

Abstract
Objective
To develop and evaluate a storytelling communication facilitation tool designed to help parents overcome barriers to discussing a complex multisystem genetic diagnosis with their affected children, using 22q11.2 deletion syndrome (22q11DS) as an exemplar condition.
Methods
A story telling communication facilitation tool (SCFT), entitled 22q and Me, was developed for a target audience of children with 22q11DS aged 9 to 12. The SCFT was evaluated by 14 parents to assess usability and utility by comparing responses to survey questions before and after viewing the SCFT, using a Likert scale.
Results
After viewing 22q and Me, parents reported that barriers to discussion were mitigated. Participants indicated they felt more comfortable and better prepared to talk to their children about 22q11DS and worried less that the diagnosis would affect their children’s self-esteem. Parents described 22q and Me as engaging and able to address parental concerns.
Conclusion
22q and Me was found to be an effective tool for increasing parental comfort and ability to talk to their children about their diagnosis of 22q11DS.
Innovation
This novel storytelling communication facilitation tool can serve as a model for the development of other educational tools geared at facilitating disclosure and discussion of other genetic conditions.
Keywords: 22q11.2 deletion syndrome, Parent-child communication, Facilitating conversation, Disclosure of genetic diagnosis, Storytelling communication facilitation tool
Highlights
-
•
Parents have identified a need for resources to help them discuss genetic diagnoses with their children
-
•
An online tool was developed to help with discussion and disclosure of 22q11 deletion syndrome
-
•
Parents felt more comfortable and capable of having these discussions after using the online tool
1. Introduction
Numerous research studies have documented that parents of children with genetic conditions face many challenges when disclosing the diagnosis to their children [[1], [2], [3], [4], [5], [6], [7], [8]]. Several common barriers have been reported across diverse genetic conditions, including concerns about: sharing information at a developmentally appropriate level, what language to use, causing fear or anxiety in the child, negatively impacting self-esteem, or the child using their diagnosis as an excuse for not attempting to overcome challenges [[1], [2], [3], [4], [5], [6], [7], [8]].
Many parents note a lack of adequate support from healthcare providers in speaking with their children about their condition, and expressed a need for resources to help them with the disclosure discussions [1,9,10]. The use of aids, such as pictures or books, has been shown to be valuable in communicating information about genetics to children [1]. Content, organization, appearance, and writing style of the material are important features that impact a child’s engagement and understanding [11]. While many written resources on genetics exist, over the last decade, there has been an increase in the use of multimedia and computer education modules. Many studies have described the successful use of multimedia tools as a vector for patient education, including the education of children with intellectual disabilities [[12], [13], [14], [15], [16], [17], [18]]. Advantages of using online educational tools include the individual’s ability to access information when they choose, the opportunity to do so on multiple occasions if necessary, and the freedom to proceed at one’s own pace [19,20]. Parents of children with complex genetic diagnoses have a variety of resources available to help them navigate various aspects of their child’s condition throughout different developmental ages. Much of this information is readily accessible on reputable websites devoted to providing information on genetic conditions. However, parents have indicated the need for specific resources to support disclosure conversations with their children, and there is limited information on the development and evaluation of tools designed to facilitate these conversations [1,[4], [5], [6],10].
22q11.2 Deletion syndrome (22q11DS) is one such genetic condition. It is caused by a heterozygous deletion at 22q11.2 and is the most common human microdeletion disorder, with an incidence of approximately 1 in 2000 births [[21], [22], [23]]. It is a multisystem disorder with medical and neurodevelopmental features that vary widely between individuals [21]. Some of the most common features include congenital heart defects, immunodeficiency, developmental delay, learning difficulties, intellectual disability, and increased incidence of psychiatric disorders [21]. One study which ascertained parents’ experiences disclosing the diagnosis of 22q11DS to their children identified similar challenges around disclosure that have been identified for other genetic conditions [10].
This study aimed to address the barriers identified by parents that hinder such conversations by:
-
1)
Developing a storytelling communication facilitation tool (SCFT) specifically designed to help facilitate communication between parents and children regarding the child’s genetic diagnosis, using 22q11DS as a model condition.
-
2)
Evaluating the SCFT’s effectiveness as a communication tool for helping parents feel better equipped to discuss their children’s genetic condition with them.
2. Methods
2.1. SCFT development
The SCFT, titled 22q and Me was developed by a team with expertise in 22q11DS, illustration, and multimedia production and editing. The SCFT was designed to target barriers to disclosure previously identified in the literature [[1], [2], [3], [4], [5], [6], [7], [8],10]. Additionally, we solicited input from parents of children with 22q11DS who attended the 7th Annual 22q at the Zoo International Awareness Day at the Toronto Zoo in June 2018. Seven parents provided written responses to open-ended questions about challenges they faced when speaking to their child about 22q11DS. The topics that parents mentioned reflected those previously reported in the literature including concerns with how to explain features of the condition and using the diagnosis as an excuse for not attempting to overcome challenges.
A script for the SCFT was developed by the lead researcher and reviewed by the co-authors (CC, AS), genetic counsellors with expertise in 22q11DS. The script follows one main character who shares his personal experience of living with 22q11DS and introduces his friends, who also have 22q11DS, to highlight the variability of the condition and model self-acceptance through a strengths-based lens. The topics in the script aimed to address the barriers previously identified by parents in the literature. The script is divided into five sections, reflecting various aspects of a child’s life frequently impacted by having a genetic syndrome, ascertained from the literature and clinical experience. The first section, titled ‘What is 22q?’ provides background information on the genetics of 22q11DS. ‘Growing up with 22q’ addresses some of the main clinical features of 22q11DS. ‘22q and school’ focuses on challenges that individuals with 22q11DS may experience at school, while ‘22q and friends’ addresses bullying and social aspects of 22q11DS. Lastly, ‘More than 22q’ emphasizes that individuals with 22q11DS are not defined by their diagnosis and highlights characteristics unrelated to their diagnosis.
The artwork and animation were developed in Adobe Animate and designed to include diverse characters, with regards to ethnicity and gender, in settings easily recognized by children. The script was reviewed and edited by a managing editor and multimedia producer from the children’s health educational website AboutKidsHealth, where the SCFT was hosted. Given the wide variability in cognitive profiles of children with 22q11DS, ranging from learning difficulties to mild–moderate intellectual disability [21], the review and editing process helped to ensure the language was appropriate for the target audience. A graphic of the components of the SCFT can be found in Fig. 1.
Fig. 1.
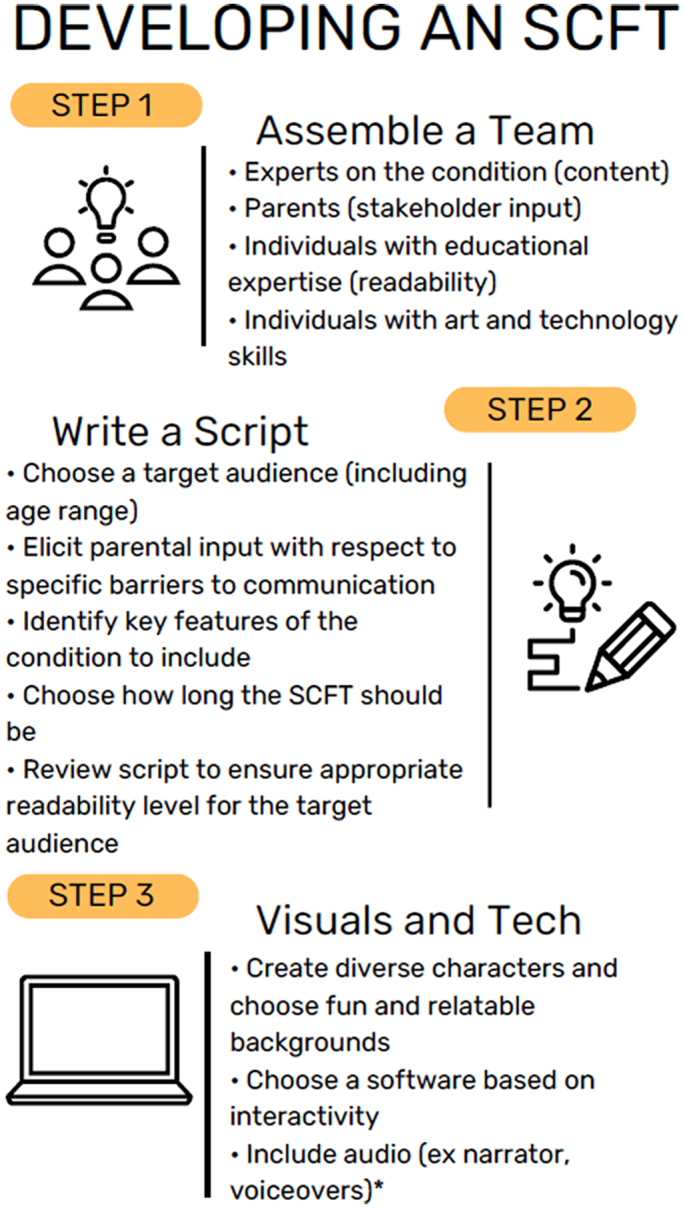
A framework for developing a storytelling communication facilitation tool that can be generalized for any complex genetic condition. *Due to time and resource constraints, audio was not included in our SCFT.
2.2. Participants
Study participants included parents of children with 22q11DS from 9 to 12 years of age, who were proficient in English. Parents, subsequently referred to as study participants, were recruited from the 22q11DS Clinic patient registry at The Hospital for Sick Children in Toronto via email, and through an advertisement at the Annual 22q11.2 Family Conference held at The Hospital for Sick Children in November 2018. A recruitment notice was also posted on three websites, including The International 22q11.2 Foundation Inc, the 22q11.2 Society, and the Deletion 22q Support Group on Facebook. Individuals who provided input at the Toronto Zoo were not included as study participants. Exclusion criteria included parents who also had a diagnosis of 22q11DS. Informed consent was obtained for research participants through protocols approved by the Research Ethics Board of The Hospital for Sick Children (REB #1000061163).
Participants received a link to survey 1 and to 22q and Me with instructions to complete the first survey prior to viewing the SCFT. Participants were required to complete an electronic consent form prior to beginning survey 1. Participants received a link to survey 2 one week after completing survey 1.
2.3. Survey development and structure
The usability and utility of the SCFT, including the effectiveness of the tool in targeting the barriers identified in the literature, were assessed using a quantitative, survey-based approach. Survey development was guided by Genetic Counseling Research: A Practical Guide [24]. Questions focused on barriers identified in the literature. Participants completed two surveys, one prior to using the SCFT (survey 1), and one after (survey 2). The purpose of survey 1 was to identify parental perspectives regarding their level of comfort, preparedness and perceived barriers impacting disclosure, as well as timing and content of prior disclosures/discussions. The responses were entered using a Likert scale from 0 to 10, with 0 representing strongly disagree and 10 representing strongly agree. Survey 1 also solicited demographic questions, including information on the child’s academic abilities and comorbidities. Survey 2 sought to assess any changes to responses after viewing the SCFT. There were 10 questions on survey 1 which were either forward- or reverse-coded, eight of which were included on survey 2. Both forward- and reverse-coded questions were used to assess a wider breadth of opinions from the participants by using words with both positive (i.e. ‘prepared’) and negative (i.e. ‘struggle’) connotations. Forward-coded questions refer to those where a higher number on the Likert scale indicates less worry or struggle. For reverse-coded questions, a high number on the Likert scale indicates more worry or struggle. Table 1 provides three examples of survey questions designed to target specific barriers. Survey 2 also included a number of questions soliciting feedback on the SCFT in both Likert and open-ended format. The open-ended questions were designed to obtain parental feedback on the tool to provide direction on enhancements for future iterations. Qualitiative analysis was not performed.
Table 1.
Examples of barriers addressed in 22q and Me and accompanying survey questions.
| Barrier | How barrier was addressed in 22q and Me | Survey question |
|---|---|---|
| Knowing how to explain 22q11DS |  |
I struggle knowing what words to use when describing 22q11DS to my child. |
| Child using 22q11DS as an excuse |  |
I worry that my child will use 22q11DS as an excuse for not attempting to overcome challenges. |
| Child feeling different because of 22q11DS |  |
I worry that knowing about 22q11DS will make my child feel different. |
2.4. Data collection
Study data were collected and managed using REDCap electronic data capture tools hosted at The Hospital for Sick Children [25]. REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies, providing: 1) an intuitive interface for validated data entry; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for importing data from external sources.
2.5. Statistical analysis
Statistical analysis was conducted using the IBM SPSS statistical software. Normality of the variables was assessed using the Shapiro-Wilk Test.
2.5.1. Likert scale association analysis
To assess differences between Likert scale responses, Friedman’s Test was used to obtain a Mean Rank to identify areas where many individuals either strongly agreed or disagreed. To assess association between Likert responses and categorical grouping variables, Kruskal-Wallis H Test and Chi-Square Test of Association were utilized. Spearman’s Correlation was used to compare the demographics to the Likert responses assessing barriers to discussion.
2.5.2. Survey 1 and 2 comparison
Differences between individual Likert responses of surveys 1 and 2 were compared using a Sign Test. To assess impact of the SCFT, a score difference was calculated between the survey scores. This score difference was compared with neutral, indicating no change, using One Sample T-Test for normal distribution, and One Sample Wilcoxon-Signed Rank Test for non-normal distribution. These were conducted as both two-tailed and one-tailed tests.
2.5.3. SCFT feedback responses
The Kruskal-Wallis Test was used to compare the level of information disclosed to the child against the Likert responses of the questions that targeted feedback for the SCFT. Responses to the feedback Likert questions were compared to neutral using a One Sample T-Test and One Sample Wilcoxon-Signed Rank Tests for normal and non-normal variables respectively, using both two-tail and one-tail approaches.
2.5.4. Post-hoc analysis
Post-hoc analysis was done to assess the Likert responses of individuals who had reported high confidence on survey 1, i.e. 9 or 10 on forward-coded variables and 0 or 1 on reverse-coded variables. A Two Sample T-Test was used for normally distributed variables, and Independent Sample Median Test was used for non-normally distributed variables. The responses of surveys 1 and 2 were compared between these individuals and those who did not indicate high confidence on survey 1.
3. Results
The following results demonstrate how the SCFT we developed and evaluated was able to successfully assist parents in having a discussion with their children about their genetic diagnosis.
3.1. Background information on children of participants
Of the 33 individuals who were recruited into the study, 20 participants completed survey 1 (61%), and 14 participants completed both surveys (42%). The demographics of participants can be found in Table 2. Parents took an average 2.7 years from the time of diagnosis to disclose information about the diagnosis to their child, with a range of 0 to 10 years. The mean age of disclosure was 7 years. Disclosure ranged from discussing syndrome-associated symptoms in a general manner to specifically providing the name of the condition.
Table 2.
Demographics.
| Characteristic | Frequency |
|---|---|
| Survey 1 (n = 20) | |
| Age (grade equivalent) | |
| 9 years (grade 4) | 4 |
| 10 years (grade 5) | 4 |
| 11 years (grade 6) | 7 |
| 12 years (grade 7) | 5 |
| Working grade level | |
| Grade 1 | 1 |
| Grade 2 | 5 |
| Grade 3 | 3 |
| Grade 4 | 4 |
| Grade 5 | 2 |
| Grade 6 | 4 |
| No value provided | 1 |
| Difference between expected and working grade | |
| 0 grades | 4 |
| 1 grade | 4 |
| 2 grade | 5 |
| 3 grade | 2 |
| 4 grade | 3 |
| 5 grade | 1 |
| No value | 1 |
| Age diagnosed with 22q11DS | Median: 3 years Range: prenatal (n = 2) to 11.5 years |
| Age when first discussed 22q11DS | Mean: 7.1 years Range: 3 to 11.5 years |
| Time between diagnosis and first discussion | Median: 2.7 years Range: 0 to 10 years |
| Informed child about 22q11DS | All responses; maximum informationa |
| Nothing | 1; 1 |
| That they have some health concerns | 7; 3 |
| The name of their condition (22q11DS) | 7; 1 |
| That their health problems are part of 22q11DS | 15; 15 |
| Diagnosis of learning disability | |
| Yes | 14b |
| No | 6 |
| Diagnosis of Autism Spectrum Disorder | |
| Yes | 2 |
| No | 17 |
| Comorbidity | |
| Yes | 6c |
| No | 14 |
| Survey 2 (n = 14) | |
| Who view the module with child | |
| Mother | 13 |
| Father | 1 |
| Other | 2d |
| Child was not present | 0 |
Notes: aFirst number includes responses where multiple options were selected, and second number includes only the highest level of information that was chosen. bDiagnoses of learning disabilities were primarily made by psychologists. cComorbidities include: Trisomy X, hearing loss, Incontinentia Pigmenti, cerebral cavernous malformation, 16q23.1 duplication, Autism Spectrum Disorder, Disruptive Mood Dysregulation Disorder, seizures, and immune deficiency. dOther individuals present include: grandmother, brother.
3.2. Responses to barriers
Analysis of the data from survey 1 using Friedman’s Test identified significant differences in overall distribution among the forward- and reverse-coded questions (p = 0.02 and 0.016 respectively). However due to limited sample size, post-hoc analysis to discern the ranking of the questions was not significant. According to the means and medians of survey 1 (Table 3), most individuals agreed or strongly agreed with feeling comfortable and prepared to talk to their children about 22q11DS, and being able to explain the condition (i.e. the forward-coded questions). Responses to the reverse-coded questions revealed that individuals were most concerned about the diagnosis affecting their children’s self-esteem (mean rank: 4.25), making them feel different (mean rank: 3.88), and not knowing how much information to provide when discussing the diagnosis (mean rank: 3.83). There were no significant overall differences in distribution of Likert responses for either forward- or reverse-coded questions for survey 2 (p > 0.05).
Table 3.
Likert questions asked in surveys 1 and 2 addressing barriers to communication, including responses to survey 1.
| Coding | Question | Mean | Median [IQR] |
|---|---|---|---|
| Forward | I am comfortable talking to my child about 22q11DS. | 7.9 | 9 [7, 10] |
| I feel prepared to talk to my child about 22q11DS. | 7.4 | 8 [5.25, 9] | |
| I know how to explain 22q11DS to my child. | 7.1 | 7 [5.25, 9] | |
| I think it would be valuable to have resources to help guide me in discussing the diagnosis with my child. | 8.2 | 8.5 [8, 10] | |
| Reverse | I struggle knowing what words to use when describing 22q11DS to my child. | 4.5 | 5 [2, 7] |
| I worry that knowing about 22q11DS will make my child feel different. | 5.8 | 5 [2.25, 9.75] | |
| I struggle knowing how much information to provide when talking about 22q11DS with my child. | 5.9 | 6 [3, 9] | |
| I worry that knowing about 22q11DS will affect my child’s self-esteem. | 6.5 | 8 [4.25, 9] | |
| I worry that my child will use 22q11DS as an excuse for not attempting to overcome challenges. | 5.5 | 6 [3.5, 7] | |
| I struggled with deciding at what age I should discuss the diagnosis of 22q11DS with my child. | 4.3 | 3.5 [0, 8.75] |
Notes: Possible responses ranged from 0 (strongly disagree) to 10 (strongly agree). The table specifies if the question was forward- or reverse-coded, and includes the mean and median responses for each question from survey 1 (n = 20). IQR (interquartile range) represents the responses between 25th and 75th percentiles, i.e. the middle 50% (n = 20).
Responses to the eight questions common to both surveys 1 and 2 were compared to determine if use of the SCFT impacted parents’ level of comfort, preparedness and perceived barriers with respect to disclosure (n = 14). Direct comparison of responses using Sign Test indicated no significant differences (p > 0.05). To assess if the change in scores between survey Likert scales was different than 0, One Sample T-Test and Wilcoxon-Signed Rank Test was conducted on the calculated difference (i.e., survey 2 Likert minus survey 1 Likert scores) against hypothesized difference value of 0. While no significant differences were found for two-tailed analysis, a one-tailed test identified a significant positive change for the questions asking about comfort (p = 0.033) and being able to explain 22q11DS (p = 0.0285), and a significant negative change for the question asking about self-esteem (p = 0.046).
The mean differences between surveys 1 and 2 also possessed a direction of change, meaning they moved in either a positive or negative direction on the Likert scale (n = 14). Response to each forward-coded Likert question had a positive mean difference, meaning most individuals agreed more strongly with the statements after viewing 22q and Me (Fig. 2). Responses to most reverse-coded questions yielded a negative mean score, meaning individuals more strongly disagreed with the reverse-coded questions after viewing 22q and Me. The only question response that did not follow this pattern addressed parents’ worry about 22q11DS making their child feel different, which had a positive mean score (Fig. 3).
Fig. 2.

Difference in means of Likert responses between surveys 1 and 2 for forward-coded questions. After viewing 22q and Me, participants tended to more strongly agree with these questions (n = 14).
Fig. 3.

Difference in means of Likert responses between surveys 1 and 2 for reverse-coded questions. After viewing 22q and Me, participants tended to more strongly disagree with almost every question, but more strongly agreed with worrying that their child will feel different (n = 14).
3.3. Trends in responses
Spearman’s correlation was used to determine if there was a relationship between Likert responses and participant characteristics (n = 20). Several relationships were identified between age at disclosure and responses to the Likert questions (Table 4), including a positive correlation between age at disclosure and concerns about self-esteem (ρ = 0.533, p = 0.028).
Table 4.
Correlations identified between age at disclosure and responses to the Likert questions.
| Likert question | Statistic | |
|---|---|---|
| Positive correlation | I worry that my child will use 22q11DS as an excuse for not attempting to overcome challenges. | ρ = 0.540, p = 0.025 |
| I worry that knowing about 22q11DS will affect my child’s self-esteem. | ρ = 0.533, p = 0.028 | |
| I struggle knowing how much information to provide when talking about 22q11DS with my child. | ρ = 0.550, p = 0.022 | |
| I worry that knowing about 22q11DS will make my child feel different. | ρ = 0.581, p = 0.014 | |
| Negative correlation | I know how to explain 22q11DS to my child. | ρ = −0.509, p = 0.037 |
| I am comfortable talking to my child about 22q11DS.a | ρ = −0.609, p = 0.036 |
Notes: aThis correlation was identified for survey 2. The remainder are for survey 1.
Post-hoc analysis assessed changes between surveys for individuals who indicated higher confidence on their responses to the questions on survey 1 (n = 14); that is, those who indicated 9 or 10 on forward-coded responses, and 0 or 1 on reverse-coded responses. To assess whether there was a decrease in confidence after viewing the SCFT, survey 1 and 2 score differences were assessed using Two Sample T-Test (non-parametric equivalent: independent sample median test), and directionality of the score differences was assessed. Significant results were identified for individuals who indicated high confidence on survey 1 to the question asking about comfort level (n = 7/14) and being able to explain 22q11DS (n = 5/14) (Fig. 4). For example, those who indicated high confidence on being able to explain 22q11DS to their children on survey 1 had a lower mean change than those with lower confidence (mean change = -0.80 and 2.56, respectively, p = 0.007), and the mean change was in the opposite direction. That is, those who felt like they were better able to explain 22q11DS to their child prior to viewing 22q and Me had a negative mean change, while those who initially indicated lower confidence had a positive mean change.
Fig. 4.

Comparing mean difference between surveys 1 and 2 for individuals who indicated high confidence on survey 1 to individuals who indicated low confidence on survey 1. The Able to Explain and Comfortable groups refer to individuals who indicated high initial confidence on the questions, “I know how to explain 22q11DS to my child” and “I am comfortable talking to my child about 22q11DS” respectively, and the bars show the mean difference for the responses to the questions on the left. Each high and low confidence comparison is statistically significant (n = 14).
3.4. Feedback
To assess participants’ opinions regarding the SCFT, the responses were compared to neutral. For Likert responses, 5 was considered neutral. For the question that asked about the amount of information provided in the SCFT, 1 was used as neutral, since the two responses were “too little” and “too much”. A One Sample T-Test was used to assess normally distributed variables, while non-normally distributed variables were assessed using a One Sample Wilcoxon-Signed Rank Test. The majority of responses were significantly different from neutral in the positive direction, including questions about the SCFT being easy to follow (median difference from neutral = 5, p = 0.01) and addressing concerns (mean difference from neutral = 1.71, p = 0.031) (Fig. 5). In terms of the amount of information provided in the SCFT, while responses were significantly different from neutral (median difference = 0, two-tail p = 0.046) as the median difference calculated was “0”, skewness was evaluated (--1.035) and confirmed that responses had a negative skew.
Fig. 5.

Mean Likert response for questions regarding feedback for the SCFT. Asterisk (*) indicates mean is significantly different from neutral (i.e. 5), assessed via a two-tailed test. Responses to whether the parents will use 22q and Me as a future reference were significantly different from neutral only when using a one-tailed test. (n = 14). Statistics: aMedian difference from neutral = 5, p = 0.006. bMean difference from neutral= 3.43, p < 0.001. cMedian difference from neutral = 3.5, p = 0.006. dMedian difference from neutral = 4, p = 0.005. eMedian difference from neutral = 5, p = 0.01. fMean difference from neutral = 3.13, p < 0.001. gMedian difference from neutral = 3.50, p = 0.036). hMean difference from neutral = 3.42, p < 0.001. iMean difference from neutral = 1.71, p = 0.031.
Review of the feedback from the free-text questions demonstrated overwhelmingly positive comments about 22q and Me. Table 5 provides examples of both supportive and constructive feedback. Constructive feedback included a suggestion to provide more information about the health problems associated with 22q11DS. Parents also suggested changes to some of the technical aspects of the SCFT including the addition of a narrator, and an option to return to the previous slide, rather than only proceeding forward.
Table 5.
Examples of some of the feedback from participants provided in free-text questions.
| Supportive Feedback | Constructive Feedback |
|---|---|
|
[The SCFT] provided a nice outline of the major areas to discuss. (Participant 1) [...] my son found it easy to identify with the characters. (Participant 17) While reading we were able to comment "oh, that's me" or "Oh, that's you". (Participant 6) She identified with one of the characters (Amy) [...]. [and] In each section she found something to point to herself. (Participant 12) As a role model for parents, this too is perfect as it shows how to structure the info and keep it simple. The examples of other kids was a great captivator of attention and was more meaningful than me just saying "well, some kids have this and some get that". (Participant 6) Thank you for this tool. We have wanted to disclose the diagnosis and introduce the 22q information to our child around this age, but it has been a very scary and overwhelming idea with lots of doubts about what to say and how to say it. This tool really provided us with a platform to start with and gave us confidence for having the conversation. It has allowed us to move forward where we would have been stuck. (Participant 16) Having the visual of the video and kid friendly graphics was very helpful. We have discussed this with our son before, but the visual for the genetics section helped with his comprehension. (Participant 19) |
Our child is 12, so at the upper range of the age this module was designed for. It was still useful for her, but would have been even more so when she was a little younger. (Participant 7) I found it to be more appropriate for younger children. (Participant 21) The focus of one deficit area for each child made it seem a little more simplistic. These kids have complicated diagnoses and multiple diagnoses. While it would be impossible to profile everything, a mention of additional issues in some way might be helpful. It did allow for me to initiate a conversation about this though. (Participant 19) More about hospitals, and blood work, and traveling for appointments, for the age group I think they can handle a little more of the tough stuff. (Participant 9) A wider range of 22q complications would be helpful so that kids with other manifestations do not feel left out or even odd within 22q. My child keep waiting for his difficulties to be talked about. (Participant 10) Wonder if it was narrated if it would appeal to kids more. My daughter hates reading so I read to her so she could concentrate on the content and not on decoding. (Participant 1) It would have been nice to be able to go back a slide if necessary. (Participant 16) |
4. Discussion and conclusion
4.1. Discussion
Our SCFT is a novel interactive educational tool that was developed to be used by parents and their children to facilitate conversations regarding disclosure of a diagnosis of 22q11DS as well as discussion following disclosure. While there are resources available that provide parents with information about genetic conditions, to our knowledge, this tool is the first of its kind to assist parents in having a conversation with their children about their diagnosis.
Most of the individuals (19/20) who completed survey 1 reported disclosing some information regarding the diagnosis of 22q11DS to their child, prior to viewing the SCFT. However, many acknowledged they had struggled with different aspects of the communication process. After viewing the SCFT, participants felt they were more comfortable and prepared to talk to their children about 22q11DS, and better equipped to explain the condition. The SCFT also helped parents to find the language to use when describing 22q11DS, and in determining how much information to provide. Finally, after viewing 22q and Me, parents felt less worried about 22q11DS affecting their children’s self-esteem and the possibility of the diagnosis being used as an excuse for not to attempting to overcome challenges. Due to the small sample size, the results were not statistically significant, but suggest that 22q and Me successfully addressed barriers to discussion and disclosure for the majority of participants.
One barrier that 22q and Me did not successfully address was parents’ worry about their children feeling different from their peers after hearing about their diagnosis. Participants indicated they worried more about this after viewing the SCFT. This could relate to the tool’s focus on differences attributable to 22q11DS. This finding has been previously reported in the literature, including one study that showed that children with epilepsy avoid speaking about their condition to their parents because it is a reminder they are different from their family and peers [26].
There were a number of correlations identified with regard to the child’s age at which parents disclosed the diagnosis of 22q11DS and concerns regarding specific barriers. As the age of disclosure increased, parents felt more concerned that the diagnosis could make their child feel different, affecting their self-esteem, and be used as an excuse for not attempting to overcome challenges. Parents also struggled more with how much information to provide and felt less comfortable and confident that they could explain 22q11DS to their children. In this study, the correlation between age of disclosure and barriers to disclosure could be due to parents’ concerns regarding disclosure. As a result, parents with more significant concerns might have delayed speaking to their children about their diagnosis, resulting in an older age of disclosure for those children. Studies have shown that earlier disclosure leads to children assimilating their condition into their self-identity, and delayed disclosure can lead to feelings of family conflicts and secrecy [5,6]. Therefore, providing parents with the tools to facilitate conversations regarding a diagnosed condition in their children would be of tremendous value.
The SCFT enabled participants to feel more comfortable and prepared to talk to their children about their diagnosis. However, this comfort and preparedness was correlated with the degree of parental confidence prior to viewing the SCFT. Participants who initially strongly agreed with feeling comfortable talking to their children about 22q11DS felt less comfortable and less prepared to talk to their children after viewing the SCFT. They also indicated they were less able to explain 22q11DS to their child and struggled more with knowing what words to use when describing the condition.
This phenomenon could be related to the Dunning-Kruger effect, which states that as an individual’s skills increases, their confidence in their performance decreases [27]. While this study did not formally assess the knowledge and communication skills of participants prior to and following viewing the SCFT, it suggests that the parents may have acquired novel information they had not considered previously about 22q11DS, resulting in a decrease in confidence regarding their overall knowledge of this condition.
Parental feedback on 22q and Me overall was positive. Most participants felt that the SCFT was helpful and addressed their concerns regarding talking to their children about 22q11DS. Parents reported that the content was age appropriate, easy to follow and that their children appeared to enjoy the SCFT and were engaged while using it. Most participants indicated that 22q and Me would have been helpful the first time they talked to their children about 22q11DS and would recommend it to other parents of children with 22q11DS. Many participants indicated they would use the SCFT as a future reference; however, there was less agreement with this statement than with the others. While many participants thought there was an appropriate amount of information included, some thought that the amount of information was too little. This is likely because the SCFT addressed the common features of 22q11DS, but not all of the concerns specific to their child. This may be why parents felt this tool would be more useful for a first-time disclosure, rather than a future reference. While we did focus on a single clinical feature of 22q11DS for each character for the sake of simplicity, an updated version of the SCFT could include characters with multiple features which would be a better representation of the real-life experience. Overall, parents evaluated 22q and Me positively both as a tool and as a means of addressing their conversational concerns.
Limitations of this study include the small sample size, which limited the analysis and potential for statistical significance. Additionally, our SCFT was designed specifically for children between the ages of 9 to 12 years old and would need to be modified in order to be helpful to parents of older or younger children. Finally, there was likely an ascertainment bias as most of the participants had already initiated some discussion with their children about their diagnosis. However, if the SCFT was deemed helpful by families with some experience, it may be even more valuable to families with less experience.
4.2. Innovation
We have demonstrated the utility of a SCFT to facilitate communication about complex genetic diagnoses between parents and their children. Our SCFT, 22q and Me was shown to be effective in assisting parents with discussions about the diagnosis of 22q11DS with their children. The barriers to communication in disclosing a diagnosis are not unique to families who have a child with 22q11DS but exist for other genetic and non-genetic conditions. The components of this innovative tool may be generalized to any genetic syndrome, and include syndrome-specific information in a story format that provides parents with appropriate language, using characters that highlight the individuals’ strengths, and messaging that targets condition-specific barriers.
4.3. Conclusion
The SCFT was an effective tool for addressing barriers identified in the literature, and parents felt this was a valuable resource. Overall, 22q and Me was successful in facilitating communication about 22q11DS between parents and their children. 22q and Me will be edited based on the feedback provided by the families and will shared more broadly with the 22q11DS community.
Funding
This work was supported by the McLaughlin Centre at the University of Toronto and the Jane Engelberg Memorial Fellowship Student Research Award, Provided by the Engelberg Foundation to the National Society of Genetic Counselors, Inc.
Declaration of Competing Interest
The authors declare no conflicts of interest.
Acknowledgements
The authors would like to thank AboutKidsHealth for hosting the SCFT, and the families who participated in this research.
I confirm all patient/personal identifiers have been removed or disguised so the patient/person(s) described are not identifiable and cannot be identified through the details of the story.
References
- 1.Dennis A., Howell S., Cordeiro L., Tartaglia N. “How should i tell my child?” Disclosing the diagnosis of sex chromosome aneuploidies. J Genet Couns. 2015;24:88–103. doi: 10.1007/s10897-014-9741-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gallo A.M., Angst D., Knafl K.A., Hadley E., Smith C. Parents sharing information with their children about genetic conditions. J Pediatr Health Care. 2005;19:267–275. doi: 10.1016/j.pedhc.2005.05.008. [DOI] [PubMed] [Google Scholar]
- 3.Metcalfe A., Plumridge G., Coad J., Shanks A., Gill P. Parents and children’s communication about genetic risk: a qualitative study, learning from families experiences. Eur J Hum Genet. 2011;19:640–646. doi: 10.1038/ejhg.2010.258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wiley K.A., Demo E.M., Walker P., Osborne Shuler C. Exploring the discussion of risk of sudden cardiac death. Pediatr Cardiol. 2016;37:262–270. doi: 10.1007/s00246-015-1272-8. [DOI] [PubMed] [Google Scholar]
- 5.Rowland E., Metcalfe A. Communicating inherited genetic risk between parent and child: A meta-thematic synthesis. Int J Nurs Stud. 2013;50:870–880. doi: 10.1016/j.ijnurstu.2012.09.002. [DOI] [PubMed] [Google Scholar]
- 6.McConkie-Rosell A., Del Giorno J., Heise E.M. Communication of genetic risk information to daughters in families with fragile X syndrome: the parent’s. Perspective. 2011;14:384–399. doi: 10.1080/10810730902873927.Testing. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Goldman A., Metcalfe A., Macleod R. The process of disclosure: mothers’ experiences of communicating x-linked carrier risk information to at-risk daughters. J Genet Couns. 2018;27:1265–1274. doi: 10.1007/s10897-018-0251-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Middleton J., Calam R., Ulph F. Communication with children about sickle cell disease: A qualitative study of parent experience. Br J Health Psychol. 2018;23:685–700. doi: 10.1111/bjhp.12311. [DOI] [PubMed] [Google Scholar]
- 9.Gallo A.M., Knafl K.A., Angst D.B. Vol. 24. 2009. NIH Public Access; pp. 194–204. [DOI] [Google Scholar]
- 10.Faux D., Schoch K., Eubanks S., Hooper S.R., Shashi V. Assessment of parental disclosure of a 22q11.2 deletion syndrome diagnosis and implications for clinicians. J Genet Couns. 2012;21:835–844. doi: 10.1007/s10897-012-9535-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Deatrick D., Jeff A., Cawley J. A Guide to Creating and Evaluating Patient Materials Guidelines for Effective Print Communication. 2010. http://www.mainehealth.org/workfiles/MH_LRC/MH_PrintGuidelines_Intranet.pdf%5Cnwww.mainehealth.org/healthliteracy
- 12.Delaine K. A computer-based interactive multimedia program to reduce HIV transmission for women with intellectual disability. J Intellect Disabil Res. 2012;56:371–381. doi: 10.1111/j.1365-2788.2011.01482.x.A. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Heimann M., Nelson K., Tjus T., Gillberg C. Increasing reading and communication-skills in children with autism through an interactive multimedia computer-program. J Autism Dev Disord. 1995;25:459–480. doi: 10.1007/BF02178294. [DOI] [PubMed] [Google Scholar]
- 14.Harris S., Lakdawala N.K., Neumann C., Cirino A.L., Greenberg J.O., Carr C.W., et al. The uptake of family screening in hypertrophic cardiomyopathy and an online video intervention to facilitate family communication. Mol Genet Genomic Med. 2019:1–10. doi: 10.1002/mgg3.940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Flores D.D., Rosario A.A., Bond K.T., Villarruel A.M., Bauermeister J.A. Parents ASSIST (Advancing Supportive and Sexuality-Inclusive Sex Talks): iterative development of a sex communication video series for parents of Gay, Bisexual, and Queer Male Adolescents. J Fam Nurs. 2020 doi: 10.1177/1074840719897905. [DOI] [PubMed] [Google Scholar]
- 16.Davis S.A., Carpenter D.M., Blalock S.J., Budenz D.L., Lee C., Muir K.W., et al. A randomized controlled trial of an online educational video intervention to improve glaucoma eye drop technique. Patient Educ Couns. 2018;102(5):937–943. doi: 10.1016/j.pec.2018.12.019. [DOI] [PubMed] [Google Scholar]
- 17.Patino M.I., Kraus P., Bishop M.A. Implementation of patient education software in an anticoagulation clinic to decrease visit times for new patient appointments. Patient Educ Couns. 2019;102:961–967. doi: 10.1016/j.pec.2018.12.023. [DOI] [PubMed] [Google Scholar]
- 18.Goessl C., Estabrooks P., You W., Britigan D., Dealba A., Almeida F. Effectiveness of DVD vs. group-initiated diabetes prevention on information uptake for high & low health literacy participants. Patient Educ Couns. 2019;102:968–975. doi: 10.1016/j.pec.2018.12.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Metcalfe S.A. Genetic counselling, patient education, and informed decision-making in the genomic era. Semin Fetal Neonatal Med. 2017 doi: 10.1016/j.siny.2017.11.010. [DOI] [PubMed] [Google Scholar]
- 20.Jimison H.B., Sher P.P., Appleyard R. Y.C.-61298 LeVernois, The use of multimedia in the informed consent process. J Am Med Inform Assoc. 1998;5:245–256. doi: 10.1136/jamia.1998.0050245. ST-The use of multimedia in the informed. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.McDonald-McGinn D.M., Sullivan K.E., Marino B., Philip N., Swillen A., Vorstman J.A.S., et al. 2016. 22Q11.2 Deletion Syndrome; pp. 1–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Shprintzen R.J. Velo-Cardio-Facial syndrome: 30 years of study. Dev Disabil Res Rev. 2008;14:3–10. doi: 10.1002/ddrr.2.Velo-Cardio-Facial. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Blagojevic C., Heung T., Theriault M., Tomita-mitchell A., Chakraborty P., Kernohan K., et al. 2021. Estimate of the contemporary live-birth prevalence of recurrent 22q11.2 deletions: a cross-sectional analysis from population-based newborn screening. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.McFarlane I.M., Veach P.M., LeRoy B. Oxford University Press; Oxford: 2014. Genetic Counseling Research: A Practical Guide. [Google Scholar]
- 25.Harris P.A., Ph D., Taylor R., Thielke R., Ph D., Payne J., et al. Research electronic data capture (REDCap) - a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2010;42:377–381. doi: 10.1016/j.jbi.2008.08.010.Research. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.O’Toole S., Lambert V., Gallagher P., Shahwan A., Austin J.K. “I don’t like talking about it because that’s not who i am”: challenges children face during epilepsy-related family communication. Chronic Illn. 2016;12:216–226. doi: 10.1177/1742395316644307. [DOI] [PubMed] [Google Scholar]
- 27.Kruger J., Dunning D. Unskilled and unaware of it: how difficulties in recognizing one ’ s own incompetence lead to inflated self-assessments. J Pers Soc Psychol. 1999;77:1121–1134. doi: 10.1037//0022-3514.77.6.1121. [DOI] [PubMed] [Google Scholar]