

Abstract
This study uses individual level consumer trace data for 2006 residents of low- and moderate-income neighborhoods for the principal cities of the 100 largest metropolitan regions in the US using their location in 2006 and 2019 to examine exposure to the following four cSDOH: healthcare access (Medically Underserved Areas), socioeconomic condition (Area Deprivation Index), air pollution (NO2, PM 2.5 and PM10), and walkability (National Walkability Index). The results control for individual characteristics and initial neighborhood conditions. Residents of neighborhoods classified as gentrifying were exposed to more favorable cSDOH as of 2006 relative to residents of low- and moderate-income neighborhoods that were not gentrifying in terms of likelihood to be in a MUA, and level of local deprivation and walkability while experiencing similar level of air pollution. As a result of changes in neighborhood characteristics and differential mobility pattern, between 2006 and 2019, individuals who originally lived in gentrifying neighborhoods experienced worse changes in MUAs, ADI, and Walkability Index but a greater improvement in exposure to air pollutants. The negative changes are driven by movers, while stayers actually experience a relative improvement in MUAs and ADI and larger improvements in exposure to air pollutants. The findings indicate that gentrification may contribute to health disparities through changes in exposure to cSDOH through mobility to communities with worse cSDOH among residents of gentrifying neighborhoods although results in terms of exposure to health pollutants are mixed.
Keywords: gentrification, contextual social determinants of health, mobility
JEL: R11, R21, R23
Introduction
The health and well-being of residents of gentrifying areas is an area of growing research and policy attention (Gibbons et al. 2018; Schnake-Mahl et al. 2020; Smith et al. 2020). Gentrification can be defined as the process through which communities with relatively low- and moderate-incomes experience a rapid rise in their relative socioeconomic position. Gentrification affects housing affordability for both owners and renters leading to potential constrained outmigration. There is evidence of both endogenous changes in factors such as improved green spaces that may affect health in gentrifying neighborhoods differently for residents with varying socioeconomic status (Cole et al. 2019; Pearsall and Eller 2020) and of changes in neighborhood environment for residents who move out of gentrifying neighborhoods (Brummet and Reed 2019). There is also strong evidence of disparities in terms of health outcomes and contextual (i.e., area level) social determinants of health (cSDOH) across communities (Diez Roux and Mair 2010; Braveman et al. 2011; Braveman and Gottlieb 2014). The main contribution of the present study is to provide evidence of the contribution of mobility to changes in contextual exposures using information about origins and destinations for a large sample of movers.
This study analyses cSDOH for residents of gentrifiable neighborhoods, defined as low- and moderate-income tracts with household median income below 80 percent of the metropolitan region median income, as of 2000. It uses their location in 2006 and 2019 in consumer trace data to examine how residing in neighborhoods categorized as gentrifying between 2000 and 2019 and the resulting different mobility patterns of residents lead to changes in exposure to selected cSDOH for residents of gentrifying tracts relative to residents of tracts that are not gentrifying in the principal cities of the largest 100 metropolitan regions. We focus on the following four key types of cSDOH that have been shown to contribute to disparities in health outcomes (Diez Roux and Mair 2010; Schnake-Mahl et al. 2020; Smith et al. 2020) and for which measures are available nationwide: healthcare access, socioeconomic condition, air pollution, and walkability.
The findings show that while gentrifying neighborhoods tend to have cSDOH that are more favorable than other low- and moderate- income households, however, mobility patterns in gentrifying neighborhoods lead to worsen cSDOH exposure. These findings indicate that changes in exposure to cSDOH may be a pathway through which gentrification can affect health disparities.
Section I reviews the evidence on the connection between gentrification and changes in exposure to social determinants of health. Section II presents the consumer trace data used in this paper along with the measures of cSDOH and the analytic model. Section III reports the findings of worse changes in terms of healthcare access, socioeconomic condition, and walkability for residents of gentrifying neighborhoods and mixed findings in terms of exposure to air pollution. Section IV discusses the implication for research on the link between gentrification and health.
I. Background: Gentrification relationship to social determinants of health through residential mobility and changes to built and social environment
a). Place and health: the importance of contextual social determinants of health
The impact of neighborhoods on health is well-established along with the effect of differences in residential environments on social and racial/ethnic inequities in health (Diez Roux and Mair 2010; Braveman et al. 2011; Braveman and Gottlieb 2014) including specifically in the context of gentrification (Gibbons et al. 2018; Schnake-Mahl et al. 2020; Smith et al. 2020). Analysis from the National Center for Health Statistics for the 2010–2015 period shows that life expectancy can vary greatly across small areas (Arias et al. 2018). In Philadelphia, for example, life expectancy at birth varies from 70 in the lower income and not gentrifying neighborhood of Greys Ferry, to 76 in gentrifying Point Breeze, to 84 in the higher income neighborhood of Fitler Square (Robert Wood Johnson Foundation 2021). This represents a 14-year range in life expectancy in neighborhoods that are located within less than 1.5 miles of each other.
There is extensive research on how differences in the neighborhood environment impact health outcomes (Diez Roux and Mair 2010; Braveman et al. 2011). The natural, built and social environment in which individuals reside impacts their health outcomes both directly through increased exposure to pollutants, or more costly (financially and in time) access to health services or physical activity and indirectly by affecting behaviors in health promoting or deleterious ways. We adopt the term of contextual social determinants of health (cSDOH) to refer to these place-based SDOH that operate through the residential environment to which individuals are exposed.
Key cSDOH that have been identified and analyzed in the literature include pollution, access to green spaces, neighborhood deprivation, crime, smoking and drinking behaviors, and access to health care with evidence of negative impact on a range of health outcomes including chronic diseases (specifically obesity and related risk factors and outcomes like heart diseases and diabetes) and mental health (specifically depression). (Diez Roux and Mair 2010; Braveman et al. 2011; Brown et al. 2016; Duncan et al. 2012; Gentili et al. 2015; Schnake-Mahl et al. 2017; 2020; Scribner et al. 2017; Shi et al. 1990; Wen et al. 2013). These place-based factors are often correlated with each other, with the same neighborhoods having high levels of deprivation as captured through an Area Deprivation Index (ADI) also having high levels of crime and limited access to healthy food. Given the lack of data available at neighborhood level for some of these indicators, the ADI can serve as a proxy for overall neighborhood condition, but direct measures of crime or health deleterious behaviors at small geographies deserve further studies.
The impact of other cSDOH, such as social capital or availability of healthy food options, also have conceptual grounding (Carpiano 2006) and suggestive but still uncertain empirical evidence of impact on health outcomes (Ahnquist et al. 2012; Braveman et al. 2011; Braveman and Gottlieb 2014; Carlson and Chamberlain 2003; Diez Roux and Mair 2010) despite potential important relationship with gentrification. In particular, with regards to social capital, measures of social cohesion based on willingness, belonging and trust developed through survey responses (Gibbons and Barton 2016) have been shown to be associated with positive reported health outcomes. Such measures would be helpful given that gentrification has been linked to changes in social cohesion (Gibbons and Barton 2016; Schnake-Mahl et al. 2020) but are not available at neighborhood level nationwide.
There is well-established evidence of inequality in exposure to cSDOH based on individual sociodemographic characteristics with lower income individuals experiencing substantially worse cSDOH, and minority households more likely to experience worse cSDOH as well (Diez Roux and Mair 2010; Braveman et al. 2011; Gentili et al. 2015; Schnake-Mahl et al. 2017). In particular there is evidence of worse access to health care (Streeter et al. 2020), air pollution (Kravitz-Wirtz et al. 2016; Liu et al. 2021), and walkability (Duncan et al. 2012) in low- and moderate-income neighborhoods. In addition, there is evidence that migration patterns can further exacerbate environmental inequality when examining exposure to industrial hazard (Crowder and Downey 2010; Pais et al. 2014).
In this study, we focus on key cSDOH that have been shown to directly affect mental and physical health outcomes and contribute to socioeconomic and racial/ethnic health disparities (Diez Roux and Mair 2010; Schnake-Mahl et al. 2020; Smith et al. 2020). Based on recent reviews of the literature on the relationship between gentrification and health (Cole 2020; Firth et al. 2020; Gibbons et al. 2018; Schnake-Mahl et al. 2020; Smith et al. 2020), we selected cSDOH that operate based on place of residence and for which adequate measures of proxy can be obtained nationwide.
b). Gentrification and health
Empirical evidence has linked gentrification to increased health disparities. Within the wider literature on cSDOH, the role of gentrification is an area of recent attention (Cole 2020; Firth et al. 2020; Gibbons et al. 2018; Schnake-Mahl et al. 2020; Smith et al. 2020). The increased attention to the relationship between gentrification and health has coincided with a rise in the share of low- and moderate-income neighborhoods that experience gentrification in the 2000s and 2010s (Martin 2017). It also marks the increasing recognition that social forces like structural racism that result in residential segregation and are reinforced by spatial separation shape household access to neighborhoods in ways that contribute to exacerbate health disparities associated with individual characteristics (Acevedo-Garcia et al. 2003; Williams and Collins 2016).
Gentrification may contribute to health disparities through increased housing instability with displaced residents at higher risk of losing social connections and being exposed to more deleterious neighborhood environments (Schnake-Mahl et al. 2020, Smith et al. 2020; Bhavsar et al. 2020; Cole 2020; Firth et al. 2020; Gibbon et al. 2018). Gentrification has potentially beneficial impacts on the health outcomes of long-term residents who remain in their neighborhood through increased public and private investments that lead to improvements in neighborhood physical and social environments. The literature finds evidence of increased green space quantity and quality, health promoting retail environments and services, and reductions in crime in gentrifying neighborhoods (Smith et al. 2020). On the other hand, gentrification may negatively impact the wellbeing and health of the original residents, more likely to be people of color, through increases in housing cost burden (resulting in trade-offs on expenditures for basic goods and services such as food and healthcare) and changes to the physical and social environment leading to loss of community (Hwang and Lin 2016; Smith et al. 2020). Renters on fixed incomes (elderly or disabled) are particularly at risk of displacement (Hwang and Lin 2016). Smith et al. (2020) find that people of color in gentrifying neighborhoods are more likely to experience negative residential and health outcomes. The same processes of structural racism that maintain health disparities may also lead people of color to experience greater worsening in cSDOH, in response to gentrification. An analysis of individual data for California finds that Black residents of gentrifying neighborhoods experienced increased levels of fair/poor self-rated health, but the same difference was not found for other racial/ethnic groups (Izenberg et al. 2018). Using national data from the CDC’s 500 Cities project, another study finds a positive association between levels of recent gentrification and self-rated health of neighborhood residents but significantly higher rates of poor self-rated health in gentrified tracts with larger Black and Hispanic populations (Gibbons et al. 2018). These studies are limited by the fact that they focus on residents remaining in, or moving to, gentrifying neighborhoods, and their inability to explore health outcomes for former residents of gentrified neighborhoods. To date, we have limited evidence about whether the destination neighborhoods of individuals who leave gentrifying neighborhoods have different characteristics in terms of cSDOH that could result in greater exposure to health-enhancing or deleterious environments.
c). Measuring gentrification and its impact on residential trajectories
A challenge of the literature on the impact of gentrification has been to agree on definitions of gentrification. The extant research has developed different definitions of gentrification that can be derived from available census data at the neighborhood level (using census tracts) such as changes in resident socioeconomic characteristics (proxied by income and educational attainment) and local housing costs (generally rent) relative to costs in the broader metropolitan region (Bhavsar et al. 2020; Firth et al. 2020; Brummet and Reed 2019; Dragan et al. 2020; Johnson et al. 2021; Preis et al. 2021). Alternative measures have been proposed that rely on the participation of local communities, attempting to incorporate dimensions such as loss of cultural anchors, and displacement risk (Bhavsar et al. 2020; Firth et al. 2020). Given the national scale of this study we rely on definitions that can be produced based on census data. We follow the existing literature and rely on existing definitions that have been implemented for large national sample of metropolitan areas based on changes in educational attainment, income and rent at the tract level (Brummet and Reed 2019; Dragan et al. 2020), acknowledging how various definitions lead to different sets of neighborhoods being categorized as gentrifiable, gentrifying or gentrified with sometimes limited overlap (Preis et al. 2021). The variation in which neighborhoods are classified as gentrifying is not only a measurement issue but has implications for agreeing on the magnitude of the phenomenon of gentrification and what neighborhoods are affected.
Recent research has shown that while most low- and moderate-income tracts are not gentrifying, the pace of gentrification has accelerated over the last decades in cities across the US increasing the relevance of its potential impacts on health (Brummet and Reed 2019; Ding et al. 2015; Dragan et al. 2020; Maciag 2015; Martin 2017). Martin (2017) find that the share of neighborhoods classified as gentrifying increased from 3.5 percent between 1980 and 1990 to 7.1 percent between 2000 and 2010 under a strict definition of gentrification.
The increased prevalence of gentrification in urban centers reflects the increased demand for central locations by higher income households with higher levels of education (Brummet and Reed 2019; Couture and Handbury 2020; Su 2018). In some regions, the increased demand for centrally located neighborhoods that have good access to employment and consumption amenities results in increased housing costs that lead to mobility out of those neighborhoods by long term residents who cannot afford the new rents or the increased property taxes (Ding and Hwang 2016). In many other cities, disinvestment in central neighborhoods continues to be the main challenge, particularly in legacy cities (Brophy 2016).
Some progress has recently been made in establishing mobility patterns for gentrifying neighborhoods but important debates remain about the prevalence and magnitude of displacement, defined as forced move out of gentrifying neighborhoods. Existing quantitative research on gentrification has focused on estimating whether gentrification leads to higher levels of mobility (Brummet and Reed 2019; Ding et al. 2016; Dragan et al. 2020) and how gentrification affects household welfare (Couture et al. 2019; Su 2018) with a particular focus on children outcomes (Brummet and Reed 2019; Dragan et al. 2019).
The link between gentrification and displacement, defined as constrained moves that force residents to move out of their original community into other neighborhoods, is a source of major concerns for community organizations and policy makers as well as to researchers (Brummet and Reed 2021; Gibbons and Barton 2017). The hypothesized link between gentrification and displacement is supported by the fact that a defining feature of gentrification is an increase in housing costs that would lead households who cannot afford these costs to move to more affordable neighborhoods. However, empirical evidence has failed to produce estimates of high levels of increased mobility, including outmigration as a result of gentrification (Brummet and Reed 2019; Ding et al. 2016). The evidence to date suggests that gentrification has a moderate to nonexistent impact on overall mobility, including mobility out of gentrifying neighborhoods (Brummet and Reed 2019; Ding et al. 2016; Dragan et al. 2020). However, when residents of gentrifying neighborhoods do move, they tend to migrate longer distances than similar residents in non-gentrifying neighborhoods, a process that may be indicative of displacement (Brummet and Reed 2019).
Whether gentrification causes substantially higher levels of residential mobility is still an unsettled question but might reflect the overall high level of residential mobility (or instability) among low- and moderate-income households and the high level of neighborhood migration, with gentrification forces only marginally worsening levels of mobility but resulting in different forms of mobility as a result of the displacement nature of the moves. Displacement and the strains associated with the fear of displacement have been tied to negative mental and physical health outcomes (Fullilove 1996; 2016; Manzo 2003; Gibbons and Barton 2017). Even if gentrification does not cause higher mobility beyond the already high level of mobility experienced by residents of low- and moderate-income neighborhoods, original residents of gentrifying neighborhoods might still experience worse outcomes in terms of cSDOH when they move if their destination neighborhood has less desirable characteristics than their neighborhood of origin. The issues of 1) whether gentrification results in higher levels of mobility and 2) whether displacement through gentrification results in changes in exposure to cSDOH are both unsettled.
In terms of changes in environment there is evidence that adults and children who are able to stay in gentrifying neighborhoods experience some improvements in terms of economic opportunity (Brummet and Reed 2019) and health outcomes (Dragan et al. 2019) but that those who move experience negative outcomes such as longer commutes and negative health outcomes (Dragan et al. 2019; Lim et al. 2017). Dragan et al. (2019) look at health outcomes of children enrolled in Medicaid in New York City and do not find an overall effect of experiencing gentrification on health system use or diagnoses of asthma and obesity but find a moderate increase in diagnoses of anxiety and depression. Lim et al. (2017), also in New York City, look at emergency visits and hospitalization and find higher likelihood among movers relative to those who remained, mainly due to mental health issues.
Among studies looking at the outcomes of gentrification on original residents, Brummet and Reed (2019) are able to produce robust population level estimates using restricted-access census microdata from the 2000 decennial and the 2010–2014 ACS to examine the potential impact of gentrification on intergenerational economic mobility in the top-100 metropolitan areas. These data allow the authors to identify mobility for a large and representative sample but their analysis focuses on economic opportunity and does not include cSDOH measures.
The findings from the other studies rely on large trace data: Medicaid Data for New York City for Dragan et al. (2020) and credit data from the FRBNY Consumer Credit Panel/Equifax (CCP) data for Ding et al. (2016). The consumer data used in this study is another source of trace data that has been used to examine migration (Phillips 2020). Trace data allow researchers to obtain detailed location information for a broad number of individuals but that information is an outcome of regular operations such as the operation of the Medicaid program or establishing credit profile for the consumer credit panel and are not collected for research purposes. The location signal associated with the address of the individuals in these databases is valuable to identify mobility, but external validity is limited by the data coverage and the source ability to link individual records over time. This study benefits from the fact that the consumer trace data are mostly used for mail advertising purposes and accurate mailing information is therefore a key feature of the dataset. In addition, it includes a broader range of households than credit data by including households that may lack credit activity.
II. Data and Methods
We use individual-level consumer data with high spatial specificity (with geographic coordinates corresponding to addresses) provided by Data Axle for the period 2006–2019 and block-group level measures of cSDOH in the US 100 largest metropolitan regions. This allows us to examine how gentrification affects exposure to key cSDOH known to contribute to social and racial/ethnic disparities in health outcomes through differences in mobility patterns for residents of low- and moderate-income neighborhoods that are gentrifying or not. Table 1 summarizes the variables used in the study.
Table 1:
Key Variables
| Key Variable | Definition | Geographic Level | Source |
|---|---|---|---|
| Outcomes | |||
| Medically Underserved Areas | Categorical (0=No, 1=Yes) variable at tract level defining Medically Underserved Areas (MUA), 2006–2019. | Census Tract | HRSA |
| Social Deprivation | Area deprivation index (ADI): percentile at state and national level based on 17 variables capturing income, education, employment, occupation, housing costs and tenure, household composition and housing condition, summarized using principal components analysis for 2000 and 2015–2019. | Blockgroup | 2000 Census and 2015–2019 ACS |
| Air pollution | Continuous annual-average estimates of outdoor concentrations for three pollutants (NO2, PM10, and PM2.5) at blockgroup level, 2006–2015. | Blockgroup | CACES |
| Walkability | National walkability index score (expressed as percentile from least to most walkable) calculated in 2019 based on measures of the built environment that affect the probability of whether people walk as a mode of transportation: street intersection density, proximity to transit stops, and diversity of land uses. | Blockgroup | EPA |
| Individual Controls | Age, household size, tenure, race and ethnicity, length of residence. | Individual | Data Axle |
| Contextual Controls | Tract median income, poverty (%), homeownership (%), white non-Hispanic residents (%), adults with college degree (%), households that moved within last year (%), median house value and median gross rent, vacancy rate, distance from the tract centroid to the city center. As of 2000. | Census Tract | 2000 Census |
A). Consumer Trace Data: 2006–2019 location for residents of low- and moderate-income households in the 100 largest metropolitan regions as of 2006
Consumer trace data such as the Data Axle data has recently emerged as a source of data to measure mobility for research purposes (Phillips 2020; Mast 2019; Mast et al. 2021). Data Axle is one of the main vendors of consumer trace data along with LexisNexis and Infutor and this data has been shown to produce reliable population and migration estimates. The Data Axle database is assembled from a variety of current sources including credit card billing statements, utility records, voter registrations, real estate tax assessments and deed transfers, public records (bankruptcies, licenses and registrations), and mailing address changes. Data Axle clients mainly use the data to distribute targeted mail or to locate customers. To meet this need, Data Axle aims to ensure residential information is as current, accurate, and comprehensive as possible. In other words, a crucial feature of the data is the ability to contact potential customers in real-time using their residential addresses.
The data from Data Axle used in this study contain a unique and time-invariant family identifier and individual identifier for up to 5 adults in the family unit, which enables us to identify changes in location over time. This allows us to identify the origins and destinations of 5.5 million adults living in gentrifiable tracts, for the 100 largest metros as of the year 2000, including 678,000 living in gentrifying tracts. For these individuals we know their location in 2006 and 2019 along with estimated race/ethnicity, number of children, tenure, marital status, age and length of residence at current address. The dataset also includes information about household income and wealth but we chose not to include these variables in our analysis because of uncertainty on their reliability due to their modelled nature.
Prior work established the usability of the Data Axle data to produce small area demographic estimates (Acolin et al. 2021). In 2010, there were 121.5 million households in the U.S. based on the decennial census and 111.5 million households recorded in the Data Axle data. The average coverage ratio (5 year estimates based on Data Axle estimates/ACS estimates) at the tract level between 2009 and 2019 was 93%, and about 80% of tract estimates fall within 20% of the ACS estimates. In addition, when looking specifically at gentrifiable tracts, the average coverage was 85%. This is lower than for all tracts, but remains substantially higher than the coverage of low- and moderate-income tracts in credit records (Brevoort et al. 2015). While it is not possible to directly assess representativeness bias, individuals with more limited consumer traces are likely to be those with lower levels of consumption, reflecting lower income and potentially higher vulnerability to gentrification.
We also validated Data Axle-provided coordinates information by re-geocoding half a million addresses for each year. The results at the national level indicated that about 90% of Data Axle records had location information with sufficient details to be independently geocoded at address level (the rest at street of Zip Code level) and that for these records, the median distance between the regeocoded points and the Data Axle coordinates was stably between 60–62 meters and overall the performance was consistent across states. We also re-geocoded the addresses using parcel-level reference files for King County, Washington. Only 1.5% of Data Axle coordinates were more than 100 meters from the correct parcel centroid. This validation exercise demonstrated the reliability of the Data Axle location information across locations and over time.
B). Contextual Social Determinants of Health: Blockgroup measures
We use measures of cSDOH for 4 domains: healthcare access, socioeconomic condition, air pollution, and walkability. The cSDOH measures are based on well-established research in operationalizing these conceptual factors (Brown et al. 2016; Liu et al. 2021; Sass et al. 2017; Pope et al 2019; Streeter et al. 2020; Messer et al. 2006). The measures we use are available nationwide but their geographic and temporal coverage varies.
In this project, we focus on cSDOH determined by the physical (air pollution), social (neighborhood deprivation and medically underserved areas) and built environments (walkability). These allow us to examine to what extent endogenous changes in gentrifying neighborhoods characteristics (when several time periods are available) combined with mobility of original residents is associated with changes in exposure to cSDOH in ways that may reinforce disparities in exposure to health promoting or deleterious environments.
We selected key cSDOH that are expected to vary by location, including at neighborhood scales and except for walkability have been measured consistently over time. The measures we adopt have been developed, validated and used in the literature on cSDOH. Other cSDOH would be worth exploring in future research, including crime and access to healthy food for example. Whenever possible we attempt to create measures that best reflect the individual exposure, adopting the approach developed by Kwan (2009: 1312) to define measures of exposure that take “the actual spatial and temporal “configuration” of exposure into account”. We match, to the extent possible, the year in which the cSDOH is measured to the observation period. In cases where the indicators are not updated annually, or not available for the entire period we rely on the closest year.
For health care access, we use Medically Underserved Areas (MUAs), tracts or counties designated by the Health Resources and Services Administration (HRSA) as lacking access to primary care services, expressed as a binary yes or no. Areas that were designated as such in December 2006 and December 2019 are used. This provides a measure of disparity in access to care that has been shown to be associated with worse health outcomes (Brown et al. 2016; Gentili 2015).
For socioeconomic conditions, we use the Area Deprivation Index (ADI) based on a measure created by the HRSA and refined, adapted and validated by the University of Wisconsin Madison at the blockgroup level (Kind 2018). The ADI is based on 17 variables capturing income, education, employment, occupation, housing costs and tenure, household composition and housing condition and estimated using Principal Component Analysis (PCA). We use this measure estimated based on the 2000 Census and 2015–2019 ACS data and expressed as percentile at the national and state level with higher percentiles reflecting more disadvantaged neighborhoods. Higher level of neighborhood deprivation, estimated through higher ADI rank, has been linked to worse health outcomes (Hu et al. 2018; Kind et al. 2014; Lantos et al. 2018; Link and Phelan 1995; Ludwig et al. 2011). In addition to the measures including in the ADI, many other cSDOH that we are not able to include in this study (crime, food access, etc.) are likely highly correlated with ADI.
For air pollution, we use average annual outdoor concentration measures estimated for blockgroups by the Center for Air, Climate, and Energy Solutions (CACES) for three pollutants: one gas, nitrogen dioxide (NO2) expressed in parts per billion and two aerosols: particulate matter less than 10 microgram per meter cubed (PM10), particulate matter less than 2.5 microgram per meter cubed (PM2.5) from 2006 to 2015 (Kim et al. 2020). We use the 2006 and 2015 estimates. The updated measures to 2019 are not available.
For walkability, we use the National Walkability Index for blockgroup levels provided by the Environmental Protection Agency (EPA) at the blockgroup level as of 2019. The index captures characteristics of the built environment that affect the likelihood people will use walking as a mode of transportation. The transformed walkability index values represent national percentiles and range from least walkable to most walkable. The index is calculated based on street intersection density, proximity to transit stops, and diversity of land uses (defined based on employment and household mix). The National Walkability Index is only available as a one time estimate. The built environment characteristics used to build the index are likely to only change slowly, so the relative ranking of neighborhoods in 2006 and 2019 are likely very comparable. However, that means that the estimated difference between residents of gentrifying and non-gentrifying neighborhoods will come exclusively from the difference in mobility patterns between the two for movers.
C). Definition of gentrifiable and gentrifying neighborhoods
We adopt a definition of gentrification as a process through which formerly low- and moderate-income neighborhoods experience an increase in demand by higher income, higher educated households resulting in a rise in housing costs. We do not propose a new measure of gentrification but rather builds on existing rule-based measures of gentrification and applies them to classify tracts in the 100 largest metropolitan regions as of 2000. As discussed in the previous section, we acknowledge the limits of rule-based approaches that have been identified in the literature and the lack of consensus in conceptualizing and operationalizing measures of gentrification (Firth et al. 2020; Preis et al. 2021). However, given the national scale of the study and the need to have a consistent measure across metropolitan regions relying on census variables and examining the sensitivity of the results to different thresholds remained the best option. This provides a measure of gentrification defined as changes in socioeconomic characteristics that may affect original resident residential trajectories.
We follow the recent literature and define ‘gentrifiable’ neighborhoods as tracts within a metropolitan area’s central city that have median incomes less than 80% of the median income for the metropolitan area as of 2000 (Martin 2017).1 We then adapt the definition proposed by Brummet and Reed (2019) in focusing on the share of adults with college degrees and add median rent and median income. We assign the label of ‘gentrifying’ to those gentrifiable tracts that between 2000 and 2015–2019 experienced above median growth in two of the following three characteristics: the share of adults with college degrees, median rent or median income.
We chose the 2000 to 2015–2019 period to capture neighborhoods that might have started gentrifying before our first year of observation (2006) and experienced an increase in educational attainment, income and rent relative to the rest of the metropolitan region over almost two decades indicating a sustained pattern of neighborhood change.
We explored the robustness of our classifications and results to alternative measures used in the recent literature (Brummet and Reed 2019; Dragan et al. 2020; Martin 2017). In particular, we produced an alternative classification using lower levels of median income of the metropolitan area (60%) to define gentrifiable neighborhoods. We also used the central city median income instead of the metropolitan area. We also used an alternative threshold for gentrification defined as growth rate within the top 25th percentile instead of above median. In order to examine sensitivity to the beginning period we also used the 2006–2010 ACS as the starting point instead of the 2000 census. Overall, the main results are qualitatively robust to these alternative definitions of gentrifiable and gentrifying (Appendix Table 2).
D). Estimation approach
Among low- and moderate-income neighborhoods, those that gentrify have characteristics distinct from those that do not. Gentrification is not a process that occurs randomly but rather reflects increased demand for a community that is driven by its location, the characteristics of its built environment and its residents. The literature has shown that neighborhoods closer to the center of the city and with higher share of white non-Hispanic residents are more likely to gentrify (Freeman 2009). In addition, residents of low- and moderate-income neighborhoods that gentrify or not also differ on observable and likely unobservable characteristics in ways that can affect their propensity to move and levels of constraints in accessing the unit of their choice in their preferred neighborhood. Estimated gentrification effects may be biased downwards by gentrifying neighborhoods’ relatively more favorable attributes and trajectories.
Another limit to estimating the impact of gentrification on existing residents of gentrifying neighborhoods is that the Data Axle data is not a representative dataset collected to produce population level estimates. While the Data Axle data has broad coverage and we are able to link a large number of individuals between 2006 and 2019, the linked dataset does not have full population coverage and may incorporate biases that cannot be fully assessed without merging to a full population registry. The sample captures adult individuals who reside in gentrifiable tracts as of 2006 and for whom we are able to observe location in 2019. Prior research with consumer trace data has found that it underrepresents individuals with more limited consumption activity that are less likely to be represented in the database and be reliably linked over time. These include younger individuals with lower income and renters (Acolin et al. 2021; Phillips 2020; Mast 2019). In addition, Infutor, another consumer trace dataset, has been shown to substantially under measure moves relative to measures based on Census data (Mast 2019).
The direction of the bias caused by underrepresentation of vulnerable residents is difficult to assess in the context of this work. Most vulnerable residents likely constitute a higher share of residents in not gentrifying neighborhoods, but the effect of gentrification is likely to lead to worse outcomes for these residents by pushing them to potentially less desirable locations. Despite these limitations, the consumer trace data follow the location of a large number of individuals over more than a decade, allowing to examine the origin and destination context of residents of gentrifiable neighborhoods in a way that is not possible with longitudinal surveys that do not include a sufficiently large sample of households living in these communities.
The lack of exogenous shock to explain gentrification and the fact that we are not able to observe the 2019 location for all original residents are limits to identifying a causal effect of gentrification on exposure to cSDOH. At the same time, this study benefits from the well established literature aiming to estimate the impact of gentrification in the absence of experimental or quasi experimental data. In particular, the factors associated with gentrification and mobility are well established, allowing to include a robust set of control variables used in previous studies. Our empirical approach follows mainly Brummet and Reed (2019) and attempts to address selection and omitted variable concerns by including an extensive set of neighborhood controls that have been shown to be associated with gentrification. We also use an estimator developed by Oster (2017) to assess the robustness of the results to potential selection and omitted variables.
We specify the following model using OLS and probit (for MUA) estimates for individual i in tract j in CBSA m adapted from Brummet and Reed (2019):
yijmt, the dependent variable is the cSDOH measure for the location of individual i based on their location jm in either t period 0 (2006) or period 1 (2019). We run a model with the dependent variable in its original unit as reported in Table 1 and standardized using a z-score with mean 0 and standard deviation 1. Gentrify is a dummy variable capturing whether the tract of residence in the first period gentrified between 2000 and 2015–2019; Period is a dummy variable indicating whether the observation is for 2006 (period 0) or 2019 (period 1); the main coefficient of interest is for the interaction term between Gentrify and Period that estimates the change in cSDOH for individuals in gentrifying tracts relative to non-gentrifying tracts in 2006 based on the change in cSDOH (with the exception of walkability) and the change in their location in 2006 and 2019. We also run separate estimates stratifying the sample based on residents of gentrifying neighborhood who stayed in the same location (for which we are not able to produce estimates for walkability) or moved. X is a vector of variables that capture individual and household characteristics available in Data Axle: age group, race/ethnicity, marital status, number of children, length of residence at current address as of 2006 and distance from the center of the metropolitan region2; and N is a vector of variables that capture characteristics of the original neighborhood as of 2000: share of movers, share of college graduates, share of white non-Hispanic, poverty rate, median income, median rent, median house value, share of units vacant and share of occupied units owned from the decennial census. All models include CBSA fixed effects (um) and clustered standard errors at the tract level.
We also implement an estimator developed by Oster (2016) and used by Brummet and Reed (2019) in order to estimate the potential influence of remaining unobservables on differences in mobility patterns and locational outcomes by running a version of the models with only gentrification and CBSA fixed effects and then the full version of the model. The Oster estimator provides a gentrification coefficient estimate that corrects for the possible bias from remaining unobservables based on assumptions about the maximum possible R-squared and the influence of remaining unobservables relative to the influence of the included controls.3 Thus it creates bounded estimates of the potential causal impact of gentrification on mobility patterns and locational outcomes. This approach requires control variables that capture a substantial amount of observable variations. Given the well established set of individual and neighborhood controls used to explain measured cSDOH outcomes and the relatively high R-squared value for most variables, the Oster estimates can provide a helpful bound on the gentrification coefficient estimate that incorporate bias from remaining observables.
III. Results
Table 2 reports the descriptive statistics for our overall sample of individuals and broken down by not gentrifiable, gentrifying and non-gentrifying tracts. The overall sample consists of 5.5 million adults living in gentriafiable neighborhoods as of 2006 and with information about location in 2006 and 2019. Among those, as of 2006, 12.4 percent resided in neighborhoods (4,573 census tracts) classified as gentrifying. Among residents of gentrifiable tracts, about one third moved between 2006 and 2019 with a 3 percentage point higher rate among residents of gentrifying tracts relative to those of non-gentrifying tracts. Residents in gentrifying tracts are less likely to be Black/African American residents, or Hispanic/Latinx than in not gentrifying tracts (13 vs 27 percent and 11 vs 20 percent respectively) and more likely to be White non-Hispanic (56 vs 39 percent). In terms of age gentrifying tracts are younger but for both gentrifying and not gentrifying tracts younger adults in the Data Axle sample are a smaller share than in the overall population. Residents in gentrifying neighborhoods are less likely to own a home and closer to the city center. Tract level information also shows higher levels of mobility and lower rates of ownership in gentrifying tracts. However, gentrifying tracts have a higher share of adults with college degrees, higher median income, rent and house value along with lower share of poverty. This indicates that among gentrifiable neighborhoods, those classified as gentrifying between 2000 and 2019 had more favorable sociodemographic characteristics as of 2000. However, both gentrifying and not gentrifying tracts are more similar to each other than to not gentrifiable tracts in which a smaller share of residents moved and a larger share are White non-Hispanic, own, are married and further from the CBD and ACS neighborhood level characteristics indicate higher levels of educational achievements, substantially lower poverty rate and higher income, rent and house value.
Table 2:
Individual and Neighborhood Characteristics by Gentrification Status
| Not Gentrifiable | Gentrifying | Not Gentrifying | |
|---|---|---|---|
| Gentrification Status | 67.1% | 4.1% | 28.8% |
| Individual Level | |||
| Moved | 27.3% | 34.3% | 31.2% |
| Race/Ethnicity | |||
| Black or African American | 6.2% | 13.3% | 27.2% |
| Hispanic or Latinx | 11.0% | 10.9% | 19.7% |
| Other race or ethnicity | 19.6% | 19.6% | 14.4% |
| White non-Hispanic | 63.3% | 56.2% | 38.7% |
| Age Group | |||
| Less than 30 | 5.6% | 11.2% | 7.2% |
| 30–39 | 18.3% | 24.5% | 20.9% |
| 40–49 | 26.6% | 24.7% | 25.6% |
| 50–59 | 25.4% | 20.5% | 22.5% |
| 60+ | 24.2% | 19.1% | 23.6% |
| Length of Residence | 12.2 | 10.1 | 11.9 |
| Number of Children in household | 0.2 | 0.10 | 0.16 |
| Own | 76.7% | 42.8% | 53.8% |
| Married | 64.0% | 33.6% | 45.2% |
| Distance to CBD (km) | 15.7 | 9.1 | 12.3 |
| Tract Level (2000 Census) | |||
| Moved | 47.3% | 55.2% | 47.5% |
| College Degree | 43.5% | 37.3% | 18.5% |
| Poverty Rate | 7.9% | 21.9% | 25.6% |
| Median Income | 57,115 | 31,756 | 27,986 |
| Median Rent | 743 | 577 | 474 |
| Median House Value | 208,917 | 168,195 | 108,077 |
| White non-Hispanic | 66.3% | 49.5% | 29.9% |
| Vacant | 4.8% | 8.7% | 8.3% |
| Own | 65.5% | 31.5% | 40.5% |
| N | 11,176,224 | 678,493 | 4,791,436 |
Note: Characteristics based on 2006 individual level location and characteristics and 2000 level tract characteristics.
Table 3 reports the average values of the cSDOH measures overall and for individuals in not gentrifiable, gentrifying, and not gentrifying tracts based on their location in 2006 and 2019 and broken down by moving status. As of 2006, residents of gentrifying tracts face more favorable outcomes in terms of ADI, walkability and MUA. The initial differences in terms of air pollution between residents of gentrifying and not gentrifying tracts are limited. For residents of gentrifying neighborhoods as of 2006, these descriptive statistics indicate overall worsen cSDOH between 2006 and 2019 except for the share of residents in Medically Underserved Areas that experienced a slight decline and for the air pollution measures that have declined over time across the country.
Table 3:
Contextual Social Determinant of Health By Gentrifiable and Gentrifying Status
| All | Not Gentrifiable | Gentrifying | Not Gentrifying | |||
|---|---|---|---|---|---|---|
| 2006 | 2019 | 2006 | 2019 | 2006 | 2019 | |
| MUA (1=Yes) | 5.9% | 6.3% | 17.5% | 15.2% | 19.6% | 17.2% |
| ADI National Rank (percentile) | 31.6 | 31.8 | 43.7 | 45.3 | 63.5 | 58.5 |
| ADI State Rank (percentile) | 38.4 | 38.4 | 54.6 | 56.5 | 74.4 | 68.0 |
| NO2 (part per billion) | 14.8 | 9.5 | 18.6 | 12.3 | 16.5 | 11.1 |
| PM10 (microgram per meter cubed) | 23.6 | 19.8 | 24.5 | 19.2 | 24.1 | 19.7 |
| PM2.5 (microgram per meter cubed) | 11.7 | 8.4 | 12.5 | 8.9 | 12.4 | 9.0 |
| National Walkability Index (percentile) | 62.0 | 60.5 | 70.5 | 68.0 | 66.3 | 64.0 |
| Stayers | Not Gentrifiable | Gentrifying | Not Gentrifying | |||
|---|---|---|---|---|---|---|
| 2006 | 2019 | 2006 | 2019 | 2006 | 2019 | |
| MUA (1=Yes) | 6.0% | 6.4% | 18.4% | 16.7% | 20.7% | 18.9% |
| ADI National Rank (percentile) | 31.8 | 31.8 | 44.9 | 44.0 | 64.1 | 60.5 |
| ADI State Rank (percentile) | 38.1 | 37.9 | 56.1 | 55.7 | 74.4 | 69.8 |
| NO2 (part per billion) | 14.7 | 9.5 | 18.5 | 12.5 | 16.4 | 11.2 |
| PM10 (microgram per meter cubed) | 23.6 | 19.8 | 24.5 | 19.3 | 24.0 | 19.8 |
| PM2.5 (microgram per meter cubed) | 11.7 | 8.4 | 12.5 | 9.0 | 12.4 | 9.0 |
| National Walkability Index (percentile) | 61.5 | 61.5 | 70.2 | 70.2 | 66.1 | 66.1 |
| Movers | Not Gentrifiable | Gentrifying | Not Gentrifying | |||
|---|---|---|---|---|---|---|
| 2006 | 2019 | 2006 | 2019 | 2006 | 2019 | |
| MUA (1=Yes) | 5.6% | 6.3% | 12.6 | 16.2% | 17.7% | 13.7% |
| ADI National Rank (percentile) | 31.5 | 32.3 | 42.1 | 48.6 | 62.9 | 54.9 |
| ADI State Rank (percentile) | 39.1 | 39.7 | 53.4 | 58.6 | 74.3 | 64.0 |
| NO2 (part per billion) | 15.3 | 9.4 | 19.0 | 12.0 | 16.8 | 10.8 |
| PM10 (microgram per meter cubed) | 23.8 | 19.7 | 24.6 | 19.1 | 24.0 | 19.6 |
| PM2.5 (microgram per meter cubed) | 11.7 | 8.3 | 12.5 | 8.8 | 12.4 | 8.9 |
| National Walkability Index (percentile) | 63.2 | 58.4 | 70.7 | 65.0 | 66.4 | 61.2 |
Table 4, reports the coefficient of the interaction term for Gentrifying Tract*Period and Gentrifying Tract*Period*Move from the probit (MUA) and OLS estimates (the full output table is reported in Appendix Table 1). The coefficients in Panel A are interpreted as the change in a given cSDOH for individuals who as of 2006 were living in tracts classified as gentrifying relative to individuals who were living in not gentrifying tracts in 2006 based on the cSDOH measure for their location in 2006 and 2019 controlling for individual and initial tract characteristics. Panel B reports the coefficients for Z transformed outcomes and Panel C the Oster estimates.
Table 4:
Gentrification Association with cSDOH Among Original Residents
| Medically Underserved Area | ADI National Rank | ADI State Rank | Nitrogen Dioxide | PM10 | PM2.5 | National Walkability Index | |
|---|---|---|---|---|---|---|---|
| 0.015*** | 3.104*** | 3.952*** | −0.784*** | −1.020*** | −0.193*** | −1.895*** | |
| (0.003) | (0.0195) | (0.0246) | (0.0026) | (0.0036) | (0.0010) | (0.0235) | |
| N | 10,779,622 | 10,651,860 | 10,777,539 | 10,777,539 | 10,777,539 | 10,779,345 | 10,651,860 |
| R-sq or Pseudo R-sq | 0.06 | 0.29 | 0.30 | 0.67 | 0.41 | 0.81 | 0.27 |
| ADI National Rank | ADI State Rank | Nitrogen Dioxide | PM10 | PM2.5 | National Walkability Index | |
|---|---|---|---|---|---|---|
| 0.151*** | 0.179*** | −0.146*** | −0.180*** | −0.074*** | −0.060*** | |
| (0.0009) | (0.0011) | (0.0006) | (0.0008) | (0.0005) | (0.0087) | |
| N | 10,651,860 | 10,651,860 | 10,777,539 | 10,777,539 | 10,777,539 | 10,779,345 |
| R-sq or Pseudo R-sq | 0.29 | 0.30 | 0.67 | 0.41 | 0.81 | 0.27 |
| Medically Underserved Area | ADI National Rank | ADI State Rank | Nitrogen Dioxide | PM10 | PM2.5 | National Walkability Index | |
|---|---|---|---|---|---|---|---|
| 0.0192 | 5.32 | 8.553 | −0.535 | −1.042 | −0.211 | −1.051 |
Note: All results are for specifications including individual and neighborhood controls, MSA fixed effects and clustered standard error at the tract level. MUA not included in Panel B since Z score not meaningful for binary indicator.
The results for Medically Underserved Areas (MUAs) indicate a 1.5 percentage point increased chance of living in a MUA for original residents of gentrifying tracts (1.9 percentage points among movers). The average share of residents of gentrifying neighborhoods living in MUA is 17.5 percent as of 2006, so this represents a meaningful difference. This is consistent with the hypothesis that gentrification of centrally located neighborhoods leads to mobility to areas with worse access to healthcare.
The results for the Area Deprivation Index (ADI) ranking at the national and state level indicate that residents of gentrifying tracts experience a relative percentile increase of 3.9 at the national level and of 4.0 at the state level, indicating being located in relatively more deprived neighborhoods. For movers, the difference is 5.5 at both levels. The estimated coefficients are 0.2 standard deviation overall and are of similar magnitude to the difference in ADI between white non-Hispanic and Black or African American individuals. It means that while among gentrifiable tracts gentrifying tracts have generally lower ADI than not-gentrifying tracts, on average original residents of gentrifying neighborhoods experienced a relatively worsening in ADI through movers ending in neighborhoods with relatively higher ADI.
The results for the measures of air pollutants indicate an improvement for residents of gentrifying tracts in terms of exposure to NO2, PM10, PM2.5. The estimated changes are between 0.1 and 0.2 standard deviation for these measures, representing substantial improvements. These improvements may reflect moves further out from the sources of emissions located in the center of urban areas but require further investigation.
The results for the National Walkability Index indicate that original residents of gentrifying tracts lived in neighborhoods with higher levels of walkability but experienced a −1.9 percentile decrease in Walkability Index on average relative to the original residents of not-gentrifying tracts or 0.1 standard deviation. As mentioned earlier, the walkability measure is only available for a single period in time, meaning that the change is coming from movers, who may be relocating further away from the center of the region in less walkable environments.
When looking at the Oster estimates, the betas are of similar magnitude but generally slightly larger with the exception of the Nitrogen Dioxide and Walkability measure for which they are relatively smaller. The relative stability of the coefficients suggest that while selection on unobservable characteristics is likely, its impact on the estimated gentrification coefficient may be moderate and towards an underestimation of a potential causal effect.
Table 5 reports the results broken down by original residents of gentrifying neighborhoods who stayed at the same address (Panel A) or moved (Panel B) between 2006 and 2019. Movers could have moved to a home in a gentrifying, not gentrifying or not gentrifiable tract. Overall residents who stayed in gentrifying neighborhoods experienced a relative improvement in the likelihood of their neighborhood being a MUA, in their ADI ranking and exposure to air pollutants while movers experienced a relative worsening in terms of MUA and ADI but also experienced a relative improvement in terms of air pollutants (although less so than stayers). Overall, these results indicate the relatively worse outcomes for movers and the need for further research looking specifically at mover outcomes and differences across race/ethnicity, whether they own or rent and local market characteristics.
Table 5:
Gentrification Association with cSDOH Among Original Residents Stratified by Stayers and Movers
| Medically Underserved Area | ADI National Rank | ADI State Rank | Nitrogen Dioxide | PM10 | PM2.5 | National Walkability Index | |
|---|---|---|---|---|---|---|---|
| −0.004*** | −2.312*** | −1.950*** | −1.103*** | −1.108*** | −0.244*** | NA | |
| (0.0005) | (0.0266) | (0.0333) | (0.0036) | (0.0050) | (0.0015) | ||
| N | 7,422,181 | 7,337,615 | 7,337,615 | 7,420,967 | 7,420,967 | 7,420,967 | 7,421,909 |
| R-sq or Pseudo R-sq | 0.07 | 0.30 | 0.32 | 0.66 | 0.41 | 0.81 | 0.19 |
| Medically Underserved Area | ADI National Rank | ADI State Rank | Nitrogen Dioxide | PM10 | PM2.5 | National Walkability Index | |
|---|---|---|---|---|---|---|---|
| 0.019*** | 5.524*** | 5.498*** | −0.627*** | −0.964*** | −0.178*** | −1.955*** | |
| (0.0004) | (0.0209) | (0.0263) | (0.0028) | (0.0039) | (0.0011) | (0.0436) | |
| N | 3,357,441 | 3,314,245 | 3,314,245 | 3,356,572 | 3,356,572 | 3,356,572 | 3,357,278 |
| R-sq or Pseudo R-sq | 0.04 | 0.26 | 0.27 | 0.70 | 0.41 | 0.81 | 0.16 |
Note: All results are for specifications including individual and neighborhood controls, MSA fixed effects and clustered standard error at the tract level.
Appendix Table 2 reports results based on different definitions of gentrifiable and gentrifying. The magnitude is generally similar across outcomes whether using the 2006–2010 ACS data instead of the 2000 census data for the beginning period, the center city median income instead of the metropolitan region median income, 60% of AMI instead of 80% of AMI to define gentrifiable tracts and changes in the top 25th percentile instead of above median to define gentrifying tracts. The relative stability of the estimates indicates that our findings are not based on a particular definition of gentrification, although alternate definitions or variations in the magnitude of the relationship across regions are certainly worth exploring.
IV. Discussion
Among the six cSDOH measures for which we have temporal variations of original residents of gentrifiable neighborhoods, whether gentrifying or not, both movers and stayers experienced lower exposure to air pollution. On average stayers experienced an improvement in the MUA and ADI measures among both gentrifying and not gentrifying tracts. Movers from gentrifying tracts experienced a worsening in terms of MUA, ADI and in the measure that is not time varying (walkability). When looking at the interaction of gentrification and period and controlling for individual and location characteristics, we find that individuals who as of 2006 were living in neighborhoods that were classified as gentrifying experienced a relative decline in their neighborhood healthcare access, socioeconomic condition, and walkability and improvements in air pollutants between 2006 and 2019 relative to residents of low- and moderate-income neighborhoods that did not gentrify. When looking at differences for residents of gentrifying neighborhoods who moved or stayed, the main driver of the changes in healthcare access, SES and walkability appear to be differential outmigration to neighborhoods with relatively worse measures on these variables for residents of gentrifying neighborhoods. The results for air pollution reflect an overall improvement in air quality in the US over time and a decline in absolute and relative racial/ethnic exposure disparities (Liu et al. 2021). For air pollution, the relevant question is to understand why gentrifying neighborhoods see greater improvements in air quality relative to non-gentrifying areas.
The existing literature on the impact of gentrification on health finds evidence that adults and children who are able to stay in gentrifying neighborhoods experience some improvements in terms of health outcomes (Dragan et al. 2019) but that those who move experience negative health outcomes (Dragan et al. 2019; Lim et al. 2017). In addition, there are evidences of differences in relationship across racial/ethnic groups with Black residents of gentrifying neighborhoods reporting increased levels of fair/poor self-rated health in California, but the same difference was not found for other racial/ethnic groups (Izenberg et al. 2018) and gentrification in minority areas being associated with higher rates of poor self-rated health at the national level (Gibbons et al. 2018). Besides Dragan et al. (2019) and Lim et al. (2017) these studies generally focus on outcomes for residents who remain in gentrifying neighborhoods due to the difficulty to observe those who moved out. As discussed above, gentrification may have positive and negative impact on cSDOH for stayers through changes in neighborhood composition and availability of public and private goods and services. However, gentrification has been shown to be a particular source of disruption for residents that are not able to continue living in their original community and experience a loss of community. A particular concern around displacement has been about whether households end up moving to neighborhoods with worse characteristics for residents’ wellbeing and intergenerational economic mobility. Therefore, the ability to measure changes in neighborhood environments for movers is of particular interest.
The results in this paper indicate that on several dimensions gentrification seems to be associated with relatively worsening cSDOH for original residents, mostly through outmigration to neighborhoods with lower levels of cSDOH relative to the pattern for residents of gentrifiable but not gentrifying neighborhoods. When it comes to the select cSDOH examined here, individuals in gentrifying neighborhoods appear to experience a relative worsening of their position compared to similar individuals in non-gentrifying tracts over the 2006–2019 period, although not in terms of air pollutants. Examining additional cSDOH, including access to healthy food and crime is necessary to understand to what extent the relationship between gentrification and exposure to cSDOH varies across types of cSDOH and the overall impact of gentrification on health environments.
Further work is also needed to examine how these results vary for different groups of residents and different locations. More vulnerable households are more likely to experience forced moves as a result of gentrification, with renters expected to be most affected since they are more directly exposed to the impact of changes in housing costs. The impact of gentrification on locational outcomes is likely to be larger in tighter housing markets at the regional level as residents may not find adequate affordable options or have to move considerable distances but evidence on the magnitude of these differences is needed. The regional context may also interact with the impact of gentrification, particularly in regions with higher levels of segregation where neighborhood options for minority households may be further constrained. It is important to further explore these variations for understanding for whom and when gentrification may be associated with a worsening in health environments and in community health and how policies can be targeted to support households most negatively affected by gentrification. Given the relatively worse outcomes for movers, policies aimed at limiting displacement and enabling original residents to remain in their community despite gentrification forces or to move to communities with health-enhancing cSDOH could have beneficial impact on households’ health outcomes and overall wellbeing.
Figure 1:
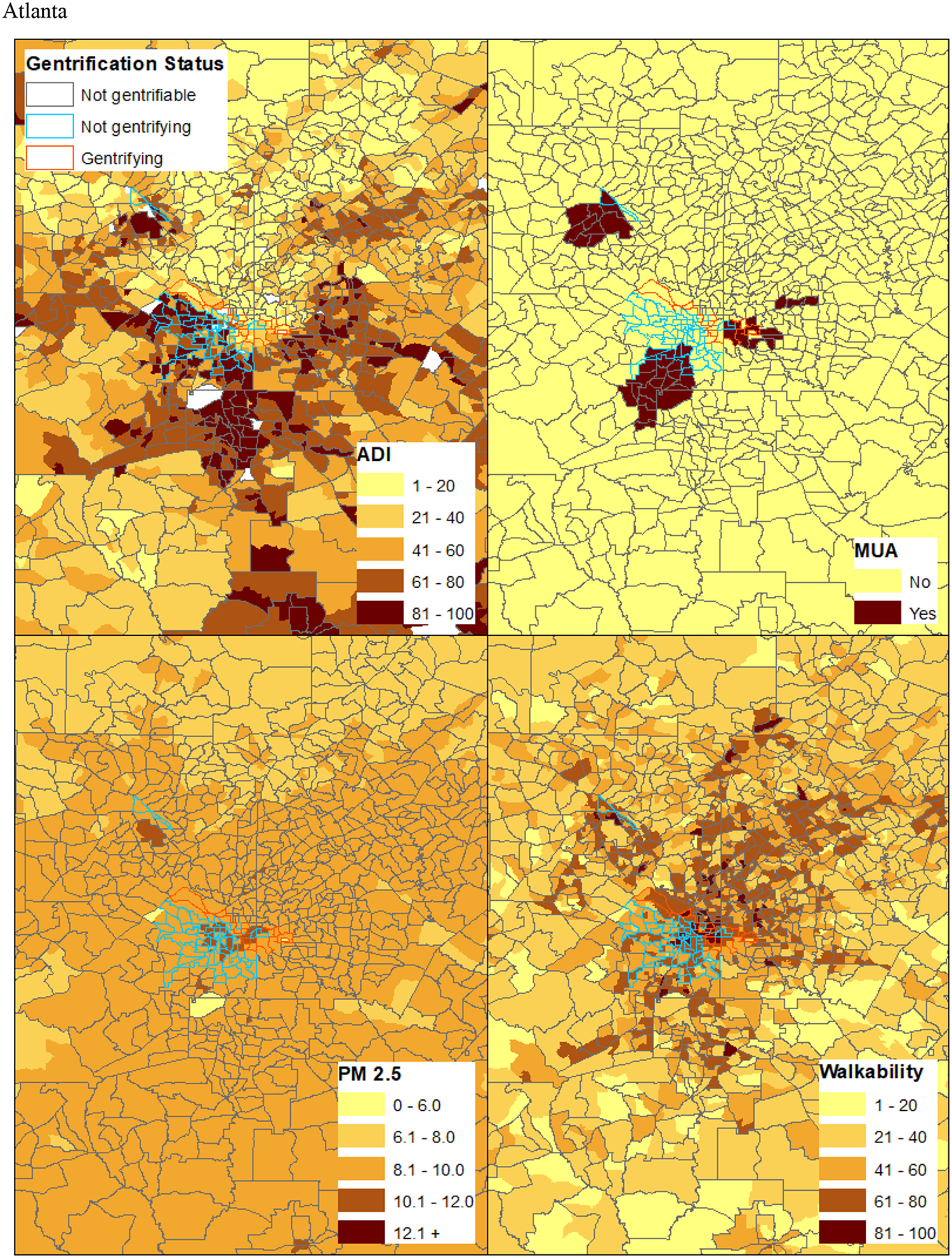
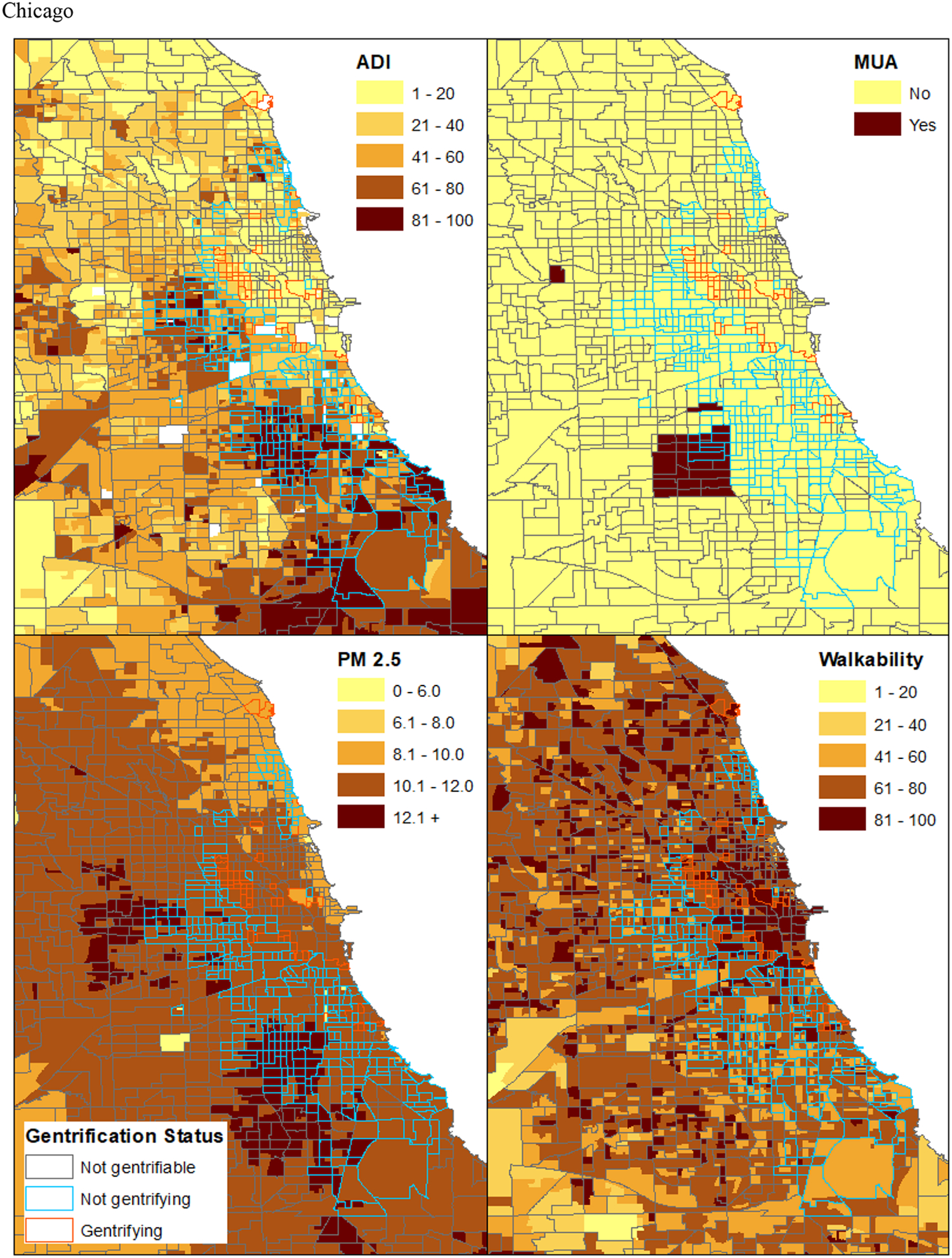
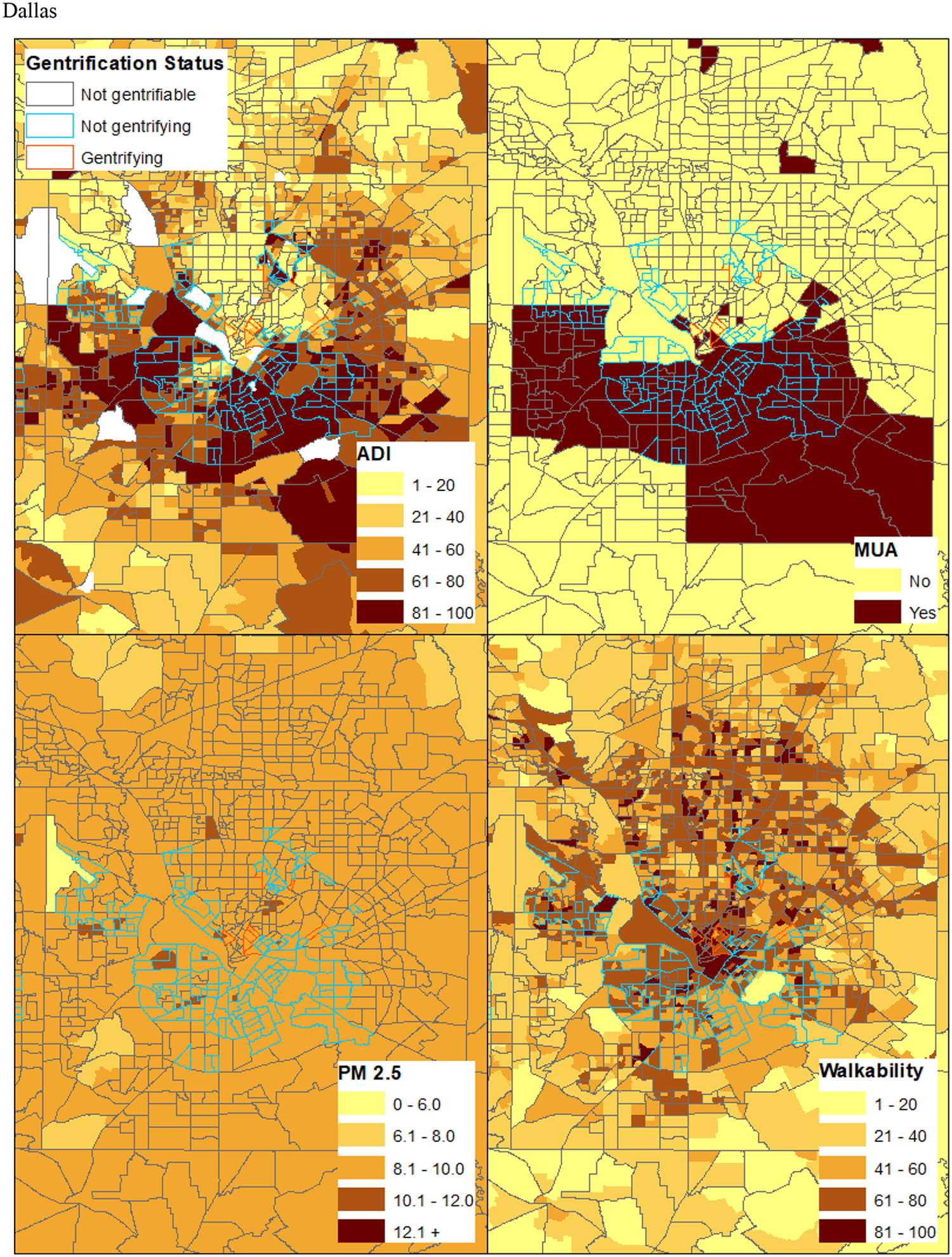
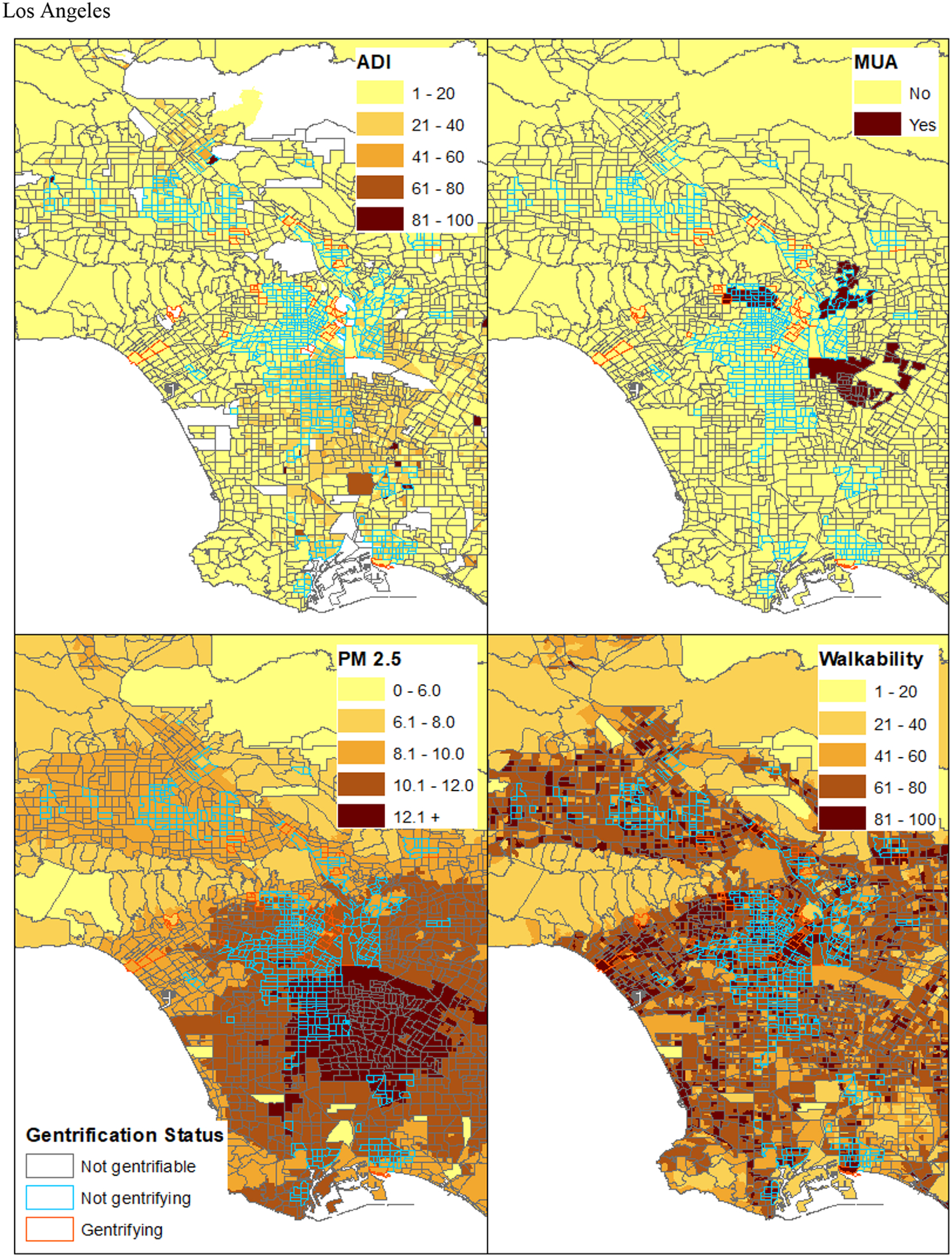
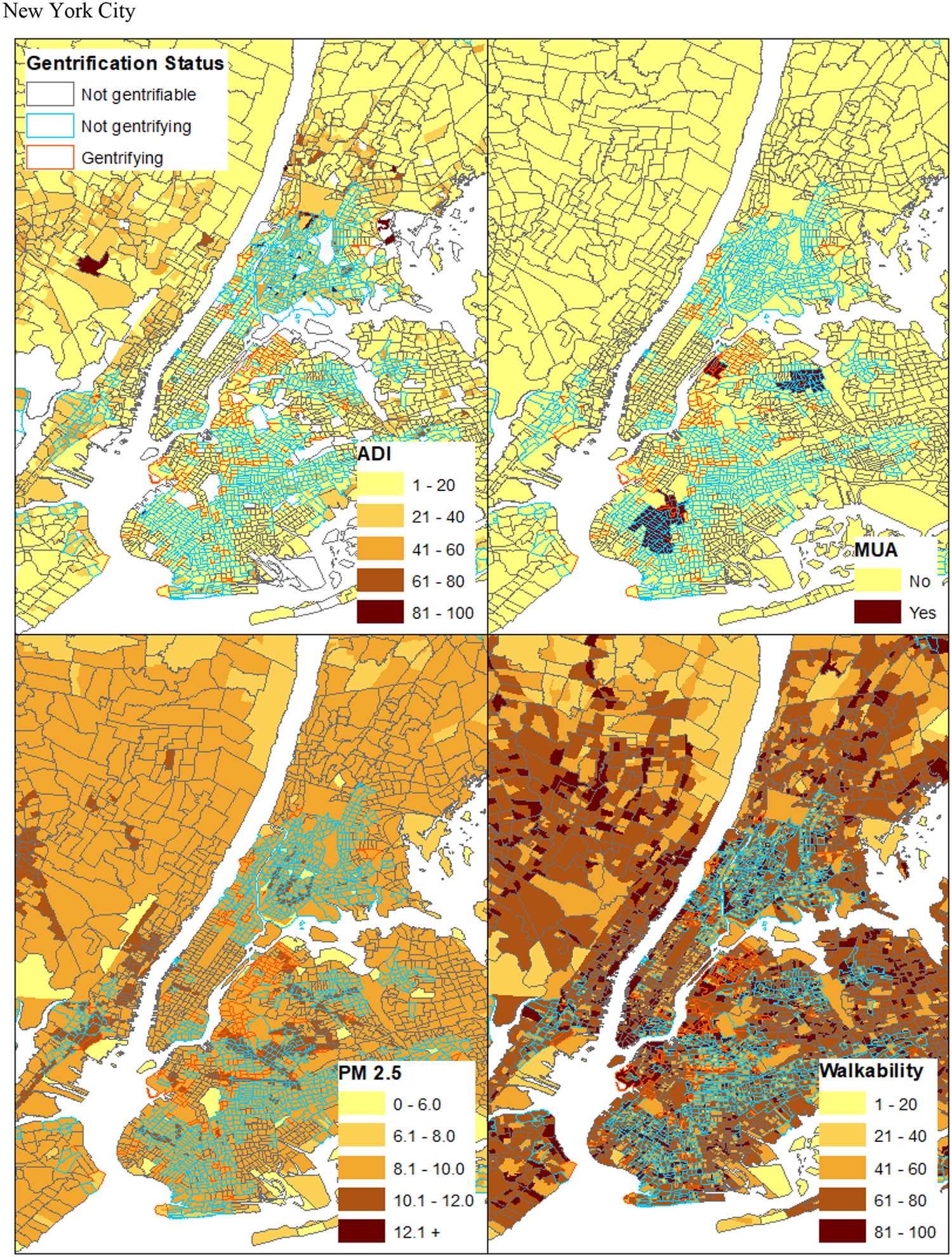
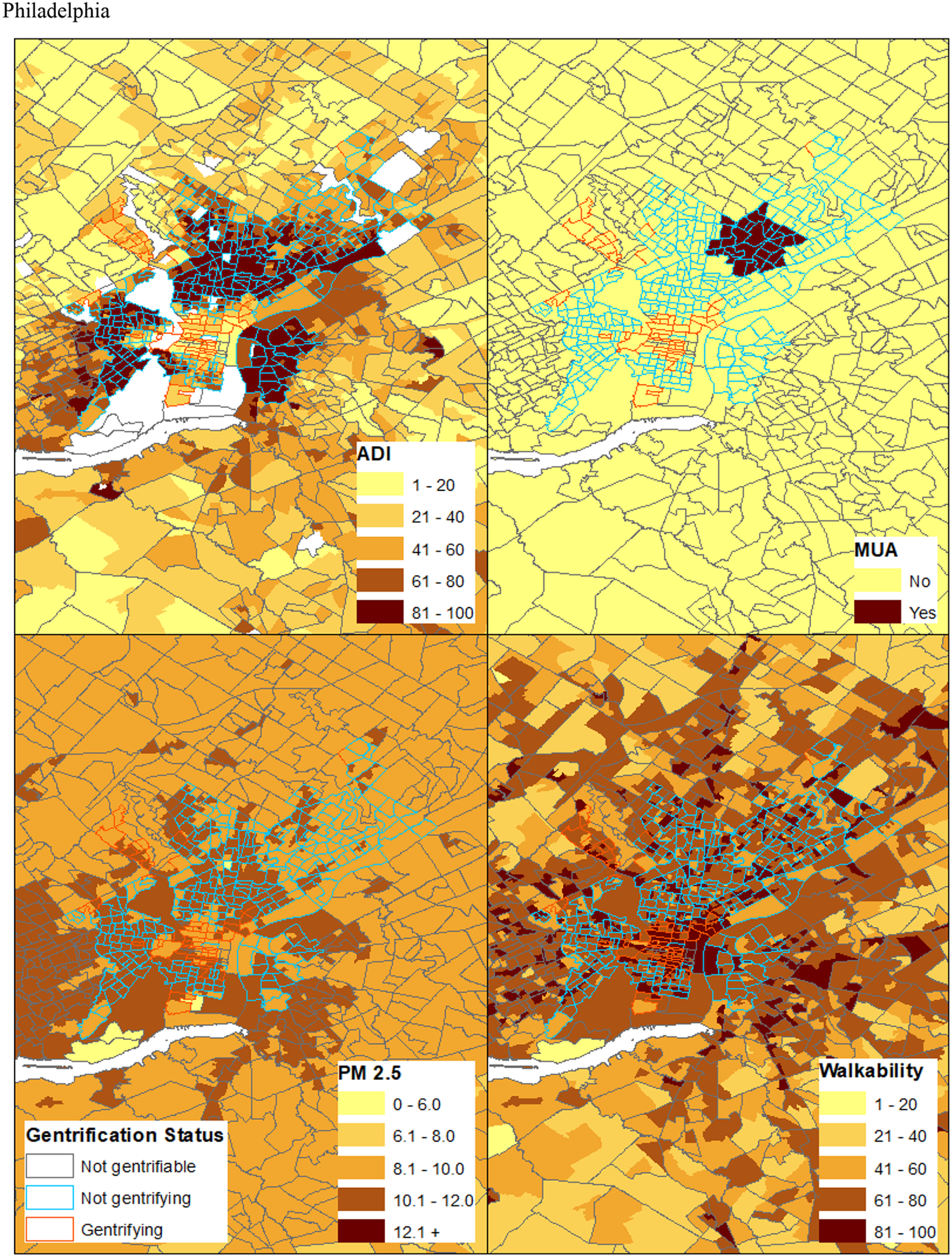
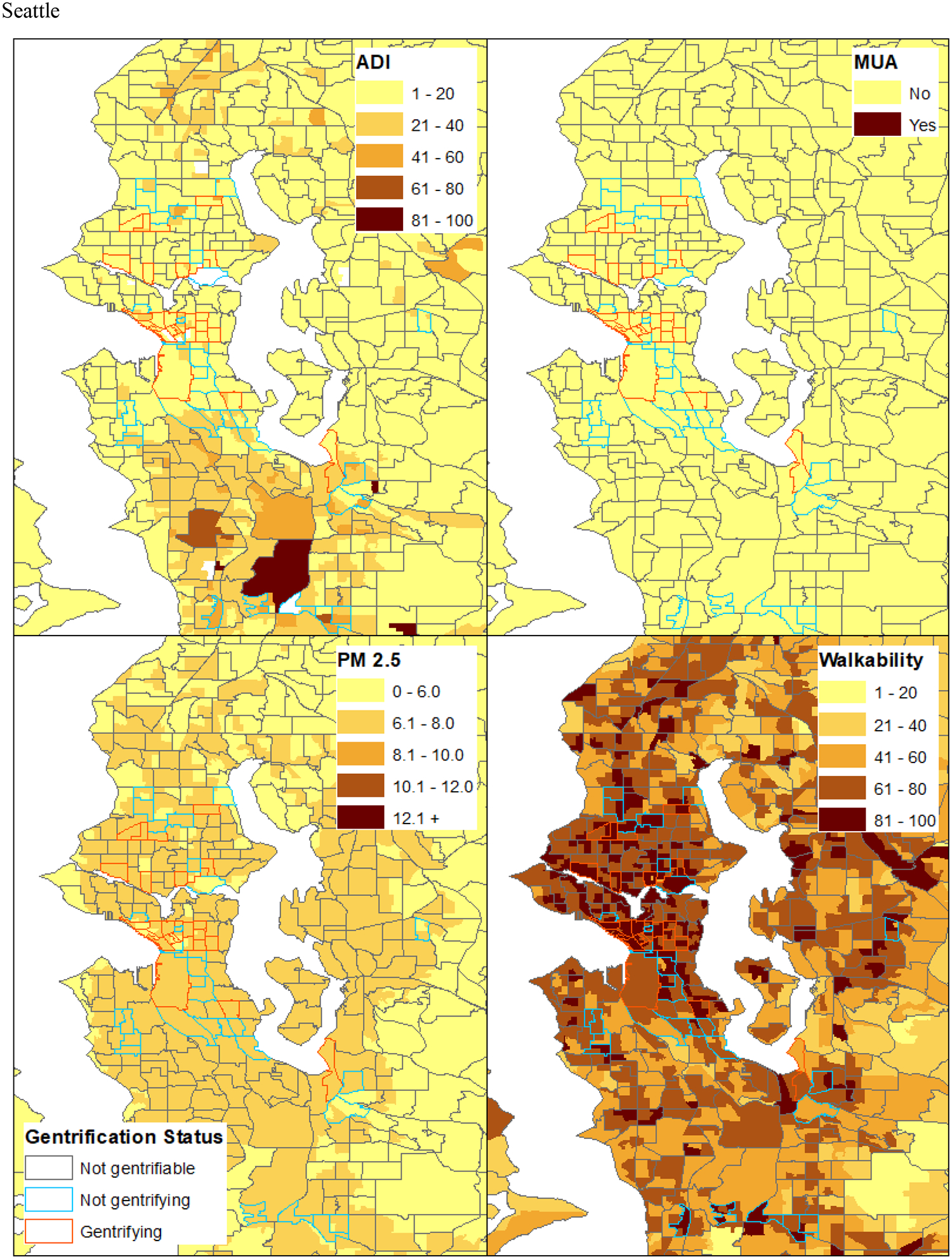
cSDOH measures by gentrifying and not gentrifying status for selected regions
Appendix
Appendix Table 1:
Gentrification Association with cSDOH Among Original Residents with Controls
| Medically Underserved Area | |
|---|---|
| Gentrifying Tract (ref.= Gentrifiable Not Gentrifying) | −0.026*** |
| (0.0003) | |
| Period (ref.= 2006) | −0.013*** |
| (0.0003) | |
| Gentrifying Tract*Period | 0.015*** |
| (0.0003) | |
| Moved during period | −0.004*** |
| (0.0004) | |
| Length of residence as of 2006 | 0.0004*** |
| (0.00001) | |
| Race/Ethnicity (ref.=White non Hispanic) | |
| Black or African American | 0.029*** |
| (0.0003) | |
| Hispanic or Latinx | 0.018*** |
| (0.0003) | |
| Other race or ethnicity | 0.018*** |
| (0.0003) | |
| Number of Children | 0.002*** |
| (0.0002) | |
| Own | −0.004*** |
| (0.0002) | |
| Married | 0.001*** |
| (0.0002) | |
| Age (ref.=Less than 30) | |
| 30–39 | 0.003*** |
| (0.0003) | |
| 40–49 | 0.005*** |
| (0.0003) | |
| 50–59 | 0.005*** |
| (0.0004) | |
| 60+ | 0.002*** |
| (0.0004) | |
| Distance from CBD (km) | |
| −0.112*** | |
| 2000 Neighborhood Controls | (0.0011) |
| Moved | −0.248*** |
| (0.0010) | |
| College degree | 0.145*** |
| (0.0014) | |
| Poverty | −0.001*** |
| (0.00003) | |
| Median income ($ 000) | 0.0001*** |
| (0.000001) | |
| Median rent | 0.0002*** |
| (0.000001) | |
| Median house value ($ 000) | 0.035*** |
| (0.0005) | |
| White non-Hispanic | −0.319*** |
| (0.0018) | |
| Vacant | 0.122*** |
| (0.0008) | |
| Own | −0.003*** |
| (0.000007) | |
| Constant | 0.223*** |
| (0.0011) | |
| N | 10,779,622 |
| Pseudo R-sq | 0.06 |
| MSA Fixed Effects | Yes |
| Clustered Standard Error at Tract Level | Yes |
| ADI National Rank | ADI State Rank | |
|---|---|---|
| Gentrifying Tract (ref.= Gentrifiable Not Gentrifying) | −8.97*** | −11.18*** |
| (0.0170) | (0.0214) | |
| Period (ref.= 2006) | −3.397*** | −4.278*** |
| (0.0176) | (0.0221) | |
| Gentrifying Tract*Period | 3.104*** | 3.952*** |
| 3.104*** | 3.952*** | |
| Moved during period | 0.258*** | 0.434*** |
| (0.0224) | (0.0282) | |
| Length of residence as of 2006 | 0.024*** | 0.021*** |
| (0.0007) | (0.0008) | |
| Race/Ethnicity (ref.=White non Hispanic) | ||
| Black or African American | 4.751*** | 6.165*** |
| (0.0154) | (0.0194) | |
| Hispanic or Latinx | 1.921*** | 2.692*** |
| (0.0155) | (0.0195) | |
| Other race or ethnicity | 0.633*** | 0.586*** |
| (0.0151) | (0.0190) | |
| Number of Children | 0.153*** | 0.148*** |
| (0.0102) | (0.0128) | |
| Own | −1.966*** | −2.134*** |
| (0.0127) | (0.0159) | |
| Married | −1.646*** | −1.905*** |
| (0.0107) | (0.0135) | |
| Age (ref.=Less than 30) | ||
| 30–39 | 0.114*** | 0.166*** |
| (0.0207) | (0.0260) | |
| 40–49 | 0.751*** | 1.030*** |
| (0.0206) | (0.0259) | |
| 50–59 | 0.964*** | 1.279*** |
| (0.0217) | (0.0273) | |
| 60+ | 1.254*** | 1.652*** |
| (0.0234) | (0.0294) | |
| Distance from CBD (km) | ||
| 15.77*** | 22.72*** | |
| 2000 Neighborhood Controls | (0.0677) | (0.0851) |
| Moved | −39.18*** | −51.25*** |
| (0.0578) | (0.0728) | |
| College degree | −2.518*** | −5.231*** |
| (0.0865) | (0.1091) | |
| Poverty | −0.441*** | −0.544*** |
| (0.00152) | (0.0019) | |
| Median income ($ 000) | 0.007*** | 0.007*** |
| (0.0001) | (0.0001) | |
| Median rent | −0.020*** | −0.029*** |
| (0.0001) | (0.0001) | |
| Median house value ($ 000) | −8.140*** | −11.67*** |
| (0.0269) | (0.0338) | |
| White non-Hispanic | −0.018 | −6.691*** |
| (0.1082) | (0.1361) | |
| Vacant | 29.25*** | 35.89*** |
| (0.0484) | (0.0609) | |
| Own | 0.057*** | 0.0914*** |
| (0.0004) | (0.0005) | |
| Constant | 61.62*** | 74.79*** |
| (0.0682) | (0.0858) | |
| N | 10,651,860 | 10,651,860 |
| R-sq | 0.29 | 0.30 |
| MSA Fixed Effects | Yes | Yes |
| Clustered Standard Error at Tract Level | Yes | Yes |
| Nitrogen Dioxide | PM10 | PM2.5 | |
|---|---|---|---|
| Gentrifying Tract (ref.= Gentrifiable Not Gentrifying) | 0.611*** | 0.568*** | 0.126*** |
| (0.0023) | (0.0031) | (0.000908) | |
| Period (ref.= 2006) | −4.870*** | −4.103*** | −3.264*** |
| (0.0024) | (0.0032) | (0.0009) | |
| Gentrifying Tract*Period | −0.784*** | −1.020*** | −0.193*** |
| (0.0026) | (0.0036) | (0.0010) | |
| Moved during period | 0.069*** | 0.010* | −0.008*** |
| (0.0030) | (0.0041) | (0.0012) | |
| Length of residence as of 2006 | 0.007*** | 0.002*** | 0.003*** |
| (0.0001) | (0.0001) | (0.00004) | |
| Race/Ethnicity (ref.=White non Hispanic) | |||
| Black or African American | −0.086*** | −0.014*** | 0.059*** |
| (0.0021) | (0.0028) | (0.0008) | |
| Hispanic or Latinx | 0.383*** | −0.067*** | 0.088*** |
| (0.0021) | (0.0029) | (0.0008) | |
| Other race or ethnicity | 0.064*** | 0.167*** | 0.030*** |
| (0.0020) | (0.0028) | (0.0008) | |
| Number of Children | −0.028*** | 0.009*** | 0.003*** |
| (0.0014) | (0.0019) | (0.0005) | |
| Own | −0.135*** | −0.009*** | 0.018*** |
| (0.0017) | (0.0023) | (0.0007) | |
| Married | −0.085*** | −0.011*** | −0.008*** |
| (0.0014) | (0.0020) | (0.0006) | |
| Age (ref.=Less than 30) | |||
| 30–39 | 0.017*** | 0.044*** | 0.011*** |
| (0.0028) | (0.0038) | (0.0011) | |
| 40–49 | 0.042*** | 0.017*** | 0.004*** |
| (0.0028) | (0.0038) | (0.0011) | |
| 50–59 | 0.043*** | 0.003 | −0.005*** |
| (0.0029) | (0.0040) | (0.0012) | |
| 60+ | −0.001 | −0.011** | −0.024*** |
| (0.0031) | (0.0043) | (0.0012) | |
| Distance from CBD (km) | |||
| −0.188*** | 0.613*** | −0.0364*** | |
| 2000 Neighborhood Controls | (0.0091) | (0.0124) | (0.0036) |
| Moved | −1.682*** | −2.041*** | −0.872*** |
| (0.0077) | (0.0105) | (0.0031) | |
| College degree | 1.808*** | 0.867*** | 0.837*** |
| (0.0116) | (0.0158) | (0.0046) | |
| Poverty | 0.033*** | −0.009*** | 0.006*** |
| (0.0002) | (0.0003) | (0.0001) | |
| Median income ($ 000) | −0.0004*** | 0.0010*** | 0.0001*** |
| (0.000009) | (0.00001) | (0.000004) | |
| Median rent | −0.001*** | 0.001*** | −0.0001*** |
| (0.00001) | (0.00001) | (0.000003) | |
| Median house value ($ 000) | 0.057*** | 0.486*** | 0.024*** |
| (0.0036) | (0.0050) | (0.0014) | |
| White non-Hispanic | 1.975*** | 0.408*** | −0.084*** |
| (0.0145) | (0.0197) | (0.0057) | |
| Vacant | −1.936*** | 1.144*** | 0.399*** |
| (0.0065) | (0.0088) | (0.0026) | |
| Own | −0.099*** | −0.032*** | −0.022*** |
| (0.00007) | (0.00009) | (0.00002) | |
| Constant | 17.93*** | 22.77*** | 12.05*** |
| (0.0091) | (0.0124) | (0.0036) | |
| N | 10,777,539 | 10,777,539 | 10,777,539 |
| R-sq | 0.67 | 0.41 | 0.81 |
| MSA Fixed Effects | Yes | Yes | Yes |
| Clustered Standard Error at Tract Level | Yes | Yes | Yes |
| National Walkability Index | |
|---|---|
| Gentrifying Tract (ref.= Gentrifiable Not Gentrifying) | 1.330*** |
| (0.0136) | |
| Period (ref.= 2006) | −1.522*** |
| (0.0141) | |
| Gentrifying Tract*Period | −1.895*** |
| (0.0235) | |
| Moved during period | −0.681*** |
| (0.0179) | |
| Length of residence as of 2006 | −0.002*** |
| (0.0005) | |
| Race/Ethnicity (ref.=White non Hispanic) | |
| Black or African American | −0.522*** |
| (0.0123) | |
| Hispanic or Latinx | 0.783*** |
| (0.0125) | |
| Other race or ethnicity | 0.878*** |
| (0.0121) | |
| Number of Children | −0.013 |
| (0.0082) | |
| Own | −0.340*** |
| (0.0102) | |
| Married | −0.528*** |
| (0.0086) | |
| Age (ref.=Less than 30) | |
| 30–39 | 0.613*** |
| (0.0165) | |
| 40–49 | 0.883*** |
| (0.0165) | |
| 50–59 | 0.969*** |
| (0.0173) | |
| 60+ | 0.807*** |
| (0.0187) | |
| Distance from CBD (km) | |
| 4.820*** | |
| 2000 Neighborhood Controls | (0.0539) |
| Moved | 5.548*** |
| (0.0459) | |
| College degree | 3.697*** |
| (0.0688) | |
| Poverty | 0.043*** |
| (0.0012) | |
| Median income ($ 000) | −0.002*** |
| (0.0001) | |
| Median rent | −0.001*** |
| (0.0001) | |
| Median house value ($ 000) | 2.519*** |
| (0.0216) | |
| White non-Hispanic | 22.01*** |
| (0.0857) | |
| Vacant | −3.127*** |
| (0.0384) | |
| Own | −0.382*** |
| (0.0004) | |
| Constant | 65.23*** |
| (0.0543) | |
| N | 10,779,187 |
| R-sq | 0.27 |
| MSA Fixed Effects | Yes |
| Clustered Standard Error at Tract Level | Yes |
Appendix Table 2:
Different Definition of Gentrifiable and Gentrification
| Medically Underserved Area | ADI National Rank | ADI State Rank | Nitrogen Dioxide | PM10 | PM2.5 | National Walkability Index | |
|---|---|---|---|---|---|---|---|
| 0.012*** | 2.144*** | 2.704*** | −0.454*** | −0.747*** | −0.045*** | −1.047*** | |
| (0.0003) | (0.0181) | (0.0226) | (0.00243) | (0.00337) | (0.0010) | (0.0030) | |
| N | 12,188,731 | 12,057,266 | 12,057,266 | 12,187,223 | 12,187,223 | 12,187,223 | 12,188,523 |
| R-sq or Pseudo R-sq | 0.06 | 0.26 | 0.28 | 0.67 | 0.38 | 0.80 | 0.18 |
| Medically Underserved Area | ADI National Rank | ADI State Rank | Nitrogen Dioxide | PM10 | PM2.5 | National Walkability Index | |
|---|---|---|---|---|---|---|---|
| 0.008*** | 3.09*** | 3.770*** | −0.794*** | −1.181*** | −0.247*** | −1.017*** | |
| (0.0004) | (0.0259) | (0.0325) | (0.0035) | (0.0051) | (0.0014) | (0.0042) | |
| N | 6,222,892 | 6,129,766 | 6,129,766 | 6,221,412 | 6,221,412 | 6,221,412 | 6,222,667 |
| R-sq or Pseudo R-sq | 0.06 | 0.30 | 0.31 | 0.68 | 0.44 | 0.79 | 0.23 |
| Medically Underserved Area | ADI National Rank | ADI State Rank | Nitrogen Dioxide | PM10 | PM2.5 | National Walkability Index | |
|---|---|---|---|---|---|---|---|
| 0.013*** | 2.589*** | 3.215*** | −0.704*** | −1.322*** | −0.164*** | −1.077*** | |
| (0.0005) | (0.0316) | (0.0398) | (0.0042) | (0.0057) | (0.0016) | (0.0048) | |
| N | 4,482,304 | 4,400,776 | 4,400,776 | 4,481,125 | 4,481,125 | 4,481,125 | 4,482,174 |
| R-sq or Pseudo R-sq | 0.06 | 0.26 | 0.26 | 0.69 | 0.46 | 0.83 | 0.27 |
| Medically Underserved Area | ADI National Rank | ADI State Rank | Nitrogen Dioxide | PM10 | PM2.5 | National Walkability Index | |
|---|---|---|---|---|---|---|---|
| 0.032*** | 3.039*** | 3.843*** | −0.800*** | −1.030*** | −0.204*** | −1.225*** | |
| (0.0003) | (0.0198) | (0.0248) | (0.0027) | (0.0037) | (0.0011) | (0.0032) | |
| N | 10,369,162 | 10,252,444 | 10,252,444 | 10,367,232 | 10,367,232 | 10,367,232 | 10,368,763 |
| R-sq or Pseudo R-sq | 0.05 | 0.29 | 0.30 | 0.67 | 0.40 | 0.81 | 0.24 |
Note: All results are for specifications including individual and neighborhood controls, MSA fixed effects and clustered standard error at the tract level.
Footnotes
We acknowledge that gentrification can also take place in suburban (Markley 2018) and rural (Sherman 2021) communities but focus here on central cities due to shared historical patterns of disinvestment and reinvestment in public and private goods in there communities that are expected to be directly related to cSDOH.
Distance to the center is estimated as the Euclidian distance in km between the individual address and City Hall for an MSA central city as determined and made available by US Census Bureau (https://www.census.gov/library/publications/2012/dec/c2010sr-01.html). This variable aims to capture the spatial location of the units within the urban system with more central locations expected to be more desirable. See Holian (2019) for a discussion of the different measures of centrality available.
Following the rule of thumb values developed by Oster and used by Brummet and Reed, we use Rmax = 1.3 times the R-squared for the model with full controls and little delta = 1, assuming the influence of remaining unobservables is proportional to the influence of full controls.
References
- Acevedo-Garcia D, Lochner KA, Osypuk TL, & Subramanian SV (2003). Future directions in residential segregation and health research: a multilevel approach. American journal of public health, 93(2), 215–221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Acolin A, Decter-Frain A., & Hall M (2021). Small Area Population Estimates from Consumer Trace Data. Working Paper. 2021.
- Ahnquist J, Wamala SP, Lindstrom M. (2012). Social determinants of health–a question of social or economic capital? Interaction effects of socioeconomic factors on health outcomes. Social science & medicine. 74(6):930–939. [DOI] [PubMed] [Google Scholar]
- Arias E, Escobedo LA, Kennedy J, Fu C, & Cisewski JA (2018). US small-area life expectancy estimates project: Methodology and results summary. [PubMed]
- Bhavsar NA, Kumar M, & Richman L (2020). Defining gentrification for epidemiologic research: A systematic review. Plos one, 15(5), e0233361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Braveman P, Egerter S, & Williams DR (2011). The social determinants of health: coming of age. Annual review of public health, 32, 381–398. [DOI] [PubMed] [Google Scholar]
- Braveman P, & Gottlieb L (2014). The social determinants of health: it’s time to consider the causes of the causes. Public health reports, 129(1_suppl2), 19–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brevoort KP, Grimm P, & Kambara M (2015). Credit Invisibles. Bureau of Consumer Financial Protection Data Point Series, (15–1). [Google Scholar]
- Brophy PC (Ed.). (2016). On the Edge: America’s Middle Neighborhoods. American Assembly. [Google Scholar]
- Brown EJ, Polsky D, Barbu CM, Seymour JW, & Grande D (2016). Racial disparities in geographic access to primary care in Philadelphia. Health Affairs, 35(8), 1374–1381. [DOI] [PubMed] [Google Scholar]
- Brummet Q, & Reed D (2019). The effects of gentrification on the well-being and opportunity of original resident adults and children.
- Carlson ED, & Chamberlain RM (2003). Social capital, health, and health disparities. Journal of Nursing Scholarship, 35(4), 325–331.. [DOI] [PubMed] [Google Scholar]
- Carpiano RM (2006). Toward a neighborhood resource-based theory of social capital for health: can Bourdieu and sociology help?. Social science & medicine, 62(1), 165–175. [DOI] [PubMed] [Google Scholar]
- Cole HV (2020). A call to engage: considering the role of gentrification in public health research. Cities & Health, 4(3), 278–287. [Google Scholar]
- Cole HV, Triguero-Mas M, Connolly JJ, & Anguelovski I (2019). Determining the health benefits of green space: Does gentrification matter?. Health & place, 57, 1–11. [DOI] [PubMed] [Google Scholar]
- Couture V, Gaubert C, Handbury J, & Hurst E (2019). Income growth and the distributional effects of urban spatial sorting (No. w26142). National Bureau of Economic Research. [Google Scholar]
- Couture V, & Handbury J (2020). Urban revival in America. Journal of Urban Economics, 119, 103267. [Google Scholar]
- Crowder K, & Downey L (2010). Interneighborhood migration, race, and environmental hazards: Modeling microlevel processes of environmental inequality. American journal of sociology, 115(4), 1110–1149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diez Roux AV, & Mair C (2010). Neighborhoods and health. Annals of the New York Academy of Sciences, 1186(1), 125–145. [DOI] [PubMed] [Google Scholar]
- Ding L, Hwang J, Divringi E. (2016). Gentrification and residential mobility in Philadelphia. Regional Science and Urban Economics. 61:38–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dragan KL, Ellen IG, & Glied SA (2019). Gentrification and the health of low-income children in New York City. Health affairs, 38(9), 1425–1432. [DOI] [PubMed] [Google Scholar]
- Dragan K, Ellen IG, & Glied S (2020). Does gentrification displace poor children and their families? New evidence from medicaid data in New York City. Regional Science and Urban Economics, 83, 103481. [Google Scholar]
- Duncan DT, Aldstadt J, Whalen J, White K, Castro MC, & Williams DR (2012). Space, race, and poverty: Spatial inequalities in walkable neighborhood amenities?. Demographic research, 26(17), 409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Firth CL, Fuller D, Wasfi R, Kestens Y, & Winters M (2020). Causally speaking: Challenges in measuring gentrification for population health research in the United States and Canada. Health & Place, 63, 102350. [DOI] [PubMed] [Google Scholar]
- Freeman L (2009). Neighbourhood diversity, metropolitan segregation and gentrification: What are the links in the US?. Urban Studies, 46(10), 2079–2101. [Google Scholar]
- Fullilove MT (1996). Psychiatric implications of displacement: Contributions from the psychology of place. American Journal of Psychiatry, 153, 12. [DOI] [PubMed] [Google Scholar]
- Fullilove MT (2016). Root shock: How tearing up city neighborhoods hurts America, and what we can do about it. New Village Press. [Google Scholar]
- Gentili M, Isett K, Serban N, & Swann J (2015). Small-area estimation of spatial access to care and its implications for policy. Journal of Urban Health, 92(5), 864–909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibbons J, & Barton MS (2016). The association of minority self-rated health with black versus white gentrification. Journal of urban health, 93(6), 909–922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibbons J, Barton M, & Brault E (2018). Evaluating gentrification’s relation to neighborhood and city health. PloS one, 13(11), e0207432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holian MJ (2019). Where is the City’s Center? Five Measures of Central Location. Cityscape, 21(2), 213–226. [Google Scholar]
- Hu J, Kind AJ, & Nerenz D (2018). Area deprivation index predicts readmission risk at an urban teaching hospital. American Journal of Medical Quality, 33(5), 493–501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hwang J, Lin J. What have we learned about the causes of recent gentrification? Cityscape. 2016;18(3):9–26. [Google Scholar]
- Izenberg JM, Mujahid MS, & Yen IH (2018). Health in changing neighborhoods: A study of the relationship between gentrification and self-rated health in the state of California. Health & place, 52, 188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson GD, Checker M, Larson S, & Kodali H (2021). A small area index of gentrification, applied to New York City. International Journal of Geographical Information Science, 1–21. [Google Scholar]
- Kim SY, Bechle M, Hankey S, Sheppard L, Szpiro AA, & Marshall JD (2020). Concentrations of criteria pollutants in the contiguous US, 1979–2015: Role of prediction model parsimony in integrated empirical geographic regression. PloS one, 15(2), e0228535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kind AJ, Jencks S, Brock J, Yu M, Bartels C, Ehlenbach W, … & Smith M (2014). Neighborhood socioeconomic disadvantage and 30-day rehospitalization: a retrospective cohort study. Annals of internal medicine, 161(11), 765–774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kravitz-Wirtz N, Crowder K, Hajat A, & Sass V (2016). The long-term dynamics of racial/ethnic inequality in neighborhood air pollution exposure, 1990–2009. Du Bois review: social science research on race, 13(2), 237–259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kravitz-Wirtz N, Teixeira S, Hajat A, Woo B, Crowder K, & Takeuchi D (2018). Early-life air pollution exposure, neighborhood poverty, and childhood asthma in the United States, 1990–2014. International journal of environmental research and public health, 15(6), 1114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kwan MP (2009). From place-based to people-based exposure measures. Social science & medicine, 69(9), 1311–1313. [DOI] [PubMed] [Google Scholar]
- Lantos PM, Hoffman K, Permar SR, Jackson P, Hughes BL, Kind A, & Swamy G (2018). Neighborhood disadvantage is associated with high cytomegalovirus seroprevalence in pregnancy. Journal of racial and ethnic health disparities, 5(4), 782–786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lim S, Chan PY, Walters S, Culp G, Huynh M, & Gould LH (2017). Impact of residential displacement on healthcare access and mental health among original residents of gentrifying neighborhoods in New York City. PloS one, 12(12), e0190139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Link BG, & Phelan J (1995). Social conditions as fundamental causes of disease. Journal of health and social behavior, 80–94. [PubMed] [Google Scholar]
- Liu J, Clark LP, Bechle M, Hajat A, Kim SY, Robinson A, … & Marshall JD (2021). Disparities in Air Pollution Exposure in the United States by Race-Ethnicity and Income, 1990–2010. Environmental Health Perspectives, 129(12), https://ehp.niehs.nih.gov/doi/10.1289/EHP8584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ludwig J, Sanbonmatsu L, Gennetian L, Adam E, Duncan GJ, Katz LF, … & McDade TW (2011). Neighborhoods, obesity, and diabetes—a randomized social experiment. New England journal of medicine, 365(16), 1509–1519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maciag M (2015). Gentrification in America report. Governing.
- Markley S (2018). Suburban gentrification? Examining the geographies of New Urbanism in Atlanta’s inner suburbs. Urban Geography, 39(4), 606–630. [Google Scholar]
- Manzo LC (2003). Beyond house and haven: Toward a revisioning of emotional relationships with places. Journal of environmental psychology, 23(1), 47–61. [Google Scholar]
- Martin RW (2017). Gentrification trends in the United States, 1970–2010.
- Mast E (2019). The effect of new market-rate housing construction on the low-income housing market. Upjohn Institute WP, 19–307. [Google Scholar]
- Massey DS, & Denton NA (1989). Hypersegregation in US metropolitan areas: Black and Hispanic segregation along five dimensions. Demography, 26(3), 373–391. [PubMed] [Google Scholar]
- Messer LC, Laraia BA, Kaufman JS, Eyster J, Holzman C, Culhane J, … & O’campo P (2006). The development of a standardized neighborhood deprivation index. Journal of Urban Health, 83(6), 1041–1062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oster E (2019). Unobservable selection and coefficient stability: Theory and evidence. Journal of Business & Economic Statistics, 37(2), 187–204. [Google Scholar]
- Pais J, Crowder K, & Downey L (2014). Unequal trajectories: Racial and class differences in residential exposure to industrial hazard. Social Forces, 92(3), 1189–1215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pearsall H, & Eller JK (2020). Locating the green space paradox: A study of gentrification and public green space accessibility in Philadelphia, Pennsylvania. Landscape and Urban Planning, 195, 103708. [Google Scholar]
- Phillips DC (2020). Measuring housing stability with consumer reference data. Demography, 57(4), 1323–1344. [DOI] [PubMed] [Google Scholar]
- Pope CA III, Lefler JS, Ezzati M, Higbee JD, Marshall JD, Kim SY, … & Burnett RT (2019). Mortality risk and fine particulate air pollution in a large, representative cohort of US adults. Environmental health perspectives, 127(7), 077007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Preis B, Janakiraman A, Bob A, & Steil J (2021). Mapping gentrification and displacement pressure: An exploration of four distinct methodologies. Urban Studies, 58(2), 405–424. [Google Scholar]
- Reina V, Acolin A, & Bostic RW (2019). Section 8 vouchers and rent limits: Do small area fair market rent limits increase access to opportunity neighborhoods? An early evaluation. Housing Policy Debate, 29(1), 44–61. [Google Scholar]
- Robert, Foundation WJ. Life Expectancy: Could where you live influence how long you live? In:N.A. [Google Scholar]
- Sass V, Kravitz-Wirtz N, Karceski SM, Hajat A, Crowder K, & Takeuchi D (2017). The effects of air pollution on individual psychological distress. Health & place, 48, 72–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schnake-Mahl AS, Jahn JL, Subramanian SV, Waters MC, & Arcaya M (2020). Gentrification, neighborhood change, and population health: a systematic review. Journal of Urban Health, 97(1), 1–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schnake-Mahl AS, & Sommers BD (2017). Health care in the suburbs: an analysis of suburban poverty and health care access. Health affairs, 36(10), 1777–1785. [DOI] [PubMed] [Google Scholar]
- Scribner RA, Simonsen NR, & Leonardi C (2017). The social determinants of health core: taking a place-based approach. American journal of preventive medicine, 52(1), S13–S19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sharkey P, & Faber JW (2014). Where, when, why, and for whom do residential contexts matter? Moving away from the dichotomous understanding of neighborhood effects. Annual review of sociology, 40, 559–579. [Google Scholar]
- Sherman J (2021). “Please Don’t Take This”: Rural Gentrification, Symbolic Capital, and Housing Insecurity. Social Problems. [Google Scholar]
- Shi L, Macinko J, Starfield B, Politzer R, Wulu J, & Xu J (2005). Primary care, social inequalities, and all-cause, heart disease, and cancer mortality in US counties, 1990. American journal of public health, 95(4), 674–680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith GS, Breakstone H, Dean LT, & Thorpe RJ (2020). Impacts of gentrification on health in the US: A systematic review of the literature. Journal of Urban Health, 97(6), 845–856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Streeter RA, Snyder JE, Kepley H, Stahl AL, Li T, & Washko MM (2020). The geographic alignment of primary care Health Professional Shortage Areas with markers for social determinants of health. PloS one, 15(4), e0231443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wen M, Zhang X, Harris CD, Holt JB, & Croft JB (2013). Spatial disparities in the distribution of parks and green spaces in the USA. Annals of Behavioral Medicine, 45(suppl_1), S18–S27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams DR, & Collins C (2016). Racial residential segregation: a fundamental cause of racial disparities in health. Public health reports. [DOI] [PMC free article] [PubMed] [Google Scholar]