

Abstract
Objective:
To examine associations between economic residential segregation and prevalence of healthy and unhealthy eating markers.
Design:
Cross-sectional. A stratified sample was selected in a three-stage process. Prevalence of eating markers and their 95 % CI were estimated according to economic residential segregation: high (most segregated); medium (integrated) and low (less segregated or integrated). Segregation was measured at the census tract and assessed using the Getis–Ord local  statistic based on the proportion of heads of household in a neighbourhood earning a monthly income of 0–3 minimum wages. Binary logistic regression using generalized estimating equations were used to model the associations.
statistic based on the proportion of heads of household in a neighbourhood earning a monthly income of 0–3 minimum wages. Binary logistic regression using generalized estimating equations were used to model the associations.
Setting:
Belo Horizonte, Brazil.
Participants:
Adults (n 1301) residing in the geographical environment (178 census tracts) of ten units of the Brazilian primary-care service known as the Health Academy Program.
Results:
Of the 1301 participants, 27·7 % lived in highly segregated neighbourhoods, where prevalence of regular consumption of fruit was lower compared with more affluent areas (34·6 v. 53·2 %, respectively). Likewise, regular consumption of vegetables (70·1 v. 87·6 %), fish (23·6 v. 42·3 %) and replacement of lunch or dinner with snacks (0·8 v. 4·7 %) were lower in comparison to more affluent areas. In contrast, regular consumption of beans was higher (91·0 v. 79·5 %). The associations of high-segregated neighbourhood with consumption of vegetables (OR = 0·62; 95 % CI 0·39, 0·98) and beans (OR = 1·85; 95 % CI 1·07, 3·19) remained significant after adjustments.
Conclusions:
Economic residential segregation was associated with healthy eating markers even after adjustments for individual-level factors and perceived food environment.
Keywords: Urban health, Residential segregation, Food consumption, Brazil
Residential segregation occurs when two or more social groups of people, categorized by a variety of scales (race, ethnicity, skin colour or socio-economic status (e.g. income)), live separately from one another, in different parts of the urban environment, and with different spatial distribution(1). Accordingly, racial residential segregation is a physical separation of the races by residence. Along these lines, economic residential segregation is a physical separation of two or more groups of people based on their income by residence (into homogeneous neighbourhoods)(1,2).
Segregated spaces, categorized by race or income, promote varied exposure to health issues, especially when comparing the less with the more affluent and integrated neighbourhoods(3–7). As a result, segregation is one possible mechanism of racism, the spatial manifestation of inequalities and one of the fundamental causes of disparities in health(2).
Associations between racially segregated neighbourhoods and proximity to availability of ultra-processed foods (fast foods, soft drinks and frozen meals) have been reported in the literature. In the USA, poor and predominantly black neighbourhoods are geographically associated with fast-food restaurants(8) and are further from stores selling healthy foods(9–11). In Brazil, scientific evidence has revealed the association between economic disadvantage and concentration of healthy food stores in affluent areas(12,13).
The characteristics of a neighbourhood regarding access to food may be a factor contributing to differences in food consumption among residents, probably linking racially segregated urban neighbourhoods to disparities in food consumption(10). Some studies showed a relationship between racial/ethnic segregation and diets with lower amounts of fat and processed foods(14,15), high expenditure on fruits and vegetables(16) and higher sodium and potassium intakes(17). However, the mechanisms explaining the associations between food consumption and economic residential segregation have not been fully understood.
The literature tends to focus on racial/ethnic segregation(17,18), and there are few recent studies on social class/economic residential segregation in Brazil(19). Studies on racial/ethnic segregation and food consumption have been conducted in the USA, but it is not clear if the mechanisms are similar in low- and middle-income country contexts. In Brazil, for instance, socio-economic classes are more commonly used in studies, because the Brazilian racial classification is very complex and makes it difficult to transfer common measures from the USA context to Brazil(19).
Calculating the economic residential segregation in an urban area, represented by the 6th most populous Brazilian city, testing whether residing in high-segregation neighbourhoods is associated with food consumption can contribute to the understanding of how residential segregation occurs in a city with lower-middle-income economy and how it is associated with disparities in food consumption. Besides, this may support evidence-based policies and interventions.
We hypothesized that individuals residing in highly segregated areas would report a lower prevalence of regular consumption of foods such as fruits, vegetables and fish, and higher or equal prevalence of regular consumption of foods such as soft drinks, artificial juice, sweet foods and/or other ultra-processed food products, in comparison to those residing in low-segregated areas. We also hypothesized the possible exception of beans, since different Brazilian studies indicate a higher prevalence of regular bean consumption among lower-income populations(20,21).
Regarding the replacement of lunch or dinner, although lacking a formal hypothesis, we aimed to better understand this very contemporary food behaviour in the Brazilian urban context. Thus, in order to expand our knowledge and understanding of the relationship between economic residential segregation and food consumption, the aim of the present study was to examine associations between the prevalence of healthy and unhealthy eating markers and economic residential segregation.
Methods
Study population
The current analysis examined data from the ‘MOVE-se Academias (2014–2015) study’, a cross-sectional study conducted by the Belo Horizonte Observatory for Urban Health of the Universidade Federal de Minas Gerais. The MOVE-se Academias study integrates the project ‘Health Academy: evaluation of physical activity promotion programs in Brazil’. It consists of a home-based health survey, for which the sample includes the resident population (users and non-users) in the geographical environment of the Health Academy Program (HAP; Programa Academia da Saúde (PAS) in Portuguese), distributed among the nine health districts of Belo Horizonte(22).
The HAP are public spaces that provide – for free, under the Unified Health System – physical activity programmes, health promotion initiatives including eating and other community education activities to users over 18 years of age(23).
The HAP was implemented in Belo Horizonte in 2006, through participatory mechanisms mostly, and therefore is located primarily in vulnerable areas. Currently, there are seventy-eight units with maximum capacity estimated at 400 users per unit(23,24).
Study sample
A probabilistic sample design was adopted to select the population using clusters in three stages: (i) ten HAP units were randomly selected from the list provided by the programme management, in which three of them (inherited from a previous study in 2008–2009) had probability equal to 1; (ii) census tracts, selected with distinct probabilities according to the proximity of the HAP (e.g. census tracts located at the HAP unit had probability of 1; census tracts located up to 500 m from any other unit had 2·4 greater chance of being selected in comparison to a unit 500 m away) and with sample size proportional to the total number of sectors surrounding each sampled HAP unit; and (iii) households, selected by means of systematic sampling based on the number of households per census tract of the Census 2010. In each household, one adult resident (aged 18 years or more) was selected according to the quota established by sex, age range and occupation.
HAP units were eligible if they met the following criteria: (i) located in the districts that participated in the baseline survey of 2008–2009; (ii) were implemented before the first semester of 2013; and (iii) were not directed to special groups or located in specific places, such as the university.
The addresses of the selected HAP units were georeferenced, and the Euclidean distances between the centroid of each census tract and the nearest HAP unit were calculated. The eligible census tracts were: (i) within a radius of 1000 m of the ten HAP units; and (ii) with more than fifty households. Out of the eligible census tracts, 246 were selected. Census tracts with only one interview were excluded (n 68), totalling seventy-five participants. Household interviewees – either included or excluded – did not differ in the analytic sample with regard to sex, age, income and education. A detailed description of the Move-se Academias study design and survey has been published elsewhere(22).
For the purpose of the present study only non-users living in the geographical areas of the ten HAP units were included, since HAP users were dissimilar from non-users in several health aspects, including food consumption and physical activity(22). The final sample totalled 1301 participants distributed in 178 census tracts.
Data collection
Household face-to-face interviews and anthropometric measurements (weight and height) were conducted by trained interviewers, with a questionnaire gathering sociodemographic, health habits and behaviour information.
Measures
Residential segregation
The unit of analysis adopted was the census tract. The 2010 Brazil Census data(25) were used to determine the proportion of heads of household in a census tract earning a monthly income of 0–3 minimum wages (approximately 0 to $US 900·00, in 2010), based on prior observational studies of economic segregation in Brazil(19,26). The cut-off point, 0–3 minimum wages, also corresponded to the average monthly income of Brazilians in 2015(27), the year of the survey, and the median income of the sample selected for the Move-se Academias study.
Economic residential segregation was calculated for all census tracts of the city using the Hot Spot Analysis Tool in ArcGIS version 10.3. Census tracts were excluded if the resident population was zero, or if data were omitted by the Census 2010 because of safety reasons, or if the total number of heads of household with a monthly income of 0–3 minimum wages was zero. A total of 3833 tracts of Belo Horizonte city were analysed; from these, 178 tracts were analysed in the Move-se Academias study in order to examine the association between economic residential segregation and individual food consumption.
The Getis–Ord local statistic (‘ statistic’ hereafter) was used to measure the spatial association and to evaluate the spatial clustering of high or low values among census tracts (i.e. census tract with higher proportion of households with 0–3 minimum-wage income surrounded by other census tracts with higher proportion of households with 0–3 minimum-wage income)(28,29). The statistic is a spatially weighted Z-score representing how much a neighbourhood’s (census tract) income composition (proportion of households with 0–3 minimum-wage income) deviates from the larger city (Belo Horizonte).
Census tracts were weighted using a first-order rook spatial weight matrix. Higher and positive Z-scores represent census tracts that are more segregated (i.e. census tract with higher proportion of households with 0–3 minimum-wage income surrounded by other census tracts with a higher proportion of households with 0–3 minimum-wage income or over-representation of the high proportion of heads of household in a neighbourhood earning a monthly income of 0–3 minimum wages), while lower and negative scores account for census tracts that are less segregated (i.e. census tract with a lower proportion of households with 0–3 minimum-wage income surrounded by other census tracts with lower proportion of households with 0–3 minimum-wage income or under-representation of the high proportion of heads of household in a neighbourhood earning a monthly income of 0–3 minimum wages).
Three categories of residential segregation were created: high, statistic ≥1·96; medium, statistic between 0 and 1·96; and low, statistic <0. The high segregation category corresponds to statistically significant clustering of high values (α = 0·05) and the low segregation category corresponds to the absence of any clustering (integrated neighbourhoods) or areas in which the group of heads of household earning a monthly income of 0–3 minimum wages is significantly under-represented, clustering of low values ( statistic <−1·96). These categories were combined since the frequency of occurrence of low category described above was very small(7).
Individual-level outcome
Healthy eating markers were defined as regular consumption of fruits (five or more times per week), vegetables (five or more times per week), beans (five or more times per week) and fish (at least once per week). On the other hand, unhealthy eating markers were defined as consumption of meat or chicken with excess fat (individuals who reported consuming meat with excessive fat and/or chicken with skin); regular consumption of soft drinks or artificial juice (five or more times per week); regular consumption of sweet foods including cakes, chocolates, cookies and candy (five or more times per week); and having sandwiches, pizzas or other ultra-processed food products for lunch or dinner (seven days per week).
The ‘regular’ classification was based on the Surveillance System for Risk and Protection Factors for Chronic Diseases by Telephone Survey (VIGITEL)(30). The seven-day cut-off point for the variable ‘regular replacement of lunch or dinner with snacks’ was used as a marker of a more specific and selected habit in order to be a proxy for those individuals whose meal-replacement habit occurs every day, which is considered not healthy(31).
The food eating markers above, considering the risk or protection factors for the occurrence of chronic non-communicable diseases, were based on the following questions employed by the National Health Survey (NHS) conducted in Brazil in 2013(32):
-
1.
‘How many days a week do you usually eat fruit? (a) 1–2, (b) 3–4, (c) 5–6, (d) Every day, (e) Almost never, (f) Never’.
-
2.
‘How many days of the week do you usually eat vegetables, such as lettuce, tomato, cabbage, carrots, chayote (not including potato, cassava or yam)? (a) 1–2, (b) 3–4, (c) 5–6, (d) Every day, (e) Almost never, (f) Never’.
-
3.
‘How many days a week do you usually eat beans? (a) 1–2, (b) 3–4, (c) 5–6, (d) Every day, (e) Almost never, (f) Never’.
-
4.
‘How many days a week do you usually eat fish? (a) 1–2, (b) 3–4, (c) 5–6, (d) Every day, (e) Almost never, (f) Never’.
-
5.
‘When you eat red meat, do you usually: (a) Cut off excess of visible fat, (b) Eat it with fat?’; ‘When you eat chicken, do you usually: (a) Cut off the skin, (b) Eat it with skin?’.
-
6.
‘How many days a week do you usually drink soft drinks (or artificial juice)? (a) 1–2, (b) 3–4, (c) 5–6, (d) Every day, (e) Almost never, (f) Never’.
-
7.
‘How many days a week do you usually eat sweet foods, such as slices of cake or pie, chocolates, sweets, biscuits or sweet biscuits? (a) 1–2, (b) 3–4, (c) 5–6, (d) Every day, (e) Almost never, (f) Never’.
-
8.
‘How many days a week do you replace lunch or dinner meals by sandwiches, or pizza? (a) 1–2, (b) 3–4, (c) 5–6, (d) Every day, (e) Almost never, (f) Never’.
These indicators are shared by the VIGITEL and the NHS(21). Thus, although no study on the data collected by the NHS has been conducted yet, these indicators had their validity analysed by VIGITEL(33–35).
Individual-level covariates
Individual sociodemographic characteristics included age (in years), sex (male or female), race/skin colour based on the 2010 Brazil Census questions (white, brown (pardos in Portuguese) and black), monthly income in minimum wages (in Brazilian Reals) and schooling level (0–4, 5–8, 9–11 and >12 years). In addition, we included health behaviours and biological risk factors that could confound the association between segregation and food consumption, such as: length of residence in the neighbourhood (years); health status (self-rated health); practice of physical activities(32) (‘Has practiced some type of physical exercise or sports in the last three months? Yes or No’); and nutritional status based on BMI.
BMI was calculated by dividing the patients’ measured weight (in kilograms) by the square of their measured height (in metres). Excess weight was categorized as BMI ≥ 25 kg/m2 (overweight) and BMI ≥ 30 kg/m2 (obesity)(36).
Finally, we included the perceived neighbourhood food environment, which could confound or partially mediate the association between segregation and food consumption. The perceived neighbourhood food environment was assessed using a three-item scale about variety, quality and price of fruits and vegetables: (i) ‘In your neighbourhood, do you find a great variety of fresh fruits, vegetables and vegetables for sale? (a) No, (b) Yes, (c) Do not know’; (ii) ‘Are the fresh fruits and vegetables in your neighbourhood of high quality? (a) No, (b) Yes, (c) Do not know’; and (iii) ‘Are the fresh fruits and vegetables in your neighbourhood on sale for an affordable price? (a) No, (b) Yes, (c) Do not know’. These questions were cross-culturally adapted from a prior work (the Multi-Ethnic Study of Atherosclerosis), with a moderatereliability(19,37). Perception of the food environment was used as a binary variable (low food environment perception: yes/no). Low perceived food environments were considered when the answers to all three questions were ‘no’.
Statistical analysis
A descriptive analysis of quantitative variables was performed using means and 95 % CI. Frequency distributions were calculated for categorical variables. Comparison of 95 % CI was used to identify any differences between selected sample characteristics by categories of economic residential segregation (high, medium and low).
To examine the association between segregation and prevalence of healthy and unhealthy food eating markers, we estimated the OR and its respective 95 % CI with binary logistic regression using generalized estimating equations, separately for each outcome. Generalized estimating equations and an exchangeable correlation structure were used because the observations were grouped in one specific structure (i.e. individuals were nested within census tracts)(38).
In our analyses, we adjusted for covariates associated with economic residential segregation and food consumption as potential confounders or mediators. Our first multivariate regression model (Model 1) was adjusted for demographic status (age, sex and race/skin colour). Model 2 was further adjusted for schooling level and family income. Model 3 was adjusted by self-rated health status and nutritional status (BMI, kg/m2), and Model 4 was further adjusted for perceived neighbourhood food environment.
All analyses were performed using the statistical software package Stata version 13 and accounted for the sampling complex design and unequal probabilities of selection. The manipulation of the geographic data was carried out using ArcMap version 10.3 (http://www.esri.com/software/arcgis/index.html). We used a significance level of 5 %.
The study was approved by the Research Ethics Committee of the Medical School, Universidade Federal de Minas Gerais (640.920 of 8 May 2014). All interviewees were informed about the objectives of the research and signed the informed consent form agreeing to participate in the study.
Results
Residential segregation in Belo Horizonte, a Brazilian city
We analysed 3833 census tracts in Belo Horizonte. Segregation scores ranged from −6·64 to 3·92, and approximately 18·9 % of the total sample were in high (Z-score ≥ 1·96 and P ≤ 0·05), 41·0 % in medium and 40·0 % in low areas of segregation (Fig. 1).
Fig. 1.
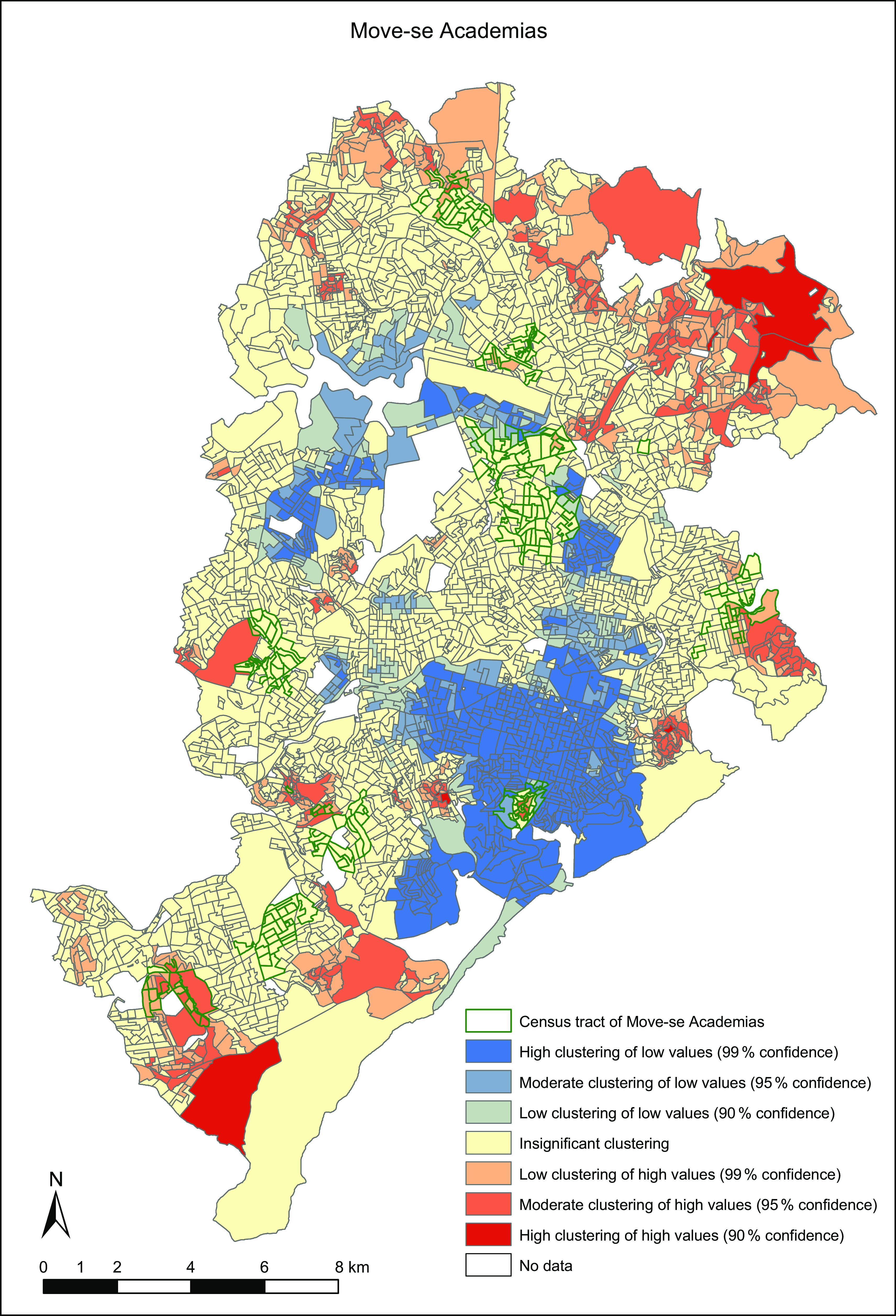
Results of Getis–Ord local statistical analysis based on the proportion of households with 0–3 minimum wages; MOVE-se Academias study, Belo Horizonte, Brazil, 2014–2015
Sample characteristics
We analysed 178 census tracts in Move-se. Segregation scores ranged from −3·25 to 3·03, and approximately 18·5 % of them were in high (Z-score ≥ 1·96 and P ≤ 0·05), 61.2 % in medium and 20.3 % in low segregation areas (Fig. 1). Of the 1301 participants of Move-se, 60·7 % were women. The mean age of the participants was 43·2 (95 % CI 41·8, 44·7) years and the mean segregation score and length of residence were 1·0 (95 % CI 0·9, 1·11) and 18·4 (95 % CI 17·3, 19·6) years, respectively (Table 1).
Table 1.
Sample characteristics overall and by categories of economic residential segregation; MOVE-se Academias study, Belo Horizonte, Brazil, 2014–2015
| Economic residential segregation | ||||||||
|---|---|---|---|---|---|---|---|---|
| Overall sample (n 1301) |
Higha (n 361) |
Mediumb (n 711) |
Lowc (n 299) |
|||||
| Mean or % | 95 % CI | Mean or % | 95 % CI | Mean or % | 95 % CI | Mean or % | 95 % CI | |
| Mean local statistic |
1·0 | 0·9, 1·1 | 2·4 | 2·3, 2·4b,c | 1·2 | 1·1, 1·3a,c | −1·1 | −1·4, 0·9a,b |
| Mean age (years) | 43·2 | 41·8, 44·7 | 44·0 | 40·5, 47·4 | 41·3 | 39·6, 42·9c | 48·9 | 46·8, 51·0b |
| Sex, female (%) | 60·7 | 57·2, 64·1 | 57·4 | 49·7, 64·7 | 60·6 | 56·0, 65·1 | 64·6 | 57·3, 71·3 |
| Race* (%) | ||||||||
| White | 38·7 | 34·7, 42·8 | 32·7 | 21·1, 46·8 | 38·7 | 34·1, 43·6 | 45·1 | 35·1, 55·5 |
| Brown | 42·0 | 38·0, 46·1 | 32·7 | 26·7, 49·1 | 44·5 | 39·5, 49·6 | 39·1 | 19·3, 49·6 |
| Black | 19·2 | 15·1, 24·2 | 30·1 | 16·0, 49·3 | 16·7 | 13·3, 20·8 | 15·8 | 11·0, 22·2 |
| Educational attainment (%) | ||||||||
| 0–4 years | 18·5 | 15·5, 21·9 | 26·5 | 19·4, 35·0c | 19·2 | 15·4, 23·3c | 7·8 | 4·4, 13·4a,b |
| 5–8 years | 23·8 | 21·0, 27·1 | 28·7 | 23·0, 35·2 | 21·3 | 17·6, 25·5 | 26·9 | 22·4, 32·0 |
| 9–11 years | 45·2 | 39·7, 50·1 | 37·2 | 28·4, 47·0 | 48·0 | 40·3, 55·8 | 44·8 | 37·2, 52·7 |
| >12 years | 12·4 | 10·0, 15·4 | 7·5 | 5·2, 10·9c | 11·6 | 8·5, 15·8 | 20·4 | 14·7, 27·6a |
| Monthly income ≤3 minimum wages† (%) | 69·9 | 61·5, 68·2 | 70·3 | 62·6, 77·0c | 68·15 | 63·4, 72·5c | 48·4 | 40·8, 56·1a,b |
| Mean length of residence (years)‡ | 18·4 | 17·3, 19·6 | 17·1 | 14·5, 19·7 | 18·4 | 16·9, 19·9 | 20·0 | 18·1, 21·9 |
| Practise physical activity§ (%) | 35·0 | 30·9, 30·8 | 30·6 | 22·3, 40·2 | 33·5 | 28·0, 39·6 | 44·6 | 38·7, 50·8 |
| Self-rated health (%) | ||||||||
| Good/very good | 64·1 | 59·6, 68·3 | 52·1 | 39·5, 64·4 | 66·5 | 61·8, 70·8 | 69·3 | 63·0, 74·9 |
| Fair | 28·6 | 25·3, 32·2 | 31·9 | 25·7, 38·7 | 28·8 | 24·3, 33·7 | 24·5 | 18·3, 31·8 |
| Poor/very poor | 7·3 | 4·9, 10·9 | 16·0 | 8·4, 28·3b | 4·8 | 2·9, 7·6a | 6·2 | 3·4, 11·1 |
| Mean BMI (kg/m2)‖ | 27·1 | 26·7, 27·6 | 26·8 | 26·4, 27·2 | 26·9 | 26·3, 27·5 | 28·1 | 27·1, 29·2 |
| BMI > 25 kg/m2 (%) | 37·8 | 34·5, 41·2 | 37·8 | 30·4, 45·9 | 36·6 | 32·6, 40·8 | 41·81 | 34·6, 49·3 |
| BMI > 30 kg/m2 (%) | 20·1 | 17·1, 23·5 | 18·4 | 12·65, 25·9 | 19·9 | 15·9, 24·6 | 22·6 | 17·2, 29·2 |
| Low perceived food environment (%) | 16·7 | 13·2, 20·9 | 27·5 | 20·0, 36·7c | 15·5 | 11·3, 21·0 | 8·8 | 5·0, 14·9a |
Residential segregation was measured for study-defined neighbourhoods using the Getis–Ord local statistic. Categories of segregation were defined as follows: high,  ; medium,
; medium,  ; and low,
; and low,  . Low perceived food environments were considered when the answers to all questions about fruit and vegetable availability (variety, quality and price) were ‘no’. In order to identify any differences, the comparison of 95 % CI was used: ahigh-segregated neighbourhood; bmedium-segregated neighbourhood (integrated); clow-segregated neighbourhood. Values within a row with unlike superscript letters were statistically different.
. Low perceived food environments were considered when the answers to all questions about fruit and vegetable availability (variety, quality and price) were ‘no’. In order to identify any differences, the comparison of 95 % CI was used: ahigh-segregated neighbourhood; bmedium-segregated neighbourhood (integrated); clow-segregated neighbourhood. Values within a row with unlike superscript letters were statistically different.
Data includes twenty-three missing values.
Data includes thirty-two missing values.
Data includes ten missing values.
Data includes three missing values.
Data includes twelve missing values.
Individuals residing in a highly segregated neighbourhood were less educated and tended to be younger. They were also more likely to self-rate their health status as poor/very poor. Furthermore, perceptions of the food environment were worse (low food environment perception) in these high-segregated areas in comparison to low-segregated, 27·5 (95 % CI 20·0, 36·7) % v. 8·8 (95 % CI 5·0, 14·9) %. No differences in BMI, race/skin colour categories, practise of physical activities and length of residence were observed across segregation categories (Table 1).
As presented in Table 2, the distribution of healthy and unhealthy eating markers was influenced by the economic residential segregation.
Table 2.
Prevalence (95 % CI) of healthy and unhealthy eating markers among adults (≥18 years) by categories of economic residential segregation; MOVE-se Academias study, Belo Horizonte, Brazil, 2014–2015
| Economic residential segregation | ||||||||
|---|---|---|---|---|---|---|---|---|
| Overall sample | Higha | Mediumb | Lowc | |||||
| % | 95 % CI | % | 95 % CI | % | 95 % CI | % | 95 % CI | |
| Healthy eating markers, regular consumption of (%) | ||||||||
| Fruit | 36·7 | 33·2, 40·3 | 34·6 | 25·5, 44·9c | 32·4 | 28·4, 36·64c | 53·2 | 47·0, 59·2a,b |
| Vegetables | 72·9 | 69·6, 76·1 | 70·1 | 62·6, 76·7c | 69·5 | 65·2, 73·4c | 87·6 | 81·7, 91·7a,b |
| Beans | 83·1 | 79·2, 86·5 | 91·0 | 86·7, 93·9b | 79·5 | 73·7, 84·4a | 86·0 | 78·0, 90·4 |
| Fish | 28·5 | 25·7, 31·5 | 23·6 | 17·2, 31·3c | 29·9 | 22·5, 29·7c | 42·3 | 37·11, 47·6a,b |
| Unhealthy eating markers, regular consumption of (%) | ||||||||
| Meat or chicken with excess fat | 41·6 | 37·7, 45·7 | 43·2 | 36·1, 50·5 | 44·1 | 38·5, 49·8c | 31·9 | 26·1, 38·3b |
| Soft drinks or artificial juice | 31·8 | 28·2, 35·6 | 34·2 | 27·8, 41·3 | 32·0 | 26·8, 37·7 | 28·6 | 21·9, 36·2 |
| Sweet foods | 16·6 | 14·2, 19·4 | 16·4 | 11·4, 23·2 | 15·3 | 12·3, 18·9 | 21·3 | 16·3, 27·3 |
| Replacement of lunch or dinner with snacks | 2·4 | 1·5, 3·7 | 0·8 | 0·4, 1·5c | 2·2 | 1·3, 3·8 | 4·7 | 1·9, 10·8a |
Residential segregation was measured for study-defined neighbourhoods using the Getis–Ord local statistic. Categories of segregation were defined as follows: high, ; medium, ; and low, . Regular consumption defined as a consumption of any amount for five days or more per week, except for fish (one or more days per week) and replacement of lunch or dinner with snacks (seven days per week). In order to identify any differences, the comparison of 95 % CI was used: ahigh-segregated neighbourhood; bmedium-segregated neighbourhood (integrated); clow-segregated neighbourhood. Values within a row with unlike superscript letters were statistically different.
Overall, the regular consumption of fruits was reported by 36·7 (95 % CI 33·2, 40·3) % of participants, being lower among individuals residing in highly segregated areas (34·6 %; 95 % CI 25·5, 44·9 %). Likewise, regular consumption of vegetables was lower in high-segregated neighbourhoods compared with low-segregated neighbourhoods (70·1 %; 95 % CI 62·6, 76·7 % v. 87·6 %; 95 % CI 81·7, 91·7 %).
Similarly, the regular consumption of fish, reported to happen at least once per week, was lower among individuals residing in highly segregated areas (23·6 %; 95 % CI 17·2, 31·3 %). On the other hand, the regular consumption of beans was reported by 83·1 % (95 % CI 79·2, 86·5 %) of participants, being higher among individuals residing in highly segregated areas (91·0 %; 95 % CI 86·7, 93·9 %).
We verified that the regular replacement of lunch or dinner with snacks was significantly lower in highly segregated areas. The regular consumption of meat with excess fat was significantly higher among medium-segregation in comparison to low-segregation areas. There were no statistically significant differences comparing consumption of soft drinks, artificial juice and sweet foods among the segregation categories.
Multiple logistic regression results
In multiple logistic regression models using the generalized estimating equations (Tables 3 and 4), we found higher odds of regular consumption of beans (OR = 1·85; 95 % CI 1·07, 3·19) among those living in high-segregated compared with low-segregated neighbourhoods, after adjustment for individual-level factors and perceived food environment. By contrast, we found lower odds of regular consumption of vegetables (OR = 0·62; 95 % CI 0·39, 0·98).
Table 3.
Adjusted OR and 95 % CI for healthy eating markers prevalence in high and medium categories of economic residential segregation; MOVE-se Academias study, Belo Horizonte, Brazil, 2014–2015
| Regular consumption of fruit | Regular consumption of vegetables | Regular consumption of beans | Regular consumption of fish | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95 % CI | P value | OR | 95 % CI | P value | OR | 95 % CI | P value | OR | 95 % CI | P value | |
| Unadjusted | ||||||||||||
| High | 0·59 | 0·40, 0·88 | 0·009 | 0·43 | 0·26, 0·70 | 0·001 | 2·00 | 1·17, 3·41 | 0·011 | 0·58 | 0·39, 0·87 | 0·008 |
| Medium | 0·57 | 0·41, 0·81 | 0·002 | 0·48 | 0·30, 0·75 | 0·001 | 1·19 | 0·77, 1·83 | 0·428 | 0·57 | 0·41, 0·81 | 0·002 |
| Low | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | Ref. | – |
| Model 1 | ||||||||||||
| High | 0·68 | 0·45, 1·03 | 0·068 | 0·49 | 0·31, 0·79 | 0·004 | 2·02 | 1·18, 3·48 | 0·010 | 0·63 | 0·42, 0·94 | 0·025 |
| Medium | 0·62 | 0·43, 0·89 | 0·009 | 0·54 | 0·35, 0·84 | 0·006 | 1·23 | 0·79, 1·90 | 0·353 | 0·60 | 0·42, 0·85 | 0·005 |
| Low | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | v | 1·00 | Ref. | – | |
| Model 2 | ||||||||||||
| High | 0·84 | 0·55, 1·28 | 0·426 | 0·60 | 0·37, 0.96 | 0·034 | 1·84 | 1·07, 3·18 | 0·026 | 0·72 | 0·48, 1·10 | 0·136 |
| Medium | 0·70 | 0·49, 1·01 | 0·059 | 0·64 | 0·42, 0·98 | 0·040 | 1·23 | 0·79, 1·91 | 0·351 | 0·66 | 0·46, 0·94 | 0·024 |
| Low | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·0 | Ref. | – | 1·00 | Ref. | – |
| Model 3 | ||||||||||||
| High | 0·86 | 0·56, 1·32 | 0·492 | 0·61 | 0·39, 0·99 | 0·044 | 1·82 | 1·06, 3·12 | 0·030 | 0·74 | 0·49, 1·12 | 0·159 |
| Medium | 0·71 | 0·49, 1·03 | 0·075 | 0·63 | 0·42, 0·97 | 0·038 | 1·23 | 0·79, 1·90 | 0·353 | 0·65 | 0·46, 0·94 | 0·022 |
| Low | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | Ref. | – |
| Model 4 | ||||||||||||
| High | 0·84 | 0·55, 1·30 | 0·443 | 0·62 | 0·39, 0·98 | 0·043 | 1·85 | 1·07, 3·19 | 0·026 | 0·73 | 0·48, 1·10 | 0·141 |
| Medium | 0.71 | 0·49, 1·03 | 0·071 | 0·64 | 0·42, 0·97 | 0·038 | 1·23 | 0·79, 1·91 | 0·344 | 0·65 | 0·45, 0·94 | 0·020 |
| Low | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | Ref. | – |
Ref., reference category.
Logistic regression models using the generalized estimating equations method were used to estimate adjusted OR and 95 % CI. Residential segregation was included in models as a categorical variable with ‘low’ residential segregation as the reference category (high, ; medium: ; and low, ). Regular consumption defined as a consumption of any amount for five days or more per week, except for fish (one or more days per week). Low perceived food environments were considered when the answers to all questions about fruit and vegetable availability (variety, quality and price) were ‘no’.
Model 1: adjusted for age, gender and skin colour.
Model 2: Model 1 + family income and education.
Model 3: Model 2 + self-rated health and BMI (kg/m2).
Model 4: Model 3 + low perceived food environment.
Bold denotes statistical significance, P < 0·05.
Table 4.
Adjusted OR and 95 % CI for unhealthy eating markers prevalence in high and medium categories of economic residential segregation; MOVE-se Academias study, Belo Horizonte, Brazil, 2014–2015
| Consumption of meat or chicken with excess fat | Regular consumption of soft drinks or artificial juice | Regular consumption of sweet foods | Replacement of lunch or dinner with snacks | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95 % CI | P value | OR | 95 % CI | P value | OR | 95 % CI | P value | OR | 95 % CI | P value | |
| Unadjusted | ||||||||||||
| High | 1·66 | 1·10, 2·50 | 0·015 | 1·27 | 0·84, 1·92 | 0·242 | 1·01 | 0·66, 1·55 | 0·941 | 0·60 | 0·19, 1·83 | 0·370 |
| Medium | 1·60 | 1·11, 2·30 | 0·011 | 0·98 | 0·68, 1·43 | 0·955 | 0·79 | 0·53, 116 | 0·228 | 0·93 | 0·37, 2·30 | 0·884 |
| Low | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | Ref. | – |
| Model 1 | ||||||||||||
| High | 1·48 | 1·00, 2·19 | 0·051 | 1·05 | 0·69, 1·59 | 0·815 | 0·90 | 0·57, 1·41 | 0·643 | 0·50 | 0·14, 1·72 | 0·274 |
| Medium | 1·55 | 1·09, 2·20 | 0·014 | 0·91 | 0·62, 1·31 | 0·605 | 0·75 | 0·49, 1·12 | 0·161 | 0·98 | 0·37, 2·61 | 0·891 |
| Low | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | ||
| Model 2 | ||||||||||||
| High | 1·36 | 0·91, 2·03 | 0·129 | 0·96 | 0·63, 1·46 | 0·839 | 1·00 | 0·62, 1·63 | 0·969 | 0·63 | 0·18, 2·17 | 0·468 |
| Medium | 1·47 | 1·03, 2·09 | 0·033 | 0·83 | 0·57, 1·20 | 0·324 | 0·83 | 0·54, 1·28 | 0·405 | 1·11 | 0·42, 2·94 | 0·828 |
| Low | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | Ref. | – |
| Model 3 | ||||||||||||
| High | 1·35 | 0·91, 2·01 | 0·129 | 0·95 | 0·62, 1·45 | 0·832 | 1·01 | 0·62, 1·64 | 0·960 | 0·62 | 0·18, 2·13 | 0·449 |
| Medium | 1·47 | 1·03, 2·09 | 0·031 | 0·82 | 0·56, 1·19 | 0·300 | 0·82 | 0·53, 1·28 | 0·319 | 1·16 | 0·43, 3·08 | 0·764 |
| Low | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | Ref. | – |
| Model 4 | ||||||||||||
| High | 1·35 | 0·92, 2·00 | 0·121 | 0·95 | 0·62, 1·45 | 0·814 | 0·98 | 0·60, 1·60 | 0·954 | 0·62 | 0·18, 2·12 | 0·443 |
| Medium | 1·46 | 1·04, 2·06 | 0·031 | 0·82 | 0·56, 1·19 | 0·297 | 0·82 | 0·54, 1·27 | 0·382 | 1·15 | 0·45, 3·07 | 0·769 |
| Low | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | Ref. | – | 1·00 | Ref. | – |
Ref., reference category.
Logistic regression models using the generalized estimating equations method were used to estimate adjusted OR and 95 % CI. Residential segregation was included in models as a categorical variable with ‘low’ residential segregation as the reference category (high, ; medium, ; and low, ). Regular consumption defined as a consumption of any amount for five days or more per week, except for replacement of lunch or dinner with snacks (seven days per week). Low perceived food environments were considered when the answers to all questions about fruit and vegetable availability (variety, quality and price) were ‘no’.
Model 1: adjusted for age, gender and skin colour.
Model 2: Model 1 + family income and education.
Model 3: Model 2 + self-rated health and BMI (kg/m2).
Model 4: Model 3 + low perceived food environment.
Bold denotes statistical significance, P < 0·05.
Although high segregation was not associated with regular consumption of fruits, fish, or consumption of meat or chicken with excess fat, we found differences between medium-segregation and low-segregation areas after adjustment. We found lower odds of regular consumption of fish (OR = 0·65; 95 % CI 0·45, 0·94) in medium-segregated neighbourhoods compared with low-segregated neighbourhoods, after adjustments. In contrast, we observed high odds of regular consumption of meat or chicken with excess fat (OR = 1·46; 95 % CI 1·04, 2·06) in medium-segregation areas in comparison to more affluent neighbourhoods.
Discussion
Belo Horizonte seems to be an urban divided space, in which ‘invisible’ barriers limit equitable occupation of the city and probably contribute to either healthy or unhealthy food consumption of the people living in high-segregated neighbourhoods.
Economically segregated urban neighbourhoods
The city of Belo Horizonte was planned, built and founded to be a symbol of modernity; however, it has experienced an urban planning that probably made the socio-spatial segregation real.
Segregation apparently divides Belo Horizonte. Highly segregated neighbourhoods correspond to one of the most vulnerable areas of the city. On the other hand, low-segregated neighbourhoods are located predominantly in the south-central areas, one of the wealthier regions. The south-central area has the highest income per capita (R$ 3915·00) and Municipal Human Development Index (0·910) of the city. The per capita income in Belo Horizonte, in the same year, was R$ 1497·29 and the Municipal Human Development Index was 0·810(39).
Disparities in food consumption
The high economic residential segregation was independently associated with higher prevalence of regular consumption of beans and a lower prevalence of regular consumption of vegetables, after adjustments for individual-level characteristics and perceived food environment.
Eating behaviour of individuals may be influenced by existing norms and values around them and this could be correlated to access to, availability and price of these foods, which, in turn, can also modulate residents’ eating behaviour or shape their food preferences(40–44).
Associations of segregation and diet were neither consistent nor significant. Research conducted in the USA described that neighbourhood-level racial/ethnic segregation and components of a healthy diet were not independently associated after adjustments(17). However, more recent findings showed racial/ethnic segregation has a negative effect on fruit and vegetable expenditure and consumption(16,18). Furthermore, regarding the availability of healthy foods, some prior research denotes a double risk in segregated areas, with an average of 30 % fewer supermarkets and more fast-food restaurants, convenience retails and other smaller stores offering an abundance of high-energy and low-nutrient foods(9,45). In addition, racial/ethnically segregated neighbourhoods had less availability of fresh fruit and less promotion of unhealthy impulse buys relative to stores in more affluent areas(46).
The high prevalence of beans consumption in the high-segregated neighbourhoods indicated that segregation may not just be a negative phenomenon. Beans are a significant component of the traditional Brazilian diet. They are considered to be a healthy food and are among the most consumed items in the country(20,47). Regular consumption of beans can be associated not only with price, high satiation/satiety capacity of this food or a concrete way to survive starvation, but also with tradition, culture and preservation of cooking habits. Segregation is a relational phenomenon involving development and sustainability of culture and identity(2,26). Thus, consumption of beans in such neighbourhoods may reveal how preservation of some aspects of food culture can differently affect social groups.
Regarding vegetable consumption, it has been well documented that racial/ethnic segregation and socio-economic disadvantage affect the quantity and quality of fresh food stores(13,16). An ecological study undertaken in Belo Horizonte revealed that the neighbourhood of a HAP had low quality of stores with limited access to healthy foods(48). Besides, previous findings in Belo Horizonte and São Paulo showed that living in neighbourhoods with stores/markets selling fresh foods was associated with fruit and vegetable consumption(13,40).
Differently from the results found for regular consumption of vegetables, the prevalence of regular consumption of fruits did not differ between high-segregated neighbourhoods, after adjustments. Like vegetables, fruits are fresh foods that are usually sold in the same section of the stores, but access to them can be different as demonstrated in a Brazilian study that audited 336 commercial establishments in Belo Horizonte. Auditing in 1600 m buffer zones of eighteen HAP sites (2013–2014), the authors reported that the quality of fruits was better and their availability was higher, compared with vegetables(49). Thus, it is important to understand other variables that can be associated with segregation, including characteristics of consumers’ eating environment and monotonous consumption of fruits among the areas studied. It is possible that residents of high-segregated neighbourhoods consume a smaller variety of fruits compared with the more affluent ones.
Differences between medium-segregation and low-segregation neighbourhoods were observed; however, caution is needed when drawing generalities, since the low-segregated category corresponds to integrated areas (no segregated) or areas in which the group of heads of household earning a monthly income of 0–3 minimum wages is significantly under-represented (low-segregated areas). We may need to evaluate availability of food, other variables representing the community and the consumer nutrition environment in these areas to understand their differences and how the association between segregation and dietary behaviours is mediated by the objective food environment.
Strengths and limitations
These findings may be influenced by some limitations, as follows. First, the design of the Move-se Academias study includes units of a health promotion programme located predominantly in vulnerable areas of the city. Thus, the proportion of heads of household earning a monthly income greater than three minimum wages in these areas was very small. As a result, the low-segregation group corresponds to the absence of any clustering or areas in which the group of heads of household earning 0–3 minimum wages is significantly under-represented. Nevertheless, with the sample of the present study, we were able to reproduce approximately 18 % of high segregation evidenced in the larger area studied. Furthermore, we can speculate that there is a possible influence of HAP and their distinct periods of existence on the eating practices of the study participants. However, we cannot determine the influence of the programme’s existence on eating practices of non-users because there is insufficient evidence in the literature. Second, possible measurement biases exist, as expected from the usual dietary risk factor information related to the interviewee’s memory failure. Third, the census tracts might not correspond to socially defined neighbourhoods. However, there are different approaches to define a geographic context; several studies have used census tracts to define neighbourhood boundaries and associated them with health outcomes(50,51).
Despite this, the present study has many strengths. To our knowledge, there is no study in the literature assessing the relationship of food consumption with economic residential segregation in Brazil. There are several consistent and significant studies examining the disparities in availability of fresh fruits, vegetables, low-fat milk and high-fibre foods among segregated urban neighbourhoods(8,10). But this is the first research conducted in Brazil aiming to describe food consumption using the statistic, a novel spatial approach to measure segregation. In addition, the present study uses an urban population sample from a large Brazilian city and 2010 Brazil Census data to understand the relationship between segregation territories and food consumption.
Conclusions
The present study provides empirical evidence that segregation is an important determinant of diet in low-medium-income countries, confirms the different profiles of food consumption in segregated areas and contributes to a growing body of research seeking to understand how segregation is associated with health and diet.
Our results suggest living in a high-segregation neighbourhood was associated with healthy food consumption in two different ways: (i) negatively, as shown by the lowest regular consumption of fresh foods; and (ii) positively, favouring the consumption of minimally processed foods, preserving traditions and culture. A better understanding of residential segregation in Brazil could potentially inform policies and/or programming by reflecting the unequal distribution of deprivation and privilege, especially at a time when progress in reducing inequality is under threat.
Segregation is a symptom of the structures of governance, work and iniquities, and Brazil is at a challenging moment. Our social welfare net, that until recently has been supporting innumerable achievements in the food and nutrition agenda (including reducing hunger and poverty, promoting food and nutrition security in the country), as well as the different assistance actions (by securing the rights and protection of vulnerable populations) are weakening. The establishment of spending cuts in education and health, associated with revisions to labour and pension laws, probably will impact the population’s income and intensify social inequalities(52–54), consequently deepening the residential segregation and its negative repercussions on the health of Brazilians.
Furthermore, considering different access to food in this area, a better understanding of neighbourhood characteristics and food environment aspects could clarify the links among eating behaviours, socio-economic disadvantages and segregation.
Acknowledgements
Financial support: This work was supported by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq; grant number 552752/2011-8 and Research Productivity Scholarships to A.A.L.F., D.C.M. and W.T.C.) and the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES; Finance Code 001). CNPq and CAPES had no role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: Authors contributed as follows. M.S.L.: analysis and interpretation of data; statistical analysis; drafting of manuscript; reviewed the final version of this manuscript and approved its publication. W.T.C.: conception and design; critical revision of manuscript; obtaining funding; administrative, technical and material support; reviewed the final version of this manuscript and approved its publication. A.C.S.A.: analysis and interpretation of data; statistical analysis; reviewed the final version of this manuscript and approved its publication. D.C.M.: conception and design; critical revision of manuscript; obtaining funding; administrative, technical and material support; reviewed the final version of this manuscript and approved its publication. S.B.: critical revision of manuscript; technical support; reviewed the final version of this manuscript and approved its publication. A.A.L.F.: conception and design; critical revision of manuscript; obtaining funding; administrative, technical and material support; reviewed the final version of this manuscript and approved its publication. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Research Ethics Committee of the Medical School, Universidade Federal de Minas Gerais (640.920 of 8 May 2014). Written informed consent was obtained from all subjects.
References
- 1.Massey DS & Denton N (1988) The dimensions of residential segregation. Soc Forces 67, 281–315. [Google Scholar]
- 2.Williams DR & Collins C (2001) Racial residential segregation: a fundamental cause of racial disparities in health. Public Health Rep 116, 404–416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Goodman M, Lyons S, Dean LT et al. (2018) How segregation makes us fat: food behaviors and food environment as mediators of the relationship between residential segregation and individual body mass index. Front Public Health 6, 92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Usher T, Gaskin JD, Bower K et al. (2018) Residential segregation and hypertension prevalence in black and white older adults. J Appl Gerontol 37, 177–202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Krieger N, Feldman JM, Waterman PD et al. (2017) Local residential segregation matters: stronger association of census tract compared to conventional city-level measures with fatal and non-fatal assaults (total and firearm related), using the index of concentration at the extremes (ICE) for racial, economic, and racialized economic segregation, Massachusetts (US), 1995–2010. J Urban Health 94, 244–258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Landrine H, Corral I, Lee JGL et al. (2017) Residential segregation and racial cancer disparities: a systematic review. J Racial Ethn Health Disparities 4, 1195–1205. [DOI] [PubMed] [Google Scholar]
- 7.Kershaw KN, Osypuk TL, Do DP et al. (2015) Neighborhood-level racial/ethnic residential segregation and incident cardiovascular disease: the Multi-Ethnic Study of Atherosclerosis. Circulation 131, 141–148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ball K, Timperio A & Crawford D (2009) Neighbourhood socioeconomic inequalities in food access and affordability. Health Place 15, 578–585. [DOI] [PubMed] [Google Scholar]
- 9.Bower KM, Thorpe RJ Jr, Rohde C et al. (2014) The intersection of neighborhood racial segregation, poverty, and urbanicity and its impact on food store availability in the United States. Prev Med 58, 33–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Morland K & Filomena S (2007) Disparities in the availability of fruits and vegetables between racially segregated urban neighbourhoods. Public Health Nutr 10, 1481–1489. [DOI] [PubMed] [Google Scholar]
- 11.Zenk SN, Schulz AJ, Israel BA et al. (2005) Neighborhood racial composition, neighborhood poverty, and the spatial accessibility of supermarkets in metropolitan Detroit. Am J Public Health 95, 41–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lopes ACS, Menezes MC & Araújo ML (2017) O ambiente alimentar e o acesso a frutas e hortaliças: ‘uma metrópole em perspectiva’. Saude Soc 26, 764–773. [Google Scholar]
- 13.Duran AC, Roux AVD, Latorre MDRDO et al. (2013) Neighborhood socioeconomic characteristics and differences in the availability of healthy food stores and restaurants in Sao Paulo, Brazil. Health Place 23, 39–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Park Y, Neckerman K, Quinn J et al. (2011) Neighbourhood immigrant acculturation and diet among Hispanic female residents of New York City. Public Health Nutr 14, 1593–1600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Osypuk TL, Diez Roux AV, Hadley C et al. (2009) Are immigrant enclaves healthy places to live? The Multi-Ethnic Study of Atherosclerosis. Soc Sci Med 69, 110–120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ryabov I (2016) Examining the role of residential segregation in explaining racial/ethnic gaps in spending on fruit and vegetables. Appetite 98, 74–79. [DOI] [PubMed] [Google Scholar]
- 17.Yi SS, Ruff RR, Jung M et al. (2014) Racial/ethnic residential segregation, neighborhood poverty and urinary biomarkers of diet in New York City adults. Soc Sci Med 122, 122–129. [DOI] [PubMed] [Google Scholar]
- 18.Corral I, Landrine H, Hao Y et al. (2012) Residential segregation, health behavior and overweight/obesity among a national sample of African American adults. J Health Psychol 17, 371–378. [DOI] [PubMed] [Google Scholar]
- 19.Barber S, Diez-Roux AV, Cardoso L et al. (2018) At the intersection of place, race, and health in Brazil: residential segregation and cardio-metabolic risk factors in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Soc Sci Med 199, 67–76. [DOI] [PubMed] [Google Scholar]
- 20.Jaime PC, Stopa SR, Oliveira TP et al. (2015) Prevalência e distribuição sociodemográfica de marcadores de alimentação saudável, Pesquisa Nacional de Saúde, Brasil 2013. Epidemiol Serv Saude 24, 267–276. [Google Scholar]
- 21.Malta DC Iser BPM, Santos MAS et al. (2015) Estilos de vida nas capitais brasileiras segundo a Pesquisa Nacional de Saúde e o Sistema de Vigilância de Fatores de Risco e Proteção para Doenças Crônicas Não Transmissíveis por Inquérito Telefônico (Vigitel), 2013. Rev Bras Epidemiol 18, 68–82. [Google Scholar]
- 22.Fernandes AP, Andrade ACS, Costa DAS et al. (2017) Programa Academias da Saúde e a promoção da atividade física na cidade: a experiência de Belo Horizonte, MG, Brasil. Cienc Saude Colet 22, 3903–3914. [DOI] [PubMed] [Google Scholar]
- 23.Prefeitura Belo Horizonte (2019) Academia da Cidade. http://portalpbh.pbh.gov.br/ (accessed December 2019).
- 24.Caiaffa W & Friche AAL (2019) Observatory for Urban Health in Belo Horizonte City: an innovative and cross-sectoral collaboration in urban health. In Urban Health [Galea S, Ettman CK and Vlahov D, editors]. Oxford: Oxford University Press; doi: 10.1093/oso/9780190915858.003.0037. [DOI] [Google Scholar]
- 25.Instituto Brasileiro de Geografia e Estatística (2011) Base de Informações do Censo Demográfico 2010: Resultados do Universo por Setor Censitário. Rio de Janeiro, RJ: IBGE. [Google Scholar]
- 26.Torres HG (2006) Residential segregation and public policies: São Paulo in the 1990’s. Rev Bras Cienc Soc 19, 41–55. [Google Scholar]
- 27.Instituto Brasileiro de Geografia e Estatística, Coordenação de Trabalho e Rendimento (2016) Pesquisa Nacional por Amostra de Domicílios: Síntese de Indicadores. Rio de Janeiro, RJ: IBGE.
- 28.Getis A & Ord JK (1992) The analysis of spatial association by use of distance statistics. Geogr Anal 24, 189–206. [Google Scholar]
- 29.Getis A & Ord JK (1995) Local spatial autocorrelation statistics: distributional issues and an application. Geogr Anal 27, 286–306. [Google Scholar]
- 30.Ministério da Saúde, Secretaria de Vigilância em Saúde, Secretaria de Gestão Estratégica e Participativa (2017) Vigitel Brasil 2016: Vigilância de Fatores de Risco e Proteção para Doenças Crônicas por Inquérito Telefônico. Brasília, DF: Ministério da Saúde. [Google Scholar]
- 31.Ministry of Health of Brazil, Secretariat of Health Care, Primary Health Care Department (2015) Dietary Guidelines for the Brazilian Population. Brasília, DF: Ministry of Health of Brazil. [Google Scholar]
- 32.Brasil (2015) Pesquisa Nacional de Saúde (PNS) 2013. http://www.pns.icict.fiocruz.br/ (accessed June 2018).
- 33.Mendes LL, Campos SF, Malta DC et al. (2011) Validade e reprodutibilidade de marcadores do consumo de alimentos e bebidas de um inquérito telefônico realizado na cidade de Belo Horizonte (MG), Brasil. Rev Bras Epidemiol 14, 80–89.22002145 [Google Scholar]
- 34.Monteiro CA, Moura EC, Jaime PC et al. (2008) Validade de indicadores do consumo de alimentos e bebidas obtidos por inquérito telefônico. Rev Saude Publica 42, 582–589. [DOI] [PubMed] [Google Scholar]
- 35.Neves ACMD, Gonzaga LAA, Martens IBG et al. (2008) Validação de indicadores do consumo de alimentos e bebidas obtidos por inquérito telefônico em Belém, Pará, Brasil. Cad Saude Publica 26, 2379–2388. [DOI] [PubMed] [Google Scholar]
- 36.World Health Organization (2000) Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation. WHO Technical Report Series no. 894. Geneva: WHO. [PubMed]
- 37.Santos SM, Griep RH, Cardoso LO et al. (2013) Cross-cultural adaptation and reliability of measurements on self-reported neighborhood characteristics in ELSA-Brasil. Rev Saude Publica 47, Suppl. 2, 122–130. [DOI] [PubMed] [Google Scholar]
- 38.Hanley JA, Negassa A, Edwardes MDB et al. (2003) Statistical analysis of correlated data using generalized estimating equations: an orientation. Am J Epidemiol 4, 364–375. [DOI] [PubMed] [Google Scholar]
- 39.Programa Das Nações Unidas Para o Desenvolvimento, Instituto De Pesquisa Econômica e Aplicada & Fundação João Pinheiro (2013) Atlas de desenvolvimento humano do Brasil de 2013. http://www.atlasbrasil.org.br/2013 (accessed May 2019).
- 40.Menezes M, Diez Roux A, Costa B et al. (2018) Individual and food environmental factors: association with diet. Public Health Nutr 21, 2782–2792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Menezes MC, Roux AVD, Lopes ACS et al. (2018) Fruit and vegetable intake: influence of perceived environment and self-eficacy. Appetite 127, 249–256. [DOI] [PubMed] [Google Scholar]
- 42.Auchincloss AH, Riolo RL, Brown DG et al. (2011) An agent-based model of income inequalities in diet in the context of residential segregation. Am J Prev Med 40, 303–311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Pessoa MC, Mendes LL, Caiaffa WT et al. (2014) Availability of food stores and consumption of fruit, legumes and vegetables in a Brazilian urban area. Nutr Hosp 31, 438–443. [DOI] [PubMed] [Google Scholar]
- 44.Story M, Kaphingst KM, Robinson-O’Brien R et al. (2008) Creating healthy food and eating environments: policy and environmental approaches. Annu Rev Public Health 29, 253–272. [DOI] [PubMed] [Google Scholar]
- 45.Walker RE, Keane CR & Burke JG (2010) Disparities and access to healthy food in the United States: a review of food deserts literature. Health Place 16, 876–884. [DOI] [PubMed] [Google Scholar]
- 46.Winkler MR, Lenk KM, Caspi CE et al. (2019) Variation in the food environment of small and non-traditional stores across racial segregation and corporate status. Public Health Nutr 22, 1624–1634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Souza AM, Pereira RA, Yokoo EM et al. (2013) Alimentos mais consumidos no Brasil: Inquérito Nacional de Alimentação 2008–2009. Rev Saude Publica 47, 190–199. [Google Scholar]
- 48.Costa BVL, Oliveira CL & Lopes ACS (2015) Food environment of fruits and vegetables in the territory of the Health Academy Program. Cad Saude Publica 31, 159–169. [DOI] [PubMed] [Google Scholar]
- 49.Menezes MC, Costa BVL, Oliveira CDL et al. (2017) Local food environment and fruit and vegetable consumption: an ecological study. Prev Med Rep 5, 13–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Almeida FC, Friche AAL, Jennings MZ et al. (2018) Contextual characteristics associated with the perceived neighbourhood scale in a cross-sectional study in a large urban centre in Brazil. BMJ Open 8, e021445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Arcaya M, Tucker-Seeley R, Kim R et al. (2016) Research on neighborhood effects on health in the United States: a systematic review of study characteristics. Soc Sci Med 168, 16–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Vasconcelos FAG, Machado ML, Medeiros MAT et al. (2019) Public policies of food and nutrition in Brazil: from Lula to Temer. Rev Nutr 32, e180161. [Google Scholar]
- 53.Jaime PC, Delmuè DCC, Campello T et al. (2018) Um olhar sobre a agenda de alimentação e nutrição nos trinta anos do Sistema Único de Saúde. Cienc Saude Colet 23, 1829–1836. [DOI] [PubMed] [Google Scholar]
- 54.Paiva AB, Mesquita ACS, Jaccoud L et al. (2016) O Novo Regime Fiscal e Suas Implicações para a Política de Assistência Social no Brasil. Nota Técnica nº 27. Brasília, DF: IPEA. [Google Scholar]