putnam FW. Differential pathways to preterm delivery for sexually abused and comparison women. J Pediatr Psychol 2007;32:1238–48. doi: 10.1093/jpepsy/jsm046 [DOI] [PubMed] [Google Scholar]
- 33.Ammerman RT, Peugh JL, Teeters AR, Putnam FW, Van Ginkel JB. Child maltreatment history and response to CBT treatment in depressed mothers participating in home visiting. J Interpers Violence 2016;31:774–91. doi: 10.1177/0886260514556769 [DOI] [PubMed] [Google Scholar]
- 34.Ammerman RT, Shenk CE, Teeters AR, Noll JG, Putnam FW, Van Ginkel JB. Impact of depression and childhood trauma in mothers receiving home visitation. J Child Fam Stud 2012;21:612–25. doi: 10.1007/s10826-011-9513-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Altemeier WA, O'Connor S, Sherrod KB, Tucker D, Vietze P. Outcome of abuse during childhood among pregnant low income women. Child Abuse Neglect 1986;10:319–30. doi: 10.1016/0145-2134(86)90007-4 [DOI] [PubMed] [Google Scholar]
- 36.Font SA, Maguire-Jack K. Pathways from childhood abuse and other adversities to adult health risks: the role of adult socioeconomic conditions. Child Abuse Neglect 2016;51:390–9. doi: 10.1016/j.chiabu.2015.05.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Jackson DB, Chilton M, Johnson KR, Vaughn MG. Adverse childhood experiences and household food insecurity: findings from the 2016 National Survey of Children's Health. Am J Prev Med 2019;57:667–74. doi: 10.1016/j.amepre.2019.06.004 [DOI] [PubMed] [Google Scholar]
- 38.Narayan AJ, Hagan MJ, Cohodes E, Rivera LM, Lieberman AF. Early childhood victimization and physical intimate partner violence during pregnancy: a developmental and person-oriented approach. J Interpers Violence 2019;34:3–26. doi: 10.1177/0886260516639261 [DOI] [PubMed] [Google Scholar]
- 39.Campbell R, Greeson MR, Bybee D, Raja S. The co-occurrence of childhood sexual abuse, adult sexual assault, intimate partner violence, and sexual harassment: a mediational model of posttraumatic stress disorder and physical health outcomes. J Consulting Clin Psychol 2008;76:194–207. doi: 10.1037/0022-006X.76.2.194 [DOI] [PubMed] [Google Scholar]
- 40.Braveman P. What is health equity: and how does a life-course approach take us further toward it? Matern Child Health J 2014;18:366–72. doi: 10.1007/s10995-013-1226-9 [DOI] [PubMed] [Google Scholar]
- 41.Hetherington E, Doktorchik C, Premji SS, McDonald SW, Tough SC, Sauve RS. Preterm birth and social support during pregnancy: a systematic review and meta-analysis. Paediatr Perinat Epidemiol 2015;29:523–35. doi: 10.1111/ppe.12225 [DOI] [PubMed] [Google Scholar]
- 42.McDonald SW, Kingston D, Bayrampour H, Dolan SM, Tough SC. Cumulative psychosocial stress, coping resources, and preterm birth. Arch Womens Ment Health 2014;17:559–68. doi: 10.1007/s00737-014-0436-5 [DOI] [PubMed] [Google Scholar]
- 43.Shonkoff JP, Garner AS, Committee on Early Childhood, Adoption, and Dependent Care, and Section on Developmental and Behavioral Pediatrics, Siegel BS, Dobbins MI, Earls MF, McGuinn L, et al. The lifelong effects of early childhood adversity and toxic stress. Pediatrics 2012;129:e232–46. doi: 10.1542/peds.2011-2663 [DOI] [PubMed] [Google Scholar]
- 44.Geronimus AT. The weathering hypothesis and the health of African-American women and infants: evidence and speculations. Ethn Dis 1992;2:207–21. [PubMed] [Google Scholar]
- 45.Riggan KA, Gilbert A, Allyse MA. Acknowledging and addressing allostatic load in pregnancy care. J Racial Ethn Health Disparities 2021;8:69–79. doi: 10.1007/s40615-020-00757-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Atzl VM, Grande LA, Davis EP, Narayan AJ. Perinatal promotive and protective factors for women with histories of childhood abuse and neglect. Child Abuse Neglect 2019;91:63–77. doi: 10.1016/j.chiabu.2019.02.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Chamberlain C, Gee G, Harfield S, Campbell S, Brennan S, Clark Y, et al. Parenting after a history of childhood maltreatment: a scoping review and map of evidence in the perinatal period. PLoS One 2019;14:e0213460. doi: 10.1371/journal.pone.0213460 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Gilgoff R, Singh L, Koita K, Gentile B, Marques SS. Adverse childhood experiences, outcomes, and interventions. Pediatr Clin North Am 2020;67:259–73. doi: 10.1016/j.pcl.2019.12.001 [DOI] [PubMed] [Google Scholar]
- 49.Montgomery E, Pope C, Rogers J. The re-enactment of childhood sexual abuse in maternity care: a qualitative study. BMC Pregnancy Childbirth 2015;15:194. doi: 10.1186/s12884-015-0626-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Coles J. Qualitative study of breastfeeding after childhood sexual assault. J Hum Lact 2009;25:317–24. doi: 10.1177/0890334409334926 [DOI] [PubMed] [Google Scholar]
- 51.Millar HC, Lorber S, Vandermorris A, Thompson G, Thompson M, Allen L, et al. “No, you need to explain what you are doing”: obstetric care experiences and preferences of adolescent mothers with a history of childhood trauma. J Pediatr Adolesc Gynecol 2021;34:538–45. doi: 10.1016/j.jpag.2021.01.006 [DOI] [PubMed] [Google Scholar]
- 52.Channell Doig A, Jasczynski M, Fleishman JL, Aparicio EM. Breastfeeding among mothers who have experienced childhood maltreatment: a review. J Hum Lact 2020;36:710–22. doi: 10.1177/0890334420950257 [DOI] [PubMed] [Google Scholar]
- 53.Hooper C-A, Koprowska J. The vulnerabilities of children whose parents have been sexually abused in childhood: towards a new framework. Br J Soc Work 2004;34:165–80. doi: 10.1093/bjsw/bch020 [DOI] [Google Scholar]
- 54.Muzik M, Ads M, Bonham C, Lisa Rosenblum K, Broderick A, Kirk R. Perspectives on trauma-informed care from mothers with a history of childhood maltreatment: a qualitative study. Child Abuse Neglect 2013;37:1215–24. doi: 10.1016/j.chiabu.2013.07.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Gokhale P, Young MR, Williams MN, Reid SN, Tom LS, O'Brian CA, et al. Refining trauma-informed perinatal care for urban prenatal care patients with multiple lifetime traumatic exposures: a qualitative study. J Midwifery Womens Health 2020;65:224–30. doi: 10.1111/jmwh.13063 [DOI] [PubMed] [Google Scholar]
- 56.Olsen JM, Galloway EG, Guthman PL. Exploring women's perspectives on prenatal screening for adverse childhood experiences. Public Health Nurs 2021;38:997–1008. doi: 10.1111/phn.12956 [DOI] [PubMed] [Google Scholar]
- 57.Watson C, Wei J, Varnado N, Rios N, Staunton M, Ferguson D, et al. Pregnant women's perspectives on screening for adverse childhood experiences and resilience during prenatal care. Psychol Trauma Theor Res Pract Pol 2022;14:1299–303. doi: 10.1037/tra0001166 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Stevens NR, Holmgreen L, Hobfoll SE, Cvengros JA. Assessing trauma history in pregnant patients: a didactic module and role-play for obstetrics and gynecology residents. MedEdPORTAL 2020;16:10925. doi: 10.15766/mep_2374-8265.10925 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Slade P, Balling K, Sheen K, Goodfellow L, Rymer J, Spiby H, et al. Work-related post-traumatic stress symptoms in obstetricians and gynaecologists: findings from INDIGO, a mixed-methods study with a cross-sectional survey and in-depth interviews. BJOG 2020;127:600–8. doi: 10.1111/1471-0528.16076 [DOI] [PubMed] [Google Scholar]
- 60.Kruper A, Domeyer-Klenske A, Treat R, Pilarski A, Kaljo K. Secondary traumatic stress in ob-gyn: a mixed methods analysis assessing physician impact and needs. J Surg Educ 2021;78:1024–34. doi: 10.1016/j.jsurg.2020.08.038 [DOI] [PubMed] [Google Scholar]
- 61.Sperlich M, Seng JS, Li Y, Taylor J, Bradbury-Jones C. Integrating trauma-informed care into maternity care practice: conceptual and practical issues. J Midwifery Womens Health 2017;62:661–72. doi: 10.1111/jmwh.12674 [DOI] [PubMed] [Google Scholar]
- 62.American College of Obstetricians and Gynecologists. Joint statement: collective action addressing racism. Accessed December 5, 2022. https://acog.org/en/news/news-articles/2020/08/joint-statement-obstetrics-and-gynecology-collective-action-addressing-racism
- 63.Levy-Carrick NC, Lewis-OʼConnor A, Rittenberg E, Manosalvas K, Stoklosa HM, Silbersweig DA. Promoting health equity through trauma-informed care: critical role for physicians in policy and program development. Fam Community Health 2019;42:104–8. doi: 10.1097/FCH.0000000000000214 [DOI] [PubMed] [Google Scholar]
- 64.Zarse EM, Neff MR, Yoder R, Hulvershorn L, Chambers JE, Chambers RA. The Adverse Childhood Experiences Questionnaire: two decades of research on childhood trauma as a primary cause of adult mental illness, addiction, and medical diseases. Cogent Med 2019;6:1581447. doi: 10.1080/2331205x.2019.1581447 [DOI] [Google Scholar]
- 65.Glowa PT, Olson AL, Johnson DJ. Screening for adverse childhood experiences in a family medicine setting: a feasibility study. J Am Board Fam Med 2016;29:303–7. doi: 10.3122/jabfm.2016.03.150310 [DOI] [PubMed] [Google Scholar]
- 66.Purewal SK, Marques SS, Koita K, Bucci M. Assessing the integration of the Center for Youth Wellness Adverse Childhood Experiences Questionnaire (CYW ACE-Q) in a pediatric primary care setting [abstract]. J Adolesc Health 2016;58:S47. doi: 10.1016/j.jadohealth.2015.10.106 [DOI] [Google Scholar]
- 67.Osofsky JD, Osofsky HJ, Frazer AL, Fields-Olivieri MA, Many M, Selby M, et al. The importance of adverse childhood experiences during the perinatal period. Am Psychol 2021;76:350–63. doi: 10.1037/amp0000770 [DOI] [PubMed] [Google Scholar]
- 68.McLennan JD, MacMillan HL, Afifi TO. Questioning the use of Adverse Childhood Experiences (ACEs) Questionnaires. Child Abuse Neglect 2020;101:104331. doi: 10.1016/j.chiabu.2019.104331 [DOI] [PubMed] [Google Scholar]
- 69.Intimate partner violence. Committee Opinion No. 518. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;119:412–7. doi: 10.1097/AOG.0b013e318249ff74 [DOI] [PubMed] [Google Scholar]
- 70.Opioid use and opioid use disorder in pregnancy. Committee Opinion No. 711. American College of Obstetricians and Gynecologists. Obstet Gynecol 2017;130:488–9. doi: 10.1097/AOG.0000000000002229 [DOI] [PubMed] [Google Scholar]
- 71.Screening for perinatal depression. ACOG Committee Opinion No. 757. American College of Obstetricians and Gynecologists. Obstet Gynecol 2018;132:e208–12. doi: 10.1097/AOG.0000000000002927 [DOI] [PubMed] [Google Scholar]
- 72.Importance of social determinants of health and cultural awareness in the delivery of reproductive health care. ACOG Committee Opinion No. 729. American College of Obstetricians and Gynecologists. Obstet Gynecol 2018;131:e43–8. doi: 10.1097/AOG.0000000000002459 [DOI] [PubMed] [Google Scholar]
- 73.Kimberg L, Wheeler M. Trauma and trauma-informed care. In: Gerber MR, editor. Trauma-informed healthcare approaches. Springer International Publishing; 2019. [Google Scholar]
- 74.Blair A, Wasson K. Professionalism and appropriate expression of empathy when breaking bad news. AMA J Ethics 2015;17:111–5. doi: 10.1001/virtualmentor.2015.17.02.ecas1-1502 [DOI] [PubMed] [Google Scholar]
- 75.van Osch M, Sep M, van Vliet LM, van Dulmen S, Bensing JM. Reducing patients' anxiety and uncertainty, and improving recall in bad news consultations. Health Psychol 2014;33:1382–90. doi: 10.1037/hea0000097 [DOI] [PubMed] [Google Scholar]
- 76.van der Meulen N, Jansen J, van Dulmen S, Bensing J, van Weert J. Interventions to improve recall of medical information in cancer patients: a systematic review of the literature. Psychooncology 2008;17:857–68. doi: 10.1002/pon.1290 [DOI] [PubMed] [Google Scholar]
- 77.Reid-Ponte P. Distress in cancer patients and primary nurses' empathy skills. Cancer Nurs 1992;15:283–92. doi: 10.1097/00002820-199208000-00006 [DOI] [PubMed] [Google Scholar]
- 78.Roter DL, Hall JA. Physician's interviewing styles and medical information obtained from patients. J Gen Intern Med 1987;2:325–9. doi: 10.1007/BF02596168 [DOI] [PubMed] [Google Scholar]
- 79.Stewart MA. What is a successful doctor-patient interview? A study of interactions and outcomes. Soc Sci Med 1984;19:167–75. doi: 10.1016/0277-9536(84)90284-3 [DOI] [PubMed] [Google Scholar]
- 80.Bochner S, Insko CA. Communicator discrepancy, source credibility, and opinion change. J Personal Soc Psychol 1966;4:614–21. doi: 10.1037/h0021192 [DOI] [Google Scholar]
- 81.Chaiken S, Maheswaran D. Heuristic processing can bias systematic processing: effects of source credibility, argument ambiguity, and task importance on attitude judgment. J Personal Soc Psychol 1994;66:460–73. doi: 10.1037//0022-3514.66.3.460 [DOI] [PubMed] [Google Scholar]
- 82.Draucker CB, Martsolf DS, Roller C, Knapik G, Ross R, Stidham AW. Healing from childhood sexual abuse: a theoretical model. J Child Sex Abuse 2011;20:435–66. doi: 10.1080/10538712.2011.588188 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.At-risk drinking and alcohol dependence: obstetric and gynecologic implications. Committee Opinion No. 496. American College of Obstetricians and Gynecologists. Obstet Gynecol 2011;118:383–8. doi: 10.1097/AOG.0b013e31822c9906 [DOI] [PubMed] [Google Scholar]
- 84.Wilkes G. Abused child to nonabusive parent: resilience and conceptual change. J Clin Psychol 2002;58:261–76. doi: 10.1002/jclp.10024 [DOI] [PubMed] [Google Scholar]
- 85.Dijkstra S. Two mothers abused as children on raising their children: making a plea for a differentiated approach. Child Abuse Rev 1995;4:291–7. doi: 10.1002/car.2380040408 [DOI] [Google Scholar]
- 86.Dunkel Schetter C. Psychological science on pregnancy: stress processes, biopsychosocial models, and emerging research issues. Annu Rev Psychol 2011;62:531–58. doi: 10.1146/annurev.psych.031809.130727 [DOI] [PubMed] [Google Scholar]
- 87.Dunkel Schetter C, Sagrestano L, Feldman Killingsworth C. Social support in pregnancy in handbook of social support and the family. Springer; 1996. p. 375–412. [Google Scholar]
- 88.Sperlich M, Seng JS. Survivor moms: women's stories of birthing, mothering and healing after sexual abuse. Motherbaby Press; 2008. [Google Scholar]
- 89.Thomas JC, Letourneau N, Bryce CI, Campbell TS, Giesbrecht GF; APrON Study Team. Biological embedding of perinatal social relationships in infant stress reactivity. Dev Psychobiol 2017;59:425–35. doi: 10.1002/dev.21505 [DOI] [PubMed] [Google Scholar]
- 90.Racine N, Zumwalt K, McDonald S, Tough S, Madigan S. Perinatal depression: the role of maternal adverse childhood experiences and social support. J Affective Disord 2020;263:576–81. doi: 10.1016/j.jad.2019.11.030 [DOI] [PubMed] [Google Scholar]
- 91.Séguin L, Potvin L, St Denis M, Loiselle J. Chronic stressors, social support, and depression during pregnancy. Obstet Gynecol 1995;85:583–9. doi: 10.1016/0029-7844(94)00449-N [DOI] [PubMed] [Google Scholar]
- 92.Giurgescu C, Templin TN. Father involvement and psychological well-being of pregnant women. MCN Am J Matern Child Nurs 2015;40:381–7. doi: 10.1097/NMC.0000000000000183 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Pilkington PD, Milne LC, Cairns KE, Lewis J, Whelan TA. Modifiable partner factors associated with perinatal depression and anxiety: a systematic review and meta-analysis. J Affective Disord 2015;178:165–80. doi: 10.1016/j.jad.2015.02.023 [DOI] [PubMed] [Google Scholar]
- 94.Olds DL, Eckenrode J, Henderson CR, Kitzman H, Powers J, Cole R, et al. Long-term effects of home visitation on maternal life course and child abuse and neglect: fifteen-year follow-up of a randomized trial. JAMA 1997;278:637–43. doi: 10.1001/jama.1997.03550080047038 [DOI] [PubMed] [Google Scholar]
- 95.Reuveni I, Lauria M, Monk C, Werner E. The impact of childhood trauma on psychological interventions for depression during pregnancy and postpartum: a systematic review. Arch Womens Ment Health 2021;24:367–80. doi: 10.1007/s00737-020-01066-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Wickramaratne P, Gameroff MJ, Pilowsky DJ, Hughes CW, Garber J, Malloy E, et al. Children of depressed mothers 1 year after remission of maternal depression: findings from the STAR*D-Child study. Am J Psychiatry 2011;168:593–602. doi: 10.1176/appi.ajp.2010.10010032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Blalock JA, Minnix JA, Mathew AR, Wetter DW, McCullough JP, Cinciripini PM. Relationship of childhood trauma to depression and smoking outcomes in pregnant smokers. J Consulting Clin Psychol 2013;81:821–30. doi: 10.1037/a0033381 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.O'Connor E, Senger CA, Henninger ML, Coppola E, Gaynes BN. Interventions to prevent perinatal depression: evidence report and systematic review for the US Preventive Services Task Force. JAMA 2019;321:588–601. doi: 10.1001/jama.2018.20865 [DOI] [PubMed] [Google Scholar]
- 99.Dennis C-L, Dowswell T. Psychosocial and psychological interventions for preventing postpartum depression. The Cochrane Database of Systematic Reviews 2013, Issue 2. Art. No.: CD001134. doi: 10.1002/14651858.CD001134.pub3 [DOI] [PubMed] [Google Scholar]
- 100.Dennis C-L, Hodnett ED. Psychosocial and psychological interventions for treating postpartum depression. The Cochrane Database of Systematic Reviews 2007, Issue 4. Art. No.: CD006116. doi: 10.1002/14651858.CD006116.pub2 [DOI] [PubMed] [Google Scholar]
- 101.Ponting C, Urizar GG, Dunkel Schetter C. Psychological interventions for prenatal anxiety in Latinas and Black women: a scoping review and recommendations. Front Psychiatry 2022;13:820343. doi: 10.3389/fpsyt.2022.820343 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Ponting C, Mahrer NE, Zelcer H, Dunkel Schetter C, Chavira DA. Psychological interventions for depression and anxiety in pregnant Latina and Black women in the United States: a systematic review. Clin Psychol Psychother 2020;27:249–65. doi: 10.1002/cpp.2424 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Brantsæter AL, Haugen M, Myhre R, Sengpiel V, Englund-Ögge L, Nilsen RM, et al. Diet matters, particularly in pregnancy: results from MoBa studies of maternal diet and pregnancy outcomes. Norsk Epidemiologi 2014;24:63–77. doi: 10.5324/nje.v24i1-2.1805 [DOI] [Google Scholar]
- 104.Teede HJ, Bailey C, Moran LJ, Bahri Khomami M, Enticott J, Ranasinha S, et al. Association of antenatal diet and physical activity–based interventions with gestational weight gain and pregnancy outcomes: a systematic review and meta-analysis. JAMA Intern Med 2022;182:106–14. doi: 10.1001/jamainternmed.2021.6373 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Morres ID, Tzouma N-A, Hatzigeorgiadis A, Krommidas C, Kotronis KV, Dafopoulos K, et al. Exercise for perinatal depressive symptoms: a systematic review and meta-analysis of randomized controlled trials in perinatal health services. J Affective Disord 2022;298:26–42. doi: 10.1016/j.jad.2021.10.124 [DOI] [PubMed] [Google Scholar]
- 106.Physical activity and exercise during pregnancy and the postpartum period. ACOG Committee Opinion No. 804. American College of Obstetricians and Gynecologists. Obstet Gynecol 2020;135:e178–88. doi: 10.1097/AOG.0000000000003772 [DOI] [PubMed] [Google Scholar]
- 107.Bacaro V, Benz F, Pappaccogli A, De Bartolo P, Johann AF, Palagini L, et al. Interventions for sleep problems during pregnancy: a systematic review. Sleep Med Rev 2020;50:101234. doi: 10.1016/j.smrv.2019.101234 [DOI] [PubMed] [Google Scholar]
- 108.Dhillon A, Sparkes E, Duarte RV. Mindfulness-based interventions during pregnancy: a systematic review and meta-analysis. Mindfulness (N Y) 2017;8:1421–37. doi: 10.1007/s12671-017-0726-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Goodman JH. Women's attitudes, preferences, and perceived barriers to treatment for perinatal depression. Birth 2009;36:60–9. doi: 10.1111/j.1523-536X.2008.00296.x [DOI] [PubMed] [Google Scholar]
- 110.Broberg L, Ersbøll AS, Backhausen MG, Damm P, Tabor A, Hegaard HK. Compliance with national recommendations for exercise during early pregnancy in a Danish cohort. BMC Pregnancy Childbirth 2015;15:317. doi: 10.1186/s12884-015-0756-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Pebole M, Gobin RL, Hall KS. Trauma-informed exercise for women survivors of sexual violence. Transl Behav Med 2021;11:686–91. doi: 10.1093/tbm/ibaa043 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Bennett GG, McNeill LH, Wolin KY, Duncan DT, Puleo E, Emmons KM. Safe to walk? Neighborhood safety and physical activity among public housing residents. PLoS Med 2007;4:1599–606. doi: 10.1371/journal.pmed.0040306 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Montgomery E. Feeling safe: a metasynthesis of the maternity care needs of women who were sexually abused in childhood. Birth 2013;40:88–95. doi: 10.1111/birt.12043 [DOI] [PubMed] [Google Scholar]
- 114.Approaches to limit intervention during labor and birth. ACOG Committee Opinion No. 766. American College of Obstetricians and Gynecologists. Obstet Gynecol 2019;133:e164–73. doi: 10.1097/AOG.0000000000003074 [DOI] [PubMed] [Google Scholar]
- 115.Simkin P, Bolding A. Update on nonpharmacologic approaches to relieve labor pain and prevent suffering. J Midwifery Womens Health 2004;49:489–504. doi: 10.1016/j.jmwh.2004.07.007 [DOI] [PubMed] [Google Scholar]
- 116.Bohren MA, Hofmeyr GJ, Sakala C, Fukuzawa RK, Cuthbert A. Continuous support for women during childbirth. The Cochrane Database of Systematic Reviews 2017, Issue 7. Art. No.: CD003766. doi: 10.1002/14651858.CD003766.pub6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Chamberlain C, Ralph N, Hokke S, Clark Y, Gee G, Stansfield C, et al. Healing the past by nurturing the future: a qualitative systematic review and meta-synthesis of pregnancy, birth and early postpartum experiences and views of parents with a history of childhood maltreatment. PLoS One 2019;14:e0225441. doi: 10.1371/journal.pone.0225441 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Optimizing postpartum care. ACOG Committee Opinion No. 736. American College of Obstetricians and Gynecologists. Obstet Gynecol 2018;132:784–5. doi: 10.1097/AOG.0000000000002849 [DOI] [PubMed] [Google Scholar]
- 119.Ford K, Hughes K, Hardcastle K, Di Lemma LCG, Davies AR, Edwards S, et al. The evidence base for routine enquiry into adverse childhood experiences: a scoping review. Child Abuse Neglect 2019;91:131–46. doi: 10.1016/j.chiabu.2019.03.007 [DOI] [PubMed] [Google Scholar]
- 120.California Department of Health Care Services. Trauma informed care. Accessed December 5, 2022. https://www.dhcs.ca.gov/provgovpart/Pages/TraumaCare.aspx
- 121.McLemore MR, Altman MR, Cooper N, Williams S, Rand L, Franck L. Health care experiences of pregnant, birthing and postnatal women of color at risk for preterm birth. Soc Sci Med 2018;201:127–35. doi: 10.1016/j.socscimed.2018.02.013 [DOI] [PubMed] [Google Scholar]
- 122.Menschner C, Maul A. Center for Health Care Strategies Inc, Robert Wood Johnson Foundation. Key ingredients for successful trauma-informed care implementation. Center for Health Care Strategies, Inc; Robert Wood Johnson Foundation; 2016. [Google Scholar]
- 123.Cronholm PF, Forke CM, Wade R, Bair-Merritt MH, Davis M, Harkins-Schwarz M, et al. Adverse childhood experiences: expanding the concept of adversity. Am J Prev Med 2015;49:354–61. doi: 10.1016/j.amepre.2015.02.001 [DOI] [PubMed] [Google Scholar]
- 124.Lewis-O’Connor A, Warren A, Lee JV, Levy-Carrick N, Grossman S, Chadwick M, et al. The state of the science on trauma inquiry. Womens Health (Lond) 2019;15:174550651986123. doi: 10.1177/1745506519861234 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Vu C, Rothman E, Kistin CJ, Barton K, Bulman B, Budzak-Garza A, et al. Adapting the patient-centered medical home to address psychosocial adversity: results of a qualitative study. Acad Pediatr 2017;17:S115–22. doi: 10.1016/j.acap.2017.01.014 [DOI] [PubMed] [Google Scholar]
- 126.Wagnild GM, Collins JA. Assessing resilience. J Psychosoc Nurs Ment Health Serv 2009;47:28–33. doi: 10.3928/02793695-20091103-01 [DOI] [PubMed] [Google Scholar]
- 127.McEwen BS. Central effects of stress hormones in health and disease: understanding the protective and damaging effects of stress and stress mediators. Eur J Pharmacol 2008;583:174–85. doi: 10.1016/j.ejphar.2007.11.071 [DOI] [PMC free article] [PubMed] [Google Scholar]