

The burden of disability is an important public health challenge as the majority of people will experience disability throughout their life. Disability includes impairments, activity limitations and participation restrictions, all of which may reduce the capability for work. People with chronic disabilities that limit the ability to work are granted disability pensions in many countries. Therefore, disability pension is informative for health and disease outcomes, as well as for economic consequences.
Previous studies have indicated that obesity as well as low cardiorespiratory fitness and muscular strength already in adolescence are related to later mortality and disease, but few studies have examined corresponding associations for future disability due to all and specific chronic diseases. Thus, we examined the associations of obesity, cardiorespiratory fitness and muscular strength in male adolescents with later disability pension due to all and specific causes in more than 1 million participants through linkage of data from the Swedish conscription registry with other nationwide registries.1–3
Low cardiorespiratory fitness in isolation1 3, or together with low muscular strength2 or obesity1 3, was a strong risk factor for later disability pension due to all and specific causes (eg, psychiatric, musculoskeletal and cardiovascular diseases). Strengths of these previous studies include the large size and representativeness of the study sample (97%–98% of all adolescent males since conscription was mandatory by law during the study years3), the long follow-up (~30 years) and the objective markers of chronic disability (ie, disability pension) and exposures. However, thus far, no actual estimation of the proportion of chronic disabilities that may have been prevented with greater levels of physical fitness in adolescence, and particularly for cardiorespiratory fitness has been conducted.1–3 Calculation of the population attributable fraction (PAF) is a common way to express the potential health effects of a specific exposure.
The PAF estimates the proportion of cases that would not occur if the risk factor was reduced or eliminated, given certain assumptions including casualty. This approach has been used in landmark studies in the field, for example, for estimating how many premature deaths would be prevented globally by increasing physical activity.4 PAF estimates from well-designed prospective cohort studies are informative and useful from a public health point of view.
POPULATION-ATTRIBUTABLE FRACTION OF CHRONIC DISABILITY ASSOCIATED WITH LOW CARDIORESPIRATORY FITNESS
In this editorial, we utilised the data from our previous study3 to compute new PAF analyses in order to quantify the proportion of future disability pensions that may have been prevented if the population would improve their cardiorespiratory fitness. A complete description on the statistical methods used for PAF computations is provided as online supplementary material. In brief, data from 1 079 128 male adolescents (16–19 years) who conscripted between 1972 and 1994 were utilised. At conscription, males had their cardiorespiratory fitness assessed as the maximal watts achieved in a maximal cycle ergometer test. Over a median follow-up of ~30 years, 54 304 men obtained a disability pension due to any cause. We calculated the later chronic disability PAF adjusted for potential confounders under two scenarios: (1) if unfit participants (deciles 1–2) were to become fit (ie, deciles 3–10), according to the most used definition of unfit (first quintile, lower 20%) and fit (quintiles second to fifth, upper 80%)5 and (2) if all participants (apart from those already in the highest decile of fitness) were to increase their fitness by 1 decile.
PAF estimates for increasing physical fitness are presented in figure 1. Briefly, PAF from all-causes were estimated to be 14.2% if all unfit adolescents were to be fit, and 10.2% if participants in deciles 1–9 improved their fitness corresponding to 1 decile, eg moving from the 50th percentile to the 60th percentile in fitness (detailed data in online supplementary table 1). Interestingly, the PAF associated with increases in cardiorespiratory fitness was relatively high for both all and specific causes of chronic disability indicating that many cases of disabilities may have been prevented through increasing physical fitness in youth. Our data indicated that a 1 decile improvement in cardiorespiratory fitness was associated with a 10% decrease in chronic disabilities. This is comparable in magnitude with previous PAF estimations of the burden of physical inactivity on major non-communicable diseases.4
Figure 1.
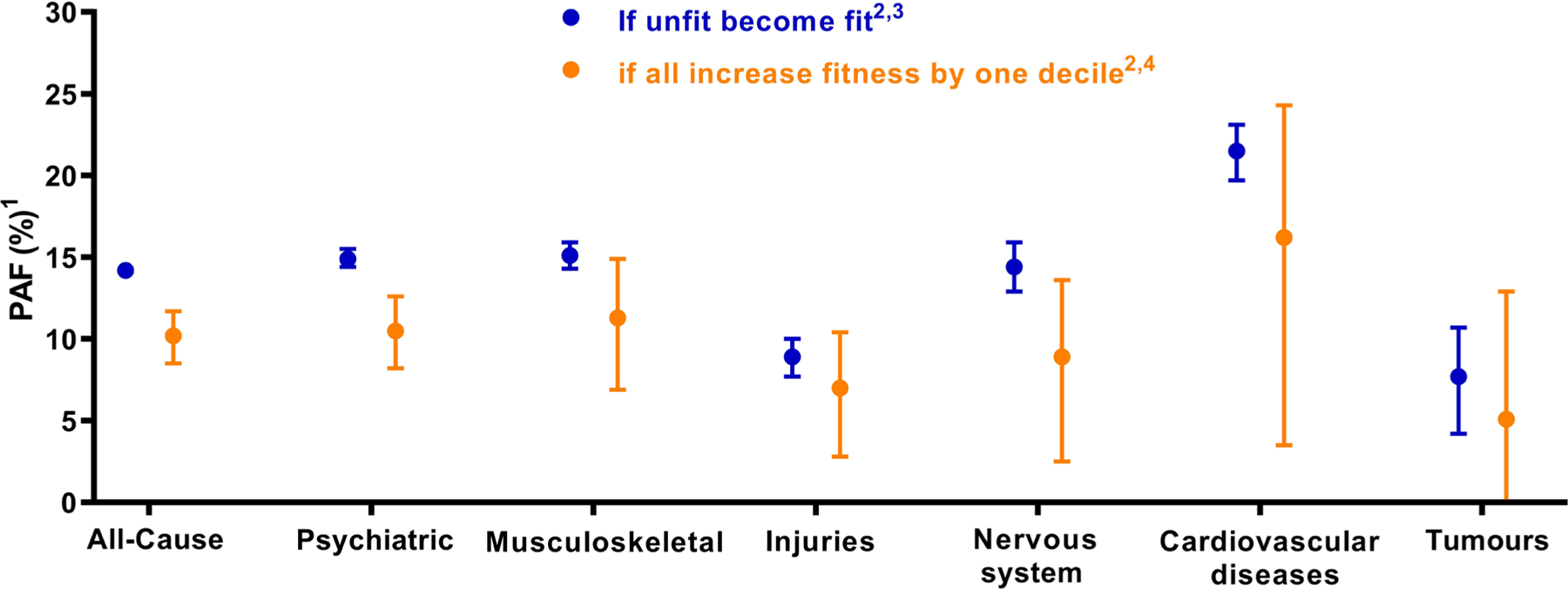
PAFs with 95% CIs for later disability by cause associated with lower physical fitness (see online supplementary table 2 for exact estimates and confidence intervals). 1PAF is adjusted for conscription year, age, childhood socioeconomic position and BMI at conscription. Models with disability pension due to all or psychiatric causes were also adjusted for any mental hospitalisation before conscription and for any psychiatric diagnosis at conscription. 2Fitness levels were categorised by deciles of cardiorespiratory fitness. Decile 1 ≤211 Watts; decile 2=212–229 Watts; decile 3=230–241 Watts; decile 4=242–254 Watts; decile 5=255–270 Watts; decile 6=271–284 Watts; decile 7=285–300 Watts; decile 8=301–320 Watts; decile 9=321–343 Watts; decile 10 ≥344 Watts. 3If unfit participants (ie, deciles 1–2) were to become fit (ie, deciles 3–10). 4If all participants with a fitness level in deciles 1–9 were to increase their fitness by 1 decile. BMI, body mass index; PAF, population attributable fraction.
These are, to the best of our knowledge, the first estimates of PAF for chronic disabilities associated with low cardiorespiratory fitness in youth. Although the observed PAFs demonstrate great potential of increasing physical fitness in youth in order to mitigate the burden of chronic disabilities, we acknowledge limitations. First, our studies were performed within a population-based cohort of male participants and there is a need for studies in women. Second, although our study controlled for a set of potentially important confounders, we cannot exclude the possibility that some residual confounding still exists. Third, as for many other traits such as body height and weight, physical fitness is the result of both genetic and environmental factors although increases in physical fitness are achievable through physical activity and/or exercise in most individuals.6
In summary, our results clearly point out that adequate cardiorespiratory fitness in adolescence may lower the risk of chronic disability decades later. Our series of studies1–3 also support that physical fitness evaluation in young ages (eg, in schools, sport and health centres) is meaningful and informative for predicting future health and disease. These findings (together with those reported in our previous studies1–3) align well with the increasing amount of evidence7 8 supporting cardiorespiratory fitness as a potential marker of future health in young people.
Supplementary Material
Funding
FBO was supported by a visiting grant (to MLs research group) from Henning and Johan Throne-Holst Foundation. EJS is supported by the Intramural Research Program at the National Institute on Aging (USA). This study was conducted under the umbrella of the ActiveBrains and the SmarterMove projects supported by the MINECO/FEDER (DEP2013–47540, DEP2016–79512-R, DEP2017–91544-EXP). Additional funding was obtained from the University of Granada, Plan Propio de Investigación 2016, Excellence actions: Units of Excellence; Scientific Excellence Unit on Exercise and Health (UCEES); and Junta de Andalucía, Consejería de Conocimiento, Investigación y Universidades and European Regional Development Funds (ref. SOMM17/6107/UGR). These funders had no role in study design, data collection, analysis, or interpretation, writing of the report or in the decision to submit the paper for publication.
Footnotes
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Additional material is published online only. To view please visit the journal online (http://dx.doi.org/10.1136/bjsports-2020-102605).
REFERENCES
- 1.Henriksson H, Henriksson P, Tynelius P, et al. Cardiorespiratory fitness, muscular strength, and obesity in adolescence and later chronic disability due to cardiovascular disease: a cohort study of 1 million men. Eur Heart J 2020;41:1503–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Henriksson H, Henriksson P, Tynelius P, et al. Muscular weakness in adolescence is associated with disability 30 years later: a population-based cohort study of 1.2 million men. Br J Sports Med 2019;53:1221–30. [DOI] [PubMed] [Google Scholar]
- 3.Henriksson P, Henriksson H, Tynelius P, et al. Fitness and body mass index during adolescence and disability later in life: a cohort study. Ann Intern Med 2019;170:230–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lee I-M, Shiroma EJ, Lobelo F, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet 2012;380:219–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ortega FB, Ruiz JR, Labayen I, et al. The Fat but Fit paradox: what we know and don’t know about it. Br J Sports Med 2018;52:151–3. [DOI] [PubMed] [Google Scholar]
- 6.Bouchard C, An P, Rice T, et al. Familial aggregation of VO(2max) response to exercise training: results from the HERITAGE Family Study. J Appl Physiol 1999;87:87. [DOI] [PubMed] [Google Scholar]
- 7.Lavie CJ, Ozemek C, Carbone S, et al. Sedentary behavior, exercise, and cardiovascular health. Circ Res 2019;124:799–815. [DOI] [PubMed] [Google Scholar]
- 8.Ross R, Blair SN, Arena R, et al. Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign: a scientific statement from the American heart association. Circulation 2016;134:e653–99. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.