

Introduction
Inflammatory linear verrucous epidermal nevus (ILVEN) is a rare disorder characterized by an early age onset [1]. It consists of pruritic linear, or whorled array of inflammatory, following Blaschko lines [2], papules and/or plaques and histologic features resembling psoriasis or lichenoid dermatitis [3]. The disease is a distinct variety of keratinocytic epidermal nevus that is clinically inflammatory and reflects a phenomenon of mosaicism caused by somatic mutations. We report the case of a 6-year-old boy in which in vivo reflectance confocal microscopy (RCM) allowed the diagnosis of ILVEN avoiding an invasive skin biopsy.
Case Presentation
A 6-year-old boy was seen for a linear, mild itchy lesion involving the left part of the nose. Diagnosed one year earlier as impetigo, after multiple ineffective topical and systemic antibiotic treatments, referred to our clinic for redness and worsening of the lesion. Clinical examination showed a linear dyskeratotic erythematous plaque with a slightly pigmented halo and fine superficial desquamation located on the nose (Figure 1A). Because of the anatomic site and age of the patient, to avoid biopsy he was subjected assessment with hand-held RCM (Vivascope 3000). It proved minimal hyperkeratosis, spongiosis (Figure 2A, white circle) with a pattern closer to the honeycombed one with thickened, highly refractive intercellular space between keratinocytes (Figure 2B). Non-rimed connective tissue papillae were observed at the level of the epithelial-connective tissue junction (Figure 2C). Below the basal layer, connective tissue papillae appeared disrupted and confluent in large dark areas (Figure 2D, white circle), peculiar signs of interface dermatitis. Based on these and on the clinical features patient was diagnosed with ILVEN and treatment started at first with hydrocortisone butyrate ointment 0.1% twice a day for one month with good improvement (Figure 1B). Then was prescribed tacrolimus ointment 0.03% twice a day for another month leading to complete resolution of the lesion.
Figure 1.

(A) Linear dyskeratotic erythematous plaque with a slightly pigmented halo and fine superficial desquamation involving the columella, tip and bridge of the left part of the nose. (B) Clinical picture one months after treatment with hydrocortisone butyrate ointment 0.1% twice a day; almost complete resolution of lesion.
Figure 2.
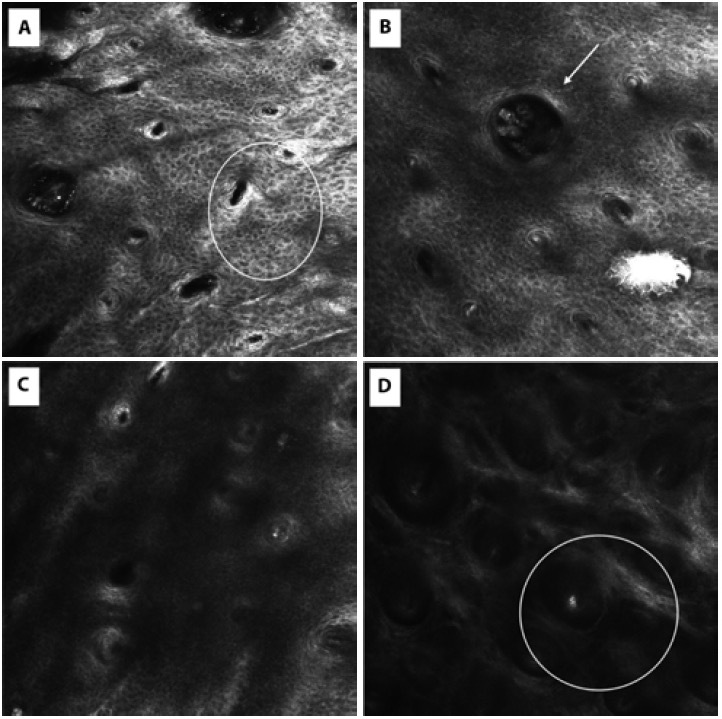
(A–D) Summary of the main features imaged by in vivo reflectance confocal microscopy (RCM) (Vivascope 3000) in RCM in Inflammatory Linear Verrucous Epidermal Nevus.
(A) Spongiosis (withe circle) with a pattern closer to the honeycombed one with thickened, highly refractive intercellular space between keratinocytes.
(B) Presence of a single roundish refractive Demodex folliculorum (arrow) within the hair follicles and a pattern closer to the honeycombed.
(C) At level of the epithelial-connective tissue junction, non-rimed connective tissue papillae were observed.
(D) Below the basal layer, connective tissue papillae appeared disrupted and confluent in large dark areas (white circle), peculiar signs of the interface dermatitis.
Conclusions
ILVEN is a relatively rare disease and remains a clinical-pathological diagnosis. There are numerous differential diagnoses to be taken into consideration such as: other epidermal nevi, Darier disease, linear porokeratosis, linear lichen planus, linear psoriasis and lichen striatus. Our diagnosis of ILVEN was based on pathognomonic clinical signs and RCM-assessed pictures of inflammatory lichenoid dermatitis thus excluding both psoriasiform dermatitis and spongiotic dermatitis [4]. In vivo RCM is a non-invasive imaging and appears interesting for assessment of lesion in special areas and in pediatric patients [5,6]. The main limitation of RCM is its penetration in dermis, reaching nowadays 350–400 μm. This prevents imaging of structures located in the deep dermis, especially in cases of hyperpigmented or hyperkeratotic lesions, as, in these cases, there is strong contrast attenuation because of absorption and scattering of light going through those structures. However, the ILVEN histological characteristics and the thinner skin of the pediatric patient make the use of this non-invasive technology particularly suitable in this case. Finally, it is important to underline how the current contact devices can be best used even on a non-flat surface; fast and handy device make it much more practical also for pediatric patients.
Footnotes
Funding: None.
Competing Interests: None.
Authorship: All authors have contributed significantly to this publication.
References
- 1.Wollina U, Tchernev G. ILVEN - COMPLETE REMISSION AFTER ADMINISTRATION O TOPICAL CORTICOSTEROID (CASE REVIEW) Georgian Med News. 2017;(263):10–13. [PubMed] [Google Scholar]
- 2.Barney E, Prose NS, Ramirez M. Inflammatory linear verrucous epidermal nevus treated successfully with crisaborole ointment in a 5-year-old boy. Pediatr Dermatol. 2019;36(3):404–405. doi: 10.1111/pde.13793. [DOI] [PubMed] [Google Scholar]
- 3.Tanita K, Fujimura T, Sato Y, Lyu C, Aiba S. Widely Spread Unilateral Inflammatory Linear Verrucous Epidermal Nevus (ILVEN) Case Rep Dermatol. 2018;10(2):170–175. doi: 10.1159/000489876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Csuka EA, Ward SC, Ekelem C, Csuka DA, Ardigò M, Mesinkovska NA. Reflectance Confocal Microscopy, Optical Coherence Tomography, and Multiphoton Microscopy in Inflammatory Skin Disease Diagnosis. Lasers Surg Med. 2021;53(6):776–797. doi: 10.1002/lsm.23386. [DOI] [PubMed] [Google Scholar]
- 5.Scharf C, Argenziano G, Brancaccio G, Licata G, Ronchi A, Moscarella E. Melanocytic or Not? Dermoscopy and Reflectance Confocal Microscopy for Lesions Difficult to Diagnose: A Cross-Sectional Diagnostic Accuracy Study. Dermatol Pract Concept. 2021;11(4):e2021127. doi: 10.5826/dpc.1104a127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ko RF, Smidt AC, Durkin JR. Reflectance confocal microscopy in pediatric dermatology: A state-of-the-art review. Pediatr Dermatol. 2021;38(6):1488–1499. doi: 10.1111/pde.14837. [DOI] [PubMed] [Google Scholar]