

Abstract
The unbalanced allocation of healthcare resources is a major challenge that hinders access to healthcare. Taking Shenzhen as an example, this study aimed to enhance equity in obtaining healthcare services, through measuring and visualizing the spatial accessibility of community healthcare centers (CHC), and optimizing CHC geospatial allocation. We used the number of health technicians per 10,000 to represent the CHC's service capacity, combined with resident points and census data to calculate the population the CHC needs to carry, and then analyzed the accessibility based on the Gaussian two‐step floating catchment area method. In 2020, five regions in Shenzhen had better spatial accessibility scores: Nanshan (0.250), Luohu (0.246), Futian (0.244), Dapeng (0.226), and Yantian (0.196). The spatial accessibility of CHCs shows a gradual decrease from the city center to the edge, which is affected by economic and topographic factors. With the support of the maximal covering location problem model, we selected up to 567 candidate locations for the new CHC, which could improve Shenzhen's accessibility score from 0.189 to 0.361 and increase the coverage population by 63.46% within a 15‐min impedance. By introducing spatial techniques and maps, this study provides (a) new evidence for promoting equitable access to primary healthcare services in Shenzhen and (b) a foundation for improving the accessibility of public service facilities in other areas.
Keywords: primary health care, spatial accessibility, Gaussian two‐step floating catchment area, location optimization
Key Points
The problem of unbalanced allocation of primary healthcare resources is gradually emerging
Shenzhen residents have unequal access to primary healthcare within 15‐min
Economic and topographic factors affect the inequity of access to primary healthcare in Shenzhen
1. Introduction
China has striven to improve its healthcare system by continuously reforming its health system and improving the quality of medical care (X. Li et al., 2017; L. Li & Fu, 2017). Consequently, during the past decade, the overall public health of the Chinese population has improved significantly, with more than 95% of its citizens covered by the health insurance system. In addition, people are living longer because of access to more affordable and higher‐quality healthcare services. However, despite these laudable achievements, distance and time are also important barriers hindering people's access to healthcare services (Song et al., 2022). People face long travel times to healthcare facilities when they are sick and seeking healthcare (Weiss et al., 2020). China is a vast country characterized by considerable regional differences. In general, rural and remote China are disadvantaged in the allocation of healthcare resources because of their underdeveloped economies and unfavorable geographic locations (C. Yang et al., 2022; Yip et al., 2019). However, the cost of healthcare facilities can also be heavy in densely populated cities as some areas lack sufficient health infrastructure, creating challenges for better healthy living across communities (J. Chen et al., 2021; C. Li & Wang, 2022; J. Shi et al., 2020; Zhao et al., 2020).
The seventh census report of China showed that the national population was 1.44 billion in 2020 (including Hong Kong, Macao, and Taiwan). Compared to the sixth census in 2010, the population grew by 5.38% (National Bureau of Statistics, 2021). As the largest developing country in the world, the challenge of providing health services to 1.44 billion citizens is huge. In China, medical institutions are grouped in a 3‐tier system (Figure 1). According to the severity of a patient's condition and the difficulty of treatment, medical institutions at different levels are responsible for treating different diseases. Primary health institutions (PHIs) provide general healthcare and preventive care services to the community. Secondary hospitals provide comprehensive health services to a region, taking in referrals from primary hospitals, and undertaking teaching and research. Finally, tertiary hospitals, typically located in urban cities, are responsible for specialist care and serve as medical hubs for multiple regions (Lu et al., 2019). Primary health institutions consist of community healthcare centers (CHC) (CHCs) in urban areas and township healthcare centers in rural areas. As the basic unit in the 3‐tier system, the PHI provides basic clinical care and public health services, playing an important role in achieving universal health coverage. Evidence shows that adequate allocation of PHIs can reduce the risk associated with disease (X. Wang et al., 2018; H. H. X. Wang & Wang, 2012). During the peak of the COVID‐19 pandemic, many CHCs set up fever clinics, which greatly reduced the strain on medical resources and the treatment burden of high‐level hospitals (Yan et al., 2022; Yong et al., 2021).
Figure 1.
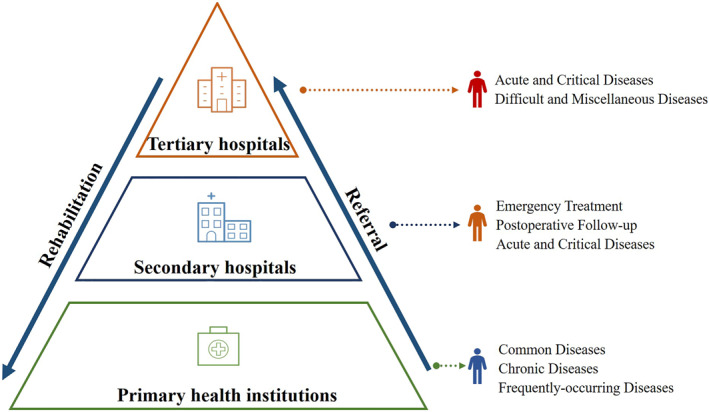
The 3‐tier hospital grouping system in China.
Spatial accessibility has become an important part of the Chinese health policy framework (Cheng et al., 2012; Delamater et al., 2012; Onega et al., 2008). In recent years, China has strived to reduce people's barriers to health services and proposed that all residents can access healthcare institutions within 15‐min to ensure equitable delivery of healthcare services (Moreno et al., 2021; Weng et al., 2019). Equitable healthcare services refer to whether residents have equal access to medical institutions, which provides the basis for the quantitative expression of this concept, and makes it directly visible on a spatial scale (X. Shi & Wang. 2016). One possible way to reduce these barriers is to measure accessibility in access to healthcare services and thus optimize the locations of healthcare facilities. Traditional economic measures for the equity in health services include the Gini coefficient, Theil index, and Concentration index (W. Liu et al., 2016; Zhou et al., 2015). However, economic measures have shortcomings as the spatial location information cannot be taken into consideration by them. With the development of Geographic Information Science, network analysis (Lang et al., 2016), cost‐weighted distance (Verma & Dash, 2020), gravity model (N. Yang et al., 2016), and two‐step floating catchment area (2SFCA) (Gu et al., 2019) have been introduced to measure the spatial accessibility of healthcare services by estimating the time for traveling to healthcare facilities. Both the gravity model and 2SFCA own a great advantage in considering characteristics of supply and demand, while 2SFCA shows superiority in data collection and analysis, thus being more commonly used (X. Shi & Wang, 2016). Related researchers use 2SFCA to identify the discrete or clustered allocation of healthcare services, after taking the spatial barriers into account, and evaluating the equity in healthcare services within a specific context or a particularly populated region (Jia et al., 2022; N. Yang et al., 2021). Optimizing the spatial distribution of healthcare institutions can improve accessibility in disadvantaged areas. Usually, the main optimization principles for healthcare institutions are to minimize travel costs (distance or time) and the number of service institutions and to maximize the service population (M. Li et al., 2022; F. Wang & Tang, 2013). The previous research has provided references for evaluating equity in healthcare services on method selection, model optimization, and spatial analysis; however, there still needs to be further discussion on factors affecting spatial accessibility and how to reduce spatial barriers to improve equity in healthcare services.
Shenzhen was the first special economic zone established in China and has developed into one of its megacities (with a resident population greater than 10 million). The seventh census of Shenzhen reported that the resident population in 2020 was 17.49 million (excluding Shenzhen‐Shanwei Special Cooperation Zone), with an urbanization rate of 99.54%. Compared to the sixth census, the resident population increased by 68.46%, with an average annual growth rate of 5.35% (Shenzhen Bureau of Statistics, 2021a). As Shenzhen's population continues to grow, the problem of unbalanced allocation of primary healthcare resources is gradually emerging. Based on the standards of PHIs and the urbanization rate of Shenzhen, we believe that CHC could represent the primary healthcare capacity in Shenzhen. In 2020, Shenzhen had 670 CHCs, and according to Shenzhen's healthcare development plan, the city plans to increase this number by up to 1,000 by 2025 (Shenzhen Health Commission, 2016). In recent years, initial efforts have been made to explore the accessibility of healthcare institutions in Shenzhen. However, they have mainly focused on general hospitals, and few have considered the distribution of CHCs (Tao et al., 2020; Wu et al., 2022). In addition, health workforce capacity has not been specifically considered in previous studies on the spatial accessibility of primary healthcare institutions. To fill this research gap, this study aimed to reduce barriers between CHCs and residents, thus enhancing spatial equity in the primary healthcare services of Shenzhen.
This study had two objectives. The first was to examine the current accessibility of Shenzhen's CHCs within 15‐min. The second was to optimize the allocation of Shenzhen's CHCs. To achieve these research objectives, we first chose the number of health technicians per 10,000 people as the service capacity of the CHC (supply) and calculated the population that the CHC needs to cater to (demand) by combining residential points with census data. We then used the Gaussian two‐step floating catchment area method to calculate the accessibility scores of the PHIs. Finally, we adopted the maximal covering location problem model to optimize the spatial location of Shenzhen's PHIs. We hope that the results of this study for the Shenzhen health sector will promote equity in access to primary healthcare services.
2. Data and Methods
2.1. Study Area
Shenzhen is located in the Pearl River Delta of China and belongs to Guangdong province, which is also an important part of the Guangdong‐Hongkong‐Macao Greater Bay Area (Figure 2). The city area of Shenzhen is 1,997.47 km2. In 2020, Shenzhen was divided into 11 administrative districts (Shenzhen Bureau of Statistics, 2021b). As we focused on the major urban area of Shenzhen, we did not include Shenzhen‐Shanwei Special Cooperation Zone in this study. Shenzhen is dominated by mountainous and hilly areas—a topographic feature that is high in the southeast and low in the northwest. The city's distribution of population and road networks is significantly influenced by its topography. Shenzhen's gross domestic product (GDP) in 2020 was CNY 2.77 trillion, accounting for 24.91% of Guangdong's GDP (Shenzhen Bureau of Statistics, 2021b). For 10 districts in Shenzhen, the rank of GDP per capita (ten thousand CNY) in 2020 was Nanshan (36.21), Yantian (30.72), Futian (30.61), Dapeng (21.78), Luohu (20.77), Pingshan (14.53), Longgang (11.92), Guangming (10.05), Longhua (9.86), and Baoan (8.59) (Shenzhen Bureau of Statistics, 2021b).
Figure 2.
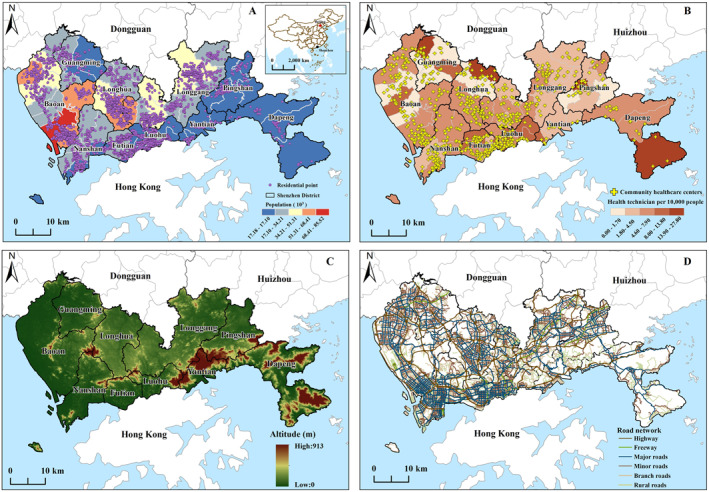
Geographical location of Shenzhen. (a) The distribution of population and residential points, (b) The distribution of the community healthcare centers and health technicians, (c) The characteristics of topography, and (d) The distribution of road networks.
2.2. Data
The population of Shenzhen in 2020 was obtained from the Worldpop data set (https://hub.worldpop.org/geodata/summary?id=49730), and the spatial resolution is 100 m. To reduce the impact of spatial resolution errors, we corrected the WorldPop data based on the correction coefficient, which was calculated using the town‐scale population ratio between the seventh census of Shenzhen and WorldPop. Residential points were collected from the points of interest (POI) of the Gaode Map (https://lbs.amap.com/api/webservice/guide/api/newpoisearch), including business residential, villa, and dormitory POI. With the guarantee that a single POI has unique attributes, we obtained 3,797 residential points (Figure 2a). However, we obtained the population of individual POIs by performing a density calculation, which can satisfy the requirement of calculating accessibility based on the relationship between supply and demand.
Information on the CHC was provided by the Shenzhen Health Development Research and Data Management Center. The data set includes the location of Shenzhen's CHCs from 2016 to 2020 and the number of their healthcare workforce (Figure 2b).
Topographic and remote sensing images could provide a basis for further analyzing the accessibility of CHCs in Shenzhen. The remote sensing image was taken by Landsat 8 in 2021. Both types of data were obtained from the geospatial data cloud constructed by the Chinese Academy of Sciences (https://lbs.amap.com/api/webservice/guide/api/newpoisearch), with a spatial resolution of 30 m (Figure 2c). Road networks were obtained from the Open Street Map (https://www.openstreetmap.org/relation/3464353), including highways, freeways, major roads, minor roads, branch roads, and rural roads (Figure 2d). The speed of different types of roads is shown in Table 1, and was set according to the code for the design of urban road engineering in China (CJJ37‐2012), as well as relevant research (J. Luo et al., 2018; Tong et al., 2021).
Table 1.
Speed of Different Road Types in Shenzhen
| Type | Driving time (km/hr) |
|---|---|
| Highway | 75 |
| Freeway | 45 |
| Major roads | 30 |
| Minor roads | 20 |
| Branch roads | 5 |
| Rural roads | 30 |
2.3. Gaussian Two‐Step Floating Catchment Area
This study was based on the analysis of supply and demand characteristics and adopted the Gaussian two‐step floating catchment area (Ga2SFCA) method to calculate the accessibility score of Shenzhen's CHCs within 15‐min. Supply was expressed as the service capacity of healthcare institutions. The healthcare workforce is one of the most important components of the Chinese healthcare sector (Zhu et al., 2018). In the Chinese health workforce system (Table S1 in Supporting Information S1), health technicians occupy a central position and can be classified as licensed doctors, registered nurses, pharmacists, and technicians. Considering that the CHC provides basic health services and the importance of health technicians in the Chinese healthcare sector, we used the number of health technicians per 10,000 people as the Shenzhen CHC supply. In addition, demand represents the number of services that the CHC needs to carry, and we combined the POI with census data to form the appropriate demand assessment.
The two‐step floating catchment area (2SFCA) method has been widely used to analyze accessibility to healthcare institutions (L. Liu et al., 2022; Mcgrail & Humphreys, 2014; S. Zhang et al., 2021). The 2SFCA method considers the accessibility barrier to healthcare institutions (W. Luo & Wang. 2003; Radke & Mu. 2000) and identifies the available facilities within the search threshold, from both supply (healthcare institutions) and demand (residents or patients) perspectives. The 2SFCA method is easy to comprehend and operate, offering the possibility of various forms of expansion. The main forms are enhanced 2SFCA, gravity 2SFCA, kernel density 2SFCA, and Gaussian 2SFCA (Dai, 2011; Polzin et al., 2014; X. Wang et al., 2018; W. Luo et al., 2020). Gaussian 2SFCA (Ga2SFCA) considers the characteristics of population decay with distance through the Gaussian function (Dai, 2010, 2011) and is most commonly used in calculating the accessibility score of public service facilities (Tong et al., 2021; F. Zhang et al., 2019). In this study, we also used Ga2SFCA to calculate the accessibility score of Shenzhen's CHCs and improved this method based on data sources, descriptions of results, and the calculation of travel costs. When calculating the cost of residents accessing CHC, we replaced the distance cost with the time cost, allowing residents to use different transportation modes (driving or taking a car) to reach a CHC. Ga2SFCA was calculated as follows:
In the first step, taking each CHC (j) as the center, the search area (m) was created with the radius of limited time () for people accessing to the CHC and the population of residential point (k) within m was counted. Considering the objectives of this study, was defined as 15 min. The Gaussian function was introduced to make the population conform to the distance decay rule. Summing the decayed population, the supply demand ratio in m (R j ) was calculated.
| (1) |
where P k is the population of k within m, is the travel time between k and j, S j is the number of supplies in j, and G (, ) is the spatial friction decay function, expressed as:
| (2) |
In the second step, taking each residential point (i) as the center, search area n was also established with the radius of the limited travel time (), and the supply demand ratio (R j ) of PHI(j) within n was summed, after being assigned a weight by the Gaussian function. Therefore, the accessibility () of residential point i based on time cost T can be obtained. A larger indicates better CHC accessibility.
| (3) |
To better show the spatial differences in accessibility scores and to construct the 15‐min living zones in Shenzhen, we constructed a hexagonal grid, which could reduce sample bias during data analysis, and introduced the natural break method (Text S1 in Supporting Information S1) to further analyze the accessibility results (Kang et al., 2020). Furthermore, the radius was defined by the maximum walkable distance within 15‐min (1 km).
2.4. Maximal Covering Location Problem Model
The optimal allocation of healthcare resources is accomplished by adding new institutions (F. Wang & Tang, 2013) and adjusting health technicians (F. Wang et al., 2015). These processes often use location‐allocation models, such as the p‐median, location set covering, and maximal covering location problems (Murray, 2016; Yong et al., 2021). The maximum covering location problem (MCLP) model aims to optimize the distribution of a few facilities to serve the maximum population and be applicable in the optimal assessment of healthcare institutions (X. Shi & Wang. 2016). Therefore, this study was based on the principles of maximizing the service population and using the MCLP model to optimize the spatial distribution of Shenzhen's CHCs. The mathematical form of the MCLP is as follows (Polo et al., 2015):
| (4) |
subject to:
where maximum is the objective function and is the demand weight coefficient. I is the set of residential points, and J is the set of facility points. The constraint determines when facility point (j) is available and selected, residential point (i) must be covered. When = 1, i receives medical services, = 0 otherwise. When = 1, j is selected, when = 0 otherwise. p denotes the total number of CHCs to be located.
3. Results
3.1. Descriptive Statistics
Table 2 shows the supply and demand of Shenzhen's CHCs in 2020. In 2020, Shenzhen had 670 CHCs, an increase of 77 from 2016. Regarding supply, in 2020, the number of health technicians per 10,000 people in Shenzhen CHC was 5.94. During the same period, the number of community health technicians per 10,000 people in Beijing, Shanghai, and Guangzhou was 15.33, 12.97, and 6.03, respectively (National Health Commission of China, 2022). Compared to a city with the same population as Shenzhen, the allocation of primary health technicians in Shenzhen is inadequate. The city also suffers from spatial equity problems caused by the unbalanced allocation of healthcare resources within the area.
Table 2.
Supply and Demand of Shenzhen's Community Healthcare Centers in 2020 (per 10,000 People)
| District | Population/million | GDP per capita/ten thousand CNY | Residential points/pcs | Community healthcare center/pcs | Health technicians | Licensed doctors | Registered nurses |
|---|---|---|---|---|---|---|---|
| Nanshan | 1.80 | 36.21 | 416 | 78 | 5.07 | 2.32 | 2.18 |
| Dapeng | 0.16 | 21.78 | 72 | 19 | 8.58 | 3.97 | 3.65 |
| Pingshan | 0.55 | 14.53 | 133 | 35 | 6.71 | 2.99 | 2.50 |
| Longhua | 2.53 | 9.86 | 518 | 72 | 6.29 | 3.07 | 2.14 |
| Guangming | 1.10 | 10.05 | 223 | 45 | 6.72 | 3.33 | 2.13 |
| Bao'an | 4.48 | 8.59 | 845 | 137 | 5.02 | 2.62 | 1.62 |
| Futian | 1.55 | 30.61 | 365 | 83 | 7.98 | 3.80 | 3.27 |
| Luohu | 1.14 | 20.77 | 340 | 55 | 9.04 | 3.58 | 3.35 |
| Yantian | 0.21 | 30.72 | 87 | 12 | 5.88 | 3.17 | 2.29 |
| Longgang | 3.98 | 11.92 | 798 | 134 | 5.16 | 2.68 | 1.92 |
In 2020, Bao'an, Longgang, Futian, and Nanshan accounted for the higher proportion of the total CHC in Shenzhen, at about 20.45%, 20.00%, 12.39%, and 11.64%, respectively, while Yantian, Dapeng, and Pingshan accounted for 1.79%, 2.84%, and 5.22% of the total CHC, respectively. Among the five types of health technician allocations, Luohu was significantly better than the other districts (Table 2). The number of health technicians per 10,000 people was relatively high in Luohu (9.04), Dapeng (8.58), and Futian (7.98). Fewer areas were found in Longgang (5.16), Nanshan (5.07), and Bao'an (5.02). Figure 2b shows the spatial distributions of CHC and town‐level health technicians. Dapeng (3.97), Futian (3.80), Luohu (3.58), Guangming (3.33), and Yantian (3.17) had considerably higher number of licensed doctors per 10,000 people than the other districts (Figure S1 in Supporting Information S1).
Regarding demand, the population of Shenzhen showed a continuous growth trend, mainly in the northwestern part of the city. Specifically, Bao'an, Longgang, and Longhua, with 4.48 million, 3.98 million, and 2.53 million people, accounted for 22.25%, 21.02%, and 13.65% of residential points, respectively. The populations of Luohu, Futian, and Nanshan districts, which developed earlier in Shenzhen, were 1.14 million, 1.55 million, and 1.80 million in 2020, with residential point shares of 8.95%, 9.61%, and 10.96%, respectively. The demand for healthcare services in Dapeng was significantly lower than that in the other districts.
3.2. Spatial Accessibility Evaluation of Shenzhen
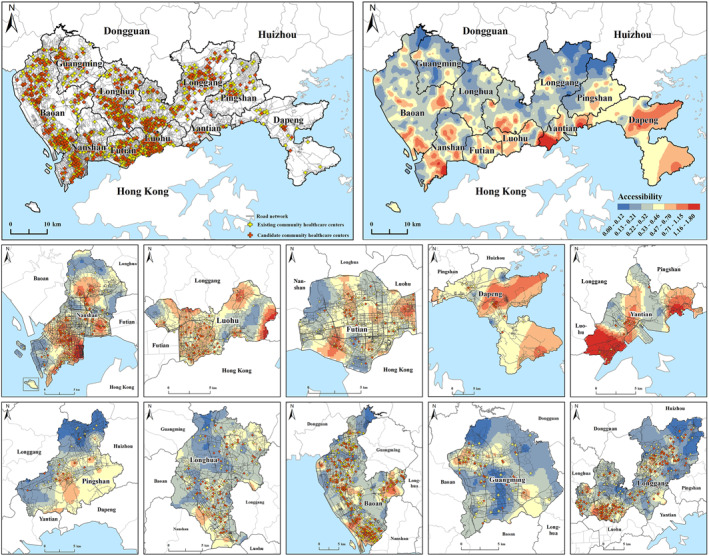
With the natural break method, the accessibility results can be divided into seven levels (Figure 3). The accessibility score of the Shenzhen CHC was 0.189 in 2020, with hotspots prominent in northeastern Nanshan, southwestern Futian, and southeastern Yantian. The Luohu hotspot was not as significant as the above districts; however, the overall accessibility was well balanced. There were widespread cold spots and poor accessibility in northeastern Longgang, north‐central Yantian, and western Bao'an. The five districts with the best accessibility scores were Nanshan (0.250), Luohu (0.246), Futian (0.244), Dapeng (0.226), and Yantian (0.196). The accessibility score of Pingshan was 0.192, whereas Longhua, Baoan, Longgang, and Guangming were below Shenzhen's average accessibility. We assume that the accessibility score was related to Shenzhen's internal economic strength, and the correlation analysis between GDP per capita and CHC accessibility score verifies this assumption (Table S2 in Supporting Information S1), there was a significant correlation between them (R 2 = 0.583, p < 0.01). In addition, licensed doctors play a critical role in healthcare resources (Zhu et al., 2020), we also illustrated the accessibility with the number of licensed doctors per 10,000 people as the CHC supply in Figure S2 in Supporting Information S1.
Figure 3.
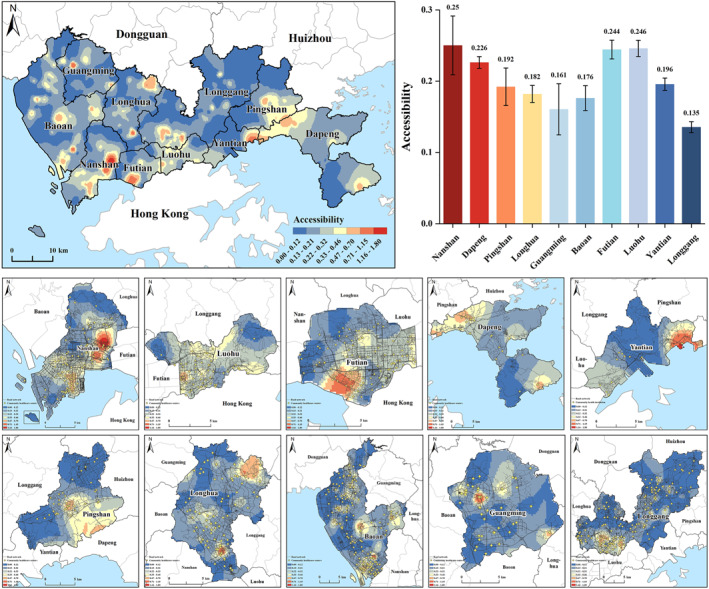
Accessibility analysis of Shenzhen's community healthcare centers with health technicians as the supply.
3.3. Primary Healthcare Within the 15‐Min Living Zones
In Shenzhen, we constructed a total of 890 living zones, and Figure 4 shows the statistics of the accessibility results. The results show that the accessibility of Shenzhen CHCs was clustered at 0.13–0.21 and 0.22–0.32 levels, with 35.62% and 23.93% living zones, including 32.82% and 26.39% residential points, affecting 17.12% and 11.33% of the population within a 15‐min impedance, respectively. In addition, 2.25% of 15‐min living zones had better accessibility scores (0.71–1.80), including 13.11% of residential points and 0.75% of the population (Table 3).
Figure 4.
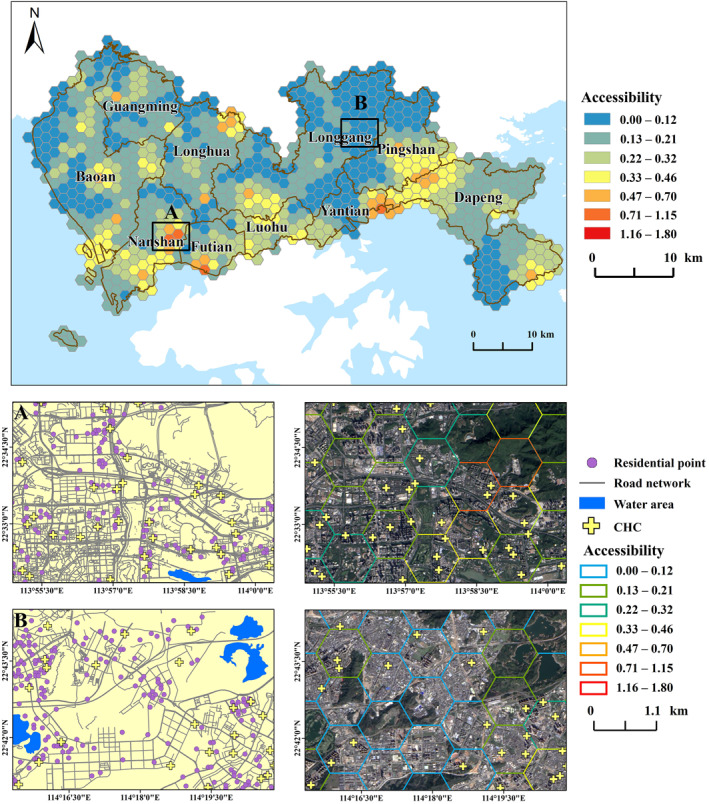
Accessibility of Shenzhen's community healthcare centers within the 15‐min living zones.
Table 3.
The Statistics and Classification of Shenzhen's Community Healthcare Centers Accessibility in the 15‐Minute Living Zones
| Accessibility | Number of living zones | Proportion of living zones (%) | Number of residential points | Proportion of residential point (%) | Population/million | Proportion of total population (%) |
|---|---|---|---|---|---|---|
| 0.00–0.12 | 174 | 19.55 | 465 | 12.25 | 1.35 | 7.72 |
| 0.13–0.21 | 317 | 35.62 | 1,246 | 32.82 | 2.99 | 17.10 |
| 0.22–0.32 | 213 | 23.93 | 1,002 | 26.39 | 1.98 | 11.32 |
| 0.33–0.46 | 121 | 13.60 | 718 | 18.91 | 1.14 | 6.52 |
| 0.47–0.70 | 45 | 5.06 | 272 | 7.16 | 0.37 | 2.12 |
| 0.71–1.15 | 10 | 1.12 | 44 | 1.16 | 0.06 | 0.34 |
| 1.16–1.80 | 10 | 1.12 | 50 | 1.32 | 0.07 | 0.40 |
Note. The statistics of the population and their proportion were counted with 15‐min impedance.
We further analyzed the obvious cold and hot spots of the CHC accessibility score in Shenzhen. By overlying the distribution characteristics of geographic elements, we obtained the factors that could influence CHC accessibility results. The northeastern part of Nanshan had a large number of CHCs and dense road networks. There were 2–3 CHCs in each 15‐min living zone that provided healthcare services to the residents, which reduced their travel cost; thus, its accessibility score was higher than those of other districts (Figure 4a). Conversely, the Yantian, Longgang, and Pingshan border areas had weak access to CHCs. Their distribution of geographical elements meant that there were fewer CHCs in these areas compared to northeastern Nanshan. Additionally, these areas were significantly affected by topography and had a scarce road network, resulting in higher costs for residents to access healthcare services (Figure 4b).
3.4. Location Optimization
Based on the MCLP model, the existing Shenzhen CHCs can ensure that 1,844 residential points, or approximately 22.66% of the population, can access healthcare services within 15‐min. Considering the current shortage of CHCs in Shenzhen and lack of an alternative institution that may be upgraded to a CHC, we suggest improving spatial accessibility by adding new institutions. We combined the spatial accessibility results, remote sensing images, and current residential points to establish 2,360 candidate locations for Shenzhen to construct the new CHC. We took the existing 670 CHCs in Shenzhen as the required facilities and added varying numbers of new CHCs. The results showed that as the number of new CHCs increased, the number of covered residential points also increased (Table 4). After the addition of 50, 150, 250, and 350 CHCs, the number of covered residential points increased by 54.23%, 58.91%, 61.55%, and 64.18%, respectively. The existing CHCs combined with the candidate CHC proposed in this study could cover a maximum population of approximately 86.12%.
Table 4.
The Community Healthcare Centers Coverage Capacity for Different Numbers of New Primary Health Institutions
| Number of CHC increase | Proportion of covered residential points (%) | Growth rate of covered residential points (%) | Average of residential points covered by candidate CHC |
|---|---|---|---|
| 50 | 54.23 | 10.82 | 4.38 |
| 150 | 58.91 | 20.40 | 2.83 |
| 250 | 61.55 | 25.78 | 2.10 |
| 350 | 64.18 | 31.16 | 1.79 |
| 450 | 65.42 | 33.69 | 2.27 |
| 550 | 65.42 | 33.69 | 2.46 |
Note. The change in the CHC's coverage capacity of the residential points were counted with 15‐min impedance.
The healthcare development target for Shenzhen was to build 1,237 CHCs by 2020. However, 45.84% of that goal has not been reached. To fill this gap, we adopted the MCLP model to select 567 optimal candidate locations for constructing new CHCs, whose coordinates are listed in Table S3 in Supporting Information S1. We assigned the average number of health technicians per 10,000 people in Shenzhen to the 567 CHCs and carried out an accessibility analysis after optimizing the CHC allocation. The Shenzhen accessibility score increased to 0.361, which was 0.16 higher than that of the existing CHCs. The districts with the greatest changes in accessibility scores were Yantian, Dapeng, and Luohu, which increased by 0.478, 0.311, and 0.212, respectively, compared to the existing CHC accessibility scores (Figure 5). In the process of effectively improving CHC spatial accessibility, the districts that needed the largest number of new CHCs were Baoan (143), Longgang (127), Longhua (73), Nanshan (66), Luohu and Futian (45). After optimization, the number of CHCs in these six districts was 280, 261, 145, 144, 100, and 128 respectively. Compared to the number of existing CHCs, Yantian, Longhua, and Baoan need to construct more CHCs. For Dapeng, Pingshan, and Guangming, the number of CHCs increased by 9, 14, and 29 after location optimization (Table S4 and Figure S3 in Supporting Information S1).
Figure 5.
Accessibility of Shenzhen community healthcare centers after adding the new institutions.
4. Discussion
Considering the importance of CHC for achieving equity in health service delivery, we calculated the CHC accessibility score of Shenzhen from the supply and demand aspects and visualized the results on the maps. Based on the accessibility results of the CHC, we optimized the geospatial allocation in Shenzhen. The inequity in access to primary healthcare services within 15‐min for Shenzhen residents is a pressing problem that needs to be addressed in the healthcare development of the area.
Shenzhen residents have unequal access to primary healthcare within 15‐min. This is due to the unbalanced allocation of health technicians and population across Shenzhen districts and the changing variations in CHC spatial accessibility. Based on the seventh census data, Shenzhen's population was concentrated in Bao'an, Longgang, Longhua, and Nanshan, which is related to the urban development process of Shenzhen. Shenzhen's urban expansion and population center have shifted to the northwestern part of the city since 1978 (Fei & Zhao, 2019; Hu et al., 2019). Combined with the statistical results of the Shenzhen CHC in 2020, the number of health technicians per 10,000 people was relatively high in Luohu (9.04), Dapeng (8.58), Futian (7.98), and Guangming (6.72). Ga2SFCA provided methodology support for calculating the CHC accessibility score in Shenzhen (Dai, 2010, 2011). In this study, we used the number of health technicians per 10,000 people as the CHC service capacity (supply), which is related to the service capacity of primary healthcare. The accessibility score of the Shenzhen CHC was 0.189, showing a gradual decrease from the center to the edge of Shenzhen. This result is similar to that of related studies (Hu et al., 2019).
Economic (GDP per capita, road networks) and natural (topographic) factors affected the inequity of access to primary healthcare in Shenzhen. There was a significant correlation between GDP per capita and Shenzhen districts' CHC accessibility score (R 2 = 0.583, p < 0.01). We also constructed 15‐min living zones and overlayed them with road networks and topography to further analyze the affected factors. The economic strength (GDP per capita) and infrastructure (road networks) of Nanshan, Futian, and Luohu—the earliest developed areas in Shenzhen—were relatively better than those of other districts. In addition, these districts had 2–3 CHCs in each 15‐min living zone to provide primary healthcare services to residents. These factors helped reduce the barrier to accessing CHCs, thus ensuring better accessibility scores. It should be noted that Dapeng received a high accessibility score because the residential points were sparsely distributed, which leads to low demand. The road networks in eastern Baoan and western Longhua were sparse, and the spatial accessibility score in these areas was relatively low. Economic factors also significantly impact the accessibility of other public institutions (Z. Liu et al., 2021; Tong et al., 2021). In Yantian, the healthcare resources (the number of CHCs and health technicians per 10,000 people) were clustered in the northeastern part; however, mountainous areas are distributed in the central part of this area, blocking intra‐regional connectivity and resulting in a sparse road network. Thus, the northeastern part was more accessible to CHCs than the southwestern part of Yantian.
Based on the accessibility analysis, we propose adding new institutions to enhance spatial equality in access to Shenzhen's CHCs within 15‐min. The process of CHC location optimization in this study was based on the MCLP model, which conforms to the constructive objective of healthcare institutions (Murray, 2016; X. Shi & Wang. 2016), and can also be used to compare accessibility before and after optimized allocation (M. Li et al., 2022). In this study, we referred to the current method of improving spatial accessibility, combined it with the healthcare development plan of Shenzhen, and optimized the allocation of CHC by adding new institutions to improve CHC accessibility within 15‐min. We calculated the coverage of residential points through the MCLP model, and found that with the increasing number of new CHCs, the coverage of residential points continued to increase; however, the growth rate of coverage decreased. We also identified 567 optimal candidate locations to construct a new CHC to fill the gap in the 2020 Shenzhen healthcare target. After optimizing the allocation of Shenzhen CHC, the percentage of residential points and the maximum population that could access primary healthcare services within 15‐min increased by 16.86% and 63.46%, respectively. After adding various numbers of CHCs in different districts, the accessibility score of the Shenzhen CHC increased to 0.36. Considering the current inadequate number of health technicians in Shenzhen, the allocation of health technicians among these CHCs should be a priority for policymakers.
This study has some limitations. First, the method used to calculate the travel cost fails to consider the timeliness and characteristics of the population. The time parameters of the 2SFCA should be based on residents' actual travel behavior for selection (Jiao et al., 2022; C. Li & Wang, 2022); however, we calculated the travel cost based on the average speed of different types of roads. On the contrary, the cost of accessing CHC services varies by population structure, such as age, gender, income, and so on, and we also need to conduct a specific travel cost analysis (Shao & Luo, 2022; F. Zhang et al., 2019).
Second, the 2SFCA expansion form needs to be considered further, and the factors that influence inequity in access to primary healthcare should be quantified. We used the most common form of Gaussian function decay in the 2SFCA method. While there are different characteristics of population decay in different public facilities, the appropriate decay function should be chosen according to the facilities' characteristics (Tao & Cheng, 2016). Based on the analysis results, the spatial accessibility of the Shenzhen CHC was affected not only by economic factors but also by topographic factors. However, the affected factors index system was inadequate, and the contribution of each factor to the accessibility score is unknown. Subsequent studies can be conducted to quantitatively analyze the more potential influencing factors through spatial statistical analysis (J. F. Wang et al., 2010, 2016).
Third, in this study, we only considered the coverage capacity of the candidate CHC for residential points within a 15‐min impedance. For the candidate CHC proposed in this study, when the added number of new institutions surpasses 450, the residential points covered by the CHC remain unchanged within the 15‐min impedance; however, the average coverage of each candidate CHC increases. The support of high‐resolution remote sensing images and more detailed primary healthcare data could provide more references for the location allocation of Shenzhen CHC on a spatial scale, thus increasing the proportion of population coverage within 15‐min (B. Y. Chen et al., 2020). Furthermore, we added the average number of health technicians per 10,000 people to the new CHC to meet the accessibility calculation requirements. Future research can investigate how to realize the health technicians' allocation of new CHC to promote equity in access to primary healthcare services for Shenzhen residents (F. Wang et al., 2015).
5. Conclusion
This study provides cogent evidence for the inequitable distribution of CHCs in Shenzhen and highlights the influence of economic and topographic factors on the distribution of CHCs. Constructing new CHCs can be an effective way to reduce the barriers that residents face in accessing general healthcare and preventive care services. Our findings may assist the government in urban planning and evidence‐based health policymaking. In the short term, adding new CHCs is suggested, aimed at different districts, by prioritizing the identified low‐accessibility area and combining it with an enhanced health workforce training system to improve the service capacity of CHCs. In the long run, the results demonstrate the significance and necessity of generating more collaborative efforts involving multiple government sectors (e.g., the health, financial, and communities) to mobilize resources to combat the unbalance distribution of CHCs. The financial sector should keep prompting the influx of government and private capital to support proprietary hospitals. A partnership between the public and private sectors in the disadvantaged districts may also prove beneficial.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supporting information
Supporting Information S1
Acknowledgments
We would like to thank the editors and reviewers for their suggestions. This study is funded by the Guangdong Basic and Applied Basic Research Foundation (2021A1515110617), Shenzhen Science and Technology Program (JCYJ20220530113208019), and Guangdong Philosophy and Social Sciences Planning Project (GD22YGL10).
Chen, L. , Zeng, H. , Wu, L. , Tian, Q. , Zhang, N. , He, R. , et al. (2023). Spatial accessibility evaluation and location optimization of primary healthcare in China: A case study of Shenzhen. GeoHealth, 7, e2022GH000753. 10.1029/2022GH000753
Data Availability Statement
The data used in this study were derived from the following resources available in the public domain: Worldpop data set at https://hub.worldpop.org/geodata/summary?id=49730; the residential points could be obtained through the API services in Gaode Map at https://lbs.amap.com/api/webservice/guide/api/newpoisearch, after defining POI types; the DEM and remote sensing data could be obtained after selecting Landsat 8 data set and DEM data set in the Geospatial Data Cloud platform at https://www.gscloud.cn/search; the road networks form Open Street Map at https://www.openstreetmap.org/relation/3464353.
References
- Chen, B. Y. , Cheng, X. P. , Kwan, M. P. , & Schwanen, T. (2020). Evaluating spatial accessibility to healthcare services under travel time uncertainty: A reliability‐based floating catchment area approach. Journal of Transport Geography, 87, 102794. 10.1016/j.jtrangeo.2020.102794 [DOI] [Google Scholar]
- Chen, J. , Lin, Z. , Li, L. A. , Li, J. , Wang, Y. , Pan, Y. , et al. (2021). Ten years of China's new healthcare reform: A longitudinal study on changes in health resources. BMC Public Health, 21, 1–13. 10.1186/s12889-021-12248-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheng, Y. , Wang, J. , & Rosenberg, M. W. (2012). Spatial access to residential care resources in Beijing, China. International Journal of Health Geographics, 11(1), 1–11. 10.1186/1476-072X-11-32 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dai, D. (2010). Black residential segregation, disparities in spatial access to health care facilities, and late‐stage breast cancer diagnosis in metropolitan Detroit. Health & Place, 16(5), 1038–1052. 10.1016/j.healthplace.2010.06.012 [DOI] [PubMed] [Google Scholar]
- Dai, D. (2011). Racial/ethnic and socioeconomic disparities in urban green space accessibility: Where to intervene? Landscape and Urban Planning, 102(4), 234–244. 10.1016/j.landurbplan.2011.05.002 [DOI] [Google Scholar]
- Delamater, P. L. , Messina, J. P. , Shortridge, A. M. , & Grady, S. C. (2012). Measuring geographic access to health care: Raster and network‐based methods. International Journal of Health Geographics, 11(1), 1–18. 10.1186/1476-072X-11-15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fei, W. , & Zhao, S. (2019). Urban land expansion in China's six megacities from 1978 to 2015. Science of the Total Environment, 664, 60–71. 10.1016/j.scitotenv.2019.02.008 [DOI] [PubMed] [Google Scholar]
- Gu, X. , Zhang, L. , Tao, S. , & Xie, B. (2019). Spatial accessibility to healthcare services in metropolitan suburbs: The case of Qingpu, Shanghai. International Journal of Environmental Research and Public Health, 16(2), 225. 10.3390/ijerph16020225 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu, W. , Li, L. , & Su, M. (2019). Spatial inequity of multi‐level healthcare services in a rapid expanding immigrant city of China: A case study of Shenzhen. International Journal of Environmental Research and Public Health, 16(18), 3441. 10.3390/ijerph16183441 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jia, P. , Wang, Y. , Yang, M. , Wang, L. , Yang, X. , Shi, X. , et al. (2022). Inequalities of spatial primary healthcare accessibility in China. Social Science & Medicine, 314, 115458. 10.1016/j.socscimed.2022.115458 [DOI] [PubMed] [Google Scholar]
- Jiao, W. , Huang, W. , & Fan, H. (2022). Evaluating spatial accessibility to healthcare services from the lens of emergency hospital visits based on floating car data. International Journal of Digital Earth, 15(1), 108–133. 10.1080/17538947.2021.2014578 [DOI] [Google Scholar]
- Kang, J. Y. , Michels, A. , Lyu, F. , Wang, S. , Agbodo, N. , Freeman, V. L. , & Wang, S. (2020). Rapidly measuring spatial accessibility of COVID‐19 healthcare resources: A case study of Illinois, USA. International Journal of Health Geographics, 19(1), 1–17. 10.1186/s12942-020-00229-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lang, W. , Radke, J. D. , Chen, T. , & Chan, E. H. (2016). Will affordability policy transcend climate change? A new lens to re‐examine equitable access to healthcare in the San Francisco Bay area. Cities, 58, 124–136. 10.1016/j.cities.2016.05.014 [DOI] [Google Scholar]
- Li, C. , & Wang, J. (2022). A hierarchical two‐step floating catchment area analysis for high‐tier hospital accessibility in an urban agglomeration region. Journal of Transport Geography, 102, 103369. 10.1016/j.jtrangeo.2022.103369 [DOI] [Google Scholar]
- Li, L. , & Fu, H. (2017). China's health care system reform: Progress and prospects. The International Journal of Health Planning and Management, 32(3), 240–253. 10.1002/hpm.2424 [DOI] [PubMed] [Google Scholar]
- Li, M. , Wang, F. , Kwan, M. P. , Chen, J. , & Wang, J. (2022). Equalizing the spatial accessibility of emergency medical services in Shanghai: A trade‐off perspective. Computers, Environment and Urban Systems, 92, 101745. 10.1016/j.compenvurbsys.2021.101745 [DOI] [Google Scholar]
- Li, X. , Lu, J. , Hu, S. , Cheng, K. K. , De Maeseneer, J. , Meng, Q. , et al. (2017). The primary health‐care system in China. The Lancet, 390(10112), 2584–2594. 10.1016/S0140-6736(17)33109-4 [DOI] [PubMed] [Google Scholar]
- Liu, L. , Yu, H. , Zhao, J. , Wu, H. , Peng, Z. , & Wang, R. (2022). Multiscale effects of multimodal public facilities accessibility on housing prices based on MGWR: A case study of Wuhan, China. ISPRS International Journal of Geo‐Information, 11(1), 57. 10.3390/ijgi11010057 [DOI] [Google Scholar]
- Liu, W. , Liu, Y. , Twum, P. , & Li, S. (2016). National equity of health resource allocation in China: Data from 2009 to 2013. International Journal for Equity in Health, 15(1), 1–8. 10.1186/s12939-016-0357-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu, Z. , Huang, Q. , & Yang, H. (2021). Supply‐demand spatial patterns of park cultural services in megalopolis area of Shenzhen, China. Ecological Indicators, 121, 107066. 10.1016/j.ecolind.2020.107066 [DOI] [Google Scholar]
- Lu, C. , Zhang, Z. , & Lan, X. (2019). Impact of China's referral reform on the equity and spatial accessibility of healthcare resources: A case study of Beijing. Social Science & Medicine, 235, 112386. 10.1016/j.socscimed.2019.112386 [DOI] [PubMed] [Google Scholar]
- Luo, J. , Chen, G. , Li, C. , Xia, B. , Sun, X. , & Chen, S. (2018). Use of an E2SFCA method to measure and analyse spatial accessibility to medical services for elderly people in Wuhan, China. International Journal of Environmental Research and Public Health, 15(7), 1503. 10.3390/ijerph15071503 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luo, W. , & Wang, F. (2003). Measures of spatial accessibility to health care in a GIS environment: Synthesis and a case study in the Chicago region. Environment and Planning B: Planning and Design, 30(6), 865–884. 10.1068/b29120 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luo, W. , Yao, J. , Mitchell, R. , & Zhang, X. (2020). Spatiotemporal access to emergency medical services in Wuhan, China: Accounting for scene and transport time intervals. International Journal of Health Geographics, 19(1), 1–14. 10.1186/s12942-020-00249-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mcgrail, M. R. , & Humphreys, J. S. (2014). Measuring spatial accessibility to primary health care services: Utilising dynamic catchment sizes. Applied Geography, 54, 182–188. 10.1016/j.apgeog.2014.08.005 [DOI] [Google Scholar]
- Moreno, C. , Allam, Z. , Chabaud, D. , Gall, C. , & Pratlong, F. (2021). Introducing the “15‐Minute City”: Sustainability, resilience and place identity in future post‐pandemic cities. Smart Cities, 4(1), 93–111. 10.3390/smartcities4010006 [DOI] [Google Scholar]
- Murray, A. T. (2016). Maximal coverage location problem: Impacts, significance, and evolution. International Regional Science Review, 39(1), 5–27. 10.1177/0160017615600222 [DOI] [Google Scholar]
- National Bureau of Statistics . (2021). The seventh 7th national census bulletin (No.2). Retrieved from http://www.stats.gov.cn/tjsj/tjgb/rkpcgb/qgrkpcgb/202106/t20210628_1818821.html
- National Health Commission of China . (2022). China health statistical yearbook 2022 (pp. 47–48). Peking Union Medical College Press. (In Chinese). [Google Scholar]
- Onega, T. , Duell, E. J. , Shi, X. , Wang, D. , Demidenko, E. , & Goodman, D. (2008). Geographic access to cancer care in the US. Cancer, 112(4), 909–918. 10.1002/cncr.23229 [DOI] [PubMed] [Google Scholar]
- Polo, G. , Acosta, C. M. , Ferreira, F. , & Dias, R. A. (2015). Location‐allocation and accessibility models for improving the spatial planning of public health services. PLoS One, 10(3), e0119190. 10.1371/journal.pone.0119190 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Polzin, P. , Borges, J. , & Coelho, A. (2014). An extended kernel density two‐step floating catchment area method to analyze access to health care. Environment and Planning B: Planning and Design, 41(4), 717–735. 10.1068/b120050p [DOI] [Google Scholar]
- Radke, J. , & Mu, L. (2000). Spatial decompositions, modeling and mapping service regions to predict access to social programs. Geographic Information Sciences, 6(2), 105–112. 10.1080/10824000009480538 [DOI] [Google Scholar]
- Shao, Y. , & Luo, W. (2022). Supply‐demand adjusted two‐steps floating catchment area (SDA‐2SFCA) model for measuring spatial access to health care. Social Science & Medicine, 296, 114727. 10.1016/j.socscimed.2022.114727 [DOI] [PubMed] [Google Scholar]
- Shenzhen Bureau of Statistics . (2021a). Shenzhen 7th national population census bulletin (No.1). Retrieved from http://www.sz.gov.cn/zwgk/zfxxgk/zfwj/bmgfxwj/content/post_8808436.html
- Shenzhen Bureau of Statistics . (2021b). Shenzhen statistical yearbook 2021. Retrieved from http://tjj.sz.gov.cn/zwgk/zfxxgkml/tjsj/tjnj/content/post_9491388.html
- Shenzhen Health Commission . (2016). Notice of public consultation on Shenzhen community health service institution setting plan (2016–2020). Retrieved from http://wjw.sz.gov.cn/gkmlpt/content/5/5559/post_5559636.html#2486
- Shi, J. , Jin, H. , Shi, L. , Chen, C. , Ge, X. , Lu, Y. , et al. (2020). The quality of primary care in community health centers: Comparison among urban, suburban and rural users in Shanghai, China. BMC Family Practice, 21(1), 1–10. 10.1186/s12875-020-01250-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shi, X. , & Wang, F. (2016). In Guan Y. (Ed.), Application of geospatial information technologies in public health (pp. 184–205). Higher Education Press. (In Chinese). [Google Scholar]
- Song, G. , He, X. , Kong, Y. , Li, K. , Song, H. , Zhai, S. , & Luo, J. (2022). Improving the spatial accessibility of community‐level healthcare service toward the ‘15‐Minute City’ goal in China. ISPRS International Journal of Geo‐Information, 11(8), 436. 10.3390/ijgi11080436 [DOI] [Google Scholar]
- Tao, Z. , & Cheng, Y. (2016). Research progress of the two‐step floating catchment area method and extensions. Progress in Geography, 35(5). (In Chinese). [Google Scholar]
- Tao, Z. , Cheng, Y. , & Liu, J. (2020). Hierarchical two‐step floating catchment area (2SFCA) method: Measuring the spatial accessibility to hierarchical healthcare facilities in Shenzhen, China. International Journal for Equity in Health, 19(1), 1–16. 10.1186/s12939-020-01280-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tong, D. , Sun, Y. , & Xie, M. (2021). Evaluation of green space accessibility based on improved Gaussian two‐step floating catchment area method: A case study of Shenzhen city, China. Progress in Geography, 40(7), 1113–1126. (In Chinese). 10.18306/dlkxjz.2021.07.004 [DOI] [Google Scholar]
- Verma, V. R. , & Dash, U. (2020). Geographical accessibility and spatial coverage modelling of public health care network in rural and remote India. PLoS One, 15(10), e0239326. 10.1371/journal.pone.0239326 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang, F. , Fu, C. , & Shi, X. (2015). Planning towards maximum equality in accessibility of NCI Cancer Centers in the US. Spatial Analysis in Health Geography, 261–274. [Google Scholar]
- Wang, F. , & Tang, Q. (2013). Planning toward equal accessibility to services: A quadratic programming approach. Environment and Planning B: Planning and Design, 40(2), 195–212. 10.1068/b37096 [DOI] [Google Scholar]
- Wang, H. H. X. , & Wang, J. J. (2012). Effects of community‐based general practitioners‐led care for 12,864 patients with hypertension: Study of cardiovascular risk intervention‐hypertension (SCRI‐HTN) in China. European Heart Journal, 33(Sup 1), 762–763. [Google Scholar]
- Wang, J. F. , Li, X. H. , Christakos, G. , Liao, Y. L. , Zhang, T. , Gu, X. , & Zheng, X. Y. (2010). Geographical detectors‐based health risk assessment and its application in the neural tube defects study of the Heshun Region, China. International Journal of Geographical Information Science, 24(1), 107–127. 10.1080/13658810802443457 [DOI] [Google Scholar]
- Wang, J. F. , Zhang, T. L. , & Fu, B. J. (2016). A measure of spatial stratified heterogeneity. Ecological Indicators, 67, 250–256. 10.1016/j.ecolind.2016.02.052 [DOI] [Google Scholar]
- Wang, X. , Yang, H. , Duan, Z. , & Pan, J. (2018). Spatial accessibility of primary health care in China: A case study in Sichuan Province. Social Science & Medicine, 209, 14–24. 10.1016/j.socscimed.2018.05.023 [DOI] [PubMed] [Google Scholar]
- Weiss, D. J. , Nelson, A. , Vargas‐Ruiz, C. A. , Gligorić, K. , Bavadekar, S. , Gabrilovich, E. , et al. (2020). Global maps of travel time to healthcare facilities. Nature Medicine, 26(12), 1835–1838. 10.1038/s41591-020-1059-1 [DOI] [PubMed] [Google Scholar]
- Weng, M. , Ding, N. , Li, J. , Jin, X. , Xiao, H. , He, Z. , & Su, S. (2019). The 15‐minute walkable neighborhoods: Measurement, social inequalities and implications for building healthy communities in urban China. Journal of Transport & Health, 13, 259–273. 10.1016/j.jth.2019.05.005 [DOI] [Google Scholar]
- Wu, J. , Fu, J. , Wang, H. , Zhao, Y. , & Yi, T. (2022). Identifying spatial matching between the supply and demand of medical resource and accessing carrying capacity: A case study of Shenzhen, China. International Journal of Environmental Research and Public Health, 19(4), 2354. 10.3390/ijerph19042354 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yan, Y. Y. , Ge, J. L. , Fan, T. Y. , Wang, H. T. , Gu, Y. F. , Xiao, X. , & Sun, X. M. (2022). Tasks of COVID‐19 prevention and control management teams at primary health care facilities in mainland China: A nationwide online cross‐sectional survey. BMC Primary Care, 23(1), 110. 10.1186/s12875-022-01703-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yang, C. , Cui, D. , Yin, S. , Yang, Y. , Ke, X. , Teng, C. , et al. (2022). Fiscal autonomy of subnational governments and equity in healthcare resource allocation: Evidence from China. Frontiers in Public Health, 10, 989625. 10.21203/rs.3.rs-1765344/v1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yang, N. , Chen, S. , Hu, W. , Wu, Z. , & Chao, Y. (2016). Spatial distribution balance analysis of hospitals in Wuhan. International Journal of Environmental Research and Public Health, 13(10), 971. 10.3390/ijerph13100971 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yang, N. , Shen, L. , Shu, T. , Liao, S. , Peng, Y. , & Wang, J. (2021). An integrative method for analyzing spatial accessibility in the hierarchical diagnosis and treatment system in China. Social Science & Medicine, 270, 113656. 10.1016/j.socscimed.2020.113656 [DOI] [PubMed] [Google Scholar]
- Yip, W. , Fu, H. , Chen, A. T. , Zhai, T. , Jian, W. , Xu, R. , et al. (2019). 10 years of health‐care reform in China: Progress and gaps in universal health coverage. The Lancet, 394(10204), 1192–1204. 10.1016/S0140-6736(19)32136-1 [DOI] [PubMed] [Google Scholar]
- Yong, Q. , Liu, D. , Li, G. , Wu, W. , Sun, W. , & Liu, S. (2021). Reducing exposure to COVID‐19 by improving access to fever clinics: An empirical research of the Shenzhen area empirical research of the Shenzhen area of China. BMC Health Services Research, 21(1), 1–10. 10.1186/s12913-021-06831-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang, F. , Li, D. , Ahrentzen, S. , & Zhang, J. (2019). Assessing spatial disparities of accessibility to community‐based service resources for Chinese older adults based on travel behavior: A city‐wide study of Nanjing, China. Habitat International, 88, 101984. 10.1016/j.habitatint.2019.05.003 [DOI] [Google Scholar]
- Zhang, S. , Song, X. , & Zhou, J. (2021). An equity and efficiency integrated grid‐to‐level 2SFCA approach: Spatial accessibility of multilevel healthcare. International Journal for Equity in Health, 20(1), 1–14. 10.1186/s12939-021-01553-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhao, P. , Li, S. , & Liu, D. (2020). Unequable spatial accessibility to hospitals in developing megacities: New evidence from Beijing. Health & Place, 65, 102406. 10.1016/j.healthplace.2020.102406 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhou, K. , Zhang, X. , Ding, Y. , Wang, D. , Lu, Z. , & Yu, M. (2015). Inequality trends of health workforce in different stages of medical system reform (1985–2011) in China. Human Resources for Health, 13(1), 1–8. 10.1186/s12960-015-0089-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhu, B. , Fu, Y. , Liu, J. , He, R. , Zhang, N. , & Mao, Y. (2018). Detecting the priority areas for health workforce allocation with LISA functions: An empirical analysis for China. BMC Health Services Research, 18(1), 1–14. 10.1186/s12913-018-3737-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhu, B. , Hsieh, C. W. , & Mao, Y. (2020). Spatio‐temporal variations of licensed doctor distribution in China: Measuring and mapping disparities. BMC Health Services Research, 20(1), 1–16. 10.1186/s12913-020-4992-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting Information S1
Data Availability Statement
The data used in this study were derived from the following resources available in the public domain: Worldpop data set at https://hub.worldpop.org/geodata/summary?id=49730; the residential points could be obtained through the API services in Gaode Map at https://lbs.amap.com/api/webservice/guide/api/newpoisearch, after defining POI types; the DEM and remote sensing data could be obtained after selecting Landsat 8 data set and DEM data set in the Geospatial Data Cloud platform at https://www.gscloud.cn/search; the road networks form Open Street Map at https://www.openstreetmap.org/relation/3464353.