

Abstract
Epilepsy neuroimaging assessment requires exceptional anatomic detail, physiologic and metabolic information. Magnetic resonance (MR) protocols are often time-consuming necessitating sedation and positron emission tomography (PET)/computed tomography (CT) comes with a significant radiation dose. Hybrid PET/MRI protocols allow for exquisite assessment of brain anatomy and structural abnormalities, in addition to metabolic information in a single, convenient imaging session, which limits radiation dose, sedation time, and sedation events. Brain PET/MRI has proven especially useful for accurate localization of epileptogenic zones in pediatric seizure cases, providing critical additional information and guiding surgical decision making in medically refractory cases. Accurate localization of seizure focus is necessary to limit the extent of the surgical resection, preserve healthy brain tissue, and achieve seizure control. This review provides a systematic overview with illustrative examples demonstrating the applications and diagnostic utility of PET/MRI in pediatric epilepsy.
Keywords: hybrid imaging, PET/MRI, pediatric epilepsy, malformations of cortical development, focal cortical dysplasia, temporal lobe epilepsy, mesial temporal sclerosis, tuberous sclerosis
Introduction
Epilepsy is a common chronic neurologic condition in childhood, affecting 0.5 to 1% of children. 1 Drug-resistant epilepsy occur in approximately 25% of pediatric patients. 2 3 Meanwhile, surgical treatment is effective but invasive and requires careful preoperative planning. 4 5 6 A multidisciplinary and multimodal imaging approach with functional PET and anatomical MRI components is necessary to accurately localize epileptogenic foci and limit extent of surgical resection and thus postoperative physical and neuropsychological deficits. 7 A diagnostic algorithm for pediatric epilepsy should ideally include semiology, interictal and ictal positron emission tomography (PET), and invasive monitoring such as stereoelectroencephalography (SEEG) or placement of surface subdural grids to guide a targeted anatomic and metabolic review for overlooked subtle abnormalities. Although invasive, SEEG is considered the gold standard for spatiotemporal definition of seizure-onset zone in the ictal period.
18 F-fluorodeoxyglucose (FDG) is the most common PET radiotracer used in clinical assessment of epilepsy patients, and in one survey, 18 F-FDG-PET was shown to provide critical additional information on the localization of epileptogenic zone in 77% of cases and guide surgical decision making in 51% of cases. 8 Epileptogenic zones are characterized by focal hypometabolism on 18 F-FDG brain PET. Hypometabolism associated with an underlying structural abnormality, such as malformations of cortical development (MCD), may be greater than the size of the lesion identified by structural imaging and the epileptogenic zone defined by invasive monitoring. 9 10 For example, Fig. 1 demonstrates a rare form of band heterotopia, 11 which was challenging to detect on magnetic resonance imaging (MRI) but much more conspicuous on PET imaging. Interictal 18 F-FDG-PET is more sensitive than MRI in localizing epileptogenic seizure nidus in both temporal lobe and extra-temporal epilepsy and may successfully identify MCD despite negative MRI. 12 13 Notably, a recent study investigated regional metabolic rate of glucose (MRGlc) derived from the analysis of FDG PET and MRI data. The authors found that MRGlc abnormality maps contributed to the localization of hypo-metabolic areas in 53% of cases when comparing patients with non-lesional extratemporal epilepsy to a normative database, but the overall quantitative PET imaging was only found to have a moderate impact on clinical management. 14
Fig. 1.
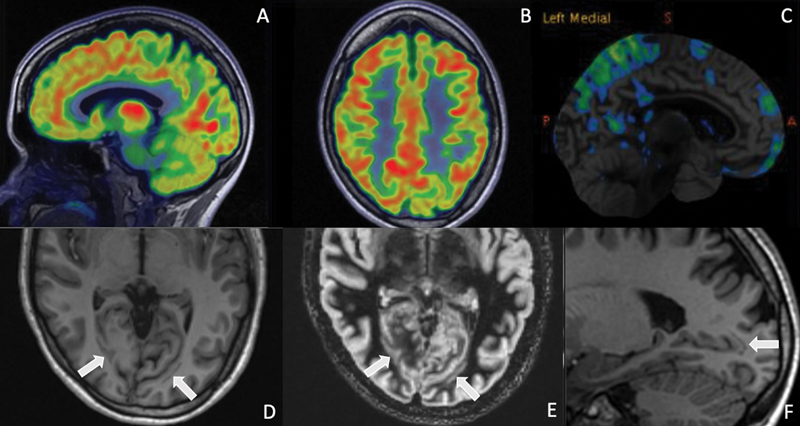
18 F-FDG-PET ( A, B ) and automated voxel by voxel z-score database map (Cortex ID, GE Healthcare) ( C ) shows focal areas of hypometabolism in the parietal and occipital lobes, more pronounced on the left side, which resulted in focused review of corresponding MRI. Focal hypometabolism corresponds to gray matter bands adjacent to the occipital horns of the lateral ventricles on the MPRAGE and DIR sequences ( D–F ), which were isointense to cortex on all sequences, and compatible with band heterotopia.
More recently, epileptogenic alterations in the central diazepine receptor system have been used in the localization of epileptogenic foci by utilizing the 11 C-flumazenil (FMZ) radiotracer, which has high affinity for GABA A receptors. 11 C-FMZ PET demonstrates interictal decreased binding in the seizure-onset zone and may provide valuable information to complement MRI and FDG-PET in presurgical evaluation. 15 The major limitation is the very short half-life of 11 C (approximately 20 minutes), which limits the use primarily to the research setting and institutions with an on-site cyclotron. 11 C-alpha-methyl-L-tryptophan (AMT) is a tryptophan analog that traces serotonin metabolism and demonstrates increased interictal activity in the epileptogenic cortex. 11 C-AMT PET has shown promise in patients with tuberous sclerosis and MCD due to specificity approaching 100% and smaller area of abnormality compared to FDG or FMZ PET. 16 AMT-PET does not require EEG monitoring and performs well even in the setting of partial volume artifacts caused by focal atrophy in the epileptogenic region. Similar to FMZ PET, it currently has limited clinical utility.
Neuroinflammation has also been implicated in epileptogenesis. PET radioligands include translocator protein (TSPO) tracers. TSPO is an 18-kDa protein found on the outer mitochondrial membrane of activated microglia and astrocytes, and therefore considered a tissue-specific biomarker of inflammation. The majority of the data supporting TSPO as a potential target for anti-inflammatory treatment in epilepsy are either preclinical or from limited clinical studies, and it is still not clear if TSPO is a more composite measurement of neuroinflammation or if it is specific enough to warrant targeted therapy. 17
Perfusion imaging for epilepsy using 15 O-H 2 O PET has not gained widespread popularity given discordance and low diagnostic accuracy between perfusion and metabolic abnormalities in epileptogenic zones. 18 Various additional radioligands are also being evaluated in epilepsy, including ligands targeted for opioid receptors, histamine receptors, N-methyl-D-aspartate (NMDA) receptors, and acetylcholine receptors, aiming to provide more specific imaging guidance to improve results following surgical intervention.
Brain PET traditionally uses CT for attenuation correction and anatomic correlation. The inherent tissue contrast resolution associated with CT is suboptimal for the evaluation of structural abnormalities related to epilepsy; therefore, necessitating a separately performed brain MRI. Hybrid PET/MRI has become increasingly more common and enables improved accuracy of brain PET and MR image fusion, however, not without some pitfalls. Attenuation correction of brain PET data from PET/MRI uses advanced image-processing techniques and is the most commonly performed with an atlas-based approach, relying on a previously compiled atlas of paired MRI and CT exams to perform a pseudo-CT from the patient's MRI for subsequent attenuation correction, as opposed to utilizing direct information from the patient. Direct attenuation correction can also be performed with MRI using dixon, ultra-short echo, or zero-echo time sequences. In a cohort of children with focal epilepsy, the diagnostic accuracy of PET/MRI was not inferior to PET/CT for seizure focus localization. 19 A more recent study comparing PET/MRI with PET/CT and standalone MRI showed that diagnostic accuracy and image quality as determined by visual score were the highest in PET/MRI. 20
Hybrid PET/MRI can be obtained with synchronous or sequential systems. A sequential system is based upon patient transportation between PET and MRI scans, which are performed separately. The sequential system is clinically easier to implement because most hospitals own separate PET and MRI scanners. A major drawback is the asynchronous acquisition of the scans, which results in a longer scan and sedation time and misregistration artifacts. A synchronous system is technically more difficult to achieve but preferable in pediatric patients 21 because the solid-state PET detectors are located between the MRI body and gradient coils in one integrated machine, which allows for truly synchronous image acquisition with reduced scan and sedation time, and reduced risk of misregistration artifact. 22 23 Synchronous acquisition also ensures that both scans are obtained at the same time with regard to seizure occurrence given that dis-synchronous assessment may be misleading if scans are obtained distant in time from each other. As outlined in the 2019 consensus report from the International League Against Epilepsy Neuroimaging Task Force, 24 epilepsy protocols benefit from the inclusion of 3D volumetric T1-weighted imaging, axial and coronal T2-weighted images FSE or TSE, axial and coronal FLAIR sequences, and axial T2* gradient echo or SWI sequences. Oblique coronal T2-weighted images of the hippocampus, DWI/DTI, and ADC maps may also prove valuable. Gadolinium-enhanced images are not routinely indicated and reserved for cases with suspected infection, vascular abnormality, or tumors. Furthermore, higher field strength magnets such as 3- or 7-Tesla (T), provide better lesion detection and contrast resolution compared to 1.5 T magnets. For example, in one study, 15 out of 23 patients with medically refractory epilepsy and a normal 1.5 T brain MRI interpreted at a tertiary care center, had abnormal findings on 3T imaging. 25
Additional advanced neuroimaging modalities such as functional MRI (fMRI), single-photon emission computerized tomography (SPECT), magnetic resonance spectroscopy (MRS), and magnetoencephalography (MEG) may also be utilized in preoperative planning. 26 27 28 29 30 31 32 33 Functional MRI with simultaneous EEG monitoring can be helpful for the localization of epileptogenic foci as interictal epileptic discharges may show corresponding BOLD response on fMRI. Resting state functional MRI (rs-fMRI) has shown promise 26 in determining seizure-onset localization in nearly 90% of cases and altered surgery in almost 60% of cases in one single institution series. 27 Fiber-tracking techniques can advantageously be obtained for temporal lobe epilepsy, which allows the evaluation of reorganization of linguistic and associated functions. 28 29 Diffusion tensor imaging (DTI) can be used for preoperative evaluation of lateralization of motor cortex and delineation of corticospinal tracts, and has been shown helpful to predict postoperative motor outcomes. 30 DTI may also prove helpful in patients who fail to obtain seizure freedom after hemispherectomy by identifying transcallosal fibers responsible for residual interhemispheric connections. These patients may benefit from additional surgery. 31 Similar to FDG-PET, SPECT allows quantitative and qualitative assessments of cerebral blood flow, which is regionally increased in the ictal state and decreased interictally. A combination of interictal and ictal SPECT by statistical parametric mapping has been shown to help localize seizure foci, particularly in temporal lobe epilepsy. 32 In subtraction SPECT, the interictal SPECT is subtracted from the ictal SPECT and then co-registered with MRI to increase the accuracy of SPECT. 33 Challenges in SPECT imaging include identification of clinical onset of seizures for ictal imaging and larger anatomic areas of hyper perfusion compared to MRI and EEG findings.
Focal Cortical Dysplasia
Focal cortical dysplasia (FCD) is the most common MCD in pediatric medically refractory epilepsy and the most frequent histopathologic diagnosis in children undergoing epilepsy surgery. 34 35 FCD may present with blurring of the gray–white matter junction ( Fig. 2 ), cortical thickening ( Fig. 3 ), hyperintense T2/FLAIR signal of gray or white matter, transmantle sign ( Fig. 2 ), segmental or lobar atrophy or hypoplasia, and abnormal sulcal or gyral pattern. MRI is the main diagnostic modality in evaluation although some cases reveal very little to no apparent abnormality. In a study of 48 children, 18 F-FDG-PET demonstrated an advantage over MRI alone, with a sensitivity of 87% for FDG-PET versus 77% for MRI alone. 36 With hybrid imaging, the sensitivity of 18 F-FDG-PET can be increased by co-registration of color-coded PET images with MRI, which improves the detection of morphologic abnormalities such as FCD type I, with up to 82% of patients seizure-free after resection guided by PET/MR findings and electrocorticography. 13 36 Notably, 18 F-FDG-PET detects areas of hypometabolism in 60 to 92% of epilepsy patients with FCD. 37
Fig. 2.
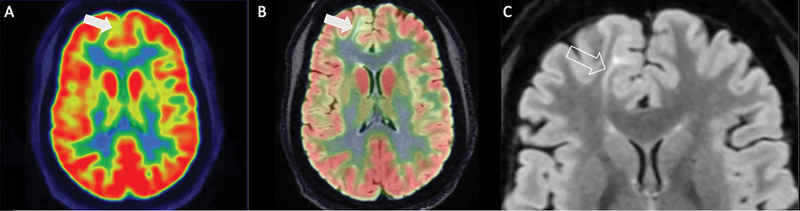
Focal hypometabolism along the medial right frontal lobe ( A ) corresponds to underlying cortical and subcortical irregularity on fused FLAIR PET/MRI sequence ( B ) with gray–white junction blurring, hyperintense T2 signal and positive transmantle sign, best defined on FLAIR sequence ( C ).
Fig. 3.
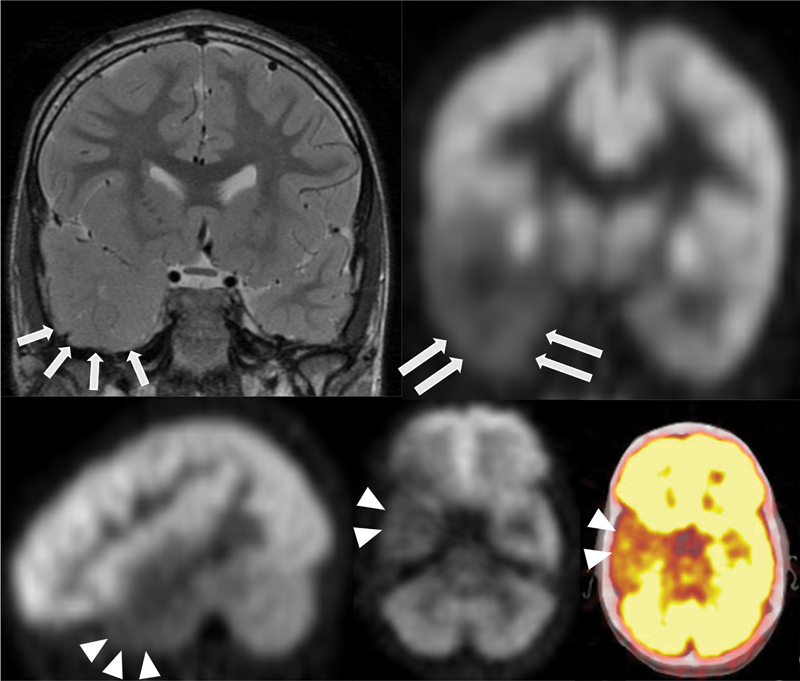
Brain MRI in patient with focal cortical dysplasia visualized as abnormal cortical thickening and effacement of white matter in the right temporal pole, best visualized on thin coronal T2-weighted MRI ( arrows , A ). On 18 F-FDG-PET ( arrows and arrowheads , B–D ) and fused axial 18 F-FDG PET/CT ( arrowheads , E ), there is corresponding hypometabolism in the right anterior temporal lobe.
In the absence of a focal lesion on MRI and surface EEG without localizing information, children undergoing presurgical evaluation may undergo 18 F-FDG-PET to obtain lateralizing and localizing information regarding epileptogenic cortex. 38 39 Identification of an epileptogenic zone and underlying lesion allows for surgical resection and increases the probability of seizure freedom. 40 Localized 18 F-FDG-PET abnormalities were reported in 84% of cases in a surgical series with patients with temporal lobe epilepsy and negative MRI. 41
Pediatric Temporal Lobe Epilepsy
Temporal lobe epilepsy (TLE) is the most common medically intractable epilepsy in adults, with mesial temporal sclerosis (MTS) as the underlying cause in approximately 60% of cases. Tumor, MCD, trauma, nonspecific gliosis, and vascular malformations are less frequent etiologies. 6 42 43 Contrarily, only about 20% of pediatric patients have TLE, and only 20% of these children have MTS ( Fig. 4 ). 44 In the adult literature, there has been recognition of MRI-negative, 18 F-FDG-PET-positive TLE, with surgical seizure outcomes comparable to MRI-positive patients with mesial temporal sclerosis. 43 45
Fig. 4.
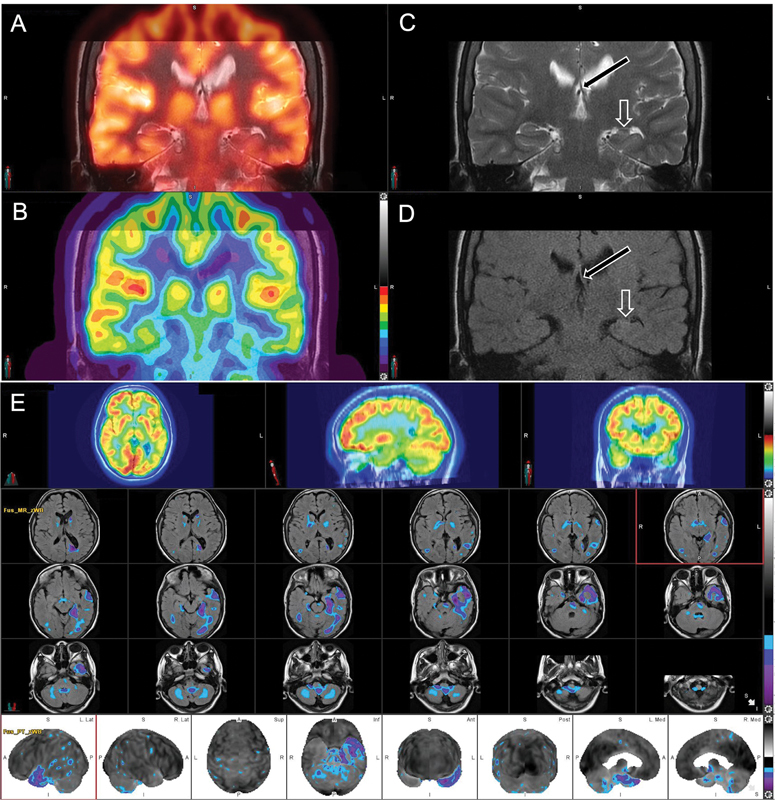
A 11-year-old male patient with medically refractory epilepsy. EEG demonstrated left temporal lobe seizure focus. Fused 18 F-FDG PET/MRI ( A, B ), coronal T2 and FLAIR ( C, D ) views demonstrate focal hypometabolism in the left temporal pole involving the left hippocampal formation, entorhinal cortex, and amygdala. There is decreased volume of the left hippocampal formation ( open arrow ) with abnormal morphology and subtle T2/FLAIR hyperintensity, and with associated decreased caliber of the left fornix ( black arrow ) and smaller size of the left mamillary body (not shown). Semiquantitative analysis using Z scores calculated in comparison to age-matched normal controls ( E ) reveals significantly decreased values in the left temporal lobe including in the left temporal pole, hippocampus, parahippocampal gyrus, and amygdala.
Reports demonstrate MCD as a common underlying histopathology in pediatric patients with pure temporal lobe epilepsy, with a predominance of type 1B and 2A focal cortical dysplasia. 46 It is important to keep in mind that many patients with pediatric TLE actually have temporal plus nosology. While detection of a lesion on MRI remains an important preoperative determinant of long-term seizure freedom following pediatric temporal lobectomy, 18 F-FDG-PET has proven invaluable in the workup of pediatric patients with refractory epilepsy.
Tuberous Sclerosis
Epilepsy develops in 80 to 90% of tuberous sclerosis patients, in some as early as infancy, and approximately 25 to 50% of TSC patients may develop medically intractable epilepsy. 44 47 Intractable seizures can have a detrimental effect on neurocognitive development and early epilepsy surgery may be beneficial. 48 Cortical tubers are typically seen as multifocal areas of glucose hypometabolism, which is hypothesized to be due to decreased number of neurons and simplified dendritic pattern within the tubers with less requirement for glucose. The area of hypometabolism is often larger than the lesions seen on MRI. 49 50 Structural imaging typically demonstrates multiple bilateral subcortical tubers, but seizures often arise primarily from a single tuber. 51 Multimodality imaging algorithms utilizing MRI and 18 F-FDG-PET co-registration can play a valuable role by noninvasively localizing epileptogenic tubers during pre-surgical evaluation. 52 Notably, AMT-PET is unique because it can differentiate epileptogenic from non-epileptogenic tubers, which is helpful to guide surgery. 15 49 Surgical outcome studies demonstrate decrease in seizure burden after resection of the suspected epileptogenic tubers while leaving the non-epileptogenic tubers untouched. 53 54 Fig. 5 shows a case of tuberous sclerosis with multiple hypometabolic cortical tubers, which was managed non-surgically.
Fig. 5.
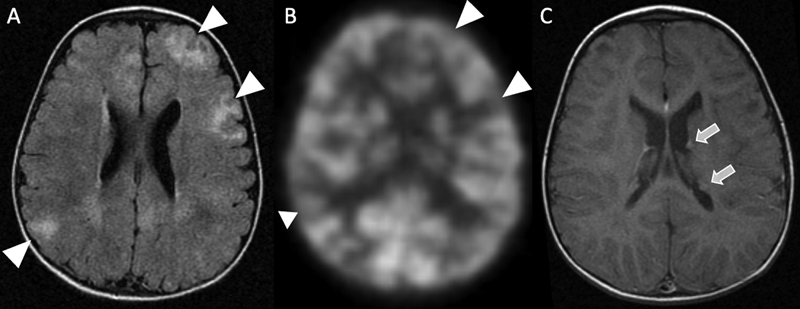
Brain MRI in a patient with tuberous sclerosis demonstrates multiple FLAIR hyperintense cortical tubers ( arrowheads , A ). The regions of the tubers appear to be hypometabolic on corresponding 18 F-FDG-PET ( arrowheads , B ). There are small enhancing subependymal nodules ( arrows ) along the left lateral ventricle, which are consistent with diagnosis of TS ( C ).
Hemispheric Abnormalities
18 F-FDG-PET is beneficial in evaluating patients with hemispheric abnormalities, including encephalomalacia, Rasmussen's encephalitis, and diffuse MCD. 55 These patients may develop intractable epilepsy and undergo evaluation for hemispherectomy, which is an effective surgical approach in children with multilobar or hemispheric epileptogenic lesions. In these cases, published large-sample studies report a rate of seizure remission of 65 to 80%. 56 18 F-FDG-PET often demonstrates diffuse hypometabolism affecting the involved hemisphere. However, patients with bilateral 18 F-FDG-PET abnormalities have unfavorable seizure outcomes following hemispherectomy, emphasizing the benefits of 18 F-FDG-PET in pre-surgical assessment. 57 Fig. 6 shows a case of N-methyl-D-aspartate (NMDA) encephalitis, which may be associated with extra-cerebral malignancy. 58
Fig. 6.
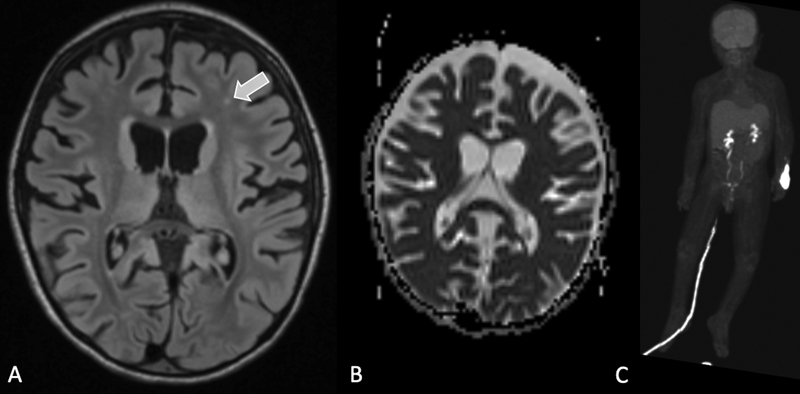
A 3-year-old child with refractory status epilepticus. MRI brain demonstrates parenchymal volume loss and white matter FLAIR hyperintense foci ( A, B ). Extensive laboratory testing was negative for arbovirus, AQP4 antibody, myelin oligodendrocyte glycoprotein, and SARS CoV-2. N-methyl-D-Aspartate IgG antibodies were detected. Subsequent 18 F-FDG-PET was performed to identify primary malignancy, which was negative ( C ).
Conclusion
Diagnosis and treatment of pediatric epilepsy are complicated and requires a multidisciplinary and multimodal imaging approach. Accurate localization of a seizure focus is paramount for optimal treatment and favorable outcomes following surgical resection. Hybrid brain 18 F-FDG PET/MRI is an optimized imaging approach that allows for comprehensive multimodal imaging evaluation with reduction in radiation dose, sedation events, and sedation time.
Footnotes
Conflicts of Interest Heike Daldrup-Link reported below details:
Grants or contracts from any entity: R01AR054458 (PI), R01HD081123 (PI), R21AR075863 (PI), R21HD103638 (PI), U24CA264298 (Co-PI), P30CA124435 (Key personnel)
Andrew McDonough B+ Foundation
ReMission Alliance
Sarcoma Foundation of America.
Royalties or licenses: US20130344003, WO2015014756, WO2018217943
Monasteria Press LLC
Patents: US20130344003, WO2015014756, WO2018217943.
Participation on a Data Safety Monitoring Board or Advisory Board:
External advisory board member, R24OD019813-01
Advisory board member, Stanford Cancer Imaging T32 Training Program, 5 T T32 Act CA009695 Project 29
Advisory Board, The Lancet Hematology
Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid:
Member, Editorial Board, Nanotheranostics
Member, Editorial Board, Journal of Nuclear Medicine
Associate Editor, Radiology: Imaging Cancer
Co-Program Director, Mentoring to AdVance womEN in Science (MAVENS) program, Stanford School of Medicine,
Associate Chair for Diversity, Department of Radiology, Stanford School of Medicine
Co-Director, Cancer Imaging & Early Detection Program, Stanford Cancer Institute, 5P30CA124435-10
Board Member, SPR Research Foundation, Society for Pediatric Radiology (SPR)
Member, Noninterpretive Skills and Practice Management Committee, Annual Meeting of the Radiological Society of North America (RSNA)
Awards Committee, World Molecular Imaging Society (WMIS)
Ana Franceschi reported:
Grants or contracts from any entity: Foundation of the ASNR Boerger Grant.
Consulting fees: Biogen, Life Molecular Imaging, Genentech.
Leadership or fiduciary role in other board: Chair, ACR Neuroradiology Commission Dementia Workgroup.
All other authors reported no conflict of interest.
References
- 1.Aaberg K M, Gunnes N, Bakken I J. Incidence and prevalence of childhood epilepsy: a nationwide cohort study. Pediatrics. 2017;139(05):e20163908. doi: 10.1542/peds.2016-3908. [DOI] [PubMed] [Google Scholar]
- 2.Fine A, Wirrell E C. Seizures in children. Pediatr Rev. 2020;41(07):321–347. doi: 10.1542/pir.2019-0134. [DOI] [PubMed] [Google Scholar]
- 3.Sultana B, Panzini M A, Veilleux Carpentier A. Incidence and prevalence of drug-resistant epilepsy: a systematic review and meta-analysis. Neurology. 2021;96(17):805–817. doi: 10.1212/WNL.0000000000011839. [DOI] [PubMed] [Google Scholar]
- 4.Engel J., Jr The current place of epilepsy surgery. Curr Opin Neurol. 2018;31(02):192–197. doi: 10.1097/WCO.0000000000000528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dwivedi R, Ramanujam B, Chandra P S. Surgery for drug-resistant epilepsy in children. N Engl J Med. 2017;377(17):1639–1647. doi: 10.1056/NEJMoa1615335. [DOI] [PubMed] [Google Scholar]
- 6.Duchowny M, Levin B, Jayakar P. Temporal lobectomy in early childhood. Epilepsia. 1992;33(02):298–303. doi: 10.1111/j.1528-1157.1992.tb02319.x. [DOI] [PubMed] [Google Scholar]
- 7.Hyslop A, Miller I, Bhatia S, Resnick T, Duchowny M, Jayakar P. Minimally resective epilepsy surgery in MRI-negative children. Epileptic Disord. 2015;17(03):263–274. doi: 10.1684/epd.2015.0766. [DOI] [PubMed] [Google Scholar]
- 8.Ollenberger G P, Byrne A J, Berlangieri S U. Assessment of the role of FDG PET in the diagnosis and management of children with refractory epilepsy. Eur J Nucl Med Mol Imaging. 2005;32(11):1311–1316. doi: 10.1007/s00259-005-1844-6. [DOI] [PubMed] [Google Scholar]
- 9.Koepp M J, Woermann F G. Imaging structure and function in refractory focal epilepsy. Lancet Neurol. 2005;4(01):42–53. doi: 10.1016/S1474-4422(04)00965-2. [DOI] [PubMed] [Google Scholar]
- 10.Lagarde S, Boucekine M, McGonigal A. Relationship between PET metabolism and SEEG epileptogenicity in focal lesional epilepsy. Eur J Nucl Med Mol Imaging. 2020;47(13):3130–3142. doi: 10.1007/s00259-020-04791-1. [DOI] [PubMed] [Google Scholar]
- 11.D'Agostino M D, Bernasconi A, Das S.Subcortical band heterotopia (SBH) in males: clinical, imaging and genetic findings in comparison with females Brain 2002125(Pt 11):2507–2522. 10.1093/brain/awf248 [DOI] [PubMed] [Google Scholar]
- 12.Rubí S, Setoain X, Donaire A. Validation of FDG-PET/MRI coregistration in nonlesional refractory childhood epilepsy. Epilepsia. 2011;52(12):2216–2224. doi: 10.1111/j.1528-1167.2011.03295.x. [DOI] [PubMed] [Google Scholar]
- 13.Salamon N, Kung J, Shaw S J. FDG-PET/MRI coregistration improves detection of cortical dysplasia in patients with epilepsy. Neurology. 2008;71(20):1594–1601. doi: 10.1212/01.wnl.0000334752.41807.2f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Traub-Weidinger T, Muzik O, Sundar L KS. Utility of absolute quantification in non-lesional extratemporal lobe epilepsy using FDG PET/MR imaging. Front Neurol. 2020;11:54. doi: 10.3389/fneur.2020.00054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ryvlin P, Bouvard S, Le Bars D.Clinical utility of flumazenil-PET versus [18F]fluorodeoxyglucose-PET and MRI in refractory partial epilepsy. A prospective study in 100 patients Brain 1998121(Pt 11):2067–2081. 10.1093/brain/121.11.2067 [DOI] [PubMed] [Google Scholar]
- 16.Kumar A, Asano E, Chugani H T. α-[ 11 C]-methyl-L-tryptophan PET for tracer localization of epileptogenic brain regions: clinical studies . Biomarkers Med. 2011;5(05):577–584. doi: 10.2217/bmm.11.68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bouilleret V, Dedeurwaerdere S. What value can TSPO PET bring for epilepsy treatment? Eur J Nucl Med Mol Imaging. 2021;49(01):221–233. doi: 10.1007/s00259-021-05449-2. [DOI] [PubMed] [Google Scholar]
- 18.Lee D S, Lee J S, Kang K W. Disparity of perfusion and glucose metabolism of epileptogenic zones in temporal lobe epilepsy demonstrated by SPM/SPAM analysis on 15O water PET, [18F]FDG-PET, and [99mTc]-HMPAO SPECT. Epilepsia. 2001;42(12):1515–1522. doi: 10.1046/j.1528-1157.2001.21801.x. [DOI] [PubMed] [Google Scholar]
- 19.Paldino M J, Yang E, Jones J Y. Comparison of the diagnostic accuracy of PET/MRI to PET/CT-acquired FDG brain exams for seizure focus detection: a prospective study. Pediatr Radiol. 2017;47(11):1500–1507. doi: 10.1007/s00247-017-3888-8. [DOI] [PubMed] [Google Scholar]
- 20.Kikuchi K, Togao O, Yamashita K. Diagnostic accuracy for the epileptogenic zone detection in focal epilepsy could be higher in FDG-PET/MRI than in FDG-PET/CT. Eur Radiol. 2021;31(05):2915–2922. doi: 10.1007/s00330-020-07389-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Daldrup-Link H. How PET/MR can add value for children with cancer. Curr Radiol Rep. 2017;5(03):15. doi: 10.1007/s40134-017-0207-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Brendle C B, Schmidt H, Fleischer S, Braeuning U H, Pfannenberg C A, Schwenzer N F. Simultaneously acquired MR/PET images compared with sequential MR/PET and PET/CT: alignment quality. Radiology. 2013;268(01):190–199. doi: 10.1148/radiol.13121838. [DOI] [PubMed] [Google Scholar]
- 23.Broski S M, Goenka A H, Kemp B J, Johnson G B. Clinical PET/MRI: 2018 update. AJR Am J Roentgenol. 2018;211(02):295–313. doi: 10.2214/AJR.18.20001. [DOI] [PubMed] [Google Scholar]
- 24.Bernasconi A, Cendes F, Theodore W H. Recommendations for the use of structural magnetic resonance imaging in the care of patients with epilepsy: a consensus report from the International League Against Epilepsy Neuroimaging Task Force. Epilepsia. 2019;60(06):1054–1068. doi: 10.1111/epi.15612. [DOI] [PubMed] [Google Scholar]
- 25.Knake S, Triantafyllou C, Wald L L. 3T phased array MRI improves the presurgical evaluation in focal epilepsies: a prospective study. Neurology. 2005;65(07):1026–1031. doi: 10.1212/01.wnl.0000179355.04481.3c. [DOI] [PubMed] [Google Scholar]
- 26.Boerwinkle V L, Mohanty D, Foldes S T. Correlating resting-state functional magnetic resonance imaging connectivity by independent component analysis-based epileptogenic zones with intracranial electroencephalogram localized seizure onset zones and surgical outcomes in prospective pediatric intractable epilepsy study. Brain Connect. 2017;7(07):424–442. doi: 10.1089/brain.2016.0479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Boerwinkle V L, Mirea L, Gaillard W D. Resting-state functional MRI connectivity impact on epilepsy surgery plan and surgical candidacy: prospective clinical work. J Neurosurg Pediatr. 2020:1–8. doi: 10.3171/2020.1.PEDS19695. [DOI] [PubMed] [Google Scholar]
- 28.Ciccarelli O, Catani M, Johansen-Berg H, Clark C, Thompson A. Diffusion-based tractography in neurological disorders: concepts, applications, and future developments. Lancet Neurol. 2008;7(08):715–727. doi: 10.1016/S1474-4422(08)70163-7. [DOI] [PubMed] [Google Scholar]
- 29.Ahmadi M E, Hagler D J, Jr, McDonald C R. Side matters: diffusion tensor imaging tractography in left and right temporal lobe epilepsy. Am J Neuroradiol. 2009;30(09):1740–1747. doi: 10.3174/ajnr.A1650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Rosazza C, Deleo F, D'Incerti L. Tracking the re-organization of motor functions after disconnective surgery: a longitudinal fMRI and DTI study. Front Neurol. 2018;9:400. doi: 10.3389/fneur.2018.00400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kiehna E N, Widjaja E, Holowka S. Utility of diffusion tensor imaging studies linked to neuronavigation and other modalities in repeat hemispherotomy for intractable epilepsy. J Neurosurg Pediatr. 2016;17(04):483–490. doi: 10.3171/2015.7.PEDS15101. [DOI] [PubMed] [Google Scholar]
- 32.Chang D J, Zubal I G, Gottschalk C. Comparison of statistical parametric mapping and SPECT difference imaging in patients with temporal lobe epilepsy. Epilepsia. 2002;43(01):68–74. doi: 10.1046/j.1528-1157.2002.21601.x. [DOI] [PubMed] [Google Scholar]
- 33.von Oertzen T J, Mormann F, Urbach H. Prospective use of subtraction ictal SPECT coregistered to MRI (SISCOM) in presurgical evaluation of epilepsy. Epilepsia. 2011;52(12):2239–2248. doi: 10.1111/j.1528-1167.2011.03219.x. [DOI] [PubMed] [Google Scholar]
- 34.Hauptman J S, Mathern G W. Surgical treatment of epilepsy associated with cortical dysplasia: 2012 update. Epilepsia. 2012;53 04:98–104. doi: 10.1111/j.1528-1167.2012.03619.x. [DOI] [PubMed] [Google Scholar]
- 35.Palmini A, Holthausen H. Focal malformations of cortical development: a most relevant etiology of epilepsy in children. Handb Clin Neurol. 2013;111:549–565. doi: 10.1016/B978-0-444-52891-9.00058-0. [DOI] [PubMed] [Google Scholar]
- 36.Lerner J T, Salamon N, Hauptman J S. Assessment and surgical outcomes for mild type I and severe type II cortical dysplasia: a critical review and the UCLA experience. Epilepsia. 2009;50(06):1310–1335. doi: 10.1111/j.1528-1167.2008.01998.x. [DOI] [PubMed] [Google Scholar]
- 37.Kim Y H, Kang H C, Kim D S. Neuroimaging in identifying focal cortical dysplasia and prognostic factors in pediatric and adolescent epilepsy surgery. Epilepsia. 2011;52(04):722–727. doi: 10.1111/j.1528-1167.2010.02950.x. [DOI] [PubMed] [Google Scholar]
- 38.Juhász C, John F. Utility of MRI, PET, and ictal SPECT in presurgical evaluation of non-lesional pediatric epilepsy. Seizure. 2020;77:15–28. doi: 10.1016/j.seizure.2019.05.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Shang K, Wang J, Fan X. Clinical value of hybrid TOF-PET/MR imaging-based multiparametric imaging in localizing seizure focus in patients with MRI-negative temporal lobe epilepsy. Am J Neuroradiol. 2018;39(10):1791–1798. doi: 10.3174/ajnr.A5814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Casse R, Rowe C C, Newton M, Berlangieri S U, Scott A M. Positron emission tomography and epilepsy. Mol Imaging Biol. 2002;4(05):338–351. doi: 10.1016/s1536-1632(02)00071-9. [DOI] [PubMed] [Google Scholar]
- 41.Gok B, Jallo G, Hayeri R, Wahl R, Aygun N. The evaluation of FDG-PET imaging for epileptogenic focus localization in patients with MRI positive and MRI negative temporal lobe epilepsy. Neuroradiology. 2013;55(05):541–550. doi: 10.1007/s00234-012-1121-x. [DOI] [PubMed] [Google Scholar]
- 42.Sinclair D B, Wheatley M, Aronyk K. Pathology and neuroimaging in pediatric temporal lobectomy for intractable epilepsy. Pediatr Neurosurg. 2001;35(05):239–246. doi: 10.1159/000050429. [DOI] [PubMed] [Google Scholar]
- 43.Yang P F, Pei J S, Zhang H J. Long-term epilepsy surgery outcomes in patients with PET-positive, MRI-negative temporal lobe epilepsy. Epilepsy Behav. 2014;41:91–97. doi: 10.1016/j.yebeh.2014.09.054. [DOI] [PubMed] [Google Scholar]
- 44.Curatolo P, Bombardieri R, Verdecchia M, Seri S. Intractable seizures in tuberous sclerosis complex: from molecular pathogenesis to the rationale for treatment. J Child Neurol. 2005;20(04):318–325. doi: 10.1177/08830738050200040901. [DOI] [PubMed] [Google Scholar]
- 45.Capraz I Y, Kurt G, Akdemir Ö. Surgical outcome in patients with MRI-negative, PET-positive temporal lobe epilepsy. Seizure. 2015;29:63–68. doi: 10.1016/j.seizure.2015.03.015. [DOI] [PubMed] [Google Scholar]
- 46.Arya R, Mangano F T, Horn P S. Long-term seizure outcomes after pediatric temporal lobectomy: does brain MRI lesion matter? J Neurosurg Pediatr. 2019;24(02):200–208. doi: 10.3171/2019.4.PEDS18677. [DOI] [PubMed] [Google Scholar]
- 47.Evans L T, Morse R, Roberts D W. Epilepsy surgery in tuberous sclerosis: a review. Neurosurg Focus. 2012;32(03):E5. doi: 10.3171/2012.1.FOCUS11330. [DOI] [PubMed] [Google Scholar]
- 48.Jarrar R G, Buchhalter J R, Raffel C. Long-term outcome of epilepsy surgery in patients with tuberous sclerosis. Neurology. 2004;62(03):479–481. doi: 10.1212/01.wnl.0000106947.18643.1d. [DOI] [PubMed] [Google Scholar]
- 49.Asano E, Chugani D C, Muzik O. Multimodality imaging for improved detection of epileptogenic foci in tuberous sclerosis complex. Neurology. 2000;54(10):1976–1984. doi: 10.1212/wnl.54.10.1976. [DOI] [PubMed] [Google Scholar]
- 50.Rintahaka P J, Chugani H T. Clinical role of positron emission tomography in children with tuberous sclerosis complex. J Child Neurol. 1997;12(01):42–52. doi: 10.1177/088307389701200107. [DOI] [PubMed] [Google Scholar]
- 51.Kalantari B N, Salamon N. Neuroimaging of tuberous sclerosis: spectrum of pathologic findings and frontiers in imaging. Am J Roentgenol. 2008;190(05):W304-9. doi: 10.2214/AJR.07.2928. [DOI] [PubMed] [Google Scholar]
- 52.Chandra P S, Salamon N, Huang J. FDG-PET/MRI coregistration and diffusion-tensor imaging distinguish epileptogenic tubers and cortex in patients with tuberous sclerosis complex: a preliminary report. Epilepsia. 2006;47(09):1543–1549. doi: 10.1111/j.1528-1167.2006.00627.x. [DOI] [PubMed] [Google Scholar]
- 53.Aboian M S, Wong-Kisiel L C, Rank M, Wetjen N M, Wirrell E C, Witte R J. SISCOM in children with tuberous sclerosis complex-related epilepsy. Pediatr Neurol. 2011;45(02):83–88. doi: 10.1016/j.pediatrneurol.2011.05.001. [DOI] [PubMed] [Google Scholar]
- 54.Lachhwani D K, Pestana E, Gupta A, Kotagal P, Bingaman W, Wyllie E. Identification of candidates for epilepsy surgery in patients with tuberous sclerosis. Neurology. 2005;64(09):1651–1654. doi: 10.1212/01.WNL.0000160389.93984.53. [DOI] [PubMed] [Google Scholar]
- 55.Verdinelli C, Olsson I, Edelvik A, Hallböök T, Rydenhag B, Malmgren K. A long-term patient perspective after hemispherotomy–a population based study. Seizure. 2015;30:76–82. doi: 10.1016/j.seizure.2015.05.016. [DOI] [PubMed] [Google Scholar]
- 56.Moosa A N, Gupta A, Jehi L. Longitudinal seizure outcome and prognostic predictors after hemispherectomy in 170 children. Neurology. 2013;80(03):253–260. doi: 10.1212/WNL.0b013e31827dead9. [DOI] [PubMed] [Google Scholar]
- 57.Ji T, Liu M, Wang S. Seizure outcome and its prognostic predictors after hemispherotomy in children with refractory epilepsy in a Chinese pediatric epileptic center. Front Neurol. 2019;10:880. doi: 10.3389/fneur.2019.00880. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Kelley B P, Patel S C, Marin H L, Corrigan J J, Mitsias P D, Griffith B. Autoimmune encephalitis: pathophysiology and imaging review of an overlooked diagnosis. AJNR Am J Neuroradiol. 2017;38(06):1070–1078. doi: 10.3174/ajnr.A5086. [DOI] [PMC free article] [PubMed] [Google Scholar]