

Abstract
Objective:
To estimate the current evidence regarding the association between gestational acrylamide (AA) exposure and offspring’s growth.
Design:
Systematic review and meta-analysis.
Setting:
A systematic literature search for relevant publications was conducted using PubMed, Medline, Embase, Web of Science databases from inception to 26 April 2019. The standardised mean difference (SMD) or OR with 95 % CI was selected as the effect sizes and was calculated using a random effects model.
Results:
Five cohort studies including 54 728 participants were identified. Offspring’s birth weight was significantly lower in high AA exposure group than in low AA exposure group (SMD –0·05, 95 % CI –0·09, –0·02, P = 0·005). There was also an association between maternal AA exposure and small for gestational age (OR 1·14, 95 % CI 1·06, 1·23, P < 0·001). In addition, pooled ORs suggested that children had a high risk of developing overweight/obesity in the future in maternal high AA exposure group (OR 1·14, 95 % CI 1·08, 1·21, P < 0·001 at age 3; OR 1·13, 95 % CI 1·07, 1·19, P < 0·001 at age 5; OR 1·09, 95 % CI 1·02, 1·16, P = 0·020 at age 8).
Conclusions:
These findings have important implications for conducting health education, providing guidance on maternal diet and developing an appropriate dietary strategy for pregnant women to reduce dietary AA exposure.
Keywords: Acrylamide, Gestational, Offspring, Growth
Acrylamide (AA), a known neurotoxicant and possible carcinogen (group 2A) to humans(1), can be formed in foodstuffs rich in carbohydrates during heating at high temperatures(2). Diet has become the main source of AA exposure for general populations(3). According to a report by European Food Safety Authority, AA was found highest in fried potato products and coffee and the average AA exposure to human was approximately 0·4–1·9 µg/kg body weight/d(4). Therefore, AA exposure from food and its influence on health outcomes have aroused worldwide concerns.
Recent studies revealed that AA could exert reproductive and developmental toxicity effects(5) as well as immunotoxicity effects(6). AA has been found to transfer via blood through the placenta to the fetus(7), and evidences(8–11) showed that maternal exposure to AA during pregnancy was associated with offspring’s birth weight and head circumference and might also increase the risk of small for gestational age (SGA). However, Nagata et al. (12) did not find the association between prenatal AA exposure and offspring’s birth size.
As we know, birth weight directly affects growth and development in childhood and health-related outcomes in adulthood. A recent meta-analysis of 7 646 267 participants proved a significant association between birth weight and type 2 diabetes mellitus, CVD and hypertension in adults(13). Another systematic review and meta-analysis of 393 471 participants revealed that an increasing birth weight could reduce 6 % risk of all-cause adult mortality(14). As maternal diet plays an important role in fetal growth and development(15), and there is lacking of reliable evidence proving the association between gestational AA exposure and the above outcomes, it is necessary and timely to conduct a meta-analysis on this topic.
The objective of the meta-analysis is to systematically evaluate all the relevant published literatures on whether gestational exposure to AA is associated with offspring’s growth. To our knowledge, this is the first meta-analysis on the topic. Findings of the present study will be important for conducting health education, providing guidance on maternal diet and developing an appropriate dietary strategy for pregnant women to reduce dietary AA exposure.
Materials and methods
Search strategy
We conducted this systematic review and meta-analysis according to Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines(16). A protocol of search strategies was prepared in accordance with the PICOS principle(17), and we defined it as follows: P(population): pregnant women and their offspring; I(intervention/exposure): different levels of gestational AA exposure; C(comparison): lowest level of AA exposure; O(outcome): offspring’s growth; S(study design): no restriction.
We searched PubMed, Medline, Embase, Web of Science from inception to 26 April 2019, with the following keywords: ‘acrylamide’/‘glycidamide’ and ‘pregnancy outcome’/‘birth size’/‘birth weight’/‘birth length’/‘head circumference’. In addition to the databases search, we screened the list of references in the previous reviews and selected papers and conducted manual searches to identify additional relevant studies.
Study selection
Studies that met the following criteria were included in the meta-analysis: (1) Original articles with full text; (2) Maternal AA exposure during pregnancy; (3) Reported at least one outcome, such as birth weight, birth length or head circumference. Studies were excluded if: (1) Review articles, conference abstracts or case reports; (2) Without prenatal AA exposure data; (3) Without sufficient details to calculate the effect sizes such as standardised mean difference (SMD) and OR. All retrieved articles were independently screened by two authors (Y.L.Z. and Y.X.) according to the above selection criteria, and discrepancies on whether to include a study were resolved by discussion.
Data extraction
Two authors (Y.L.Z. and Y.X.) independently retrieved from each of the articles’ data by using a data extracting sheet. When data were reported from overlapping study samples, the most recent and comprehensive reports were considered. Disagreements on data extraction were resolved through consensus and, if needed, by consulting a third author (Y.J.). Data in all eligible studies were extracted as follows:
Study information: first author, publication year, country, study design, total sample size, study duration.
Maternal characteristics: maternal age, nulliparous or multiparous, gestational weight gain, gestational age, smoking or not.
AA exposure data: AA measured method, average exposure level of AA, partition of AA exposure level, which foods high in AA.
Outcomes: birth weight, head circumference, SGA, overweight/obesity.
Quality assessment
Two authors (Y.X. and S.Y.Z.) independently assessed the risk of bias and graded the quality of all the included studies. Newcastle–Ottawa Scale (NOS) was used to assess the quality of all the included cohort studies(18), and study quality was classified into the following three categories: high, seven or more items of NOS criterion fulfilled; medium, 4–6 items of NOS criterion fulfilled; low, three or less items of NOS criterion fulfilled.
Statistical analysis
The SMD with its 95 % CI was used to analyse the difference of birth weight and head circumference between high AA exposure group and low exposure group. The OR with its 95 % CI was used to evaluate the risk of SGA and overweight/obesity in the high AA exposure group compared with the low AA exposure group. All the effect sizes were calculated using a random effects model. SMD was considered statistically significant at the P < 0·05 level with its 95 % CI not including the value 0, while OR at the P < 0·05 level with its 95 % CI not including the value 1.
Inter-study heterogeneity was assessed by a Q statistic with significance set at the P < 0·10 level instead of the level of 0·05 because of the low test power. We also applied the I 2 statistic to quantify the percentage of variation across studies attributable to heterogeneity, and the inter-study heterogeneity was categorised as low (<25 %), moderate (25–75 %) and high (>75 %)(19).
Subgroup analyses of the primary outcomes were performed according to smoking or not, continent, AA measured method, partition of AA exposure level and study quality. In addition, to examine the robustness of the results, we collected data for which confounders have been adjusted and conducted the sensitivity analyses. Another sensitivity analysis to evaluate whether any study dominated the results of the meta-analysis when the pooled result was significantly heterogeneous was also conducted. Finally, we constructed a funnel plot and Egger’s test(20) to assess the possibility of publication bias for the pooled outcomes of birth weight with significance at P < 0·05. All the statistical analyses were conducted through Review Manager 5.3 (Cochrane Collaboration) and STATA 12.0 (Stata Corporation).
Results
Study selection
The steps of our systematical search are shown in Fig. 1. A total of 1028 articles were identified, and after removal of duplicates (n 474), 554 articles remained. After title and abstract screening and full-text review, five full-text studies(8–12) met the inclusion criteria and were remained for the present meta-analysis.
Fig. 1.

Flow diagram of the included studies (1028 publications from PubMed, Embase, Medline, Web of Science were identified using the predefined search strategy, and after duplication checking, title and abstract screening and full-text review, five studies fulfilled the predefined inclusion criteria and were included in the final analysis.)
Characteristics of included studies
The included studies are summarised in Table 1. All of the five studies were cohort studies and were published between 2012 and 2018. Three studies reached high quality according to NOS criterion. Four studies were conducted in Europe. Most studies reported that FFQ was the measured method of AA exposure, and the main sources of exposure to AA were fried potatoes and crispbread. All the included studies looked for offspring’s growth outcomes resulting from maternal AA exposure during pregnancy.
Table 1.
Characteristics of included studies in the meta-analysis
| Study | Country | Study duration (years) | Sample size (n) | Maternal age (year) | Nulliparous (%) | GWG (kg) | Gestational age (week) | Smoker (%) | Acrylamide exposure | Quality | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Measured | Partition | Average level | Sources | ||||||||||||||
| Duarte-Salles et al.(8) | Norway | 9 | 50 651 | 30·1 | 4·5 | 52·0 | 14·9 | 6·2 | 39·5 | 1·7 | 8·3 | FFQ | Quartiles | 27·1 (µg/d) | 13·4 | Potato chips, nuts, popcorn, fried potatoes, crisp bread | High |
| Kadawathagedara et al.(9) | Norway | 9 | 51 952 | 30·3 | 4·4 | 46·3 | 14·8 | 5·8 | 40·0 | 1·6 | 6·8 | FFQ | Quartiles | 24·7 (μg/d) | 18·4–33·2 | Pancakes, sweet bakery products, bread, crispbread | High |
| Kadawathagedara et al. (10) | France | 3 | 1471 | 29·5 | 4·80 | 44·3 | 9·1 | 5·0 | 39·5 | 1·2 | 26·9 | FFQ | Quartiles | 23·8 (μg/d) | 17·3 | Fried potatoes (French fries, pan-fried and crisps) | Medium |
| Nagata et al.(12) | Japan | 1·5 | 204 | 28·9 | 4·2 | 44·6 | 9·6 | 3·0 | 39·5 | 1·0 | 4·0 | FFQ | Tertiles | 0·34 (lg/kg per bw) | 0·17 | Potato chips, coffee, meat and vegetables and their products | Medium |
| Pedersen et al.(11) | Multi-center | 4 | 1101 | 30·9 | 5·2 | 35·2 | – | – | 1·6 | HbAA | Quartiles | 19·7 (pmol/g Hb) | 16·5 | – | High | ||
HbAA, Hb adducts of acrylamide; bw, body weight.
Primary outcomes: acrylamide and birth size
Five studies(8–12) (two studies(8,9) had overlapping study samples) reported the relationship between prenatal AA exposure and birth weight. The pooled SMD suggested that offspring’s birth weight was significantly lower in high AA exposure group (SMD –0·05, 95 % CI –0·09, –0·02, P = 0·005) (Fig. 2). The pooled OR of three studies(8,10,11) also revealed an association between maternal AA exposure and SGA (OR 1·14, 95 % CI 1·06, 1·23, P < 0·001) (Fig. 3). However, the pooled SMD of head circumference from two studies(11,12) showed no statistically significant difference between high and low AA exposure groups (SMD 0·05, 95 % CI –0·17, 0·27, P = 0·640) (Fig. 4).
Fig. 2.
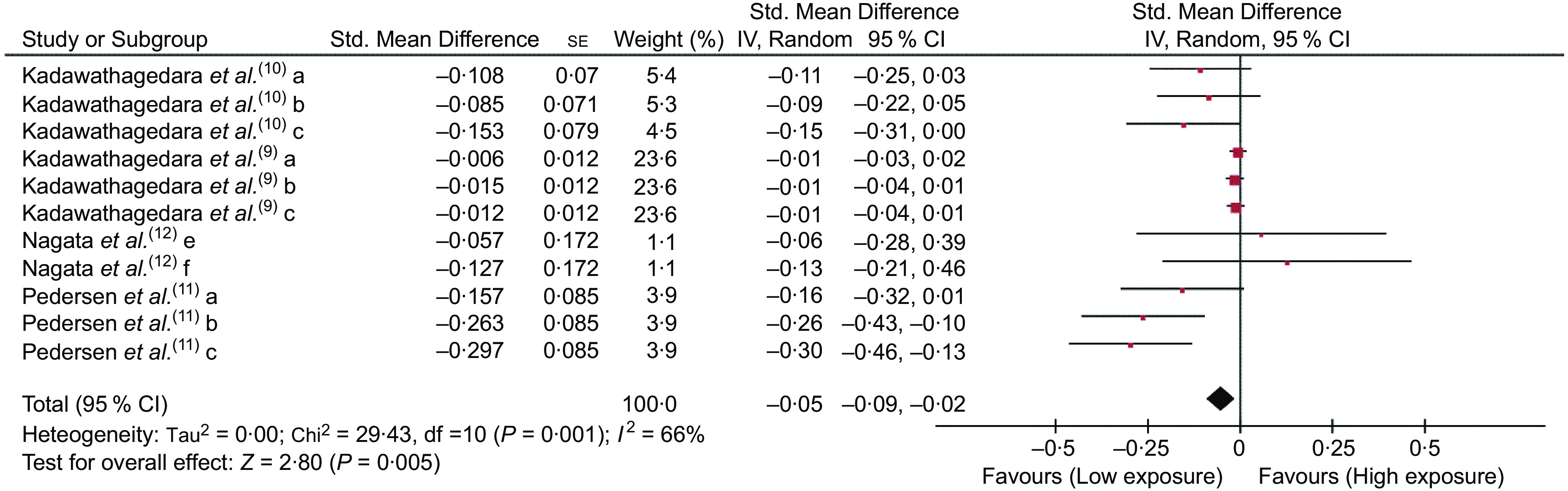
Forest plot of the pooled standardised mean difference of offspring’s birth weight between the high and low acrylamide exposure groups (The pooled standardised mean difference suggested that offspring’s birth weight was significantly lower in high acrylamide exposure group. a: quantile 2 v. quantile 1; b: quantile 3 v. quantile 1; c: quantile 4 v. quantile 1; e: tertile 2 v. tertile 1; f: tertile 3 v. tertile 1)
Fig. 3.
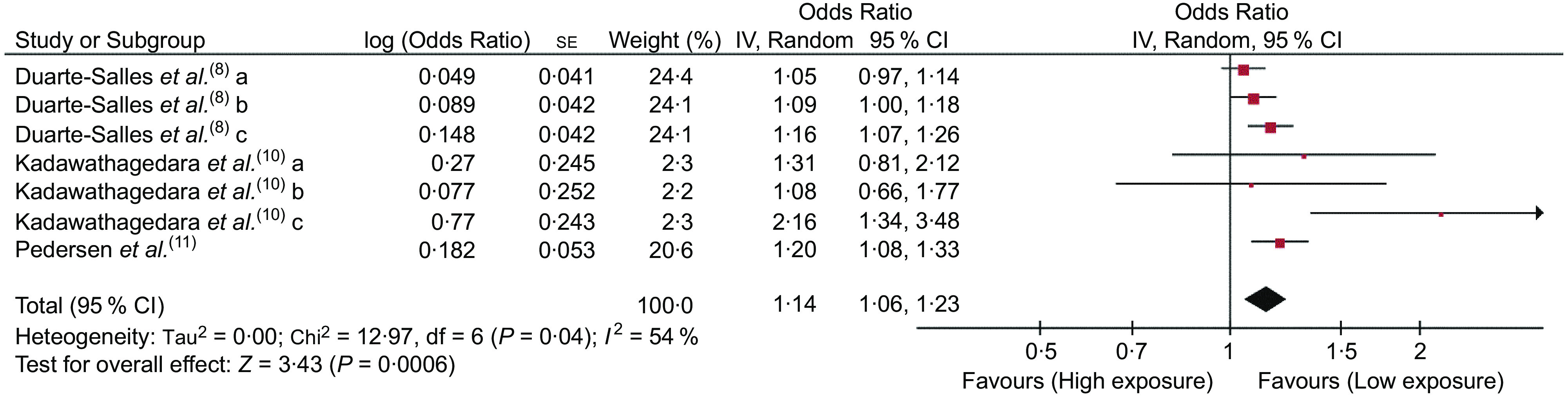
Forest plot of the pooled OR of small for gestational age between the high and low acrylamide exposure groups (The pooled OR revealed maternal high acrylamide exposure significantly increased the risk of small for gestational age. a: quantile 2 v. quantile 1; b: quantile 3 v. quantile 1; c: quantile 4 v. quantile 1)
Fig. 4.
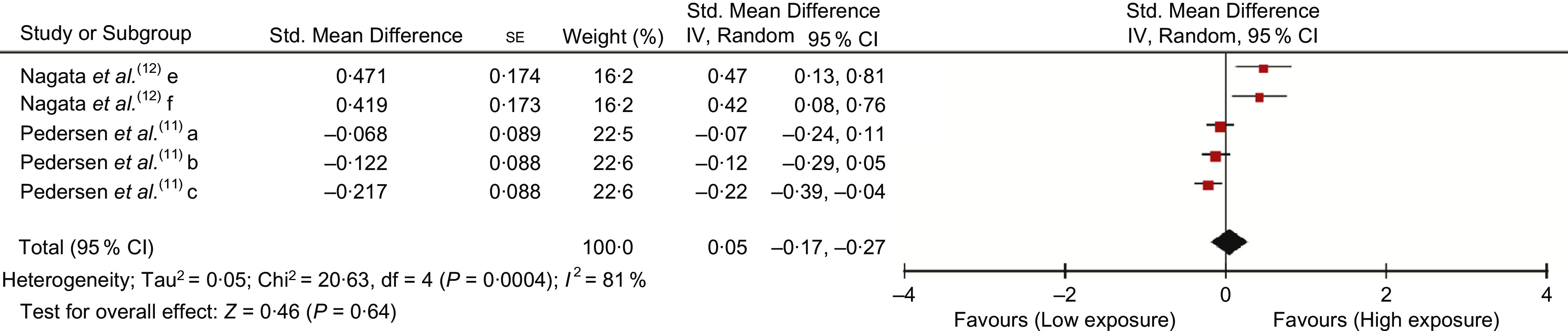
Forest plot of the pooled standardised mean difference of offspring’s head circumference between the high and low acrylamide exposure groups (The pooled standardised mean difference suggested that offspring’s head circumference was no significant difference between the two groups. a: quantile 2 v. quantile 1; b: quantile 3 v. quantile 1; c: quantile 4 v. quantile 1; e: tertile 2 v. tertile 1; f: tertile 3 v. tertile 1)
Secondary outcomes: acrylamide and offspring’s growth
One study(9) reported the association between prenatal AA exposure and offspring’s overweight/obesity. OR suggested that children had a high risk of developing overweight/obesity in the future in maternal high AA exposure group (OR 1·14, 95 % CI 1·08, 1·21, P < 0·001 at age 3; OR 1·13, 95 % CI 1·07, 1·19, P < 0·001 at age 5; OR 1·09, 95 % CI 1·02, 1·16, P = 0·020 at age 8) (online Supplemental Fig. 1).
Subgroup analysis
After conducting subgroup analysis on birth weight, we found that there was no significant difference between high AA exposure group and low AA exposure group in Asian people (SMD 0·09, 95 % CI –0·15, 0·33, P = 0·446), also in measure method by FFQ group (SMD –0·01, 95 % CI, –0·03, 0·00, P = 0·067) and partition method by tertiles group (SMD 0·09, 95 % CI –0·15, 0·33, P = 0·446). As to subgroup analysis on SGA, we could not find any differences between two groups in medium quality study (SMD 1·46, 95 % CI 0·97, 2·19, P = 0·069). Surprisingly, we could not find any significant difference between highest and lowest AA exposure group on birth weight and SGA (SMD –0·12, 95 % CI –0·26, 0·06, P = 0·203; OR 1·51, 95 % CI 0·83, 2·76, P = 0·179, respectively). Other subgroup results are shown in Table 2.
Table 2.
Subgroup meta-analysis of birth weight and small for gestational age
| Outcomes | Included studies (n) | Participants(n) | Effect size (SMD/OR) | 95 % CI | P | Heterogeneity (I 2, %) |
|---|---|---|---|---|---|---|
| Birth weight | ||||||
| Smoker | ||||||
| Yes | 1 | 4231 | –0·08 | –0·13, –0·03 | 0·003 | 0·0 |
| No | 2 | 47 392 | –0·04 | –0·07, –0·01 | 0·020 | 59·3* |
| Continent | ||||||
| Europe | 3 | 54 524 | –0·06 | –0·10, –0·02 | 0·003 | 72·1* |
| Asia | 1 | 204 | 0·09 | –0·15, 0·33 | 0·446 | 0·0 |
| Measured method of acrylamide exposure | ||||||
| FFQ | 3 | 53 627 | –0·01 | –0·03, 0·00 | 0·067 | 3·5 |
| HbAA | 1 | 1101 | –0·24 | –0·34, –0·14 | <0·001 | 0·0 |
| Partition of acrylamide exposure | ||||||
| Quartiles | 3 | 54 524 | –0·06 | –0·10, –0·02 | 0·003 | 72·1* |
| Tertiles | 1 | 204 | 0·09 | –0·15, 0·33 | 0·446 | 0·0 |
| Acrylamide exposure | ||||||
| HG v. LG | 4 | 27 000 | –0·12 | –0·26, 0·06 | 0·203 | 79·7* |
| Study quality | ||||||
| High | 2 | 53 053 | –0·05 | –0·09, –0·01 | 0·029 | 78·4* |
| Medium | 2 | 1675 | –0·09 | –0·17, –0·01 | 0·023 | 0·0 |
| SGA | ||||||
| Smoker | ||||||
| Yes | 2 | 4627 | 1·10 | 1·01, 1·21 | 0·039 | 0·0 |
| No | 3 | 48 289 | 1·12 | 1·06, 1·18 | <0·001 | 27·8 |
| Measured method of acrylamide exposure | ||||||
| FFQ | 2 | 52 122 | 1·13 | 1·03, 1·23 | 0·007 | 54·9* |
| HbAA | 1 | 1101 | 1·20 | 1·08, 1·33 | 0·001 | – |
| Acrylamide exposure | ||||||
| HG v. LG | 2 | 26 012 | 1·51 | 0·83, 2·76 | 0·179 | 84·3* |
| Study quality | ||||||
| High | 2 | 51 752 | 1·12 | 1·06, 1·18 | <0·001 | 42·6 |
| Medium | 1 | 1471 | 1·46 | 0·97, 2·19 | 0·069 | 52·7 |
HG, highest group; LG, lowest group; SGA, small for gestational age; FFQ, food frequency questionnaires; HbAA, Hb adducts of acrylamide.
P < 0·10.
Sensitivity analysis
Sensitivity analyses of adjusting confounders for the primary outcomes showed that the pooled SMD of high AA exposure group v. low exposure group for birth weight was –0·12 (95 % CI –0·19, –0·06, P < 0·001), and the pooled OR of high exposure group v. low exposure group for SGA was 1·11 (95 % CI 1·02, 1·20, P = 0·017). No significance difference was found between two groups on head circumference (SMD 0·10, 95 % CI –0·10, 0·31, P = 0·321) (Table 3).
Table 3.
Sensitivity analyses of adjusting confounders for the primary outcomes
| Outcomes | Study | Participants (n) | Adjusted variables | Pooled effect | |||
|---|---|---|---|---|---|---|---|
| Effect size (SMD/OR) | 95 % CI | P | Heterogeneity (I 2, %) | ||||
| Birth weight | Kadawathagedara et al.(10) | 1471 | Study centre, maternal age and gestational age at delivery, parity, height, education level, tobacco consumption during pregnancy, sex, maternal weight gain, pre-pregnancy BMI, the interaction between maternal BMI and weight gain | –0·12 | –0·19, –0·06 | <0·001 | 0·0 |
| Nagata et al.(12) | 204 | Age, parity, smoking status, pre-pregnancy height and weight, weight gain, weeks of gestation at the time of blood sampling, total energy | |||||
| Pedersen et al.(11) | 747 | Gestational age, maternal smoking during pregnancy, passive smoking, sex, pre-pregnancy BMI, parity, maternal age, maternal ethnicity, maternal education, and maternal consumption of fruit and vegetables, fish, soft drinks | |||||
| SGA | Duarte-Salles et al.(8) | 50 651 | Gestational age, parity, sex of the child, maternal age, maternal BMI, gestational weight gain, smoking during pregnancy | 1·11 | 1·02, 1·20 | 0·017 | 46·9* |
| Kadawathagedara et al.(10) | 1471 | Study centre, maternal age at delivery, education level, tobacco consumption during pregnancy, specific maternal weight gain during pregnancy | |||||
| Head circumference | Nagata et al.(12) | 204 | Age, parity, smoking status, pre-pregnancy height and weight, weight gain, weeks of gestation at the time of blood sampling, total energy | 0·10 | –0·10, 0·31 | 0·321 | 71·3* |
| Pedersen et al.(11) | 713 | Gestational age, maternal smoking during pregnancy, passive smoking, sex, pre-pregnancy BMI, parity, maternal age, maternal ethnicity, maternal education, and maternal consumption of fruit and vegetables, fish, soft drinks | |||||
SGA, small for gestational age.
P < 0·10.
Another sensitivity analysis was conducted on birth weight. We could find one study might dominate the pooled results from online Supplemental Fig. 2, and after deleting, the heterogeneity reduced (I 2 dropped from 66 to 3 %) but the association became not significant (SMD –0·01, 95 % CI –0·03, 0·00, P = 0·070).
Publication bias
After conducting funnel plots on the results of birth weight, we found the distributions of studies were relatively symmetrical in the figures (online Supplemental Fig. 3). We also conducted an Egger’s test and did not identify the significant statistical publication bias on the result of birth weight (P = 0·389).
Discussion
The present systematic review and meta-analysis of five cohort studies including 54 728 participants suggest the associations between gestational AA exposure and decreasing birth weight, head circumference and offspring’s overweight/obesity. These findings have important implications for conducting health education, providing guidance on maternal diet and developing an appropriate dietary strategy for pregnant women to reduce dietary AA exposure.
In the body, AA can be converted metabolically to glycidamide, a chemically reactive and genotoxic epoxide(21). Studies showed that AA had short- and long-term effects on the growth and development of offspring. A potential mechanism of AA affecting birth weight is that AA and its metabolite glycidamide can react with or create specific adducts on nucleophilic sites of DNA or protein implicated in the regulation of growth(8). As to the long-term effect, gestational AA exposure increases the risk on overweight/obesity in the childhood. On the one hand, endocrine disrupting chemicals that can mimic or interfere with the effects of endogenous hormones have been proved to increase the susceptibility to overweight and obesity(22). Although AA is not known to be an endocrine disrupting chemical, maternal AA intake is positively associated with umbilical cord oestradiol levels(12), which may influence children’s growth. On the other hand, high AA exposure level is related with increased reactive oxygen radicals and inflammation(23) in adults. And, maternal inflammation during pregnancy has been associated with a higher risk of childhood overall adiposity and central adiposity(24).
A recent study indicated the significant associations between AA exposure level and the likelihoods of allergy-related outcomes in the general US population(6). The biological mechanisms for the effects of AA on immunological health outcomes are still unclear. A hypothesis is that AA exerts immunotoxicity effect through the influence on glucose homoeostasis(6) because AA has been reported to be associated with decreased serum insulin level and insulin resistance in adults(25), and further affects immune responses(26). In fact, impaired glucose homoeostasis is closely related to inflammation and immune responses.
FFQ is a convenient and economic method to estimate AA intake, but may not reflect the real exposure in human body. Hb adducts of AA is stable and reflects longer time window for exposure and thus is a well-established biomarker of internal exposure(27). Though a study(8) supported that AA intake estimated by the FFQ was highly correlated with Hb adduct levels in blood samples, the subgroup analysis in the present study showed that the pooled result was different in FFQ group and Hb adducts of AA group, indicating that there might be a measurement bias assessed by FFQ. What is more, smoking is another main source of AA. Our meta-analysis proved that smoking plus high AA dietary exposure further increased the risk of lower birth weight and SGA, which was consistent with the results of previous studies(8,10,11).
Our studies summarised the main food sources of exposure to AA were fried potatoes, chips, crispbread and coffee. However, fibre-rich bread including crispbread and dark bread has been recommended as components of a healthy diet during pregnancy(28,29). In addition to AA, the effect of fried potatoes or chips may be even more detrimental due to a combined effect with other Maillard products with potential toxic effects(30). In the current study, we could not identify any significant differences on birth weight and SGA between the highest and lowest AA exposure group by subgroup analysis, which might similarly suggest a neutralising effect with other compounds in healthy food rich in AA.
Although we have collected data for which confounders have been adjusted from the included studies and conducted the sensitivity analyses, it is difficult to examine the real effect of AA exposure on adverse pregnancy outcomes. Because AA intake is enormously susceptible to the following residual confounders but most studies fail to adjust for them on the overall findings. On one hand, the main sources of AA are foods for which there would be reasonable concerns of adverse perinatal effects based on their nutritional characteristics alone (such as glycaemic load of fried potatoes and bread)(31). On the other hand, high exposure of AA can affect maternal and fetal health by virtue of being part of dietary patterns including unhealthy foods (e.g. fried potatoes being part of diet patterns favouring consumption of fast foods)(32). Therefore, the results of high exposure of AA intake inducing adverse pregnancy outcomes require well-designed prospective studies and more biological mechanisms to confirm.
The present meta-analysis has the following limitations that should be taken into account. First, only five eligible studies were included, and the combined results might not be robust. Second, most of the studies estimated AA exposure by FFQ, which could not reflect the real internal exposure and could not provide direct and reliable inference of causality. Third, we could not eliminate the heterogeneity among the included studies, but we performed subgroup analyses and sensitivity analyses to explore the sources of heterogeneity. Finally, there might be potential confounders in different studies, which influenced the pooled effect sizes, and the pooled results should be treated with caution.
Conclusions
In conclusion, the present meta-analysis provides evidence to support that higher gestational AA exposure increases the risk of lower birth weight, lower head circumference and overweight/obesity. Our findings require more biological mechanisms to confirm. But for the ubiquitous exposure to AA, the potential public health applications of the findings are substantial.
Acknowledgements
Acknowledgements: None. Financial support: This research received no specific grant from any funding agency, commercial or not-for-profit sectors. Conflict of interest: None. Authorship: Y.J. formulated the research question; S.Z. designed the study and Y.Z. carried it out. Y.X. and T.G. analysed the data; All authors are involved in writing the article. Ethics of human subject participation: None.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980019005123.
click here to view supplementary material
References
- 1. IARC (1994) IARC working group on the evaluation of carcinogenic risks to humans: some industrial chemicals. Lyon, 15–22 February 1994. IARC Monogr Eval Carcinog Risks Hum 60, 1–560.7869568 [Google Scholar]
- 2. Tareke E, Rydberg P, Karlsson P et al. (2002) Analysis of acrylamide, a carcinogen formed in heated foodstuffs. J Agric Food Chem 50, 4998–5006. [DOI] [PubMed] [Google Scholar]
- 3. Vikstrom AC, Warholm M, Paulsson B et al. (2012) Hemoglobin adducts as a measure of variations in exposure to acrylamide in food and comparison to questionnaire data. Food Chem Toxicol 50, 2531–2539. [DOI] [PubMed] [Google Scholar]
- 4. EFSA Panel on Contaminants in the Food Chain (2015) Scientific opinion on acrylamide in food. EFSA J 13, 4104. [Google Scholar]
- 5. Yilmaz BO, Yildizbayrak N, Aydin Y et al. (2017) Evidence of acrylamide- and glycidamide-induced oxidative stress and apoptosis in Leydig and Sertoli cells. Hum Exp Toxicol 36, 1225–1235. [DOI] [PubMed] [Google Scholar]
- 6. Guo J, Yu D, Lv N et al. (2017) Relationships between acrylamide and glycidamide hemoglobin adduct levels and allergy-related outcomes in general US population, NHANES 2005–2006. Environ Pollut 225, 506–513. [DOI] [PubMed] [Google Scholar]
- 7. von Stedingk H, Vikstrom AC, Rydberg P et al. (2011) Analysis of hemoglobin adducts from acrylamide, glycidamide, and ethylene oxide in paired mother/cord blood samples from Denmark. Chem Res Toxicol 24, 1957–1965. [DOI] [PubMed] [Google Scholar]
- 8. Duarte-Salles T, von Stedingk H, Granum B et al. (2013) Dietary acrylamide intake during pregnancy and fetal growth-results from the Norwegian Mother and child cohort study (MoBa). Environ Health Perspect 121, 374–379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Kadawathagedara M, Botton J, de Lauzon-Guillain B et al. (2018) Dietary acrylamide intake during pregnancy and postnatal growth and obesity: results from the Norwegian Mother and Child Cohort Study (MoBa). Environ Int 113, 325–334. [DOI] [PubMed] [Google Scholar]
- 10. Kadawathagedara M, Tong ACH, Heude B et al. (2016) Dietary acrylamide intake during pregnancy and anthropometry at birth in the French EDEN mother-child cohort study. Environ Res 149, 189–196. [DOI] [PubMed] [Google Scholar]
- 11. Pedersen M, Von Stedingk H, Botsivali M et al. (2012) Birth weight, head circumference, and prenatal exposure to acrylamide from maternal diet: the European prospective mother–child study (NewGeneris). Environ Health Perspect 120, 1739–1745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Nagata C, Konishi K, Wada K et al. (2018) Maternal acrylamide intake during pregnancy and sex hormone levels in maternal and umbilical cord blood and birth size of offspring. Nutr Cancer 14, 1–6. [DOI] [PubMed] [Google Scholar]
- 13. Knop MR, Geng TT, Gorny AW et al. (2018) Birth weight and risk of type 2 diabetes mellitus, cardiovascular disease, and hypertension in adults: a meta-analysis of 7 646 267 participants from 135 studies. J Am Heart Assoc 7, e008870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Risnes KR, Vatten LJ, Baker JL et al. (2011) Birthweight and mortality in adulthood: a systematic review and meta-analysis. Int J Epidemiol 40, 647–661. [DOI] [PubMed] [Google Scholar]
- 15. Godfrey KM & Barker DJ (2000) Fetal nutrition and adult disease. Am J Clin Nutr 71, 1344S–1352S. [DOI] [PubMed] [Google Scholar]
- 16. Moher D, Liberati A, Tetzlaff J et al. (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 151, 264–269. [DOI] [PubMed] [Google Scholar]
- 17. Higgins J & Green S (2011) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration. http://handbook.cochrane.org (accessed March 2011). [Google Scholar]
- 18. Wells GA, Shea B, O’Connell D et al. (2011) The Newcastle–Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in Meta-Analyses. www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed November 2012).
- 19. Higgins JP, Thompson SG, Deeks JJ et al. (2003) Measuring inconsistency in meta-analyses. BMJ 327, 557–560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Egger M, Davey Smith G, Schneider M et al. (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315, 629–634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Sweeney LM, Kirman CR, Gargas ML et al. (2010) Development of a physiologically-based toxicokinetic model of acrylamide and glycidamide in rats and humans. Food Chem Toxicol 48, 668–685. [DOI] [PubMed] [Google Scholar]
- 22. Botton J, Kadawathagedara M & de Lauzon-Guillain B (2017) Endocrine disrupting chemicals and growth of children. Ann Endocrinol 78, 108–111. [DOI] [PubMed] [Google Scholar]
- 23. Naruszewicz M, Zapolska-Downar D, Kosmider A et al. (2009) Chronic intake of potato chips in humans increases the production of reactive oxygen radicals by leukocytes and increases plasma C-reactive protein: a pilot study. Am J Clin Nutr 89, 773–777. [DOI] [PubMed] [Google Scholar]
- 24. Gaillard R, Rifas-Shiman SL, Perng W et al. (2016) Maternal inflammation during pregnancy and childhood adiposity. Obesity 24, 1320–1327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Lin CY, Lin YC, Kuo HK et al. (2009) Association among acrylamide, blood insulin, and insulin resistance in adults. Diabetes Care 32, 2206–2211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Takeda Y, Shimomura T & Wakabayashi I (2014) Immunological disorders of diabetes mellitus in experimental rat models. JPN J HYG 69, 166–176. [DOI] [PubMed] [Google Scholar]
- 27. Vesper HW, Caudill SP, Osterloh JD et al. (2010) Exposure of the U.S. population to acrylamide in the National Health and Nutrition Examination Survey 2003–2004. Environ Health Perspect 118, 278–283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. von Ruesten A, Brantsaeter AL, Haugen M et al. (2014) Adherence of pregnant women to Nordic dietary guidelines in relation to postpartum weight retention: results from the Norwegian Mother and Child Cohort Study. BMC Public Health 14, 75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Englund-Ogge L, Brantsaeter AL, Sengpiel V et al. (2014) Maternal dietary patterns and preterm delivery: results from large prospective cohort study. BMJ 348, g1446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. El-Sayyad HI, Abou-Egla MH, El-Sayyad FI et al. (2011) Effects of fried potato chip supplementation on mouse pregnancy and fetal development. Nutrition 27, 343–350. [DOI] [PubMed] [Google Scholar]
- 31. Maslova E, Hansen S, Grunnet LG et al. (2019) Maternal glycemic index and glycemic load in pregnancy and offspring metabolic health in childhood and adolescence – a cohort study of 68,471 mother-offspring dyads from the Danish National Birth Cohort. Eur J Clin Nutr 73, 1049–1062. [DOI] [PubMed] [Google Scholar]
- 32. Raghavan R, Dreibelbis C, Kingshipp BL et al. (2019) Dietary patterns before and during pregnancy and birth outcomes: a systematic review. Am J Clin Nutr 109, 729S–756S. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980019005123.
click here to view supplementary material