

Abstract
Objective:
To examine the psychometric properties of an Arabic version of the Child Feeding Questionnaire (CFQ-A) in a sample of Saudi pre-schoolers and their mothers.
Design:
Cross-sectional study. Mothers completed questionnaires over the telephone and child anthropometry was measured objectively using standardized procedures; BMI Z-scores (BMIZ) were calculated based on the age- and sex-specific WHO growth standards and reference data. Confirmatory factor analysis was used to examine the original seven-factor CFQ model, as well as a modified nine-factor model. Cronbach’s α was calculated to examine the internal consistency of each factor; Spearman correlation was used to examine 2-week retest reliability. Factor–factor and factor–child BMIZ correlations were examined.
Setting:
Jeddah, Kingdom of Saudi Arabia.
Participants:
A total of 209 mothers and children were recruited from eight different pre-schools.
Results:
Both the original seven-factor and modified nine-factor CFQ-A exhibited good fit (root-mean-square-error of approximation < 0·05). Six out of nine factors had excellent internal consistency and all factors showed excellent 2-week test–retest reliability. There were significant correlations between child BMIZ and five out of the nine factors; Perceived Child Weight, Perceived Parent Weight, Restriction and Monitoring were each positively correlated with child BMIZ, while Concern about Child’s Diet was negatively correlated with child BMIZ.
Conclusions:
The study provided evidence supporting the validity and reliability of the original seven-factor and modified nine-factor CFQ-A. Future studies are needed to further establish the psychometric properties of the CFQ-A in addition to other feeding assessment tools.
Keywords: Validation, Maternal feeding, Pre-schoolers, BMI Z-score
Globally, the troubling burden of obesity continues to be evident among both children and adults(1) as the prevalence of elevated BMI and its associated morbidity and mortality continue to soar(1,2). Since childhood is a critical period for shaping lifelong obesity risk(3), identifying modifiable risk factors at an early age is vital for the promotion and maintenance of a healthy weight status(4).
Characteristics of the mealtime environment and the behaviour of family members around food have been associated with child eating behaviours and weight status in several predominantly developed countries, including the USA, the UK and Australia(5–10). For example, overly demanding maternal feeding behaviours and restriction, such as use of punishments and rewards, were found to be inversely associated with children’s ability to self-regulate food intake, which can lead to overeating and weight gain(11–14). Indulgent feeding behaviours and low involvement in child feeding have also been associated with higher weight status among children(6,15). Although evidence supporting causal associations between maternal feeding behaviours and child obesity is lacking(16), results from several studies show that the association between maternal feeding and child eating behaviours is bidirectional; mothers may adjust and adapt the way they approach feeding in response to the child’s temperament, behaviour and weight status(9,17,18) and the mother’s approach to feeding can in turn influence the child’s counter-response and behaviour around food(19). Therefore, maladaptive feeding and eating behaviours of mothers and their children may be described as a viscous cycle of obesogenic events that can ultimately promote an unhealthy weight status. Hence, validated instruments that aid in the evaluation of both maternal feeding and child eating behaviours are needed in order to efficiently identify maladaptive behaviours and subsequently promote a healthier mealtime environment.
As seen in many countries around the world, the prevalence of obesity and obesity-related diseases (e.g. type 2 diabetes) in the Kingdom of Saudi Arabia (KSA) has been increasing alarmingly(20). The prevalence of overweight and obesity among children is concerning, where about 32 % of children were found to be overweight or obese(21). Moreover, KSA is classified as a country experiencing advanced nutrition transition, such that dietary patterns are changing rapidly and drastically to mimic those seen in Western countries(22,23). It is hypothesized that these changes in dietary intake are secondary to changes in socio-economic status and social and familial norms(24). Although these sociocultural adaptations are likely to be accompanied by changes in the family mealtime environment, family mealtimes and the behaviour of family members around food in Saudi society have not been efficiently explored. Although one study found that Saudi mothers of pre-school children may use restriction and pressure to eat in feeding(25), we were unable to identify any other studies evaluating maternal feeding behaviours and practices as they relate to child weight status. Additionally, we were able to identify only one study that evaluated initial validity of a child feeding assessment tool in a convenience sample of highly educated Saudi mothers living in the USA(25).
The Child Feeding Questionnaire (CFQ) is a feeding behaviour assessment tool that was first developed by Birch et al. in 2001 to assess parental beliefs, attitudes and practices relating to child feeding in a US cohort of parents of 2–11-year-old children(26). The questionnaire consists of thirty-one items with 5-point Likert response scales and generates seven factors: Perceived Responsibility; Perceived Parent Weight; Perceived Child Weight; Concern about Child Weight; Restriction; Pressure to Eat; and Monitoring. Although some studies involving CFQ subscales have shown poor or mediocre model fit(27) and problematic structure of some factors (mainly Restriction)(27–30), several studies have reported evidence of validity and reliability in US(26,31,32) and non-US samples(10,29,30,33,34).
Given the immediate need for valid and reliable, culturally sensitive instruments to assess feeding in KSA, the objective of the present study was to examine the psychometric properties of an Arabic version of the CFQ (CFQ-A) in a sample of Saudi pre-schoolers and their mothers by: (i) testing the original seven-factor CFQ-A model in addition to a modified nine-factor CFQ-A model and examining model fit and internal reliability of subscales; (ii) examining test–retest reliability of CFQ-A factors; and (iii) examining intercorrelations among CFQ-A factors as well as correlations with child BMI Z-score (BMIZ).
In developing the modified nine-factor CFQ-A model, we hypothesized that Saudi mothers are more invested and indulgent in feeding and that they like to ensure that their children are ‘eating enough food’ and that they are at the heavier end of the normal weight range(25,35,36). We therefore added the two additional factors, Use of Food as a Reward and Concern about Child’s Diet. Moreover, we hypothesized that Perceived Child Weight, Concern about Child Weight and Concern about Child’s Diet are correlated with feeding practices including Restriction, Pressure to Eat, Monitoring, Perceived Responsibility and Use of Food as a Reward, and that these maternal perceptions and practices are also correlated with child BMIZ(37). Results from the present study can help provide evidence regarding the appropriateness of use of an Arabic version of the CFQ in Saudi Arabia. Findings can also help identify and inform future work needed for further development of efficient feeding assessment tools among Saudi/Arab populations.
Methods
Sample and procedures
A total of 209 mothers and children were included in the present study. Participants were recruited from eight different pre-schools around the city of Jeddah, KSA. Schools were randomly selected based on location; two schools were located in the northern area, two in the southern area, two in the eastern area and two in the western area. Of the eight pre-schools, four were public (government-subsidized) and four were private pre-schools. A description of the study and consent forms were placed in the backpacks of all students enrolled in the pre-schools. Research assistants contacted mothers who returned signed consent forms and completed the study questionnaire with them over the telephone. The study questionnaire included the CFQ-A, questions that assessed use of food as a reward and concern about child’s diet, and questions that assessed demographic characteristics.
Within 1 week of completing the questionnaire, the study team performed school visits in order to obtain weight and height measurements of participating children. Study inclusion criteria were as follows: child is Saudi or a permanent resident of KSA; between 3 and 5 years old; resides with his/her mother and is healthy with no serious medical problems or history of food allergies; and mother is an Arabic speaker. In order to examine test–retest reliability, forty randomly selected mothers (19 %) completed the questionnaire for a second time approximately 2 weeks after the initial telephone call.
Measures
Demographic characteristics
Mothers were asked questions that assessed demographic characteristics including the child’s sex, birthdate and nationality; the mother’s birthdate, educational level, employment status, marital status and nationality; as well as the family’s total monthly income. Birthdates and dates of interviews were used to calculate child and maternal age.
The Arabic version of the Child Feeding Questionnaire
Mothers completed the CFQ-A in Arabic language, following a forward–backward translation process conducted by bilingual professionals(10,38). The final version of the CFQ-A was pretested using a different sample consisting of sixty mothers of pre-school children and was reviewed by an expert committee of four health-care professionals. Clarifications were made to wording of questions and response options based on comments from mothers and expert committee members.
Use of food as a reward and concern about child’s diet
Saudi mothers may be more indulgent in feeding, traditionally use food as a reward to encourage desirable behaviours and may consciously or subconsciously follow the traditional belief that heavier children are healthier(25,35,36). We therefore elected to evaluate a modified CFQ-A model that assessed Use of Food as a Reward as a separate construct, rather than including these items with the Restriction subscale, as employed in the original questionnaire(26). This approach yielded satisfactory results among a sample of Chinese mothers(33). Furthermore, we included a separate subscale for assessing Concern about Child’s Diet.
Mothers completed questions that were adapted from the Meals in Our Household Questionnaire, a questionnaire developed to assess family meals in the households of 3–11-year-old children(40). Questions included six items that assessed Use of Food as a Reward (FR; response options ranging from 1 = ‘never’ to 5 = ‘always’)(39). These items were: FR1, ‘I give my child food to keep him/her quiet when shopping or travelling’; FR2, ‘I give my child food to reward him/her for good behaviour’; FR3, ‘I withhold a food my child likes as a consequence for bad behaviour’; FR4, ‘My child expects to be given a favourite food as a reward’; FR5, ‘I give my child a special food to celebrate an achievement’; and FR6, ‘I give my child food to persuade him/her to do something he/she does not really want to do’. In addition, mothers completed seven out of seventeen items that assessed Concern about Child’s Diet (CD; response options ranging from 1 = ‘not at all concerned’ to 6 = ‘extremely concerned’)(39). We selected items that reflected concern about child’s diet in general, rather than those that measured concern about child’s consumption of specific food types (e.g. CD14 and CD17 concerning eating vegetables and meat). These items were: CD1, ‘Child is not eating enough’; CD2, ‘Child is eating too much’; CD3, ‘Child eats a lot of junk food’; CD4, ‘Child eats only a few types of food’; CD5, ‘Child is not getting good nutrition’; CD6, ‘Child has poor eating habits’; and CD7, ‘Child will not try new foods’.
The same translation and pretesting process was utilized with these items, which were used to construct a modified nine-factor CFQ-A model as described in following sections.
Child BMI Z-score
Trained staff members followed standardized procedures to measure children’s weights and heights. Calibration of the instruments was checked periodically. Shoes and heavy clothing were removed and the child was asked to stand still on a digital scale, with his/her weight equally distributed on both feet. Each child was weighed twice and if the two readings were inconsistent by more than 0·1 kg, the child was weighed two more times and the average of the two measurements was calculated. Similarly, height was measured twice and if the measurements differed by more than 0·5 cm, two more measurements were taken and the average of the two measurements was calculated. BMI was calculated for each child by dividing weight (in kilograms) by the square of height (in metres)(40). BMIZ were calculated based on the age- and sex-specific WHO growth standards for children aged ≤5 years and the WHO growth reference data for children who were between 5 and 6 years old(41,42). Two children had missing weight and height data due to transferring to other schools and were therefore excluded from analyses involving child BMI data.
Statistical analysis
Analyses were conducted using the statistical software package IBM SPSS Statistics version 21.0. Descriptive statistics were used to examine sample characteristics, as well as the distribution of questionnaire factors, maternal BMI and child BMIZ.
To examine internal reliability, Cronbach’s α was calculated for each factor in the seven- and nine-factor CFQ-A models. A Cronbach’s α value of 0·70 or higher is considered favourable(43,44). Spearman correlation coefficients were calculated to examine the 2-week test–retest reliability of the CFQ-A factors.
To assess validity of the seven- and nine-factor models, confirmatory factor analysis was performed using lavaan version 0.5-23(45) in R version 3.3.1. Diagonally weighted least squares was used to estimate model parameters. Diagonally weighted least squares was specifically designed for ordinal data and is more appropriate/recommended for use with Likert-type scales(46,47).
Fit indices were estimated for each of the models by calculating the root-mean-square error of approximation, Tucker–Lewis index, comparative fit index, standardized root-mean-square residual, and the likelihood ratio test or the minimum sample discrepancy function/df(48,49). The suitability of confirmatory factor analysis was assessed prior to conducting the analysis, and inspection of the correlation matrix showed that all variables in both the seven-factor and nine-factor models had correlation coefficients greater than 0·30.
Table 1 summarizes factors and subscales of the original seven-factor CFQ-A, as well as the modified nine-factor CFQ-A. The modified nine-factor CFQ-A model includes two additional factors: Use of Food as a Reward and Concern about Child’s Diet(39). As described earlier, items relating to using food as a reward were removed from the Restriction subscale and were included only in the Use of Food as a Reward subscale in the modified nine-factor model. These items were RST3A and RST3B. Scores for all factors were calculated as the mean of contributing items, with higher scores reflecting more of the given behaviour(26).
Table 1.
Summary of factors and subscales of the original seven-factor and modified nine-factor Arabic version of the Child Feeding Questionnaire (CFQ-A)
| Original seven-factor CFQ-A | Modified nine-factor CFQ-A |
|---|---|
| Perceived Responsibility (PR) | Perceived Responsibility (PR) |
| Items: PR1, PR2, PR3 | Items: PR1, PR2, PR3 |
| Response options: 1 = never; 2 = seldom; 3 = half of the time; 4 = most of the time; 5 = always | Response options: 1 = never; 2 = seldom; 3 = half of the time; 4 = most of the time; 5 = always |
| Perceived Parent Weight (PPW) | Perceived Parent Weight (PPW) |
| Items: PPW1, PPW2, PPW3, PPW4 | Items: PPW1, PPW2, PPW3, PPW4 |
| Response options: 1 = markedly underweight; 2 = underweight; 3 = normal; 4 = overweight; 5 = markedly overweight | Response options: 1 = markedly underweight; 2 = underweight; 3 = normal; 4 = overweight; 5 = markedly overweight |
| Perceived Child Weight (PCW) | Perceived Child Weight (PCW) |
| Items: PCW1, PCW2, PCW3, PCW4 (PCW5 and PCW6 not included due to sample age) | Items: PCW1, PCW2, PCW3, PCW4 (PCW5 and PCW6 not included due to sample age) |
| Response options: 1 = markedly underweight; 2 = underweight; 3 = normal; 4 = overweight; 5 = markedly overweight | Response options: 1 = markedly underweight; 2 = underweight; 3 = normal; 4 = overweight; 5 = markedly overweight |
| Concern about Child Weight (CN) | Concern about Child Weight (CN) |
| Items: CN1, CN2, CN3 | Items: CN1, CN2, CN3 |
| Response options: 1 = unconcerned; 2 = a little concerned; 3 = concerned; 4 = fairly concerned; 5 = very concerned | Response options: 1 = unconcerned; 2 = a little concerned; 3 = concerned; 4 = fairly concerned; 5 = very concerned |
| Restriction (RST) | Restriction (RST) |
| Items: RST1A, RST1B, RST1C, RST2, RST3A, RST3B, RST4A, RST4B | Items: RST1C, RST2, RST4A, RST4B |
| Response options: 1 = disagree; 2 = slightly disagree; 3 = neutral; 4 = slightly agree; 5 = agree | Response options: 1 = disagree; 2 = slightly disagree; 3 = neutral; 4 = slightly agree; 5 = agree |
| Pressure to Eat (PE) | Pressure to Eat (PE) |
| Items: PE1, PE2, PE3, PE4 | Items: PE1, PE2, PE3, PE4 |
| Response options: 1 = disagree; 2 = slightly disagree; 3 = neutral; 4 = slightly agree; 5 = agree | Response options: 1 = disagree; 2 = slightly disagree; 3 = neutral; 4 = slightly agree; 5 = agree |
| Monitoring (MN) | Monitoring (MN) |
| Items: MN1, MN2, MN3 | Items: MN1, MN2, MN3 |
| Response options: 1 = never; 2 = rarely; 3 = sometimes; 4 = mostly; 5 = always | Response options: 1 = never; 2 = rarely; 3 = sometimes; 4 = mostly; 5 = always |
| Use of Food as a Reward (FR) | |
| Items: FR1, FR2, FR3, FR4, FR5, FR6 | |
| Response options: 1 = never; 2 = rarely; 3 = sometimes; 4 = often; 5 = very often | |
| Concern about Child’s Diet (CD) | |
| Items: CD1, CD2, CD3, CD4, CD5, CD6, CD7 | |
| Response options: 1 = not at all concerned; 2 = a little concerned; 3 = somewhat concerned; 4 = quite concerned; 5 = very concerned; 6 = extremely concerned |
Intercorrelations among the modified CFQ-A factors as well as correlations with child BMIZ were examined. Interpretation of the correlation coefficients were based on Cohen’s guidelines(50); correlations between 0·5 and 1·0 were considered large, correlations between 0·3 and 0·5 as medium and correlations between 0·1 and 0·3 as small. Only children with complete BMIZ data (n 207) were included in the correlation analysis between CFQ-A factors and child BMIZ. For all statistical analyses, the significance level was set at 0·05.
Results
Sample characteristics
Mean child age was 4·79 years (sd = 0·79 years), and about half of the sample (51·7 %) was male. The majority (approximately 70 %) of children and mothers were Saudi. Of the sixty-four non-Saudi children, about half (n 29, 45·3 %) were Egyptian, ten (15·6 %) were Syrian, eight were Yemeni (12·5 %), six were Jordanian (9·4 %), five (7·8 %) were Lebanese, five (7·8 %) were Palestinian and one (1·6 %) was Sudanese. In addition, the majority of mothers (80 %) had a college education or higher, and about half (51·2 %) reported that they were housewives (Table 2).
Table 2.
Characteristics of the sample of pre-schoolers and their mothers (n 209) recruited from eight different pre-schools in Jeddah city, Kingdom of Saudi Arabia, October 2017–April 2018
| Variable | Mean or n | sd or % |
|---|---|---|
| Child age (years) | 4·79 | 0·79 |
| Child sex | ||
| Male | 108 | 51·7 |
| Female | 101 | 48·3 |
| Child nationality | ||
| Saudi | 145 | 69·4 |
| Non-Saudi | 64 | 30·6 |
| Child BMI Z-score | 0·17 | 1·34 |
| Total monthly income | ||
| <5000 SR | 21 | 10·0 |
| 5000–10 000 SR | 74 | 35·4 |
| >10 000 SR | 114 | 54·5 |
| Maternal age (years) | 33·05 | 4·98 |
| Maternal nationality | ||
| Saudi | 140 | 67·0 |
| Non-Saudi | 69 | 33·0 |
| Maternal education | ||
| Middle school | 3 | 1·4 |
| High school | 39 | 18·7 |
| College | 142 | 67·9 |
| Postgraduate | 24 | 12·0 |
| Maternal employment | ||
| Employed | 84 | 40·2 |
| Housewife | 107 | 51·2 |
| Student | 15 | 7·2 |
| Other | 3 | 1·4 |
Data are presented as mean and sd for continuous variables or as n and % for categorical variables.
Table 3 shows the distribution (including mean, sd and range) of questionnaire factors.
Table 3.
Distribution and internal consistencies of factors of the Arabic version of the Child Feeding Questionnaire (CFQ-A) in the sample of pre-schoolers and their mothers (n 209) recruited from eight different pre-schools in Jeddah city, Kingdom of Saudi Arabia, October 2017–April 2018
| Minimum | Maximum | Mean | sd | Cronbach’s α | ||
|---|---|---|---|---|---|---|
| Seven-factor model | Nine-factor model | |||||
| Perceived Responsibility | 1·00 | 5·00 | 4·23 | 0·93 | 0·74 | 0·74 |
| Perceived Parent Weight | 2·00 | 5·00 | 3·20 | 0·47 | 0·67 | 0·67 |
| Perceived Child Weight | 2·00 | 4·75 | 2·90 | 0·35 | 0·70 | 0·70 |
| Concern about Child Weight | 1·00 | 5·00 | 1·62 | 1·17 | 0·88 | 0·88 |
| Restriction | 1·00 | 5·00 | 4·40 | 0·94 | 0·60 | 0·62 |
| Pressure to Eat | 1·00 | 5·00 | 3·91 | 1·14 | 0·49 | 0·49 |
| Monitoring | 1·00 | 5·00 | 4·44 | 0·80 | 0·86 | 0·86 |
| Use of Food as a Reward | 1·00 | 5·00 | 2·22 | 1·01 | – | 0·73 |
| Concern about Child’s Diet | 1·00 | 5·00 | 2·26 | 1·14 | – | 0·82 |
Internal and test–retest reliability
Table 3 shows the respective Cronbach’s α for each factor of the seven- and nine-factor CFQ-A models. For the seven-factor CFQ-A model, three factors fell below the 0·70 threshold: Perceived Parent Weight (Cronbach’s α=0·67), Restriction (Cronbach’s α = 0·60) and Pressure to Eat (Cronbach’s α=0·49). These same factors were also below the 0·70 threshold for the nine-factor CFQ-A model: Perceived Parent Weight (Cronbach’s α = 0·67), Restriction (Cronbach’s α = 0·62) and Pressure to Eat (Cronbach’s α = 0·49). All factors showed excellent 2-week test–retest reliability, with Spearman correlations > 0·70 (all P < 0·05).
Confirmatory factor analysis
The seven-factor CFQ-A model
Forced extraction of seven factors explained 19·53, 13·71, 10·17, 9·12, 7·10, 6·07 and 4·84 % of the total variance, respectively. The seven-factor solution explained 70·5 % of the total variance. The root-mean-square error of approximation of 0·02 indicates good fit(51). The Tucker–Lewis index and comparative fit index were calculated to be 0·96 and 0·97, respectively. The seven-factor model is illustrated in Fig. 1.
Fig. 1.

Seven-factor model of the Arabic version of the Child Feeding Questionnaire (CFQ-A), with the factors Perceived Responsibility, Perceived Parent Weight, Perceived Child Weight, Concern about Child Weight, Restriction, Monitoring and Pressure to Eat (see Table 1 for a description of the factors and subscales). Fit indices: root-mean-square error of approximation = 0·02 (95 % CI 0·00, 0·04), Tucker–Lewis index = 0·96, comparative fit index = 0·97, standardized root-mean-square residual = 0·07, χ2 = 267·7 (P < 0·001), minimum sample discrepancy function/df = 1·10 (ε1–ε29 are error terms)
The nine-factor CFQ-A model
Forced extraction of nine factors had explained 15·42, 13·43, 11·84, 7·57, 6·79, 5·01, 4·16, 3·62 and 3·59 % of the total variance, respectively. The nine-factor solution explained 71·4 % of the total variance. The root-mean-square error of approximation of 0·04 indicates good fit(51). The Tucker–Lewis index and comparative fit index were estimated to be 0·90 and 0·88, respectively. The nine-factor model is illustrated in Fig. 2. A comparison of fit indices of the seven- and nine-factor models is shown in Table 4.
Fig. 2.
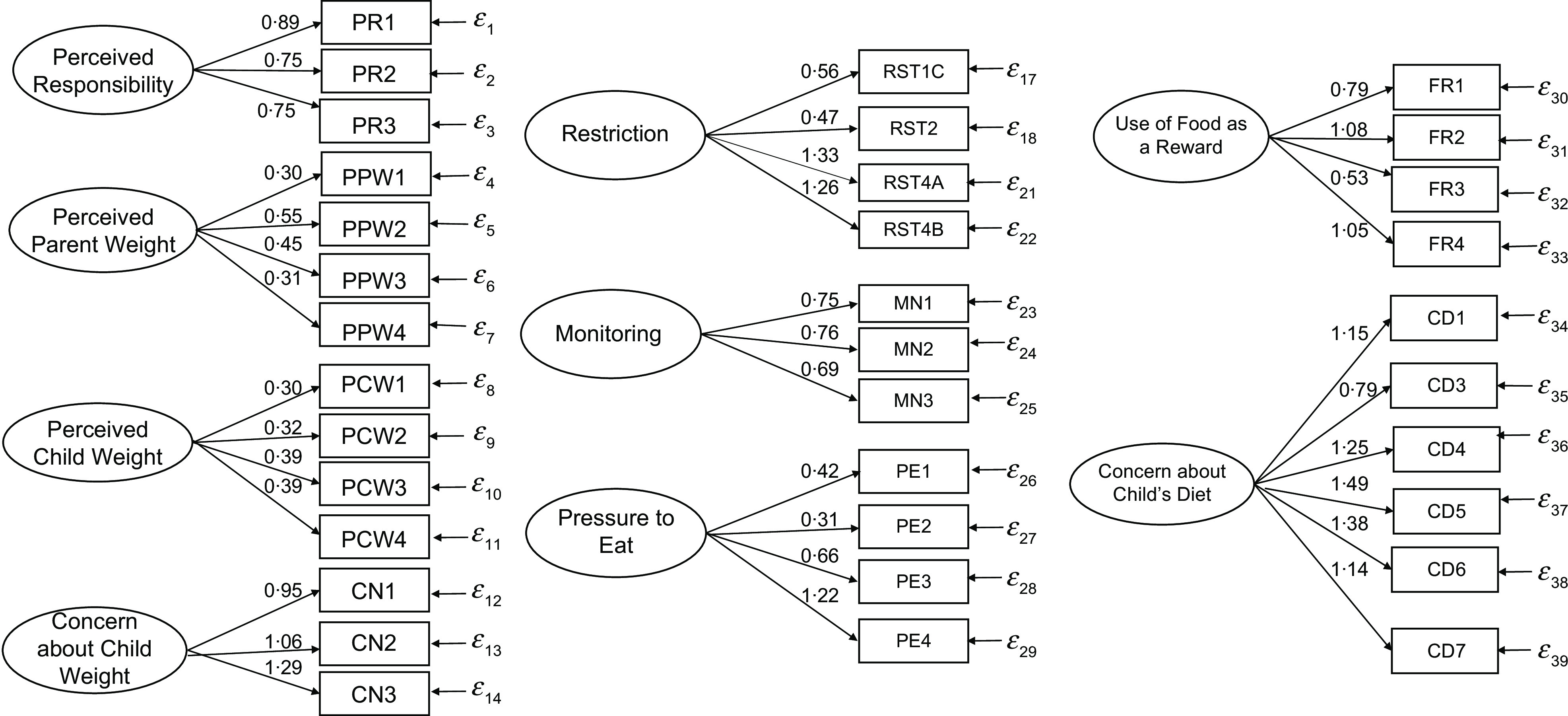
Nine-factor model of the Arabic version of the Child Feeding Questionnaire (CFQ-A), with the factors Perceived Responsibility, Perceived Parent Weight, Perceived Child Weight, Concern about Child Weight, Restriction, Monitoring, Pressure to Eat, Use of Food as Reward and Concern about Child’s Diet (see Table 1 for a description of the factors and subscales). Fit indices: root-mean-square error of approximation = 0·04 (95 % CI 0·03, 0·05), Tucker–Lewis index = 0·88, comparative fit index = 0·90, standardized root-mean-square residual = 0·07, χ2 = 694·0 (P < 0·001), minimum sample discrepancy function/df = 1·41 (ε1–ε18 and ε21–ε39 are error terms)
Table 4.
Comparison of fit indices between the seven-factor and nine-factor models of the Arabic version of the Child Feeding Questionnaire (CFQ-A) in the sample of pre-schoolers and their mothers (n 209) recruited from eight different pre-schools in Jeddah city, Kingdom of Saudi Arabia, October 2017–April 2018
| Model | CMIN/df | χ 2 | P value | TLI | CFI | SRMR | RMSEA | 95 % CI |
|---|---|---|---|---|---|---|---|---|
| Seven-factor | 1·10 | 256·7 | <0·001 | 096 | 0·97 | 0·07 | 0·02 | 0·00, 0·04 |
| Nine-factor | 1·41 | 694·0 | <0·001 | 0·89 | 0·90 | 0·07 | 0·04 | 0·03, 0·05 |
| Δχ² | – | 437·3 | – | – | – | – | – | – |
CMIN, minimum sample discrepancy function; χ2, chi-square statistic; TLI, Tucker–Lewis index; CFI, comparative fit index; SRMR, standardized-root-mean square residual; RMSEA, root-mean-square error of approximation.
Factor–factor and factor–child BMI Z-score correlations
As shown in Table 5, the highest correlations between factors were between Restriction and Monitoring (r = 0·50, P < 0·001), Perceived Responsibility and Monitoring (r = 0·40, P < 0·001) and Perceived Responsibility and Restriction (r = 0·30, P < 0·001). There were small positive correlations between Perceived Child Weight and Restriction (r = 0·20, P < 0·001) and Perceived Child Weight and Monitoring (r = 0·17, P = 0·01), as well as between Concern about Child’s Diet and Concern about Child Weight (r = 0·18, P < 0·001) and Concern about Child’s Diet and Use of Food as a Reward (r = 0·16, P = 0·01). Although marginally significant, Perceived Responsibility was also positively correlated with Perceived Child Weight (r = 0·13, P = 0·06) and Pressure to Eat (r = 0·12, P = 0·07).
Table 5.
Factor–factor and factor–child BMI Z-score (BMIZ) correlations of the modified nine-factor model of the Arabic version of the Child Feeding Questionnaire (CFQ-A), October 2017–April 2018
| Perceived Responsibility | Perceived Parent Weight | Perceived Child Weight | Concern about Child Weight | Restriction | Pressure to Eat | Monitoring | Use of Food as a Reward | Concern about Child’s Diet | Child BMIZ (n 207) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Perceived Responsibility | 1 | |||||||||
| Perceived Parent Weight | −0·02 | 1 | ||||||||
| Perceived Child Weight | 0·13* | 0·09 | 1 | |||||||
| Concern about Child Weight | −0·03 | 0·09 | 0·05 | 1 | ||||||
| Restriction | 0·30*** | 0·03 | 0·20*** | −0·009 | 1 | |||||
| Pressure to Eat | 0·12* | −0·12* | −0·20*** | −0·14** | 0·06 | 1 | ||||
| Monitoring | 0·40*** | −0·07 | 0·17** | −0·09 | 0·50*** | 0·08 | 1 | |||
| Use of Food as a Reward | −0·19*** | −0·12* | −0·009 | −0·07 | −0·03 | −0·03 | −0·09 | 1 | ||
| Concern about Child’s Diet | −0·24*** | −0·15** | −0·23*** | 0·18*** | −0·09 | −0·09 | −0·11* | 0·16** | 1 | |
| Child BMIZ (n 207) | 0·11* | 0·30*** | 0·49*** | 0·02 | 0·21*** | −0·12* | 0·16** | 0·05 | −0·18** | 1 |
n 209 unless otherwise specified.
*P < 0·10, **P < 0·05, ***P < 0·01.
We detected negative correlations between Perceived Responsibility and Concern about Child’s Diet (r = −0·24, P < 0·001) and between Perceived Responsibility and Use of Food as a Reward (r = −0·19, P < 0·001). Furthermore, Concern about Child’s Diet was negatively correlated with Perceived Parent Weight (r = −0·15, P = 0·03) and Perceived Child Weight (r = −0·23, P = 0·001). Concern about Child Weight was negatively correlated with Pressure to Eat (r = −0·14, P = 0·04).
There were significant correlations between child BMIZ and five out of the nine factors; Perceived Child Weight (r = 0·49, P < 0·001), Perceived Parent Weight (r = 0·30, P < 0·001), Restriction (r = 0·21, P < 0·001) and Monitoring (r = 0·16, P = 0·02) were each positively correlated with child BMIZ, while Concern about Child’s Diet was negatively correlated with child BMIZ (r = −0·18, P = 0·01; Table 5).
Discussion
Our study including 209 Saudi mothers and their pre-school children provides initial evidence of the validity and reliability of a modified nine-factor CFQ-A model. Our results suggest that modifying the restriction subscale and including a separate subscale to assess using food as a reward may be suitable for Saudi mothers. This approach has previously provided satisfactory results among a sample of Chinese mothers of pre-schoolers(33), suggesting that parenting/feeding strategies among Middle-Eastern and Asian families might be comparable. Indeed, when comparing our restriction factor mean with that of the study involving Chinese mothers(33) (total mean scores out of 5), we observed that they are almost similar (mean=4·40, sd = 0·94 and mean=4·18, sd = 0·80, respectively), whereas a larger difference is seen when comparing with Western samples of pre-school (mean = 2·72, sd=0·99)(10) and school-age children (mean = 2·50, sd=;0·95)(26). Likewise, perceived responsibility was higher among our Saudi mothers (mean = 4·23, sd = 0·93), as well as Chinese (mean = 4·26, sd = 0·71) and Turkish mothers (mean = 4·14, sd = 0·67), compared with US (mean = 3·40, sd = 0·95) and Swedish (mean = 4·02, sd = 0·69) mothers. Interestingly, monitoring among our sample of Saudi mothers (mean = 4·44, sd = 0·80) was noticeably higher than that of other samples of Chinese (mean = 3·68, sd = 1·12), Turkish (mean = 2·96, sd = 0·70), US (mean = 3·60, sd = 0·90) and Swedish (mean = 3·87, sd = 0·88) mothers. These cross-cultural similarities/differences might be attributed to societal norms regarding the role and responsibility of mothers in feeding their children, as well as availability and access to quality early childhood care centres (e.g. daycare centres and pre-schools), which affects the amount of time mothers spend being in charge of feeding their children.
Both the original seven-factor model as well as the modified nine-factor model showed good fit to data (root-mean-square error of approximation < 0·05)(52). Furthermore, our findings suggest adequate internal reliability for six out of the nine factors in the modified nine-factor CFQ-A model. The three factors with Cronbach’s α that fell below the 0·70 cut-off were: Perceived Parent Weight, Restriction, and Pressure to Eat. This is consistent with results from other validation studies that also found lower internal reliability for the Restriction and Pressure to Eat factors(10,27). One possible explanation for the less satisfactory estimates for the Restriction and Pressure to Eat subscales could be the variation between mothers in defining some phrases used in questionnaire items, such as ‘I have to be sure that my child does not eat too many high-fat foods’. For example, while one mother might define ‘being sure’ as actively or physically removing food items from the child’s reach, another might define this as more subtle behaviours such as stating the harms of high-fat foods in front of the child. In line with previous studies, ours showed evidence of adequate test–retest reliability(10).
Overall, intercorrelations between factors in the modified model were in the expected direction and give support to our hypothesis that perceived child weight and concern about child weight and diet are each associated with feeding practices among Saudi mothers. Results suggest that mothers who apply higher restriction may monitor their children’s eating to a greater extent. Mother who perceive that they are highly responsible for their children’s eating may apply greater restriction. Although the original CFQ study by Birch et al. did not find a correlation between perceived responsibility and restriction(26), our findings are consistent with those of a study involving Turkish mothers(53). In line with our findings, both the original CFQ study and the Turkish study reported a positive correlation between perceived responsibility and monitoring(26,53). Additionally, our findings suggest that mothers who perceive their children to have a higher weight status may apply higher restriction and monitoring, and mothers who are more concerned about their children’s weight may be more concerned about their diet.
Furthermore, we found that mothers who perceive that they are highly responsible for their children’s eating also reported lower concern about their child’s diet. This is probably due to these mothers exerting higher restriction and monitoring, leading them to feel more in control of what their children eat. Additionally, some of the Concern about Child’s Diet items were related to the child receiving ‘good nutrition’ and him/her having ‘poor eating habits’, which can be relevant to both underweight and overweight children. This might explain the negative correlation between Concern about Child’s Diet and Perceived Child Weight. Our results showed a negative correlation between Concern about Child Weight and Pressure to Eat, which is consistent with results from previous studies in Western samples(10,11,26).
Correlations detected between the modified CFQ-A factors and child BMIZ also give support to our hypothesis that maternal perceptions and practices around feeding are associated with child BMIZ in a sample of Saudi mothers and pre-schoolers. While some studies did not detect an association between restriction and child BMI(33,37) consistent with our results, others have reported a link with overeating and obesity risk(13,14,54). Furthermore, although only marginally significant, our finding of a negative correlation between pressure to eat and child BMIZ is consistent with those of previous studies(33,55) suggesting that mothers may pressure their children to eat more when they are thinner.
Since the present analyses did not take potential confounders into account, further studies that test adjusted statistical models are needed to further establish the association between maternal feeding behaviours and child BMI in a Saudi sample. Our findings, in addition to evidence from previous studies(25,36), suggest that Saudi mothers may feel great responsibility towards their role in feeding their families. Future studies that characterize feeding behaviours and examine associations with weight status are needed to help inform intervention studies aiming to enhance adaptive feeding practices and promote healthy eating behaviours among children in Saudi Arabia(56).
Our study was the first to evaluate validity and reliability of an Arabic version of the CFQ in a cohort residing in KSA. We were able to slightly modify the CFQ in order to better capture traditional feeding practices among Saudi mothers. Child anthropometry was objectively measured, and the sample was recruited from eight different pre-schools with varying degrees of socio-economic status. Limitations of the study included that our sample size was relatively small. Mothers were recruited through an opt-in approach by placing consent forms in children’s backpacks. This might have increased the likelihood of self-selection bias, such that mothers who were more interested in the topic of feeding might have been more inclined to participate. Administration of the questionnaire over the telephone might have increased the likelihood that mothers will give socially desirable responses, although this approach can help minimize missing data. Furthermore, since the majority of mothers in our study had a college degree or higher, our results may not be generalizable to other population groups with lower educational levels.
Future studies with larger sample sizes that include mothers with different educational backgrounds and studies that employ different recruitment strategies are warranted. Longitudinal designs are also needed in order to evaluate the effect of feeding behaviours over time and draw inferences regarding causal associations. Additionally, qualitative studies and those that include direct observation of mother–child interactions during mealtimes may be useful in identifying unique feeding behaviours among Saudi and Arab families.
Conclusion
Identifying characteristics of the mealtime environment and how they relate to child eating behaviours and weight status can help inform effective prevention and intervention strategies among Saudi families. Culturally sensitive assessment tools are needed in order to evaluate feeding behaviours among Saudi mothers. Our study provides evidence that supports the validity and reliability of the original seven-factor CFQ-A as well as a modified nine-factor CFQ-A model. Future larger studies are needed to further establish the psychometric properties of the CFQ-A as well as other feeding assessment tools.
Acknowledgements
Financial support: This project was funded by the Deanship of Scientific Research (DSR) at King Abdulaziz University, Jeddah (grant number J-734-142-38). The author acknowledges and thanks DSR for technical and financial support. Conflict of interest: The author has no financial relationships relevant to this article to disclose. Authorship: R.H.M. designed the study, oversaw data collection, analysed the data, wrote the manuscript and approved final the version as submitted. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Unit of Biomedical Ethics at King Abdulaziz University. Written informed consent was obtained from all participants.
References
- 1.GBD 2015 Obesity Collaborators (2017) Health effects of overweight and obesity in 195 countries over 25 years. New Engl J Med 377, 13–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Friedrich MJ (2017) Global obesity epidemic worsening. JAMA 318, 603. [DOI] [PubMed] [Google Scholar]
- 3.Cunningham SA, Kramer MR & Narayan KMV (2014) Incidence of childhood obesity in the United States. N Engl J Med 370, 403–411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Deckelbaum RJ & Williams CL (2001) Childhood obesity: the health issue. Obes Res 9, Suppl. 11, 239S–243S. [DOI] [PubMed] [Google Scholar]
- 5.Wardle J, Guthrie CA, Sanderson S et al. (2001) Development of the Children’s Eating Behaviour Questionnaire. J Child Psychol Psychiatry 42, 963–70. [DOI] [PubMed] [Google Scholar]
- 6.Faith M, Scanlon K, Birch L et al. (2004) Parent-child feeding strategies and their relationships to child eating and weight status. Obes Res 12, 1711–1722. [DOI] [PubMed] [Google Scholar]
- 7.Hughes S, Power T & Fisher J (2005) Revisiting a neglected construct: parenting styles in a child-feeding context. Appetite 44, 83–92. [DOI] [PubMed] [Google Scholar]
- 8.Ventura AK & Birch LL (2008) Does parenting affect children’s eating and weight status? Int J Behav Nutr Phys Act 5, 15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Byrne R, Jansen E & Daniels L (2017) Perceived fussy eating in Australian children at 14 months of age and subsequent use of maternal feeding practices at 2 years. Int J Behav Nutr Phys Act 14, 123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Nowicka P, Sorjonen K, Pietrobelli A et al. (2014) Parental feeding practices and associations with child weight status. Swedish validation of the Child Feeding Questionnaire finds parents of 4-year-olds less restrictive. Appetite 81, 232–241. [DOI] [PubMed] [Google Scholar]
- 11.Faith MS, Berkowitz RI, Stallings VA et al. (2004) Parental feeding attitudes and styles and child body mass index: prospective analysis of a gene–environment interaction Pediatrics 114, e429–e436. [DOI] [PubMed] [Google Scholar]
- 12.Johnson S & Birch L (1994) Parents’ and children’s adiposity and eating style. Pediatrics 94, 653–661. [PubMed] [Google Scholar]
- 13.Fisher J & Birch L (1999) Restricting access to foods and children’s eating. Appetite 32, 405–419. [DOI] [PubMed] [Google Scholar]
- 14.Fisher J & Birch L (2002) Eating in the absence of hunger and overweight in girls from 5 to 7 y of age. Am J Clin Nutr 76, 226–231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hughes SO, Shewchuk RM, Baskin ML et al. (2008) Indulgent feeding style and children’s weight status in preschool. J Dev Behav Pediatr 29, 403–410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lumeng JC, Kaciroti N, Retzloff L et al. (2017) Longitudinal associations between maternal feeding and overweight in low-income toddlers. Appetite 113, 23–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Garcia KS, Power TG, Beck AD et al. (2018) Stability in the feeding practices and styles of low-income mothers: questionnaire and observational analyses. Int J Behav Nutr Phys Act 15, 28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Haszard JJ, Russell CG, Byrne RA et al. (2019) Early maternal feeding practices: associations with overweight later in childhood Appetite 132, 91–96. [DOI] [PubMed] [Google Scholar]
- 19.Galindo L, Power TG, Beck AD et al. (2018) Predicting preschool children’s eating in the absence of hunger from maternal pressure to eat: a longitudinal study of low-income, Latina mothers. Appetite 120, 281–286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Al-Othaimeen AI, Al-Nozha M & Osman AK (2007) Obesity: an emerging problem in Saudi Arabia. Analysis of data from the National Nutrition Survey. East Mediterr Health J 13, 441–448. [PubMed] [Google Scholar]
- 21.El-Mouzan M, Foster P, Al-Herbish A et al. (2010) Prevalence of overweight and obesity in Saudi children and adolescents. Ann Saudi Med 30, 203–208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Sibai SAM, Nasreddine L, Mokdad AH et al. (2010) Nutrition transition and cardiovascular disease risk factors in Middle East and North Africa countries: reviewing the evidence. Ann Nutr Metab 57, 193–203. [DOI] [PubMed] [Google Scholar]
- 23.Ng SW, Zaghloul S, Ali H et al. (2011) Nutrition transition in the United Arab Emirates. Eur J Clin Nutr 65, 328–1337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Popkin BM (2006) Global nutrition dynamics: the world is shifting rapidly toward a diet linked with noncommunicable diseases. Am J Clin Nutr 84, 289–298. [DOI] [PubMed] [Google Scholar]
- 25.Almarhoon I, Ramsay S, Fletcher J et al. (2015) Saudi Arabian mothers’ child feeding practices, autonomy, and concern about child weight. J Food Nutr Diet 1, 103. [Google Scholar]
- 26.Birch LL, Fisher JO, Grimm-Thomas K et al. (2001) Confirmatory factor analysis of the Child Feeding Questionnaire: a measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite 36, 201–210. [DOI] [PubMed] [Google Scholar]
- 27.Boles RE, Nelson TD, Chamberlin LA et al. (2010) Confirmatory factor analysis of the Child Feeding Questionnaire among low-income African American families of preschool children. Appetite 54, 402–405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Anderson CB, Hughes SO, Fisher JO et al. (2005) Cross-cultural equivalence of feeding beliefs and practices: the psychometric properties of the Child Feeding Questionnaire among Blacks and Hispanics. Prev Med 41, 521–531. [DOI] [PubMed] [Google Scholar]
- 29.Geng G, Zhu Z, Suzuki K et al. (2009) Confirmatory factor analysis of the Child Feeding Questionnaire (CFQ) in Japanese elementary school children. Appetite 52, 8–14. [DOI] [PubMed] [Google Scholar]
- 30.Corsini N, Danthiir V, Kettler L et al. (2008) Factor structure and psychometric properties of the Child Feeding Questionnaire in Australian preschool children. Appetite 51, 474–481. [DOI] [PubMed] [Google Scholar]
- 31.Musher-Eizenman D & Holub S (2007) Comprehensive Feeding Practices Questionnaire: validation of a new measure of parental feeding practices. J Pediatr Psychol 32, 960–972. [DOI] [PubMed] [Google Scholar]
- 32.Kaur H, Li C, Nazir N et al. (2006) Confirmatory factor analysis of the child-feeding questionnaire among parents of adolescents. Appetite 47, 36–45. [DOI] [PubMed] [Google Scholar]
- 33.Liu WH, Mallan KM, Mihrshahi S et al. (2014) Feeding beliefs and practices of Chinese immigrant mothers. Validation of a modified version of the Child Feeding Questionnaire. Appetite 80, 55–60. [DOI] [PubMed] [Google Scholar]
- 34.Camcı N, Bas M & Buyukkaragoz AH (2014) The psychometric properties of the Child Feeding Questionnaire (CFQ) in Turkey. Appetite 78, 49–54. [DOI] [PubMed] [Google Scholar]
- 35.Al-Hussyeen AA & Al-Sadhan SA (2006) Oral hygiene practices and dietary habits among children with Down’s syndrome in Riyadh, Saudi Arabia. Saudi Dent J 18, 141–148. [Google Scholar]
- 36.Mosli RH, Bakhsh JA, Madani NA et al. (2019) Indulgence and stress around feeding: initial evidence from a qualitative study of Saudi mothers. Appetite 138, 242–251. [DOI] [PubMed] [Google Scholar]
- 37.Gregory JE, Paxton SJ & Brozovic AM (2010) Pressure to eat and restriction are associated with child eating behaviours and maternal concern about child weight, but not child body mass index, in 2-to 4-year-old children. Appetite 54, 550–556. [DOI] [PubMed] [Google Scholar]
- 38.Cramer JA, Perrine K, Devinsky O et al. (1998) Development and cross-cultural translations of a 31-item quality of life in epilepsy inventory. Epilepsia 39, 81–88. [DOI] [PubMed] [Google Scholar]
- 39.Anderson SE, Must A, Curtin C et al. (2012) Meals in our household: reliability and initial validation of a questionnaire to assess child mealtime behaviors and family mealtime environments. J Acad Nutr Diet 112, 276–284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Mosli RH, Miller AL, Peterson KE et al. (2016) Birth order and sibship composition as predictors of overweight or obesity among low-income 4- to 8-year-old children. Pediatr Obes 11, 40–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Onis MD, Onyango AW, Borghi E et al. (2007) Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ 85, 660–667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.World Health Organization (2006) WHO Child Growth Standards: Length/Height for Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age, Methods and Development. Geneva: WHO. [Google Scholar]
- 43.DeVellis RF (2003) Scale Development: Theory and Applications, 2nd ed. Thousand Oaks, CA: SAGE Publications, Inc. [Google Scholar]
- 44.Kline RB (2005) Principles and Practice of Structural Equation Modeling, 2nd ed. New York: Guilford Press. [Google Scholar]
- 45.Rosseel Y (2012) lavaan: an R package for structural equation modeling. J Stat Softw 48, issue 2, 1–36. [Google Scholar]
- 46.Li CH (2016) Confirmatory factor analysis with ordinal data: comparing robust maximum likelihood and diagonally weighted least squares. Behav Res Methods 48, 936–949. [DOI] [PubMed] [Google Scholar]
- 47.Lin CY, Pakpour AH, Broström A et al. (2018) Psychometric properties of the 9-item European Heart Failure Self-Care Behavior Scale using confirmatory factor analysis and Rasch analysis among Iranian patients. J Cardiovasc Nurs 33, 281–288. [DOI] [PubMed] [Google Scholar]
- 48.Cole DA (1987) Utility of confirmatory factor analysis in test validation research. J Consult Clin Psychol 55, 584–594. [DOI] [PubMed] [Google Scholar]
- 49.Hoelter JW (1983) The analysis of covariance structures: goodness-of-fit indices. Sociol Methods Res 11, 325–344. [Google Scholar]
- 50.Cohen J (1998) Statistical Power Analysis for the Behavioral Sciences. Hillsdale, NJ: Lawrence Erlbaum. [Google Scholar]
- 51.MacCallum RC, Browne MW & Sugawara HM (1996) Power analysis and determination of sample size for covariance structure modeling. Psychol Meth 1, 130–149. [Google Scholar]
- 52.Browne MW & Cudeck R (1993) Alternate ways of assessing model fit. In Testing Structural Equation Models, pp. 136–162 [Bollen KA and Long JS, editors]. Newbury Park, CA: SAGE Publications, Inc. [Google Scholar]
- 53.Polat S & Erci B (2010) Psychometric properties of the child feeding scale in Turkish mothers. Asian Nurs Res 4, 111–121. [DOI] [PubMed] [Google Scholar]
- 54.Farrow C, Haycraft E & Blissett J (2018) Observing maternal restriction of food with 3–5-year-old children: relationships with temperament and later body mass index (BMI). Int J Environ Res Public Health 15, 1273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.de Souza Rezende P, Bellotto de Moraes DE, Mais LA et al. (2019) Maternal pressure to eat: associations with maternal and child characteristics among 2- to 8-year-olds in Brazil. Appetite 133, 40–46. [DOI] [PubMed] [Google Scholar]
- 56.Patrick H, Nicklas TA, Hughes SO et al. (2005) The benefits of authoritative feeding style: caregiver feeding styles and children’s food consumption patterns. Appetite 44, 243–249. [DOI] [PubMed] [Google Scholar]